
Abstract
Background
The etiology, epidemiology, treatment patterns, and clinical outcomes of neonatal and pediatric pneumonia patients in China are not well reported. This retrospective chart review study aimed to describe such information among neonatal (0 to 27 days) and pediatric (28 days to <18 years) pneumonia patients in two regions of China.
Methods
Electronic medical records of pneumonia hospitalizations (aged <18 years) admitted between 2008 and 2013 from four hospitals under Guangdong Provincial Hospital of Chinese Medicine (Southern China) and between 2010 and 2014 at Peking University People’s Hospital (Beijing, Northern China) were reviewed.
Results
The average age of neonatal hospitalizations in Beijing (n=92) was 3.5 days. The mean length of hospital stay was 11.2 days, and no deaths occurred. Staphylococcus epidermidis was the most common bacteria found in Beijing patients, whereas Mycoplasma pneumoniae was the most common bacteria found in Guangdong patients. The average age of pediatric hospitalizations was 3.3 (±3.1) and 6.5 (±5.6) years in Guangdong (n=3,046) and Beijing (n=222), respectively. The mean length of hospital stay was 17.4 and 5.8 days, and overall mortality rates were 0.2% and 0.5%.
Conclusion
The findings revealed a low level of bacterial isolation and hence microbiological diagnoses. There was a low level of in-hospital mortality due to pneumonia, and the majority of hospitalizations were discharged from hospital, suggesting that current practice was generally effective. Neonatal hospitalizations were greater than pediatric hospitalizations in Beijing along with disparity in bacterial profile when compared with Guangdong, intending a need to improve neonatal pneumonia prophylaxis and selection of appropriate treatment.
Introduction
Children are the most common victims of pneumonia. Annually, close to 156 million children present with pneumonia within 5 years of birth worldwide. It is estimated that two million cases result in death, of which ~95% occur in developing countries.Citation1 China alone contributes to 21 million pediatric pneumonia cases annually with towering rates of hospitalizations and mortality.Citation2 Neonates are at the greatest risk of death from pneumoniaCitation3,Citation4 as many of the normal lung defenses are not yet fully developed, leading to an increased susceptibility to infection.Citation4 Additionally, mortality rates are considerably higher among low birth weight neonates compared with normal birth weight neonates.Citation5 The etiology of bacterial pneumonia differs depending on the source of infection. Community-acquired pneumonia (CAP) is the single leading cause of death globally in children aged <5 years.Citation6 The etiological agents implicated in childhood CAP worldwide vary with age. Group B streptococcus and Gram-negative enteric bacteria are the most commonly isolated CAP pathogens in neonates <3 weeks old and are often acquired from the mother by vertical transmission.Citation7 Streptococcus pneumoniae is the most common etiological agent of CAP in infants aged 3 weeks to 3 months, followed by viral pathogens,Citation8 whereas Mycoplasma pneumoniae and Chlamydia pneumoniae are the common bacterial causes of CAP from 4 months to adolescence.Citation7
Hospital-acquired pneumonia (HAP) is one of the fatal hospital-acquired infections in the pediatric intensive care unit (ICU) associated with a different epidemiological and etiological profile compared with CAP. Viruses (most commonly respiratory syncytial virus) cause majority of the pediatric HAP cases globally.Citation8 Gram-negative bacteria, such as Escherichia coli, Klebsiella pneumoniae, and Pseudomonas aeruginosa, are the predominant causes of HAP.Citation9 Early-onset neonatal pneumonia often develops in utero or within the first week of life and is predominantly caused by Gram-negative bacteria.Citation3 Gram-negative bacilli are responsible for 30% of nosocomial pneumonias in neonates.Citation10 In contrast, Gram-positive bacteria are responsible for the largest proportion of HAP later in the neonatal periodCitation3 and many, including methicillin-resistant S. aureus (MRSA), coagulase-negative staphylococci (predominantly Staphylococcus epidermidis), and vancomycin-resistant enterococci, are multidrug resistant.
Because of the large number of pathogenic agents that can cause pneumonia in neonates and children, determining the cause in an individual patient may be challenging. Even with the use of sophisticated laboratory techniques, it is not possible to identify a causative pathogen in 25%–33% of pneumonia cases.Citation11 Etiological studies of childhood pneumonia are complicated by difficulties in obtaining an accurate microbiological diagnosis, due to the reluctance of physicians to perform invasive procedures such as lung aspiration and bronchoalveolar lavage (BAL) in children, difficulties obtaining adequate sputum samples, and the low yield of pathogens identified from blood cultures.Citation12 Such difficulties are exacerbated in the developing world due to limited facilities and resources to perform appropriate specimen collection and testing.
Few recent studies have documented the bacterial etiology of childhood pneumonia in China. S. pneumoniae and Haemophilus influenzae have been implicated in pediatric pneumonia in China;Citation13 however, these results were based on the presence of bacteria in the nasopharynx, which may not necessarily be indicative of lower respiratory tract infection, as normal bacterial flora, as well as pneumonia pathogens, are frequently identified.Citation10,Citation11 A retrospective study on the neonatal mortality rates in China from the last two decades revealed that 4/5th of the total mortality was due to premature birth, congenital abnormalities, or pneumonia and that the scenario has improved lately in both urban and rural areas since then.Citation14 Interhospital variations in prescribing treatments and microbiological diversity may differ among different regions of the country. Hence, a comparative study on the prevalence, microbial profile, prescribing patterns, and hospital diagnosis of different hospitals may be useful for health care professionals and researchers to realize and rectify the gaps in the prevention of the disease and to set novel/updated treatment guidelines. For this purpose, we reviewed patient demographics, microbiological characteristics, treatment patterns, and clinical outcomes of hospitalized neonatal and pediatric patients diagnosed with pneumonia in hospitals of northern and southern China.
Methods
Study sites, subjects, and design
This was a retrospective, noninterventional, chart review to assess the epidemiology, clinical management, and outcomes of neonatal and pediatric patients hospitalized with pneumonia, using data from Guangdong Provincial Hospital of Chinese Medicine (CM), Guangzhou, Guangdong Province, China, and Peking University People’s Hospital, Beijing, China.
Electronic medical records (EMR) of all unique hospitalizations (admissions to hospital) with an International Classification of Diseases diagnosis code of pneumonia, interstitial pulmonary disease/other lung infection with a positive bacterial culture, or influenza with no virus identified prior to discharge between 2008 and 2013 at the Guangdong hospital and between 2010 and 2014 at the Beijing hospital were reviewed and extracted for analysis.
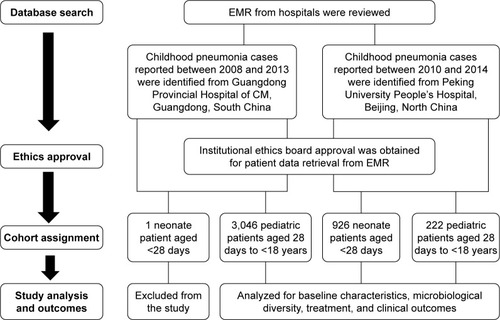
Study flow chart is depicted in . Data for hospitalizations aged <18 years are presented. Data from the two study sites were analyzed separately to enable comparison. Neonatal and pediatric data were analyzed separately, due to the inherent differences between these two patient populations. Neonatal hospitalizations were defined as those aged 0 to 27 days, and pediatric hospitalizations were defined as those aged 28 days to <18 years. Data for adult hospitalizations aged 18 years or older will be reported separately. Hospitalizations receiving CM only (without any conventional antimycotic, antiviral, or antibiotic therapy) were excluded from the clinical outcome analyses to avoid biasing the results.
Figure 1 Study flow chart.
Ethical considerations
Individual patient data were anonymized, and ethical approval was granted by the relevant institutional ethics board committees at each site (Ethics Committee of Guangdong Provincial Hospital of CM and Ethics Committee of Peking University People’s Hospital). This study involved the collection of existing data and records. Informed consent was exempted according to the decision of institutional ethics board committees.
Data collection
Study variables included patient baseline demographics, medical history (including comorbidities and surgical intervention), frequently used antibiotics, and clinical outcomes. Demographic information extracted for analysis included: age, gender and ethnic origin. Clinical outcomes data extracted for analysis included length of hospital stay, recurrence of infection, ICU admission, discharge from hospital, and in-hospital mortality. Microbiological data regarding bacteria identified by culture tests (except for M. pneumoniae in Beijing, which was identified using serological methods) of patient sputum/respiratory secretions and blood samples, which were collected when possible/as clinically indicated, were also extracted. Bacteria were identified according to the Clinical and Laboratory Standards Institute guidelines.Citation15
Statistical analysis
All descriptive analyses were conducted using R Statistics Software (Version R3.1.1). Continuous data are expressed as the mean ± standard deviation. Categorical data are expressed as the number of events and percentages.
Results
Baseline characteristics
The study included 3,046 pediatric hospitalizations (2,706 unique patients) from Guangdong Provincial Hospital and 926 neonatal and 226 pediatric hospitalizations (1,112 unique patients) from Peking University People’s Hospital. One patient may have more than one hospitalization visit. Since only one neonatal hospitalization was identified from Guangdong Provincial Hospital of CM, it was excluded from the study. The most common comorbidities were hospital tonsillitis, bronchial disorder, and anemia in Guangdong pediatric hospitalizations, whereas blood tumor was predominant in pediatric hospitalizations of Peking University People’s Hospital. Neonatal hospitalizations of Peking University People’s Hospital presented anemia, neonatal hyperalbuminemia, and septicemia. Further details on baseline demographics, concomitant medication use, and surgical intervention are presented in .
Table 1 Baseline patient demographics, comorbidities, and surgical interventions
Pathogen profiling
Microbiological characteristics and outcomes of pediatric hospitalizations in Guangdong Provincial Hospital of CM
A total of 241 microbiological samples were culture positive, the majority (180/241 [74.7%]) of which were collected from pharyngeal swabs. Fifty (20.7%) culture positive samples were collected from sputum, nine (3.7%) samples were collected from blood, and two (0.8%) samples were collected from BAL. Bacteria were isolated from 236/3,046 (7.7%) hospitalizations; 21 (8.9%) had multiple bacterial organisms identified, and the remainder had a single bacterial organism identified. Two hundred seven (78.1%) of the 265 bacteria isolated were from samples collected within 2 days of hospital admission. The atypical organism M. pneumoniae was the most frequently isolated organism, identified in 154/236 (65.3%) hospitalizations (). The most common bacteria were S. aureus (20/236 [8.5%]) and Acinetobacter baumanii (12/236 [5.1%]; ). Of the 20 hospitalizations in whom S. aureus was isolated, three had MRSA and 17 had methicillin-susceptible S. aureus (MSSA).
Table 2 Bacteria isolated ≥2 hospitalizations at either hospitalTable Footnotea
Microbiological characteristics and outcomes of neonatal hospitalizations in Peking University People’s Hospital
A total of 25 microbiological samples were culture positive, of which 24 samples were collected from blood and one sample was obtained from sputum. Bacteria were isolated from 24/926 (2.6%) neonates; one neonate had two bacterial organisms identified (P. aeruginosa + Listeria monocytogenes), and the remainder had a single bacterial organism identified. Twenty-one (84.0%) of the 25 bacteria isolated were from samples collected within 2 days of hospital admission. The most common bacteria, isolated in 10/24 (41.7%) hospitalizations, was S. epidermidis ().
Microbiological characteristics and outcomes of pediatric hospitalizations in Peking University People’s Hospital
A total of 14 microbiological samples were culture positive, of which 7/14 (50.0%) were collected from sputum and 7/14 (50.0%) were obtained from blood; none were obtained from BAL, pharyngeal swabs, or bronchial secretions. Eight of the 18 (44.4%) bacteria isolated were from samples collected within 2 days of hospital admission. Bacteria were isolated from 14/222 (6.3%) hospitalizations; a single bacterial organism was identified in 11 hospitalizations; multiple bacterial organisms were identified in the remaining three hospitalizations. The bacteria most frequently identified using culture-based methods was Acinetobacter junii, isolated in 3/14 (21.4%) hospitalizations (). Of the 50 hospitalizations, whose blood was tested for antibodies against M. pneumoniae, seven (14.0%) were positive.
Choice of treatment and outcomes
Clinical outcomes and treatment patterns of pediatric hospitalizations in Guangdong Provincial Hospital of CM
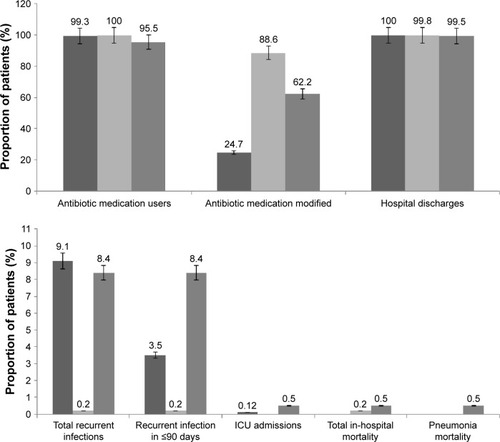
The mean (SD) length of hospital stay was 5.8 (3) days, and the median length of stay was 5 days. The majority of hospitalizations (2,526/3,046 [82.9%]) received antibiotic therapy; among these hospitalizations, medication was modified in 625 (24.7%) hospitalizations ().
Figure 2 Clinical outcomes of neonatal and pediatric patients in Guangdong and Peking University hospitals.
In addition, CM was used only in Guangdong Provincial Hospital of CM. In total, CM was used in 2,814/3,046 (92.4%) hospitalizations. Four hundred fifty-two (14.9%) hospitalizations received CM without any concomitant antimycotic, antiviral, or antibiotic therapy and were excluded from the clinical outcome analyses. Clinical outcomes for the remaining 2,545/3,046 (83.6%) hospitalizations who received conventional antimycotic, antiviral, or antibiotic therapy are detailed in . The mean (SD) length of hospital stay was 5.8 (3.0) days, and the median length of stay was 5 days. Recurrence of infection within 90 days was low (80/2,297 [3.5%] patients for whom recurrence data were available). The majority of hospitalized patients were discharged, only one patient reported death caused by severe influenza A (H1N1) virus infection, which was not considered attributable to pneumonia infection.
Table 3 Frequently used antibiotics for initial therapy and overall at both the study hospitals
As S. aureus was the most common bacteria isolated, clinical outcomes of hospitalizations with S. aureus infection were assessed. The mean length of stay was similar in hospitalizations with MRSA (6.0 days) and longer in hospitalizations with MSSA (9.4 days) when compared with the overall population (5.7 days). None of the hospitalizations with MRSA or MSSA died due to pneumonia. Note that there were only three hospitalizations with MRSA (); due to the low number there may be a bias in the results.
Clinical outcomes and treatment patterns of neonatal hospitalizations in Peking University People’s Hospital
The mean (SD) length of hospital stay was 11.2 (7.4) days, and the median length of stay was 9 days. The majority of hospitalized patients were discharged (924/926 [99.8%]), while two patients died during the hospitalization course, and these deaths were not attributable to pneumonia infection. Recurrence of infection within 90 days was low (2/924 patients for whom recurrence data were available). Of all the patients given antibiotics, modification of initial antibiotic treatment occurred in 820/926 (88.6%) patients ().
Clinical outcomes and treatment patterns of pediatric hospitalizations in Peking University People’s Hospital
The mean (SD) length of hospital stay was 17.4 (19.9) days, and the median length of stay was 11 days. The majority of hospitalizations (221/222 [99.5%]) were discharged. One hospitalized patient died, and the death was considered attributable to the pneumonia infection. Recurrence of infection within 90 days was low (16/190 [8.4%] patients for whom recurrence data were available). The majority of hospitalizations (212/222 [95.5%]) received antibiotic therapy; among these hospitalizations, medication was modified in 138 (62.2%) patients (). The most frequently used antibiotics at both hospitals for neonatal and pediatric patients are listed in .
Discussion
This retrospective, observational study gathered detailed epidemiological information on patient characteristics, treatment patterns, and clinical outcomes in neonatal and pediatric pneumonia hospitalizations from hospitals in different regions of China. It is plausible that, as in Western countries, there is a high frequency of viral pneumonia in pediatric populations in China,Citation6 potentially explaining the low isolation rate of bacteria. The most common bacterial organism isolated in pediatric hospitalizations in Beijing was A. junii. Acinetobacter species are commonly found in the context of HAP,Citation16 and it is plausible that A. junii infection may have been acquired in the hospital setting due to the long mean length of hospital stay observed in pediatric hospitalizations in Beijing. However, due to the low number of hospitalizations with at least one bacterial organism isolated and the fact that it was impossible to distinguish between colonization and infection in this study, clearly determining the microbiological cause of pneumonia in these hospitalizations was not possible.
M. pneumoniae was the predominant bacteria isolated from pediatric hospitalizations in Guangdong, followed by S. aureus and A. baumanii. M. pneumoniae is a well-known cause of CAP among pediatric patients,Citation17 and a high prevalence of atypical pathogens among Asian patients with CAP has been reported in a previous study.Citation17 There was a greater prevalence of M. pneumoniae in Guangdong than in Beijing. However, it should be noted that different detection methods were used for M. pneumoniae at the two sites – culture was used in Guangdong and antibody testing in Beijing – highlighting the difficulty in the comparison of retrospective data from two independent study centers. There was a low level of in-hospital mortality due to pneumonia (zero in Guangdong and close to zero in Beijing), with 99.6%–100% of hospitalizations being discharged. The high proportion of M. pneumoniae isolates may be a factor in this low mortality rate, as M. pneumoniae is generally associated with favorable clinical outcomes.Citation18 Additionally, previous studies indicate that the most fatal pneumonia cases in children are caused by H. influenzae or S. pneumoniae;Citation19 the low level of isolation of these bacteria in the current study may help to explain the low number of deaths due to pneumonia. The mean length of stay was considerably longer for pediatric hospitalizations in Beijing as compared with Guangdong, and the frequency of modification of antibiotic therapy was three times higher. The fact that Beijing is a tertiary referral facility for patients requiring specialist care might explain this finding, as it is plausible that there may have been a greater proportion of severe or complicated cases compared with Guangdong Provincial Hospital of CM. Recurrence of infection was rare in neonatal hospitalizations (0.2%), and in pediatric hospitalizations, the frequency of recurrence was the same across the participating hospitals (8.4% in both Beijing and Guangdong). The frequency of ICU admission was close to zero at both sites in all patient subgroups. In hospitalizations with S. aureus infection, the length of stay was longer and the frequency of antibiotic modification was higher compared with the overall population; however, no deaths occurred in hospitalizations with S. aureus infection. The causative pathogens implicated in pediatric pneumonia are distinct in developed countries where there is greater involvement of viral and atypical organismsCitation20–Citation23 compared with developing countries where bacterial pathogens account for a significant proportion (60%) of pneumonia cases,Citation24 the most important of which are S. pneumoniae and H. influenza.Citation17,Citation25 Pneumococcal vaccination is not common in China and, therefore, cannot explain the low frequency of S. pneumoniae isolated in the current study. Pneumococcal urinary antigen tests were not performed at either of the hospitals; this is in line with Western guidelines, which recommend that urinary pneumococcal antigen detection should not be done in young children.Citation11,Citation26 S. epidermidis was the most common bacteria isolated in neonatal hospitalizations in Beijing. Given that all the 10 isolates were from blood samples, it is possible that this is an artifact of contamination with skin flora.Citation27 However, S. epidermidis has been linked to neonatal pneumonia of late onset (>48 hours after birth) and pneumonia in immunocompromised individualsCitation28,Citation29 and is a recognized HAP pathogen in pediatric patients. S. epidermidis was recently identified as a leading opportunistic pathogen in neonatal sepsis at another hospital in China,Citation30 and in the current study, nine of the 10 neonatal hospitalizations with S. epidermidis isolated from blood cultures had comorbid sepsis. It is possible that these bacteria may have been associated with the comorbid septicemia that was reported in 5.9% of neonatal hospitalizations in Beijing, rather than pneumonia. The low level of positive bacterial cultures and the high levels of modification of initial antibiotic in the present study imply that empirical antibiotic therapy was generally modified on the basis of clinical signs. These data highlight the difficulties faced in providing appropriate empiric therapy, which must ultimately be guided by recent knowledge of local pathogens and resistance patterns and is limited in the current study by the low bacterial isolation rates. In the present study, the combination of a macrolide with a cephalosporin was the most common initial therapy. However, it should be noted that in patients for whom bacteria could be isolated, initial antibiotic coverage was de-escalated based upon patient-specific culture results.
The limitation that must be taken into consideration when comparing findings between the Guangdong and Beijing hospitals is the differing patient age distributions between the hospitals. Only one neonatal hospitalization was identified with pneumonia in Guangdong Provincial Hospital of CM during the study period, likely as a result of its small maternity department, and therefore, data of neonates from this site were excluded from this analysis. Furthermore, for the purposes of this study, pediatric and adolescent hospitalizations aged 28 days to <18 years were grouped into one category, which is a wide age range from an epidemiological point of view. In Guangdong, most hospitalizations were aged 3 weeks to 5 years, whereas the majority of hospitalizations in Beijing were neonatal hospitalizations (aged 0–27 days). Etiological agents commonly responsible for pneumonia differ by age group;Citation6 therefore, this variation must be taken into consideration. A further limitation of this study is that it was not possible to distinguish between CAP and HAP.
However, it is rare for EMR to be used for retrospective studies in Asia, especially in China.Citation31 EMR system is still relatively new in China compared to western countries, and the difficulty in cleaning data from Chinese EMR system is also a big problem. In addition, it is hard to access the EMR systems from different hospitals due to the lack of readiness to share data. Our work is the first study in China to compare microbial profile and current treatment practices between two large conglomerate hospitals, which may reflect the scenario and thrust areas of improvements in the field of pneumonia.
Conclusion
This large, retrospective observational study of hospitalizations in different regions of China provides new epidemiological insights into neonatal and pediatric pneumonia in China. The findings revealed M. pneumoniae and S. epidermis as the most common pathogen found in children of Guangdong and Beijing, respectively. There was a low level of in-hospital mortality due to pneumonia, and the majority of hospitalizations were discharged from hospital, suggesting that current practice was generally effective; however, guidelines recommend obtaining microbiological diagnoses wherever possible. We also found that neonatal hospitalizations were greater than pediatric hospitalizations in Beijing, proposing a need to improve neonatal pneumonia prophylaxis and selection of appropriate treatment. In addition, ongoing local and regional surveillance is necessary to monitor the antimicrobial susceptibility and prevalence of pathogens associated with the infection and prescribing patterns.
Author contributions
ZW, JW, and HX conceptualized the study. All authors contributed toward data analysis, drafting and critically revising the paper, gave final approval of the version to be published, and agree to be accountable for all aspects of the work. ZW and JW contributed equally to this work.
Acknowledgments
This study was funded by AstraZeneca. Medical writing support was provided by Liz Bolton of Prime Medica Ltd, Knutsford, Cheshire, UK, and Dr Amit Bhat of Indegene Pvt Ltd, Bangalore, India, funded by AstraZeneca. The authors would like to acknowledge Weiguo Gao of AstraZeneca R&D Information, China, for the medical advice, Shizhou Deng of Peking University People’s Hospital for the data collection support, and Tong Zhu of Yidu Cloud Technology Co., Ltd, for the extraction, integration, and linking of data from EMR. This helped to clarify certain statistically relevant epidemiological characteristics of pediatric pneumonia, which was considered valuable to the subsequent research. The design and conduct of the study, as well as analysis of the study data and opinions, conclusions, and interpretation of the data, are the responsibility of the authors.
Disclosure
JW, HX, and JH are employees of AstraZeneca. DM and JG are former employees of AstraZeneca. ZW, XL, and ZC received institutional/research grant funding from AstraZeneca for the conduct of the study. The authors report no other conflicts of interest in this work.
References
- RudanIBoschi-PintoCBiloglavZMulhollandKCampbellHEpidemiology and etiology of childhood pneumoniaBull World Health Organ200886540841618545744
- GuanXSilkBJLiWPneumonia incidence and mortality in mainland China: systematic review of Chinese and English literature, 1985–2008PLoS One201057e1172120668535
- DukeTNeonatal pneumonia in developing countriesArch Dis Child Fetal Neonatal Ed2005903F211F21915846010
- NissenMDCongenital and neonatal pneumoniaPaediatr Respir Rev20078319520317868917
- MartinsALNascimentoDDSchneiderIJIncidence of community-acquired infections of lower airways among infantsRev Paul Pediatr20163420420926987781
- MichelowICOlsenKLozanoJEpidemiology and clinical characteristics of community-acquired pneumonia in hospitalized childrenPediatrics2004113470170715060215
- ZarHJCottonMFNosocomial pneumonia in pediatric patients: practical problems and rational solutionsPaediatr Drugs200242738311888355
- OstapchukMRobertsDMHaddyRCommunity-acquired pneumonia in infants and childrenAm Fam Physician200470589990815368729
- Htoutou SedlákováMPudováVKolářMBacterial pathogens causing hospital-acquired pneumonia – a multicenter study in the Czech RepublicKlin Mikrobiol Infekc Lek201521101426098488
- Cevey-MacherelMGaletto-LacourAGervaixAEtiology of community-acquired pneumonia in hospitalized children based on WHO clinical guidelinesEur J Pediatr2009168121429143619238436
- HarrisMClarkJCooteNBritish Thoracic Society guidelines for the management of community acquired pneumonia in children: update 2011Thorax201166suppl 2ii1ii2321903691
- ScottJABrooksWAPeirisJSHoltzmanDMulhollandEKPneumonia research to reduce childhood mortality in the developing worldJ Clin Invest200811841291130018382741
- LevineOSLiuGGarmanRLDowellSFYuSYangYHHaemophilus influenzae type B and Streptococcus pneumoniae as causes of pneumonia among children in Beijing, ChinaEmerg Infect Dis20006216517010756150
- LuRLiXGuoSNeonatal mortality in the urban and rural China between 1996 and 2013: a retrospective studyPediatr Res201679568969626761125
- Clinical and Laboratory Standards InstituteAbbreviated identification of bacterial and yeast; approved guidelineDocument m35-a22nd edWayne, PAClinical and Laboratory Standards Institute2015
- Bergogne-BerezinETownerKJAcinetobacter spp. As nosocomial pathogens: microbiological, clinical, and epidemiological featuresClin Microbiol Rev199691481658964033
- NgeowYFSuwanjuthaSChantarojanasririTAn Asian study on the prevalence of atypical respiratory pathogens in community-acquired pneumoniaInt J Infect Dis20059314415315840455
- von BaumHWelteTMarreRSuttorpNLückCEwigSMycoplasma pneumoniae pneumonia revisited within the German competence network for community-acquired pneumonia (CAPNETZ)BMC Infect Dis200996219439072
- ShannFThe management of pneumonia in children in developing countriesClin Infect Dis199521suppl 3S218S2258749670
- GendrelDRaymondJMoulinFEtiology and response to antibiotic therapy of community-acquired pneumonia in French childrenEur J Clin Microbiol Infect Dis19971653883919228482
- IshiwadaNKurosakiTTobaTEtiology of pediatric inpatients with pneumoniaKansenshogaku Zasshi1993676426478360519
- NumazakiKChibaSUmetsuMEtiological agents of lower respiratory tract infections in Japanese childrenIn Vivo200418677115011754
- WubbelLMunizLAhmedAEtiology and treatment of community-acquired pneumonia in ambulatory childrenPediatr Infect Dis J19991829810410048679
- JohnsonWAbdulkarimAChildhood pneumonia in developing countriesAfr J Respir Med2013849
- FaladeAGAyedeAIEpidemiology, aetiology and management of childhood acute community-acquired pneumonia in developing countries – a reviewAfr J Med Med Sci201140429330822783679
- BradleyJSByingtonCLShahSSThe management of community-acquired pneumonia in infants and children older than 3 months of age: clinical practice guidelines by the pediatric infectious diseases society and the infectious diseases society of AmericaClin Infect Dis2011537e25e7621880587
- OttoMStaphylococcus epidermidis – the ‘accidental’ pathogenNat Rev Microbiol2009755556719609257
- TaussigLLandauLPediatric Respiratory Medicine2nd edPhiladelphiaElsevier Health Sciences2008
- WebberSWilkinsonARLindsellDNeonatal pneumoniaArch Dis Child1990652072112107797
- LiZXiaoZLiZZhongQZhangYXuF116 cases of neonatal early-onset or late-onset sepsis: a single center retrospective analysis on pathogenic bacteria species distribution and antimicrobial susceptibilityInt J Clin Exp Med20136869369924040479
- MileaDAzmiSReginaldPVerpillatPFrancoisCA review of accessibility of administrative healthcare databases in the Asia-Pacific regionJ Mark Access Health Policy20153128076