
Abstract
Background
There are very few reports describing the development of gallstone disease after renal transplantation (GSDART) in Asia. The aim of this population-based study was to explore the prevalence, predictive factors, and outcomes of newly developed GSDART. The relationship between immunosuppressant and GSDART was also explored.
Patients and methods
Renal transplantation (RT) recipients were identified from the National Health Insurance Research Database of Taiwan during January 1998–December 2012. In total, 2,630 adult patients, who had neither been diagnosed with gallstone disease (GSD) nor undergone cholecystectomy, were included in this study. These patients underwent follow-up till the diagnosis of GSDART was established. Risk factors and post-RT immunosuppressant treatments were investigated and analyzed using Cox regression analysis. The cumulative mortality in patients with and without GSDART was also evaluated.
Results
The final dataset comprised 143 patients who developed GSDART and 2,487 patients who had not been diagnosed with GSDART during the follow-up period. The prevalence of GSDART was 5.4%. On performing univariate analysis, age (p=0.0276) and certain immunosuppressant administrations were identified as significant risk factors for GSDART. After adjusting for age, multivariable analysis showed that everolimus (adjusted hazard ratio 0.287, p=0.0013) was independently associated with the development of GSDART. The overall mortality rate (6.99%, p=0.0341) was significantly decreased in the GSDART group.
Conclusion
Increased age was the most consistent risk factor for GSD, and everolimus-based immunotherapy indicated a decreased incidence of GSDART in RT recipients. The long-term mortality rate was significantly decreased in patients with GSDART.
Introduction
Gallstone disease (GSD) is prevailing throughout the world. It is usually discovered incidentally by abdomen ultrasonography during a health survey. The prevalence of GSD in Taiwan has been reported ranging from 4.3% to 10.7%, which appears to be approximately half the rate found in the West.Citation1 According to previous studies, patients with GSD may remain asymptomatic; however, approximately one-third of victims developed symptoms, of which 80% presented as biliary colic.Citation2,Citation3 Complications associated with GSD, such as acute cholecystitis, pancreatitis, and cholangitis, were reported to be the major causes of gastrointestinal morbidity that led to hospital admission.Citation4
The pathogenesis of GSD has been deemed multifactorial. Former epidemiology studies have suggested that age, sex, obesity, diabetes mellitus, dyslipidemia, fatty liver, cirrhosis, hepatitis C virus infection, and chronic kidney disease are possible risk factors for the condition in the general population. Additionally, other constitutive elements were observed in these specific populations. In diabetic patients, impaired cholesterol metabolism due to insulin resistance was proposed as a possible mechanism for gallstone formation.Citation5 Meanwhile, abnormally regulated gastrointestinal mobility that results in gallbladder stasis has been the leading hypothesis of gallstone formation in patients with chronic renal failure.Citation6,Citation7
The development of cholelithiasis in renal transplantation (RT) recipients was known to be higher than in the general population. A previous studyCitation8 reported a prevalence of 20.7% among patients who received RT and developed gallstones thereafter during the 7.7-year period of follow-up. In another cohort consisting of 1,608 RT recipients, 267 (17%) patients were diagnosed with gallstones, 62% of whom developed them after undergoing RT.Citation9 It was believed that immunosuppressants prescribed following RT played an important role in this phenomenon.Citation10,Citation11 Meanwhile, immunosuppressed patients with GSD seemed to exhibit a significant morbidity and mortality during a flare up of the disease and the consequent emergent cholecystectomy. Ultrasound screening for GSD or prophylactic cholecystectomy before RT was suggestedCitation12 and raised wide discussions over a period of time.Citation9,Citation13,Citation14
The prevalence of cholelithiasis has varied depending on the region of the world. However, reports describing the development of GSD after renal transplantation (GSDART) in Asia are scarce.Citation15 Therefore, to identify independent risk factors and to elucidate the effect of GSD in patients undergoing RT, we conducted a retrospective population-based study using RT recipients from the Taiwanese National Health Insurance (NHI) database and investigated the prevalence, predictive factors, and outcomes of newly developed GSDART.
Patients and methods
Data sources
This retrospective population-based cohort study was evaluated and approved by Taiwan’s National Health Insurance Research Database (NHIRD) research committee and the institutional review board of Chang Gung Memorial Hospital. Taiwan’s NHI is a universal and mandatory health insurance program that was launched in 1995. This medical benefit program provides comprehensive coverage for health services, including ambulatory care, hospital services, and prescription drugs. Computerized data are compiled and encrypted by the National Health Research Institute (NHRI), which are made available for research purposes without disclosing identifiable patient data. This study was conducted using ambulatory claims and inpatient claims with beneficiaries aged 20 years or older from 1998 to 2012.
Patient selection
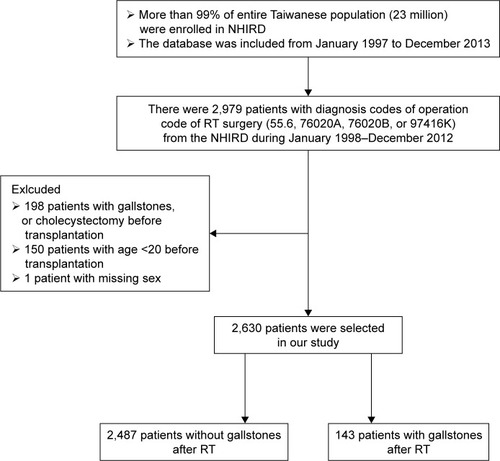
shows the flowchart of how the study population was selected. RT recipients were identified from the NHIRD using the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) code 55.6, 76020A, 76020B, or 97416K from January 1998, when RT was first included in the health insurance system in Taiwan, to December 2012. During this time, 2,979 patients who received RT were registered in the NHIRD. Of these, we excluded 198 patients who had been diagnosed with GSD (ICD-9-CM 574) or had undergone cholecystectomy (ICD-9 -CM 51.22 or 51.23) prior to RT surgery, another 150 patients who were younger than 20 years at the time of receiving RT, and one patient whose sex was not disclosed. The final study cohort consisted of 2,630 RT recipients ().
Figure 1 Study design and flow chart of patient selection.
Covariates and end points
Preoperative medical comorbidities were included when the corresponding diagnosis appearing in the medical record existed for more than three times in the outpatient department or once in the inpatient department. All diagnoses were verified using the ICD-9-CM codes. The comorbidities (ICD-9-CM) investigated in our study cohort included hypertension (401–405), diabetes mellitus (249, 250), hyperlipidemia (272), gout (274), obesity (278), peptic ulcer (531, 532, 533), fatty liver (571.0, 571.8), liver cirrhosis (571.2, 571.5, 571.6), chronic hepatitis (070, 571, 573.3, A347), hepatitis B (070.2, 070.3, V0261, V0269), hepatitis C (070.41, 070.44, 070.51, 070.54, 070.7, V0262), inflammatory bowel disease (555, 556, 557.0), cerebrovascular disease (433–438), coronary heart disease (410–414, A279), chronic obstructive pulmonary disease (490, 491, 495, 496), and hemolytic anemia (282–283).
All patients in the study cohort were followed up from the index day of RT surgery till the date when the diagnosis of GSDART was established. GSDART was identified using ICD-9-CM code 574 with at least one presentation in ambulatory visits or hospitalization claims. Mortality was defined as detection of insurance death codes or the termination of inclusion in the NHI program.
Measurements
The primary outcome parameter was the prevalence of GSDART and the independent risk factors for GSDART. In addition to previously identified epidemic risk factors, post-RT immunosuppressant administration was also investigated. The complications associated with GSDART and subsequent surgeries to treat GSD were described. The cumulative mortality in patients with and without GSDART was evaluated during the follow-up periods of 1, 3, 5, 10, and 16 years.
Statistical analysis
Between-group differences in the distribution of demographic data and coexisting medical diseases were compared using independent Student’s t-test, chi-square test, or Fisher’s exact test, whenever appropriate. To identify independent risk factors for GSDART, multivariable Cox regression analysis was adopted adjusting for significant covariates. Hazard ratios (HRs) with 95% confidence intervals (CIs) were calculated for the identified relevant factors. All analyses were performed using SAS software (version 9.3; SAS Institute Inc., Cary, NC, USA) with a two-tailed p-value <0.05 being assumed to indicate statistical significance.
Results
Study population and baseline characteristics
The study population comprised 143 patients who developed GSDART and 2,487 patients who had not been diagnosed with GSDART during the follow-up period. Relevant demographic data and clinical characteristics are shown in . Patients with GSDART were significantly older in age (p=0.0276) than patients without GSDART. However, there were no differences between these two groups in sex and the presence of comorbidities, including diabetes mellitus, hyperlipidemia, and cirrhosis, which were previously proposed to be clinical risk factors for GSD.
Table 1 General demographics and clinical characteristics of the RT recipients in the study
Prevalence of new-onset cholelithiasis after RT
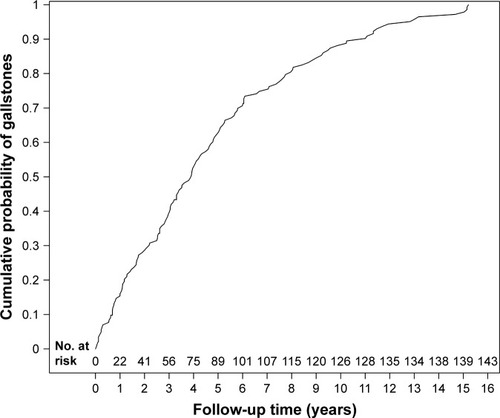
A total of 143 patients with new-onset cholelithiasis were diagnosed after RT surgery during the study period. The prevalence of newly developed GSD in recipients after RT was 5.4% during the overall 16-year follow-up period. Among patients with GSDART, 50% of patients developed GSD within 4 years following RT surgery. The cumulative rate of GSDART during the 16-year follow-up is shown in .
Figure 2 Cumulative prevalence of GSDART.
Abbreviations: GSDART, gallstone disease after renal transplantation; GSD, gallstone disease; No, number; RT, renal transplantation.
Immunosuppressants associated with new-onset cholelithiasis after RT
Six common immunosuppressants were analyzed and are listed in . Compared to the patient group without GSDART, patients who developed GSDART were more likely to take cyclosporine (p=0.0198) and azathioprine (p=0.0142). On the contrary, tacrolimus (p=0.0261) and everolimus (p<0.0001) were significantly less used in the group with GSDART. After adjusting for age, multivariate Cox regression analysis showed that everolimus (adjusted HR 0.287, p=0.0013) was independently associated with a diminishing hazard of developing new-onset cholelithiasis after RT surgery ().
Table 2 Immunosuppressant use in RT recipients with or without GSDART
Table 3 Multivariable Cox regression analysis of immunosuppressant use for GSDART
Adverse events of new-onset cholelithiasis after RT
In all, 27 (18.88%) of 143 patients who developed new-onset cholelithiasis after RT experienced acute cholecystitis as a major complication. Other complications associated with GSDART included biliary pancreatitis occurring in 12 (8.39%) patients and acute cholangitis occurring in 11 (7.69%) patients. Subsequent cholecystectomy was performed in 44 (30.77%) patients with GSDART, of whom 33 (24.48%) patients underwent elective cholecystectomy and nine (6.29%) patients underwent nonelective cholecystectomy. There were eight (5.59%) patients with GSDART who underwent endoscopic retrograde cholangiopancreatography (ERCP). The details of the aforementioned clinical variables are listed in .
Table 4 Adverse events of RT recipients with GSDART (n=143)
Mortality rate of new-onset cholelithiasis after RT
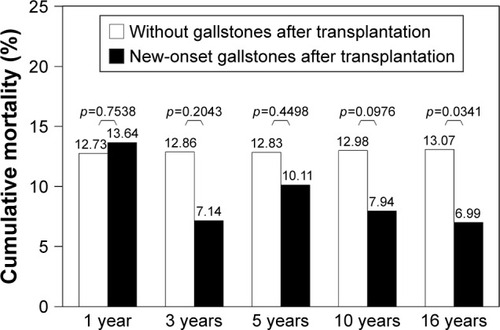
shows the trend of cumulative mortality rates at the indicated years of follow-up. Probability of death after diagnosis of GSDART was 13.64% in the first year, which lowered to 7.14% in the third year and 6.99% in the sixteenth year of follow-up. In contrast, the probability of death in patients who had not been diagnosed with GSDART was maintained (12.73% during the first year and 13.07% during the last year of follow-up). The overall mortality rate (6.99%, p=0.0341) was significantly decreased in patients with GSDART.
Figure 3 Long-term mortality rates.
Abbreviations: RT, renal transplantation; GSDART, gallstone disease after renal transplantation.
Discussion
The prevalence of GSDART in this study population was 5.3%, which lies within the lower range of the previously reported data in other populations in Taiwan.Citation1,Citation16,Citation17 Notably, the prevalence varied from the different subjects and methods adopted. One prospective ultrasonographic study of GSD conducted in a Chinese population enrolled subjects who exhibited gallbladder stones upon ultrasonography, or cholecystectomy for gallstones, in the GSD group. This study, after excluding cases with mixed gallstones and polyps, found that the overall prevalence of GSD was 10.7%.Citation16 Compared to prior studies, our study focused on subjects with newly developed GSD as we excluded RT recipients who had been diagnosed with GSD and/or had undergone cholecystectomy before RT surgery. The advantage is that once our study population was traced from the index day of RT surgery, data were not influenced by preexisting GSD. However, since we did not consider the recurrence rate of GSD, the prevalence of GSD may have been lower in our study. In addition, our GSD group, which was determined using the ICD-9-CM code 574, included patients with gallstones that caused symptoms or were detected using abdomen ultrasonography, while those with silent gallbladder stones would not be identified.
The risk factors for GSD found in the RT population appeared to be different from those in other populations. The main risk factors for GSD reported in community studies included older age of both sexes, hepatitis C virus infection, and fatty liver.Citation1,Citation16,Citation17 Other hospital-based studies found that increasing age, chronic kidney disease, high body mass index, metabolic syndrome, and cirrhosis were significantly related to GSD.Citation18,Citation19 However, in our cohort study of RT recipients, age and the use of certain immunosuppressants were associated with the occurrence of GSDART. No associations were found in comorbidities and metabolic profiles, which was consistent with a population-based study on kidney transplantation in Finland.Citation9
Immunosuppressant use has been proposed as an important risk factor for gallstone formation in the context of transplantation surgeries.Citation11 In particular, cyclosporine use was associated with the development of cholelithiasis in transplantation recipients. Alberu et al found that RT recipients who had used cyclosporine for more than 2 years exhibited an increased prevalence of gallstones (odds ratio 6.1, p=0.046).Citation10 Although the specific mechanism for lithogenesis of cyclosporine use has not been definitively elucidated, human and animal studies have suggested that cyclosporine’s metabolism in liver and predominant excretion via biliary secretion, impaired biliary excretion of biliary salts, thereby resulting in cholestasis.Citation20,Citation21 Tacrolimus, which, like cyclosporine, is a calcineurin phosphatase inhibitor (CNI), was found to increase the risk of gallstone formation in transplantation recipients. However, it was reported that tacrolimus increased bile secretion with little influence on bile flow in a rat model.Citation22,Citation23 In a heart transplantation study, Stief et al found that female patients seemingly benefited from a tacrolimus-based treatment as the occurrence of gallstones was rare.Citation11
In our study, the univariate analysis in shows consistent findings with previous studies that previously documented when cyclosporine and tacrolimus were used. The common use of azathioprine in combination with cyclosporine may account for the observation that azathioprine use increased the incidence of GSDART. However, after adjusting for age (the major risk factor for GSD), only everolimus use was shown to be independently associated with and protective against the occurrence of GSDART. Since CNIs may potentially result in serious side effects, such as nephrotoxicity and neurotoxicity,Citation24,Citation25 diminishing or even eliminating CNI use has become the focus of further optimization of immunosuppressive therapy in RT. Everolimus, a mammalian target of the rapamycin inhibitor (mTORi), is 100-fold more potent than cyclosporine and it binds to the identical intracellular immunophilin as tacrolimus but exhibits a divergent mode of action in comparison to CNIs. The side effects of everolimus are also different from those of CNIs.Citation26 Furthermore, everolimus may improve renal function and reduce the occurrence of malignancy, which makes it an attractive alternative to CNIs for maintenance therapy after RT.Citation27 The use of everolimus with either a reduced or eliminated dose of CNIs in RT recipients might partly account for the decreased incidence of GSDART. However, as the other mTORi, sirolimus, did not show advantage in reducing the incidence of GSDART in our study, the possibility that a direct effect of anti-cholestasis comes from everolimus cannot be ruled out.
Because of this immunosuppressive therapy, complications associated with GSD can be severe and the diagnosis can be delayed during the posttransplantation period.Citation14 In our study, there were 27 (18.88%) patients with GSDART whose cases became complicated with acute cholecystitis, of whom nine (6.29%) underwent nonelective cholecystectomy. In a prior study,Citation9 among 165 patients with GSDART, there were 13 (8%) patients who required emergent surgery due to biliary complications. This outcome was comparable to our study. However, the overall cumulative mortality rate was significantly decreased in the GSDART group in our study. Although there has been controversy as to whether GSD should be screened for or treated prior to transplantation, we agree that the expectant managementCitation28 for GSDART based on symptoms, without precedent screening or prophylactic cholecystectomy, is safe for RT recipients.
Limitations
Our large retrospective population-based study has several limitations that warrant consideration. The NHIRD is a secondary database and, therefore, does not include actual medical measurements, such as physical examination findings, laboratory data, or ultrasound imaging reports. However, given the nature of the NHIRD, we did not have access to the actual medical measurements mentioned. The discrepancies in consideration of GSD risk factors among previous hospital- and community-based studies may possibly be due to various study designs and settings. Additionally, considering the previous diagnosis of GSD could adhere to the patients permanently, we did not include the RT recipients with previous history of GSD nor subsequently analyze the precipitating factors for recurrence of GSD in patients undergoing RT surgery.
Apart from detection of insurance death codes, we enlisted patients who terminated the NHI program as definition of mortality. According to the regulations, there are three possible situations, including death, disappearance for ≥6 months, and loss of the qualification of residency in Taiwan, when the insured people terminate the program. Despite this, patients who received RT surgery were cautiously tracked in the documentation of catastrophic illness, and very few patients who were still living would forgo the beneficial social assistance because of the expensive medical expenditure.
As there were numerous recommended immunosuppressant regimens with various doses initiated after RT surgery, it was impossible for us to discuss the influence of each combination of immunosuppressants on lithogenesis in RT recipients. Thus, we adopted the form of an immunosuppressant-based treatment to describe the major action of the indicated immunosuppressant. Unlike the maintenance therapy, the course of induction therapy is usually short (~1 week), which is considered to have little impact on the long-term development of GSDART, and thus, we did not incorporate the induction therapy into analysis. However, future randomized controlled trials are needed to prove if everolimus can directly decrease the effect of cholestasis in RT recipients.
Conclusion
The prevalence of GSDART was 5.4% in Taiwan, with increasing age being the most consistent risk factor for GSD. Immunosuppressive therapy with everolimus-based treatment indicated a decreased incidence of GSDART in RT recipients, and further prospective clinical studies are suggested to prove the effect of everolimus on newly developed cholestasis in recipients of RT. Because of no increased risks of adverse outcomes observed in this study, the expectant management for GSDART is agreed to be safe for patients referred for RT surgery.
Disclosure
The authors report no conflicts of interest in this work.
References
- ChenCHHuangMHYangJCPrevalence and risk factors of gallstone disease in an adult population of Taiwan: an epidemiological surveyJ Gastroenterol Hepatol200621111737174316984599
- AhmedACheungRCKeeffeEBManagement of gallstones and their complicationsAm Fam Physician2000616167316801687168810750875
- HuangJChangCHWangJLNationwide epidemiological study of severe gallstone disease in TaiwanBMC Gastroenterol20099637219698126
- BeckinghamIJABC of diseases of liver, pancreas, and biliary system. Gallstone diseaseBMJ2001322919411154626
- BiddingerSBHaasJTYuBBHepatic insulin resistance directly promotes formation of cholesterol gallstonesNat Med200814777878218587407
- PauletzkiJAlthausRHollJSackmannMPaumgartnerGGallbladder emptying and gallstone formation: a prospective study on gallstone recurrenceGastroenterology199611137657718780583
- GladziwaUWagnerSKockRMannHSieberthHGSonographic evaluation of gallbladder motility in patients with end-stage renal disease on haemodialysisNephrol Dial Transplant1992788408431325618
- van PetersenASvan der PijlHWRingersJLemkesHHde FijterHWMascleeAAGallstone formation after pancreas and/or kidney transplantation: an analysis of risk factorsClin Transplant200721565165817845641
- SarkioSSalmelaKKyllonenLRosliakovaMHonkanenEHalmeLComplications of gallstone disease in kidney transplantation patientsNephrol Dial Transplant200722388689017205965
- AlberuJGaticaMCachafeiro-VilarMAsymptomatic gallstones and duration of cyclosporine use in kidney transplant recipientsRev Invest Clin200153539640011795104
- StiefJStempfleHUGotzbergerMBiliary disease in heart transplanted patients: a comparison between cyclosporine A versus tacrolimus-based immunosuppressionEur J Med Res20091420620919541577
- European Expert Group on Renal TransplantationEuropean best practice guidelines for renal transplantation (part 1)Nephrol Dial Transplant200015suppl 7185
- KaoLSKuhrCSFlumDRShould cholecystectomy be performed for asymptomatic cholelithiasis in transplant patients?J Am Coll Surg200319730231212892816
- MekaMPotdarSBenottiPHartleJESenkowskiCRole of ultrasound screening for gallbladder disease in pretransplant patientsAm Surg200874983283318807672
- ParkSHHahmJSSeongSSIncidence of gallbladder stones in renal transplant recipientsKorean J Gastroenterol200444424615266132
- ChenCYLuCLHuangYSAge is one of the risk factors in developing gallstone disease in TaiwanAge Ageing19982744374419883999
- LaiSWNgKCRisk factors for gallstone disease in a hospital-based studySouth Med J200295121419142312597310
- LaiS-WLiaoK-FLaiH-CChouC-YChengK-CLaiY-MThe prevalence of gallbladder stones is higher among patients with chronic kidney disease in TaiwanMedicine2009881465119352299
- ChenJYHsuCTLiuJHTungTHClinical predictors of incident gallstone disease in a Chinese population in Taipei, TaiwanBMC Gastroenterol2014148324775330
- KadmonMKlunemannCBohmeMInhibition by cyclosporin A of adenosine triphosphate-dependent transport from the hepatocyte into bileGastroenterology19931045150715147683296
- ChanussotFBotta-FridlundDLechene de la PortePEffects of cyclosporine and corticosteroids on bile secretion in the ratTransplantation19925422262311496534
- MizutaKKobayashiEUchidaHFujimuraAKawarasakiHHashizumeKInfluence of tacrolimus on bile acid and lipid composition in continuously drained bile using a rat model. Comparative study with cyclosporineTranspl Int199912531632210551996
- MizutaKKobayashiEUchidaHHishikawaSKawarasakiHIncrease of bile acid production by tacrolimus in the rat liverTransplant Proc20033543743812591477
- AlmeidaCSilveiraMde AraújoVSafety of immunosuppressive drugs used as maintenance therapy in kidney transplantation: a systematic review and meta-analysisPharmaceuticals (Basel)20136101170119424275847
- NankivellBJP’NgCHO’ConnellPJChapmanJRCalcineurin inhibitor nephrotoxicity through the lens of longitudinal histologyTransplantation20161001723173127306529
- ZazaGTomeiPRiaPGranataSBoschieroLLupoASystemic and nonrenal adverse effects occurring in renal transplant patients treated with mTOR inhibitorsClin Dev Immunol2013201340328024151517
- LimWHErisJKanellisJA systematic review of conversion from calcineurin inhibitor to mammalian target of rapamycin inhibitors for maintenance immunosuppression in kidney transplant recipientsAm J Transplant20141492106211925088685
- TakeyamaHSinananMNFishbeinDPAldeaGSVerrierEDSalernoCTExpectant management is safe for cholelithiasis after heart transplantJ Heart Lung Transplant200625553954316678032