
Abstract
Background
A long-axis in-plane (LA-IP) approach and a short-axis out-of-plane (SA-OOP) approach are the two main approaches used in ultrasound (US)-guided vascular catheterization. However, the efficacy and safety of these approaches remain controversial. Therefore, we performed this meta-analysis to compare the two techniques in vascular catheterization.
Materials and methods
Relevant studies were searched in PubMed, Embase, and the Cochrane Library databases from database inception until August 2017. Randomized controlled trials comparing a long-axis approach with a short-axis approach for US-guided vascular cannulation were selected. The RevMan software was used to analyze the results, and trial sequential analysis (TSA) was further applied to determine whether the currently available evidence was sufficient and conclusive.
Results
Eleven studies met the inclusion criteria. Overall, 1,210 patients were included. The total success rate was similar between the SA-OOP and LA-IP approaches for US-guided vascular catheterization (risk ratio [RR], 1.01; 95% CI, 0.99–1.04; P=0.35; I2=48%). In the radial artery (RA; RR, 1.00; 95% CI, 0.96–1.05; P=0.88; I2=49%) and internal jugular vein (IJV; RR, 1.00; 95% CI, 0.98–1.02; P=0.99; I2=0%) subgroups, the total success rate was also similar and was confirmed by the TSA. For populations with subclavian vein (SCV) and axillary vein catheterization, the SA-OOP approach showed a benefit for first-attempt success rate. No significant differences in first-attempt success rate, cannulation times, or complications were found between the two approaches.
Conclusion
Despite a similar total success rate between the SA-OOP approach and the LA-IP approach when used for RA and IJV catheterization (as confirmed by TSA), further robust well-designed trials are warranted to evaluate other outcomes. There is insufficient evidence to definitively state that the SA-OOP approach was superior to the LA-IP approach when used for SCV and axillary vein catheterization. High-quality trials are needed to confirm or refute this finding.
Background
Ultrasound (US)-guided vascular cannulation has become more popular in recent years, and US is a proven tool to increase the success rate and decrease complications in a wide variety of vascular catheterization procedures.Citation1 Numerous meta-analysesCitation2–Citation7 have demonstrated the advantage of US-guided vascular catheterization over a blind landmark approach. However, there is a controversy regarding which approach is preferable for the US probe, ie, the short-axis out-of-plane (SA-OOP) approach or the long-axis in-plane (LA-IP) approach. Each approach has distinct advantages and disadvantages that may either increase or decrease complications.Citation8 In the SA-OOP approach, the relationships of the target vessel to the adjacent vessels are visualized, but the needle tip may not be continuously visualized during catheter placement. In the LA-IP approach, the needle path including the tip can be continuously visualized during catheterization; however, the relationship of the target vessel to adjacent vessels may be lost.Citation9 A previous meta-analysis of five studies showed that there is insufficient evidence to definitively determine which approach is superior in patients undergoing US-guided vascular catheterization.Citation10 Several randomized controlled trials (RCTs) on this topic have been published recently. Therefore, we performed this updated meta-analysis of RCTs to compare the efficacy and safety of these two techniques and further applied trial sequential analysis (TSA) to determine whether the currently available evidence was sufficient and conclusive. This in turn can provide more reliable evidence for clinical practice.
Materials and methods
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA statement) guidelines were used to perform this meta-analysis.Citation11 Ethical approval was not required.
Search strategy and study selection
A search of the PubMed (US National Library of Medicine, Bethesda, MD, USA), Embase, and Cochrane Central Register of Controlled Trials databases was conducted from database inception to August 2017. Specific search strategies were developed for each database using exploded Medical Subject Headings and the appropriate corresponding keywords including “ultrasound,” “ultrasonography,” “ultrasonic” AND “catheterization,” “cannulation,” “catheter,” “catheters,” “insertion” AND “long axis,” “short axis,” “in plane,” “out of plane,” “longitudinal,” “transverse” AND “RCTs.” In addition, the reference lists of the screened full-text studies were searched to identify other potentially eligible trials. Searches were performed without language restrictions. A further search by manually reviewing conference proceedings and the references of review articles was performed.
The inclusion criteria were as follows: 1) population: adult patients requiring vascular catheterization; 2) comparison: the study compared LA-IP vs SA-OOP techniques for US-guided vascular catheterization; 3) outcome measure: the total success rate was reported; and 4) study design: RCTs.
Data extraction and outcome measurement
Two investigators (CL and ZM) independently performed the study selection. When data were missing or incomplete, the original authors were contacted by written correspondence for clarification. Disagreements between the two investigators were resolved by consensus or adjudicated by a third investigator (FZ). The dynamic needle tip positioning (DNTP) technique was classified as the SA-OOP approach. One standard form was used for data collection, which included the following information: first author, year of publication, patient population, the number of patients, age of patients, total success rate, first-attempt success rate, cannulation time, number of attempts, experience of the operators, puncture site, and type of US equipment. The primary outcome was the total success rate, and secondary outcomes included the first-attempt success rate, cannulation time, and the number of attempts.
Risk of bias assessment
We assessed the internal validity of included trials using the Cochrane Collaboration Risk of Bias tool.Citation12 The criteria in the tool included a description of the random sequence generation, allocation concealment, blinding of outcome assessment, incomplete outcome data, selective reporting, and other bias. Criteria were individually scored as high, low, or unclear risk of bias.
Statistical analysis
The statistical analysis was performed using RevMan software (version 5.3; Cochrane Collaboration, Copenhagen, Denmark) for outcome measurements. The results of the risk ratio (RR) for dichotomous outcomes or the mean difference (MD) for continuous data were expressed as means and 95% CIs. A random-effects model was used regardless of heterogeneity, which was estimated using the I2 statistic. A value of I2>50% indicated significant heterogeneity.Citation13 Potential sources of heterogeneity were identified by sensitivity analyses. We further conducted subgroup analyses according to the puncture site. Publication bias was assessed using the Begg and Egger tests. P<0.05 was considered to indicate a statistically significant difference. The sample mean and SD were estimated according to the sample size, median, range, and/or interquartile range.Citation14
TSA
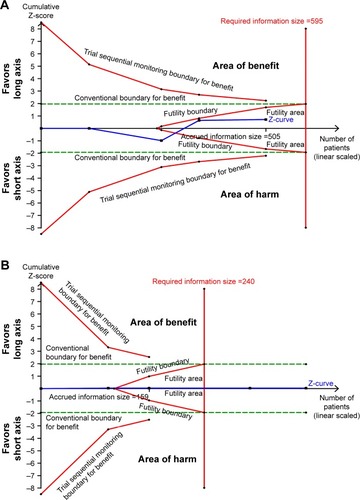
An updated meta-analysis with new studies may result in false positive results; thus, to decrease the risk of type I errors, the TSA was used. This method can determine whether the present evidence is reliable and conclusive.Citation15 When the cumulative Z-curve crosses the trial sequential monitoring boundary or enters the futility area, a sufficient level of evidence for the anticipated intervention effect may have been reached, and no further trials are needed. If the Z-curve does not cross any of the boundaries and the required information size (RIS) has not been reached, evidence to reach a conclusion is insufficient, and more trials are needed to confirm the results. For this TSA, we estimated the RIS using α=0.05 (two sided), β=0.10 (power 90%), the control event proportions calculated from the long-axis group, and a relative risk reduction of 10% in outcomes. TSA was conducted using TSA Version 0.9 Beta (www.ctu.dk/tsa).Citation16
Results
Study enrolment and characteristics
A total of 348 potentially relevant studies were collected, of which 334 studies were excluded based on titles, abstracts, and duplicate studies. Three articles were excluded because the article type was a letter or meta-analysis. Ultimately, 11 studiesCitation17–Citation27 fulfilled the inclusion criteria for the meta-analysis (). The study characteristics are summarized in . These studies were published between 2011 and 2017, and a total of 1,210 patients were included. The sample size of the studies ranged from 40 to 190 subjects. Baseline characteristics were similar between the two groups. All of the operators had experience in US-guided vascular catheterization. All studies reported the total success rate, and various complications were reported among these studies. The details for the risk of bias tool are shown in . No study fulfilled all criteria for a low risk of bias. A randomized sequence was adequately generated in all studies. Due to the nature of the studies, it was impossible to perform the study blinded. No potential publication bias was observed for primary outcomes (data not shown).
Figure 1 Flow chart of the study selection process.
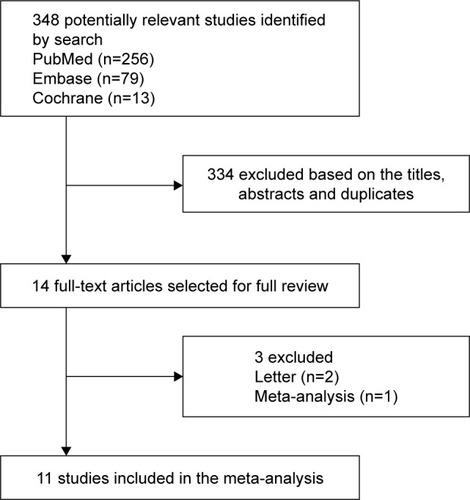
Figure 2 Assessment for risk of bias.
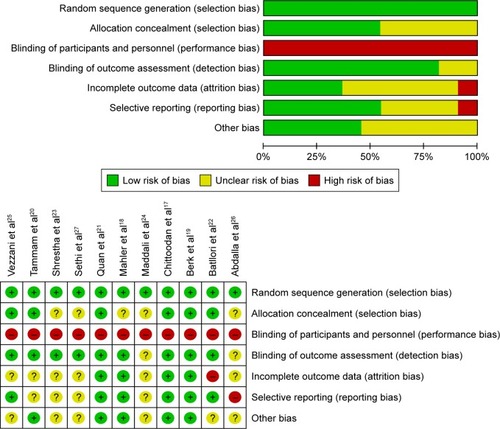
Table 1 Characteristics of the 11 included trials
Primary outcome
Total success rate
All studies investigated the total success rate of both the SA-OOP and LA-IP approaches for US-guided vascular catheterization. No significant difference was observed between the two groups (RR, 1.01; 95% CI, 0.99–1.04; P=0.35; I2=48%; ). Subgroup analyses were performed to investigate the source of heterogeneity. In the radial artery (RA) subgroup,Citation19,Citation21,Citation26,Citation27 the total success rate was no different between the SA-OOP and LA-IP groups (RR, 1.00; 95% CI, 0.96–1.05; P=0.88; I2=49%; ), and the TSA confirmed this result (the cumulative Z-curve crossed the futility boundary and entered the futility area; ). In the internal jugular vein (IJV) subgroup,Citation17,Citation20,Citation22,Citation23 the total success rate was also no different between the SA-OOP and LA-IP groups (RR, 1.00; 95% CI, 0.98–1.02; P=0.99; I2=0%; ) and the TSA also confirmed the result (the cumulative Z-curve crossed the futility boundary and entered the futility area; ). Only one studyCitation25 was included in the subclavian vein (SCV) subgroup, and the results show that the SA-OOP approach was more efficacious than the LA-IP approach in increasing the total success rate (RR, 1.23; 95% CI, 1.10–1.38; P<0.01; ).
Figure 3 Forest plot of total success rate.
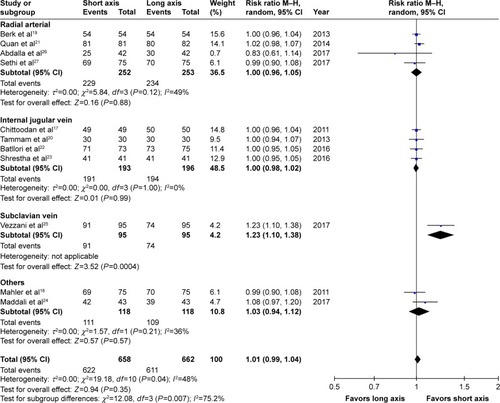
Figure 4 TSA result.
Abbreviations: DL, DerSimonian–Laird; IJV, internal jugular vein; M–H, Mantel–Haenszel; RA, radial artery; TSA, trial sequential analysis.
Secondary outcomes
First-attempt success rate
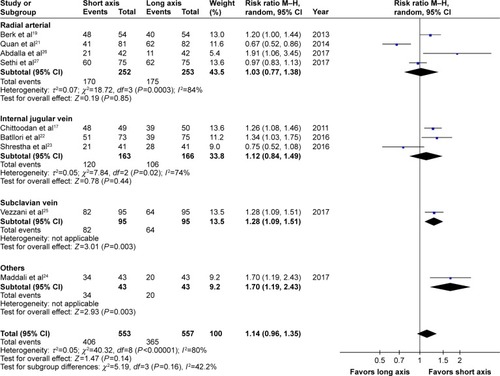
Nine studiesCitation17,Citation19,Citation21–Citation27 reported the first-attempt success rate. There was no significant difference between the LA-IP approach group and the SA-OOP approach group (RR, 1.14; 95% CI, 0.96–1.35, P=0.14, I2=80%; ). Due to remarkable heterogeneity, preset subgroup analyses were performed for the populations with RA catheterization (RR, 1.03; 95% CI, 0.77–1.38; P=0.85, I2=84%; ) and IJV catheterization (RR, 1.12; 95% CI, 0.84–1.49; P=0.33; I2=74%; ). No significant differences were observed. For populations with SCV catheterizationCitation25 and axillary vein catheterization,Citation24 the SA-OOP approach showed a benefit.
Figure 5 Forest plot of the first attempt success rate.
Other secondary outcomes are summarized in , including cannulation times, the number of attempts, complications of hematoma, and arterial puncture. The cannulation times of the two approaches used in the US-guided RA and IJV catheterization were similar. The number of attempts may be reduced when the SA-OOP approach is used in US-guided IJV catheterization and the LA-IP approach is used in US-guided RA catheterization. No significant differences were observed when comparing the complications of hematoma and arterial puncture between the two approaches.
Table 2 Secondary outcomes
Discussion
The key findings of this updated meta-analysis are as follows. 1) The total success rate was similar between the SA-OOP approach and LA-IP approach when used for RA and IJV catheterization, as confirmed by TSA. The SA-OOP approach showed a benefit when used for SCV catheterization; however, further RCTs are needed to confirm this. 2) The first-attempt success rate was also similar between the two approaches when used for US-guided RA or IJV catheterization. Whether the SA-OOP approach has an advantage in increasing the first-attempt success rate when used for SCV and axillary vein catheterization also requires further studies to confirm or refute this finding. 3) The number of attempts may be reduced when the SA-OOP approach is used in US-guided IJV catheterization and when the LA-IP approach is used in US-guided RA catheterization. 4) No significant differences in cannulation times or complications were found between the two approaches.
There are several differences between our meta-analysis and a previous meta-analysis.Citation10 First, this meta-analysis included an additional six studies.Citation22–Citation27 Thus, this updated meta-analysis represents the latest and most comprehensive study. Second, TSA was further applied to better establish sufficient and conclusive evidence. Third, we also analyzed the difference between the two approaches when used in different vessels.
In this meta-analysis, the total success rate was similar when the two approaches were used for US-guided RA and IJV catheterization and was confirmed by TSA. Moreover, more studies are needed to further evaluate whether the complications, first-attempt success rate, and cannulation times are different between the two approaches. A studyCitation25 included in this meta-analysis showed that the SA-OOP approach may increase the total success rate when used for SCV catheterization; however, this led to controversy.Citation28 High-quality studies are needed to confirm or refute this finding.
One studyCitation26 included in this meta-analysis reported that the oblique approach for US-guided RA catheterization may replace the two classic approaches due to its superior success rate, higher first-attempt success, and shorter time consumed for catheterization with higher operator satisfaction after the procedure. Confirmation of this requires further research. Another studyCitation22 in this meta-analysis compared three transducer orientation approaches for US-guided IJV catheterization and found that the oblique-axis (OAX) approach showed a higher first-needle pass success rate than LA-IP approach and a lower mechanical complications rate than the SA-OOP approach. Although more clinical studies are needed, this new approach may be superior in reducing complications related to IJV catheterization.
US-guidance for vascular catheterization is a user-dependent technology, and it is necessary to use medical simulators to train novice US users before they practice on patients. However, there are some discrepancies between the medical simulator result and the patient result. For example, one studyCitation29 evaluated the two approaches used in SCV catheterization in a human torso mannequin and found that the LA-IP view for SCV catheterization was more efficient with a decreased time to cannulation and fewer redirections. The simulators could not reflect the actual circumstances of the patients, and they lacked the nerves and arteries from soft tissue that commonly complicate US-guided vascular catheterization.Citation30 Hence, whether the benefit obtained from the medical simulators can be proven in live patients is unknown. Therefore, to provide more reliable evidence for clinical practice, more high-quality, anatomically accurate, vascular phantoms and standardized performance procedures are needed for US training.Citation31 Furthermore, when using the medical simulator to train novice US users, we should carefully consider the discrepancy between the medical simulator and the patient to improve clinical practice.
This meta-analysis has several potential limitations. First, considerable heterogeneity was observed between the included studies with respect to blood vessel type, operator experience, US equipment, and outcome definition, which could have influenced the results; second, due to the limited data, it is difficult to perform more subgroup or sensitivity analyses. Third, double blinding was not performed due to the features of the trials, which may result in performance and detection bias.
Conclusion
A similar total success rate between the SA-OOP approach and the LA-IP approach for RA and IJV catheterization was confirmed by TSA. However, further robust and well-designed trials are warranted to evaluate other outcomes. There is insufficient evidence to definitively state that the SA-OOP approach was better than the LA-IP approach when used for SCV and axillary vein catheterization. High-quality trials are needed to confirm or refute this finding.
Data sharing statement
The authors confirm that all data underlying the findings are fully available without restriction. All relevant data are within the paper.
Acknowledgments
This work was not supported by any funding.
Disclosure
The authors report no conflicts of interest in this work.
References
- MooreCLUltrasound first, second, and last for vascular accessJ Ultrasound Med20143371135114224958398
- RandolphAGCookDJGonzalesCAPribbleCGUltrasound guidance for placement of central venous catheters: a meta-analysis of the literatureCrit Care Med19962412205320588968276
- HindDCalvertNMcWilliamsRUltrasonic locating devices for central venous cannulation: meta-analysisBMJ2003327741136112919984
- GuWJTieHTLiuJCZengXTEfficacy of ultrasound-guided radial artery catheterization: a systematic review and meta-analysis of randomized controlled trialsCrit Care2014183R9324887241
- GaoYBYanJHGaoFQPanLWangXZLvCJEffects of ultrasound-guided radial artery catheterization: an updated meta-analysisAm J Emerg Med2015331505525453476
- LaluMMFayadAAhmedOUltrasound-guided subclavian vein catheterization: a systematic review and meta-analysisCrit Care Med20154371498150725803646
- StolzLAStolzUHoweCFarrellIJAdhikariSUltrasound-guided peripheral venous access: a meta-analysis and systematic reviewJ Vasc Access201516432132625656255
- EricksonCSLiaoMMHaukoosJSUltrasound-guided small vessel cannulation: long-axis approach is equivalent to short-axis in novice sonographers experienced with landmark-based cannulationWest J Emerg Med201415782483025493126
- DilisioRMittnachtAJThe “medial-oblique” approach to ultrasound-guided central venous cannulation – maximize the view, minimize the riskJ Cardiothorac Vasc Anesth201226698298422683157
- GaoYBYanJHMaJMEffects of long axis in-plane vs short axis out-of-plane techniques during ultrasound-guided vascular accessAm J Emerg Med201634577878326830218
- MoherDLiberatiATetzlaffJAltmanDGGroup PPreferred reporting items for systematic reviews and meta-analyses: the PRISMA statementInt J Surg20108533634120171303
- HigginsJPAltmanDGGotzschePCThe Cochrane collaboration’s tool for assessing risk of bias in randomised trialsBMJ2011343d592822008217
- HigginsJPThompsonSGDeeksJJAltmanDGMeasuring inconsistency in meta-analysesBMJ2003327741455756012958120
- WanXWangWLiuJTongTEstimating the sample mean and standard deviation from the sample size, median, range and/or interquartile rangeBMC Med Res Methodol20141413525524443
- LiuCMaoZKangHHuJZhouFRegional citrate versus heparin anticoagulation for continuous renal replacement therapy in critically ill patients: a meta-analysis with trial sequential analysis of randomized controlled trialsCrit Care201620114427176622
- ThorlundKEngstrømJWetterslevJBrokJImbergerGGluudC webpage on the InternetUser Manual for Trial Sequential Analysis (TSA)Copenhagen, DenmarkCopenhagen Trial Unit, Centre for Clinical Intervention Research20111115 Available from: www.ctu.dk/tsaAccessed May 3, 2017
- ChittoodanSBreenDO’DonnellBDIohomGLong versus short axis ultrasound guided approach for internal jugular vein cannulation: a prospective randomised controlled trialMed Ultrason2011131212521390339
- MahlerSAWangHLesterCSkinnerJArnoldTCConradSAShort-vs long-axis approach to ultrasound-guided peripheral intravenous access: a prospective randomized studyAm J Emerg Med20112991194119720951527
- BerkDGurkanYKusAUlugolHSolakMTokerKUltrasound-guided radial arterial cannulation: long axis/in-plane versus short axis/out-of-plane approaches?J Clin Monit Comput201327331932423417581
- TammamTFEl-ShafeyEMTammamHFUltrasound-guided internal jugular vein access: comparison between short axis and long axis techniquesSaudi J Kidney Dis Transpl201324470771323816718
- QuanZTianMChiPCaoYLiXPengKModified short-axis out-of-plane ultrasound versus conventional long-axis in-plane ultrasound to guide radial artery cannulation: a randomized controlled trialAnesth Analg2014119116316924806143
- BatlloriMUrraMUriarteERandomized comparison of three transducer orientation approaches for ultrasound guided internal jugular venous cannulationBr J Anaesth2016116337037626705350
- ShresthaGSGurungAKoiralaSComparison between long- and short-axis techniques for ultrasound-guided cannulation of internal jugular veinAnn Card Anaesth201619228829227052071
- MaddaliMMAroraNRChatterjeeNUltrasound guided out-of-plane versus in-plane transpectoral left axillary vein cannulationJ Cardiothorac Vasc Anesth20173151707171228416391
- VezzaniAMancaTBrusascoCA randomized clinical trial of ultrasound-guided infra-clavicular cannulation of the subclavian vein in cardiac surgical patients: short-axis versus long-axis approachIntensive Care Med201743111594160128289815
- AbdallaUEElmaadaweyAKandeelAOblique approach for ultrasound-guided radial artery catheterization vs transverse and longitudinal approaches, a randomized trialJ Clin Anesth2017369810128183585
- SethiSMaitraSSainiVSamraTMalhotraSKComparison of short-axis out-of-plane versus long-axis in-plane ultrasound-guided radial arterial cannulation in adult patients: a randomized controlled trialJ Anesth2017311899427761661
- PredaGBigeNBonseyMDiscussion on “a randomized clinical trial of ultrasound-guided infra-clavicular cannulation of the subclavian vein in cardiac surgical patients: short-axis versus long-axis approach”Intensive Care Med20174381169117028509948
- VogelJAHaukoosJSEricksonCLIs long-axis view superior to short-axis view in ultrasound-guided central venous catheterization?Crit Care Med201543483283925517477
- ResnickJRCydulkaRJonesRComparison of two transducers for ultrasound-guided vascular access in long axisJ Emerg Med200733327327617976555
- AIUM practice guideline for the use of ultrasound to guide vascular access proceduresJ Ultrasound Med201332119121523269727