
Abstract
Esophageal bronchogenic cysts are extremely rare. Here we report a case of massive upper digestive tract hematoma and bronchogenic cyst mimicking aortic dissection that was safely removed without esophagectomy. A 30-year-old man was referred to our hospital for the treatment of a mediastinal cystic tumor located in the submucosa of the distal esophagus. His chief complaints were dysphagia > 1 week and severe persistent upper abdominal pain mimicking aortic dissection with constant vomiting for 1 day after gastroscopy examination. The serum level of carbohydrate antigen (CA)199 was > 1,000 U/mL and CA125 was 4,816 U/mL. Hemoglobin levels decreased from 122 g/L to 85 g/L in 5 days. Imaging examinations detected a huge hematoma of the gastric wall. Preoperative diagnosis was difficult. Although the pain indicated a possible aortic dissection, the abnormal levels of tumor biomarkers suggested malignancy. The patient underwent left thoracotomy. The cyst showed an exophytic lesion connected to the esophageal wall at the level of the gastroesophageal junction. Muddy brown contents were obtained by aspiration of the mass intraoperatively. Because enucleation could not be performed, esophageal myotomy in the distal esophagus and partial resection of the cyst were selected. Histopathological examination indicated a bronchogenic cyst of the esophagus. At a follow-up visit 3 months later, the patient had no signs of disease recurrence or any complaints. Postoperative tumor biomarkers returned to normal range. The present report summarizes the clinical details of the case and reviews the literature in order to improve the accuracy of diagnosis.
Introduction
Bronchogenic cysts (BCs) are rare congenital malformations arising during the development of the ventral foregut, and they are most commonly found in the middle and superior mediastinum.Citation1 They are mainly located near the tracheobronchial tree or lung parenchyma with or without a well-defined wall.Citation2,Citation3 Although these lesions are often benign, BCs can also cause symptoms such as chest pain, cough, dysphagia, and dyspnea due to compression of the surrounding structures.Citation4 As the majority of cysts are within the mediastinum, paraesophageal BCs are frequently reported. Intramural esophageal BCs are reported occasionally.Citation5 Typically, BCs are negative for carbohydrate antigen (CA)199 and CA125. Hematoma of the gastric wall has not been previously reported in any BC patients. We herein describe an extremely rare case of intramural esophageal BC and hematoma of the gastric wall with positive expressions of CA199 and CA125. Surgical resection is generally recommended in cases showing relevant complications and changes of the esophageal cyst. Complete excision of the entire cyst is necessary to avoid recurrence. This report describes the feasibility of thoracotomy for removing esophageal cysts and hematoma of the gastric wall associated with violent persistent abdominal pain mimicking aortic dissection. Although enucleation is a standard treatment for small-sized cysts, the technique has not been adopted for large cysts with severe inflammatory adhesions. To our best knowledge, no similar case has been previously reported. The patient signed an informed consent preoperatively.
Case report
A 30-year-old man was referred to our hospital for the treatment of a mediastinal cyst located in the submucosa of the distal esophagus in November 2016. His chief complaints were dysphagia > 1 week and severe persistent upper abdominal pain mimicking aortic dissection with constant vomiting for 1 day after gastroscopic examination. The patient was unable to take in solids or liquids. The patient denied any chest symptoms, such as coughing and chest pain. His past medical history was unremarkable.
Physical examination did not reveal any obvious abnormal signs, and preoperative laboratory data were within the normal range, with the exception of the tumor markers CA199 and CA125. The serum level of CA199 was > 1,000 U/mL (normal range:<37 U/mL), and CA125 was 4,816 U/mL (normal range: <37 U/mL), while carcinoembryonic antigen (normal range: <5 μg/L) and squamous cell carcinoma antigen (normal range: <1.5 μg/L) were within the normal range.
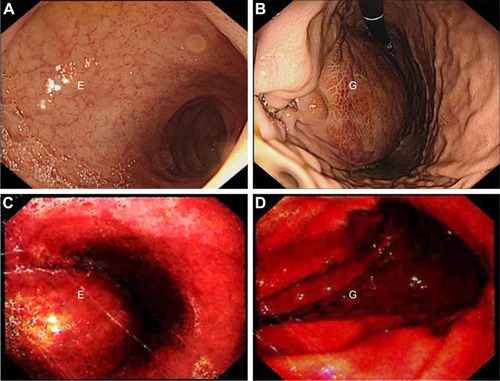
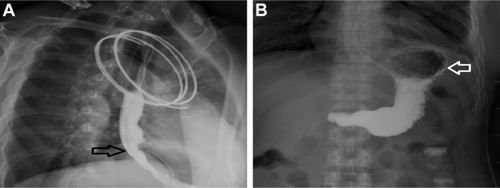
The thoracic computed tomography (CT) scan revealed a well-defined low-density mass originating from the distal esophageal wall, measuring 67 × 51 × 60 mm with a CT value of 28 HU. The day before admission, the gastroscopy examination showed a smooth surface causing partial obstruction of the lower esophagus and a normal stomach fundus. An abdominal CT revealed a normal shape of the stomach (). Five days later, transverse contrast-enhanced chest CT showed a sharply defined mass measuring 47 × 70 × 85 mm with a CT value of 31 HU. Transverse contrast-enhanced abdominal CT showed a huge lump in the stomach wall (). The distal esophageal lumen was almost closed. After admission, a mass with a smooth surface causing partial obstruction of the lower esophagus (labelled E on ) and stomach fundus (labelled G on ) was observed by gastroscopy (). Laboratory data showed that hemoglobin (HGB) was 85 g/L (normal range: 120–160 g/L) compared with 122 g/L 5 days before.
Figure 1 Preoperative imaging diagnoses. (A) Chest CT scan at the day before admission shows a smooth cystic tumor measuring 67 × 51 × 60 mm (white arrow). CT value was 28 HU. The esophagus was compressed by the cystic tumor. (B) An abdominal CT at the day before admission revealed a normal shape of the stomach (white arrow). (C) Transverse contrast-enhanced chest CT at 5 days after admission showed the sharply defined mass measuring 47 × 70 × 85 mm (white arrow). CT value was 31 HU. (D) Transverse contrast-enhanced abdominal CT at 5 days after admission showed a huge contusion of the stomach wall (black arrow).
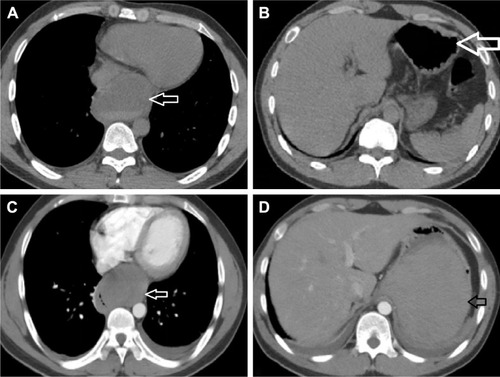
Figure 2 Gastroscopy images. (A, B) After admission, gastroscopy showed a mass with a smooth surface causing a partial obstruction of the lower esophagus and stomach fundus. (C, D) The day before admission, gastroscopy showed a mass with a smooth surface causing partial obstruction of the lower esophagus and a normal stomach fundus.
Given these findings and evaluation, an esophageal cyst with malignancy was suspected and the patient underwent surgery. Preoperatively, we chose among surgical procedures including enucleation, complete resection of the cyst, esophageal reconstruction, and radical resection of esophageal cancer according to the characteristics of the cyst and the hematoma of the gastric wall.
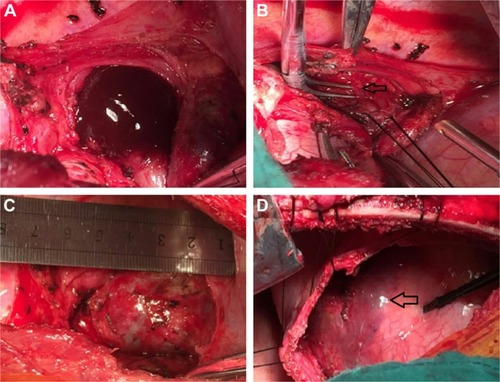
In the operation room, under general anesthesia, the left lung was collapsed using a double-lumen endotracheal tube while the patient was in a right lateral position. A left thoracotomy revealing a mass in the distal esophagus was performed. The mass was large and had severely adhered to the adjacent tissues, especially the diaphragm. The muddy brown contents were observed by aspiration of the mass. Because complete resection of the cyst was difficult, enucleation could not be performed. Esophageal myotomy in the distal esophagus was selected to preserve esophageal dynamic function and mucosal integrity. Partial resection of the cyst was performed simultaneously. A longitudinal 5-cm esophageal myotomy was performed, and a 40 × 70 × 80 mm unilocular cystic mass was identified. The cyst showed an exophytic swelling appearance and dense adhesions were observed between the cystic wall and the esophageal mucosa (). After separating the adhesions around the distal esophagus, the cyst was decompressed and intracystic fluid was suctioned to dissect the adjacent tissues easily and safely. The residual cyst wall was treated with electrocautery and iodine to prevent recurrence. The absence of mucosal perforation or esophagostenosis was confirmed intraoperatively by injecting water into the esophagus and stomach. The proper muscle layer of the esophagus was recovered approximately. Opening of the diaphragm and removal of the hematoma were achieved by making a small incision in the surface of the gastric muscle. A chest drainage tube was inserted through the eighth intercostal space.
Figure 3 Intraoperative images. (A) Brown fluid was observed in the bronchogenic cyst after dissection of the cystic wall. (B) The nutrient artery (arrow) supplying the cyst was revealed distinctly. (C) The shape of the bronchogenic cyst was revealed. (D) Because of the gastric hematoma, a violet surface (arrow) was observed after incision of the diaphragm.
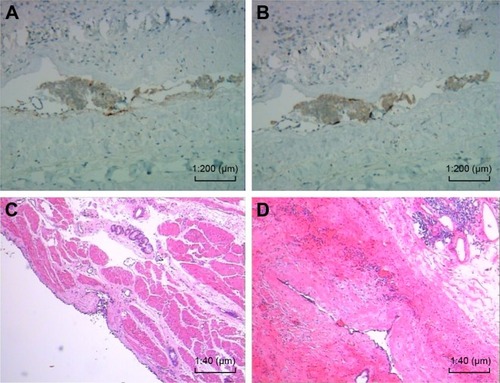
Histopathologically, the wall of the cyst was lined with ciliated columnar epithelium. The wall also contained cartilage and bronchogenic glands. We also detected positive expression of CA199 and CA125 in cyst sections by immunohistochemical staining (). A bronchial cyst of the esophagus was finally confirmed based on these findings ().
Figure 4 Immunohistochemical and histopathological examination of the cyst sections. (A) Positive expression of CA199, original magnification ×200. (B) Positive expression of CA125, original magnification ×200. (C, D) The cystic wall was lined with ciliated columnar epithelium. The wall also contained cartilage and bronchogenic glands (H&E stained, original magnification ×40).
The postoperative process was favorable. A control esophagogram (barium meal) performed on postoperative day 30 showed neither stenosis nor leakage (), and oral fluid intake was resumed. The patient was discharged tolerating liquids and soft food uneventfully. The serum CA199 and CA125 levels decreased to normal levels after the operation. The patient is presently doing well at 3 months after surgery. No recurrence or dysphagia was noted during the follow-up period.
Figure 5 (A) A control esophagogram showed that the esophagus (black arrow) had neither stenosis nor leakage. (B) The shape and function of the stomach (white arrow) were normal.
Patient consent
Written informed consent was obtained from the patient for publication of clinical data including all images in this case report.
Discussion
BCs are congenital malformations arising from abnormal budding of the ventral foregut during the early stage of gestation. Considering the time of separation from the primary airways, BCs may present as mediastinal cysts approaching the tracheobronchial tree or as pulmonary cysts within the lung parenchyma.Citation6–Citation9 Over 20 cases have been reported in the literature since 2000 and are summarized in .Citation2,Citation4,Citation10–Citation34 The most common thoracic location of BCs is the middle mediastinum close to the carina, whereas the paratracheal, hilar, and intraparenchymal locations are rare. BCs have been reported in the posterior and anterior mediastinum, and occasionally in the diaphragm and intrapericardial or intracardiac regions.Citation15,Citation19 BCs are also located in extrathoracic regions such as cervical, skin, and retroperitoneum. Paraesophageal BCs are uncommon and difficult to differentiate from esophageal duplications. However, esophageal BCs are extremely rare, and their morbidity remains unknown because most patients are asymptomatic.Citation35 Most often, these cysts are discovered at an early age, between 20 and 40 years, and they are rarely diagnosed in elderly patients or in the pediatric population.Citation6–Citation9 The present 30-year old patient is in his prime of life and his symptoms was consistent with his common age group of patients. Symptoms can be found incidentally or occasionally, and they vary according to the age of presentation, and the size of the cyst and its location. The symptoms are usually caused by compression of the surrounding structures or by complications related to the cyst.Citation31 The most frequent symptoms are pain, cough, fever, and dyspnea; in rare cases, the cyst is complicated by a superior vena cava obstruction, pneumothorax, dysphagia, severe hemoptysis, or malignancies.Citation6–Citation9 Although BCs in the mediastinum are generally asymptomatic, the gastroscopy performed in our case irritated the cyst, resulting in intracapsular hemorrhage and hematoma of the gastric wall. The esophageal and gastric cavity almost disappeared, leading to dysphagia.
Table 1 Summary of published cases with periesophageal or intramural esophageal bronchogenic cysts
The correct preoperative diagnosis is very difficult due to the rarity of the disease and the lack of specific imaging methods. Different laboratory tests and imaging techniques can be used for preoperative diagnosis, and some differential diagnoses need to be considered, such as aortic aneurysm, recurrent tuberculosis, tuberculoma, aspergilloma, hydatid disease, fungal disease, benign or malignant tumor, paraesophageal cyst, cystic nervous tumor, pulmonary sequestration, congenital cystic adenomatoid malformation, esophageal leiomyoma, pleural fibroma, lymphadenopathy, and intracystic hemorrhage.Citation24 However, the characteristics of the mass need to be defined by histopathological examination. Intracystic hemorrhage can be detected by decreased HGB levels, as in the present case.
The characteristics of the mass can be assessed by measuring tumor marker levels. CA199 is the primary marker of choice for pancreatic, colorectal, and hepatocellular cancers, and it is also elevated in pancreatitis, cirrhosis, and obstructive disease of the bile duct.Citation36 CA125 is the marker of choice for ovarian cancer.Citation37 High levels of tumor markers such as CA199 and CA125 are rarely observed in patients with esophageal cysts. Reports of high levels of both CA199 and CA125 are extremely rare.Citation16,Citation33,Citation38 In the present case, abnormal levels of CA199 and CA125 were also detected in the serum and the cyst sections, and the elevated CA199 and CA125 levels decreased to a normal range postoperatively. These findings suggested that the serum levels of CA199 and CA125 were partly correlated with epithelial cell secretion from the esophageal BC in our patient. Although all these cases have remarkably elevated CA199 and CA125 levels, only the present case has developed massive upper digestive tract hematoma, leading to severe, tearing pain in the abdomen. To our best knowledge, no similar cases have been previously reported.
Despite the use of several imaging techniques such as radiography, barium meal, CT scan, magnetic resonance imaging (MRI), endoscopic ultrasound (EUS), EUS-fine needle aspiration (EUS-FNA), and gastroscopy for the diagnosis of esophageal cysts, a definitive diagnosis remains difficult preoperatively. Mediastinal BCs usually present as non-specific middle or posterior mediastinal masses on chest radiographs. Barium meal can show a local exogenous mass in the esophagus, although it is difficult to discriminate esophageal cysts from other diseases. CT can reveal the location of a cyst and its relationship with surrounding tissues and it is superior to radiography. BCs typically manifest as spherical masses of either water or soft tissue attenuation. If BCs manifest as water attenuation masses in CT scans, they can be differentiated from other mediastinal masses such as lymphadenopathy or neoplasia. However, BCs are detected as soft tissue attenuation masses in CT scans; therefore, differentiation from solid lesions is difficult. If lesions located in the esophagus compress the esophageal lumen, precise definition of the outer wall of the esophagus remains difficult. Differences in CT values enable the characterization of different tissues. CT values vary from water density (0–20 HU) to high density (80–90 HU) according to the contents of the cyst, such as protein, calcium, and the presence of infection.Citation39 However, cysts cannot be distinguished from tumor parenchyma based only on CT values. MRI is more sensitive and more accurate than CT regarding location and diagnosis. St-Georges et al reported that the diagnostic accuracy rate of preoperative CT is 69.2%, whereas the diagnostic accuracy of MRI is 100%.Citation40 However, when a cyst is infected or contains protein or calcium, its density may be the same as that of a solid mass, which increases the diagnostic difficulty.Citation14,Citation41 EUS uses the esophagus as an acoustic medium to image the mediastinum layers. EUS has been proposed as a modality for the accurate diagnosis of esophageal cystic lesions. This technique identifies lesions of the esophagus and can distinguish between cystic and solid lesions by differentiating anechoic tissue from that containing dense hyperechoic debris in the intracystic space. EUS-FNA can provide a definitive diagnosis of mediastinal tumors; however, fluid cytology cannot be used to determine the origin of esophageal cysts. Furthermore, direct puncture of the cyst can induce infection, making the operation more difficult. Therefore, the universal application of EUS-FNA is not recommended for all BCs. In particular, the present case should not be recommended for EUS-FNA because of the probability of hemorrhage of the tumor. Gastroscopy is used to distinguish cysts from esophageal cancer by observing the integrity of the esophageal mucosa.
Surgical procedures such as video-assisted thoracoscopy (VATS), thoracotomy, and mediastinoscopy remain the standard treatment for esophageal BCs. A precise diagnosis is based on the surgical specimen, and even if patients are asymptomatic, precautions need to be taken against future complications such as infection, rupture, intracystic hemorrhage, and cancerization.Citation27,Citation42 Thoracoscopy is a mini-traumatic operation that is effective and as safe as open surgery. It can provide a good field of vision, allowing identification of both the vagal nerve and the phrenic nerve during dissection. In addition, the advantages of thoracoscopy include reducing postoperative pain, promoting patient recovery, and minimizing incisions. Thoracotomy is the conventional approach to remove an esophageal cyst, and it allows maintenance of the integrity of the esophageal mucosa. Despite certain disadvantages associated with postoperative recovery, thoracotomy would be preferred over thoracoscopy as the surgical approach for the present patient in case of potential intraoperative emergency because of the uncertainty of preoperative diagnosis.
Regardless of the preferred surgical approach, complete resection is necessary in cases of recurrence. However, if a cyst is severely adhered to vital tissues (such as the thoracic aorta or vena cava), complete resection is not possible and thoracoscopy can increase the surgical risk. Thoracotomy and total resection with de-epithelization may be a good option in these cases. The residual epithelial layer should be destroyed using toxic agents.Citation43 In the present case, the adhesion to the distal esophagus and a huge hematoma of the gastric wall were resolved using thoracotomy. This technique enabled not only a reduction of the risk of mucosal damage, but also the simultaneous removal of the hematoma. The integrity of the mucosa was preserved, which was confirmed by injecting water into esophagus and stomach. Close observation and timely postoperative care provided further confirmation of the lack of perforation or putrescence of the esophageal and gastric mucosa.
Conclusion
Esophageal BC mimicking aortic dissection is extremely rare. The preoperative diagnosis is complicated and the definite diagnosis is based on pathological examination. Surgical excision is the principal treatment for this disease. The rare case of massive upper digestive tract hematoma and BC mimicking aortic dissection was safely removed without esophagectomy. The procedure described had a favorable outcome and is worthy of reference. To the best of our knowledge, no similar case has ever been reported previously in the currently available literature.
Disclosure
The authors report no conflicts of interest in this work.
References
- ThallerPBlanchetCBadrMMesnageRLeboucqNMondainMCambonieGNeonatal respiratory distress syndrome revealing a cervical bronchogenic cyst: A case reportBMC Pediatr2015157226112048
- WangWNiYZhangLWA case report of para-esophageal bronchogenic cyst with esophageal communicationJ Cardiothorac Surg201279423013612
- CioffiUde SimoneMShould video-assisted surgery be the first-line approach for bronchogenic cysts?Asian Cardiovasc Thorac Ann2011193/428921885563
- VannucciJPecorielloRTassiVCeccarelliSPumaFGiant tho-racoabdominal esophageal bronchogenic cystDis Esophagus201326334022236421
- SudaKSueyoshiROkawadaMKogaHLaneGJYamatakaADoiTCompletely intramural bronchogenic cyst of the cervical esophagus in a neonatePediatr Surg Int20153168368726002606
- MaierHCBronchogenic cysts of the mediastinumAnn Surg1948127347650217859095
- LimaïemFAyadi-KaddourADjilaniHKilaniTEl MezniFPulmonary and mediastinal bronchogenic cysts: A clinicopathologic study of 33 casesLung20081861556118064522
- RibetMECopinMCGosselinBHBronchogenic cysts of the lungAnn Thorac Surg1996616163616408651761
- RibetMECopinMCGosselinBHBronchogenic cysts of the medi-astinumJ Thorac Cardiovasc Surg19951095100310107739231
- SashiyamaHMiyazakiSOkazakiYEsophageal bronchogenic cyst successfully excised by endoscopic mucosal resectionGastrointest Endosc200256114114512085056
- HallaniHEslickGDCoxMWyattJMLeeCHChest pain? CauseLancet2004363940745214962526
- WesterterpMvan den BergJGvan LanschotJJFockensPIntramural bronchogenic cysts mimicking solid tumorsEndoscopy200436121119112215578307
- MeloNPitmanMBRattnerDWBronchogenic cyst of the gastric fundus presenting as a gastrointestinal stromal tumorJ Laparoendosc Adv Surg Tech A200515216316515898909
- PagesONRubinSBaehrelBIntra-esophageal rupture of a broncho-genic cystInteract Cardiovasc Thorac Surg20054428728817670412
- KoSFHsiehMJLinJWHuangCCLiCCCheungYCNgSHBronchogenic cyst of the esophagus: Clinical and imaging features of seven casesClin Imaging200630530931416919550
- AkutsuYMatsubaraHHayashiHOkazumiSAokiTKozuTOchiaiTEndoscope-assisted thoracoscopic technique for esophageal bronchogenic cyst which presented elevated CA 125Dig Surg200623420921416874000
- ChuangKHHuangTWChengYLEsophageal bronchogenic cyst: A rare entityZ Gastroenterol200745995896017874358
- GroverMGuptaAWagnerDPOrringerMBHard to swallowAm J Med2007120121023102518060919
- TurkyilmazAErogluASubasiMFindikGIntramural esophageal bron-chogenic cysts: A review of the literatureDis Esophagus200720646146517958719
- EomDWKangGHKimHWRyuDSUnusual bronchopulmonary foregut malformation associated with pericardial defect: bronchogenic cyst communicating with tubular esophageal duplicationJ Korean Med Sci200722356456717596673
- KiralHTezelCSKosarAKelesMClinicopathologic demonstration of complex bronchopulmonary foregut malformationAnn Thorac Surg20088562114211618498835
- RubinSSanduSDurandEBaehrelBDiaphragmatic rupture during labour, two years after an intra-oesophageal rupture of a bronchogenic cyst treated by an omental wrappingInteract Cardiovasc Thorac Surg20099237437619423509
- Diaz NietoRNaranjo TorresAGómez AlvarezMIntraabdominal bronchogenic cystJ Gastrointest Surg201014475675819475460
- ChafikABenjellounAQassifHIntramural esophageal bron-chogenic cystsAsian Cardiovasc Thorac Ann2011191697121357324
- FernandezJLBauzaGMcAnenyDBMinimally invasive management of lesser sac bronchogenic cystJSLS201115457157422643521
- BarbetakisNAsteriouCKleontasAPapadopoulouFTsilikasCVideo-assisted thoracoscopic resection of a bronchogenic esophageal cystJ Minim Access Surg20117424925222022117
- GhobakhlouMFatemiSRDezfouliAATirgaryFZaliMRLong-term dysphagia due to bronchogenic cyst of the esophagusEndoscopy201244Suppl. 2E129E13022477181
- BallehaninnaUKShawJPBrichkovISubdiaphragmatic bronchogenic cyst at the gastroesophageal junction presenting with dysphagia: A case reportSurg Laparosc Endosc Percutan Tech2013234e170e17223917610
- TangXJiangBGongWEndoscopic submucosal tunnel dissection of a bronchogenic esophageal cystEndoscopy201446Suppl. 1E626E62725502273
- GouYWangYFangHXuXYuWZhangKYuYBronchogenic cyst in the hepatogastric ligament masquerading as an esophageal mesenchymal tumor: A case reportInt J Clin Exp Pathol2015811153071531126823885
- AltieriMSZhengRPryorADHeimannAAhnSTelemDAEsophageal bronchogenic cyst and review of the literatureSurg Endosc201529103010301525669636
- TrehanMSinglaSSinghJGargNMahajanAA rare case of intra-abdominal bronchogenic cyst – a case reportJ Clin Diagn Res2015911PD03PD04
- HanCLinRYuJA case report of esophageal bronchogenic cyst and review of the literature with an emphasis on endoscopic ultra-sonography appearanceMedicine (Baltimore)20169511e311126986156
- LinJSYuYRChiouEChumpitaziBPSchadyDBrandtMLIntramural esophageal bronchogenic cyst mimicking achalasia in a toddlerPediatr Surg Int201733111912327822780
- LiangJSYinGLZhangXMZhuSBDongYQIntramural esophageal bronchogenic cyst with wall hemorrhage results in acute esophageal obstruction: Report of two casesAm Surg2014801E27E2924401509
- SunLHLuLFuWHLiWDLiuTGastric bronchogenic cyst presenting as a gastrointestinal stromal tumorInt J Clin Exp Pathol2015810136061361226722583
- RandolphLKHopkinsMKHopkinsMPWasdahlDAHepatoid carcinoma of the ovary: A case report and review of the literatureGynecologic Oncol Rep2015136467
- GotoTMaeshimaAOyamadaYKatoREsophageal cyst producing CA19-9 and CA125Interact Cardiovasc Thorac Surg201010344845020008896
- ChangYCChenJSChangYLVideo-assisted thoracoscopic excision of intradiaphragmatic broncho genic cysts: Two casesJ Laparoendosc Adv Surg Tech A200616548949217004875
- St-GeorgesRDeslauriersJDuranceauAClinical spectrum of bronchogenic cysts of the mediastinum and lung in the adultAnn Thorac Surg19915216132069465
- LimLLHoKYGohPMPreoperative diagnosis of a paraesophageal bronchogenic cyst using endosonographyAnn Thorac Surg200273263363511845887
- HasegawaTMurayamaFEndoSSoharaYRecurrent bronchogenic cyst 15 years after incomplete excisionInteract Cardiovasc Thorac Surg20032468568717670158
- KosarATezelCOrkiAKiralHArmanBBronchogenic cysts of the lung: Report of 29 casesHeart Lung Circ200918321421819119078