
Abstract
Acute necrotizing encephalopathy following influenza infection is a rapidly progressing disease with high morbidity. Although the neurological disorder is sometimes reported in children, it is very rare in adults. We herein describe an adult with acute necrotizing encephalopathy captured on a series of brain magnetic resonance images. A 55-year-old man had fever and impaired consciousness. He was diagnosed with influenza A (H1N1). Brain magnetic resonance imaging revealed symmetrical lesions in the cerebellum and basal nucleus, showing typical acute necrotizing encephalopathy. Physicians should know that influenza-associated acute necrotizing encephalopathy can occur even in middle-aged adults.
Introduction
Although neurological manifestations in children with influenza A (H1N1) are reported, it is rare in adults.Citation1 Acute necrotizing encephalopathy, which is characterized by multifocal, symmetric brain lesions that affect the thalami bilaterally, is one of the features of influenza-associated encephalitis/encephalopathy.Citation2 During an epidemic of encephalitis/encephalopathy in Japan in 1998–1999, 121 of 148 (81.8%) patients were aged <5 years, and the disease was rare in those aged >10 years, with acute necrotizing encephalopathy occurring in 10% of all patients.Citation2 In a multicenter surveillance study of children and adults performed through the British Pediatric Neurology Surveillance Unit and British Neurological Surveillance Unit between February 2011 and February 2013, acute necrotizing encephalopathy was observed in 4 children and no adults among 25 patients (21 children and 4 adults) who had a neurological presentation.Citation1
Acute necrotizing encephalopathy is a rare central nervous system complication of influenza or other viral infections causing altered mental status often with seizures, which may be rapidly progressive and with a high mortality.Citation3,Citation4 The prognosis varies from complete recovery to death: the mortality rate is about 30% and <10% of patients recovered completely, and neurological sequelae were frequently seen in survivors.Citation4 Here, we describe an adult with acute necrotizing encephalopathy captured on a series of brain magnetic resonance imaging (MRI).
Case report
During the influenza season (February 2014), a 55-year-old man had fever of 39°C 4 hours before he presented to our hospital with impaired consciousness of Glasgow Coma Scale E4V4M5. His blood pressure was 66/42 mmHg. Physical examination did not reveal any other abnormal findings. Although impaired glucose tolerance was pointed out a few years ago, there was no other significant past medical history. There was no history of recent lower respiratory tract infection. The laboratory data were as follows: white blood cell count, 10,420/μL (reference level 3,500–9,500/μL); hemoglobin level 15.9 g/dL (13.0–16.5 g/dL); platelet count, 6.1×104/μL (15.0–35.0×104/μL), D-dimer, 13.70 μg/mL (<1.0 μg/mL); international normalized ratio of prothrombin time, 1.34 (0.85–1.13); activated partial thromboplastin time, 53.9 s (26.1–35.8 s); aspartate aminotransferase, 197 U/L (10–35 U/L); alanine aminotransferase, 123 U/L (7–42 U/L); lactase dehydrogenase, 348 U/L (120–240 U/L); γ-glutamyl transpeptidase, 643 U/L (5–60 U/L); total bilirubin, 4.8 mg/dL (0.3–1.2 mg/dL); ammonia, 3 μg/dL (12–66 μg/dL); total protein, 5.8 g/dL (6.5–8.0 g/dL); albumin, 3.2 g/dL (3.8–4.9 g/dL); creatinine 6.27 mg/dL (0.6–1.1 mg/dL); blood urea nitrogen, 41 mg/dL (8–22 mg/dL); creatinine phosphokinase, 1,039 U/L (54–324 U/L); blood glucose level, 155 mg/dL; hemoglobin A1c, 6.8% (≤6.2%); and C-reactive protein, 15.33 mg/dL (<0.3 mg/dL). Thus, multiple organ failure was suspected. He was diagnosed with influenza A by rapid antigen test using nasal swab and was treated with the antiviral drug peramivir (300 mg) once. Subsequently, influenza A H1N1 was confirmed by polymerase chain reaction using nasal secretion. Brain MRI revealed symmetrical lesions in the cerebellum () and basal nucleus, showing typical acute necrotizing encephalopathy.Citation5 Although he did not manifest a convulsion, his state of consciousness deteriorated 7 hours after the first MRI, which was consistent with the worsening MRI findings at that time (). Cerebrospinal fluid was not examined because his platelet count was decreased to 1.1×104/μL the day after next.
Figure 1 Brain magnetic resonance imaging revealed symmetrical lesions of cerebellum (left, diffusion-weighted imaging; center, apparent diffusion coefficient-map; right, fluid-attenuated inversion recovery) at diagnosis (A), 7 hours (B), and 28 days (C) after the onset of acute necrotizing encephalopathy.
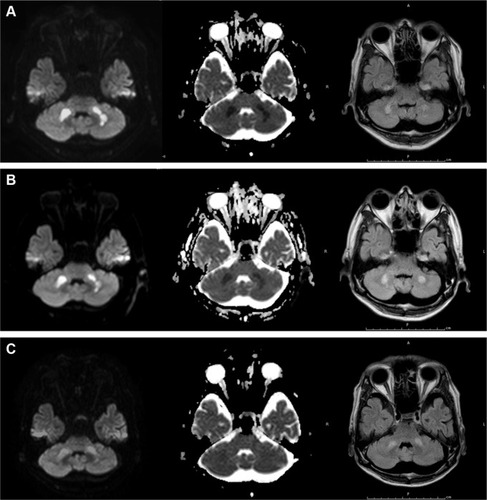
Intravenous hydration, vasopressor, gabexate mesylate, methylprednisolone (1 g/d, 3 days), and immunoglobulin (2.5 g/d, 3 days) were administered in particular. Mechanical ventilatory support and plasmapheresis, followed by continuous hemodiafiltration for acute renal failure, were also performed. On day 6 of his hospitalization, ventilator weaning was successfully done. He moved out of the intensive care unit on day 14. The treatment led to almost complete recovery, with slight disruption in daily life, and improved MRI findings 28 days after disease onset ().
Discussion
To the best of our knowledge, only one case of acute necrotizing encephalopathy in a patient aged >50 years was reported.Citation6 However, brain MRI was not performed in the patient. He was an 80-year-old man, whose past and social history included diabetes for a few years, cerebral infarction at the age of 52, and a smoking history of 40 years.Citation5 Brain MRI images of acute necrotizing encephalopathy in children have been reported.Citation6–Citation8 The brain MRI images in young adults with disease, such as a 23-year-old woman,Citation9 a 27-year-old man,Citation10 and a 27-year-old woman,Citation11 resembled those in children. The typical images showed multiple focal lesions of edematous necrosis which are symmetrically distributed in the bilateral thalami and other brain regions such as the putamina, cerebral and cerebellar deep white matter, and brainstem tegmentum.Citation3 Although acute necrotizing encephalopathy is usually lethal, the patient in our case fortunately recovered. Rates of mortality (31.8%) and disability (27.7%) in Japanese patients with acute necrotizing encephalopathy were found to be high.Citation2 Although the presence of hemorrhage and localized tissue loss on MRI would predict a poor prognosis,Citation4 there were no particular features in our case. In addition to the diagnosis by typical MRI, the prognosis could be predicted by serial MRI findings.
One might assume that the patient could have just acute encephalopathy, but not acute “necrotizing” encephalopathy. Actually, acute encephalopathy shows cytotoxic edema, producing high signal intensity on diffusion-weighted imaging asymmetrically.Citation12,Citation13 However, the MRI findings in the present case were compatible with those found in the previous cases of acute necrotizing encephalopathy, described earlier. Due to the decreased incidence of autopsies, the diagnosis of acute necrotizing encephalopathy was mainly based on characteristic neuroradiologic findings.Citation4 Finally, serial brain MRI scans showed that the images were correlated with his clinical course.
The pathogenesis of influenza-associated acute necrotizing encephalopathy remains unclear. Influenza virus has been rarely identified in cerebrospinal fluid.Citation13 It is hypothesized that the “cytokine storm” due to the systemic inflammation caused by influenza infection may be associated with the severe encephalopathy.Citation13 Thus, immune response rather than direct viral invasion seems to be pathogenesis of the disease. Intensive care, symptomatic treatment, and empirical treatment are usually performed in patients with acute necrotizing encephalopathy, and intravenous glucocorticoids, immunoglobulin, plasmapheresis, or therapeutic hypothermia have also been tried; however, a standard treatment has not been established.Citation4 We administered intravenous glucocorticoids and immunoglobulin and performed plasmapheresis. However, the usefulness of these remains unclear.
Conclusion
Physicians should know that influenza-associated acute necrotizing encephalopathy can occur even in middle-age adults and should be aware of the typical MRI findings of this disease.
Ethics approval and consent to participate
The authors’ institution does not require ethical approval for publication of a single case report. Written informed consent for publication of clinical details and images was obtained from the patient.
Author contributions
All authors contributed toward data analysis, drafting and critically revising the paper, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
- GoenkaAMichaelBDLedgerENeurological manifestations of influenza infection in children and adults: results of a National British Surveillance StudyClin Infect Dis20145877578424352349
- MorishimaTTogashiTYokotaSEncephalitis and encephalopathy associated with an influenza epidemic in JapanClin Infect Dis20023551251712173123
- MizuguchiMYamanouchiHIchiyamaTShiomiMAcute encephalopathy associated with influenza and other viral infectionsActa Neurol Scand20071154 Suppl455617362276
- WuXWuWPanWWuLLiuKZhangHLAcute necrotizing encephalopathy: an underrecognized clinicoradiologic disorderMediators Inflamm2015201579257825873770
- IshiiNMochizukiHMoriguchi-GotoSAn autopsy case of elderly-onset acute necrotizing encephalopathy secondary to influenzaJ Neurol Sci201535412913025982501
- ZengHQuinetSHuangWClinical and MRI features of neurological complications after influenza A (H1N1) infection in critically ill childrenPediatr Radiol2013431182118923567910
- LyonJBRemigioCMilliganTDelineCAcute necrotizing encephalopathy in a child with H1N1 influenza infectionPediatr Radiol20104020020520020117
- HaktanirAMR imaging in novel influenza A(H1N1)-associated meningoencephalitisAJNR Am J Neuroradiol20103139439520150309
- NarraRMandapalliAKamarajuSKAcute necrotizing encephalopathy in an adultJ Clin Imaging Sci201552025973284
- IijimaHWakasugiKAyabeMShojiHAbeTA case of adult influenza A virus-associated encephalitis: magnetic resonance imaging findingsJ Neuroimaging20021227327512116748
- LeeYJSmithDSRaoVAFatal H1N1-related acute necrotizing encephalopathy in an adultCase Rep Crit Care2011201156251624826323
- TokunagaYKiraRTakemotoMDiagnostic usefulness of diffusion-weighted magnetic resonance imaging in influenza-associated acute encephalopathy or encephalitisBrain Dev20002245145311102732
- AkinsPTBelkoJUyekiTMH1N1 encephalitis with malignant edema and review of neurologic complications from influenzaNeurocrit Care20101339640620811962