Abstract
Background
The data comparing daily versus intermittent iron supplementation during pregnancy remain controversial. This study was undertaken to compare the efficacy of daily versus two different intermittent iron supplementation regimes on hematologic markers and birth outcomes in nonanemic pregnant women.
Methods
Two hundred and ten women with singleton pregnancies, no known disease, and hemoglobin levels >11.0 g/dL were randomly assigned to one of three groups, ie, Group A consuming two iron supplementation tablets once weekly (100 mg iron per week, n = 70), Group B consuming one tablet twice weekly (100 mg iron per week, n = 70) and Group C, consuming one tablet daily (50 mg iron per day, n = 70). No additional micronutrients were supplied. Hemoglobin and serum ferritin levels were measured at 20, 28, and 38 weeks. Pregnancy and birth outcomes (pregnancy termination, method of delivery, birth weight, stillbirth) were analyzed.
Results
In total, 201 women completed the protocol. There was a significant difference in mean hemoglobin and ferritin levels in Group B at 38 weeks (P = 0.018 and P = 0.035, respectively) but this difference was not clinically significant (hemoglobin >12 g/dL, ferritin >19 μg/L). There was a significant increase in ferritin in Group C (P = 0.03) at 28 weeks. No significant difference was observed with respect to pregnancy or birth outcome across the groups. All regimens prevented the occurrence of hemoglobin <10.5 g/dL, but weekly supplementation was associated with development of a hemoglobin level <11.0 g/dL (risk ratio 0.044).
Conclusion
Twice-weekly supplementation is as effective as daily supplementation, and may represent an acceptable compromise in iron supplementation regimens for nonanemic pregnant women.
Introduction
Iron deficiency is considered to be the most prevalent nutrient deficiency in the world, and iron deficiency anemia is estimated to affect 1–2 billion people globally.Citation1 Groups demonstrating the highest prevalence of iron deficiency anemia are infants, children, and pregnant women.Citation2 More than 50% of pregnant women in developing countriesCitation3 and approximately 20% in industrialized countriesCitation4 suffer from iron deficiency.
During pregnancy, iron is a critical element for both the pregnant mother and the growing fetus,Citation5 and is essential to neurotransmitter synthesis and myelination of the central nervous system. Iron also functions as a cofactor for enzymes involved in brain development.Citation6 Fetal iron supply is provided by deflection of a significant proportion of maternal iron to the developing fetus.Citation7
Despite some controversy, anemia in pregnancy has been linked with preterm delivery and low birth weight,Citation8 and maternal iron deficiency in pregnancy has been linked with altered neurocognitive development of the infant.Citation3 Thus, determination of the potentially most effective approach towards prevention and accurate management of anemia in pregnancy represents a clinical problem with global impact.
Although the World Health Organization (WHO) published recommendations on the design of large-scale iron supplementation programs in 1989Citation9 to alleviate this nutritional disease, iron supplementation during pregnancy remains a controversial issue. The ultimate goal of providing iron supplementation to a healthy, nonanemic pregnant woman is to ensure sufficient iron storage in her body to provide effective cover for the increased physiologic need of iron during pregnancy, because the natural mechanisms of increasing iron intake, such as higher absorption of iron from the gastrointestinal tract, are not always adequate. Women with iron deficiency are particularly susceptible to iron deficiency anemia during pregnancy, because the demand for iron increases from 0.8 to ≤7.5 mg of absorbed iron per day.Citation10 Latent or overt iron deficiency will gradually progress to iron deficiency anemia, characterized by microcytosis and increased amounts of protoporphyrin IX in red blood cells,Citation4 which is linked with a risk of an unfavorable pregnancy outcome, as mentioned previously.
In the Islamic Republic of Iran, the prevalence of iron deficiency anemia in pregnant women varies between 2.4% and 27.8% with respect to specific regions,Citation11 and thus represents a severe public health issue. The current policy of the Iranian Ministry of Health is to examine pregnant women for anemia at 12–17 weeks’ gestation and to supply 30 mg/ day of iron as ferrous sulfate to each pregnant woman from gestational week 20 until three months after delivery.Citation11
However, discussion regarding the true desirability of daily iron supplements versus intermittent iron supplements has arisen in recent years. The reasons for initial consideration of other than daily iron supplementation regimens are based on the lack of effectiveness of daily iron intervention in developing countries,Citation12 indicated by low compliance with many daily supplementation programs,Citation12 insufficient supply of iron,Citation11 and insufficient coverage of at-risk populations.Citation12 More evidence-based theory behind intermittent iron supplementation reflects the original concept of mucosal block of iron absorption due to an increase in the proportion of iron that is stored in the enterocyte, and a decrease in transfer of iron to transferrin in the vascular pool,Citation13 confirmed decades later to some extent by in vivo studies in rats showing a rapid decline in the absorptive and iron retention capacities during daily iron administration compared with an intermittent regimen. Hence, daily iron supplementation may not be the most efficient approach towards maintaining or improving the iron status of a woman during pregnancy.Citation14,Citation15
This paper reports a randomized, unsupervised field study designed to evaluate the relative effectiveness of once-weekly, twice-weekly, and daily antenatal iron supplementation for maintaining safe hemoglobin and serum ferritin (indicator of iron reserves) levels during pregnancy and at delivery.
Subjects and methods
The study was conducted in North-West Iran in the urban regions of Urmia city. The study population was randomly drawn from pregnant women attending local public health care centers at seven prenatal health care clinics between September, 2007 and February, 2009. Thirty women were finally enrolled at each participating clinic. The women were invited to participate in the study during their first visit to the government antenatal clinic at 17–20 weeks and were informed by an assigned health care provider of its purpose, the procedures and tests entailed, and what data would be collected for analysis. Participants were free to withdraw from the study at any time without any disadvantage to themselves. Written informed consent was obtained from each literate woman and an improvised linear shaped signature in front of a witness was obtained on behalf of illiterate women who agreed to participate in the study. Before the start of the study, its protocol was approved by the University Ethics Committee and by the Faculty of Medicine. The protocol required participants to take the supplements on an assigned basis, to fill out forms about pill-taking and return these at each return clinic visit, and to have a 5 mL venipuncture for hemoglobin and ferritin concentration at 20, 28, and 38 weeks’ gestation. Women with previously demonstrated low hemoglobin levels or overt anemia were not eligible to participate. Exclusion criteria were hemoglobin <11 g/dL, noncompliance, intolerance of iron tablets or a physician’s recommendation to refrain from iron intake, previous consumption of iron-containing supplements, multiple pregnancy, thalassemia, chronic systemic disease, eclampsia or pre-eclampsia, more than five previous completed pregnancies, history of bleeding or surgery during previous pregnancy, pregnancy terminated before 36 weeks, and relocation to another area.
Sample size, allocation of group, and tablet intake
A total of 210 nonanemic pregnant women with a hemoglobin level >11.0 g/dL, set as a cutoff value for anemia based on the WHO definition,Citation16 were recruited at >17 and <20 weeks of gestation for participation in this study. The power of the study was 80%, and the level of significance was considered to be P < 0.05. The prevalence of anemia at delivery in the daily control group versus weekly group was reported to be 9% versus 45%, respectively, according to a literature review. The women were randomly assigned to receive two iron tablets once weekly (100 mg/dose, Group A), one tablet twice weekly (50 mg/dose, Group B), or once daily (50 mg/day) as ferrous sulfate. The weekly supplemented group received two 50 mg ferrous sulfate tablets on Friday, and the twice-weekly supplemented group received one 50 mg ferrous sulfate tablet on Monday and Wednesday. Therefore, both groups received the same total amount of elemental iron per week, ie, 100 mg. All women were instructed to take the tablets on an empty stomach before sleep.
Subsequently, at 28 weeks’ gestation, four women were excluded due to hemoglobin <11 g/dL, lack of compliance (n = 2, Groups A and B) or relocation to another area (n = 2, Group A). Two hundred and six women continued to participate in the study beyond 28 weeks. Data for the excluded women were not included in the final analysis.
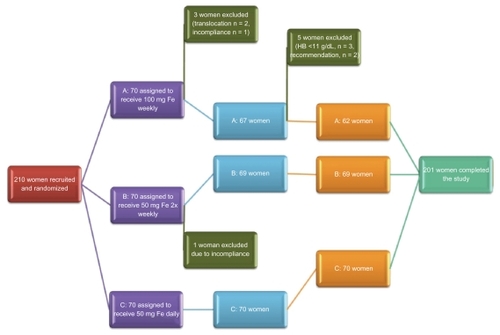
At 38 weeks, three women from Group A were excluded due to hemoglobin levels <11 g/dL and two women decided of their own volition to transfer to a daily supplementation regimen based on the recommendation of their private physician, in spite of having safe hemoglobin levels (12.8 g/dL and 11.7 g/dL). Two hundred and one women completed the study protocol and their data were analyzed. The study outline is summarized in .
Figure 1 Overview of clinical study.
Data on age, body weight, parity, and height were recorded at the time of study enrolment (). Body mass index was calculated according to the standard formula as weight in kilograms divided by the square of height in meters, and weight gain was assessed by the difference in weight at 20 and 38 weeks’ gestation. Parity was determined by self-reporting and calculated as the number of deliveries assigned to a particular group divided by total number of completed pregnancies reported by women in the group.
Table 1 Geometric mean (± standard deviation) of baseline characteristics of participating women at time of enrolment (≤20 weeks’ gestation) and delivery
Serum ferritin and hemoglobin levels
Participants were sent to a reference laboratory at assigned weeks of gestation according to the protocol to provide venous blood samples for assessment of hemoglobin and serum ferritin concentrations. Women with hemoglobin < 11 g/dL at or after 28 weeks’ gestation (n = 3, Group A) were excluded from the study and referred to a physician to be treated with daily supplementation of two 50 mg ferrous sulfate tablets until the end of their pregnancy, and this supplementation regimen was continued for three months after delivery. The remaining participants were followed until delivery and a blood sample was obtained according to the protocol at 38 weeks’ gestation. After delivery, data on infant outcome (birth weight and gestational age) were collected from the family medical file at the local health center and analyzed. Venous blood samples of 5 mL obtained at 20, 28, and 38 weeks’ gestation were analyzed for hemoglobin level by the antenatal clinic reference laboratory using an H1 automated counter (Technicon, Bayer, Tehran, Iran). At these times, a second tube of venous blood was collected for measurement of serum ferritin concentration and kept refrigerated until analysis. Samples for that assessment were analysed in the same laboratory using an immunoradiometric assay technique (Kavoshyar Ferritin IRMA [I125] kit, Kavoshyar Iran Co, Tehran, Iran).
Adherence to regimen and side effects
Overall adherence to the regime was calculated as the number of tablets women swallowed according to given forms, divided by the total number of tablets they should have received during supplementation, ie, number of weeks enrolled in the program multiplied by the number of tablets received in each group. Side effects were recorded at regular visits.
Medical record extraction
Birth weight and date of delivery were extracted by health care providers from the family file using standardized data entry forms for all women who completed the study protocol and who delivered at the local medical center at Koversusar Hospital, Urmia. Each women who delivers in a government center is given a form which she brings to the hospital and fills out after the birth before being discharged, which is then maintained in a family file.
Birth outcomes
Low birth weight was defined as <2500 g. Gestational age was determined either on the basis of a participant-reported estimate of the last menstrual period or by an ultrasound examination performed early in the pregnancy. Determination of preterm birth was based solely on duration of gestation, with deliveries that occurred at <37 completed weeks designated as preterm. Deliveries via cesarean section and stillbirths were noted.
Statistical analysis
An analysis of variance test was used to assess baseline characteristics across the groups. We conducted analyses on outcomes based on randomization of the study participants and compared the average measurements at the designated time points by randomization group. Kruskal-Wallis nonparametric analysis of variance was used for comparison of mean ferritin and hemoglobin levels across the groups. Unpaired t-tests were used to compare continuous outcomes between the randomization groups, and Chi-squared tests and post hoc tests, where appropriate, were used to compare differences in categorical outcomes. Risk ratios and 95% confidence intervals were estimated for comparisons between the supplementation groups for the outcomes of preterm delivery. Statistical significance was set at P < 0.05. The Statistical Package for Social Sciences for Windows version 16.0 (SPSS Inc, Chicago, IL) was used for all analyses.
Results
Characteristics of study sample and participation
A total of 210 women were initially invited to participate in the study and randomly assigned to one of three treatment groups, ie, 70 in Group A, 70 in Group B, and 70 in Group C. Of these, four (1.9%) were excluded at 28 weeks and five (2.38%) at 38 weeks due to detection of exclusion criteria, leading to a total dropout rate of 4.28%. Two hundred and one remaining subjects (95.72%; 62 in Group A, 69 in Group B, and 70 in Group C) completed the study protocol, and had blood samples taken at baseline and at all assigned time points after supplementation (). The participants were matched according to body mass index (P = 0.75), parity (P = 0.50), age (P = 0.21), baseline hemoglobin (P = 0.7), and ferritin levels (P = 0.37).
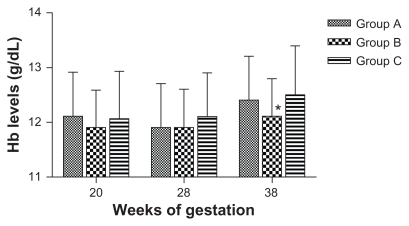
Figure 2 Geometric means of hemoglobin level.
Withdrawals from the study before 36 weeks’ gestation were due to relocation (n = 2, Group A) noncompliance (n = 2, Group A and Group B), and hemoglobin <11 g/dL at 38 weeks (n = 3, Group A) and were therefore excluded from the study and treated appropriately. Two women withdrew on the recommendation of their physician.
The baseline characteristics of the participating women by treatment group are shown in . The women did not differ in any of the physiologic study variables (body mass index, age, parity, weight gain), or initial hemoglobin or ferritin concentrations.
The mean age of the participating women was 25.5 ± 5.04 (range 19.7–30.7) years; 49.2% of the participants were aged 19–24 years, 27.7% were aged 25–29 years, and 23.1% were aged 30 years or older. More than 50% of participants (n = 104) were nulliparous at study entry. The average baseline hemoglobin and ferritin concentrations were 12.03 ± 0.79 g/dL and 14.16 ± 11.13 μg/L, respectively. The baseline range for hemoglobin concentration was 11.19–12.93 g/dL.
Iron status and relative effectiveness of iron supplementation regimens
summarizes the data comparing mean hemoglobin and serum ferritin levels for women who completed the study as measured at designated time points. and show time point-correlated geometric mean values for hemoglobin. No significant difference was found between the treatment groups for hemoglobin levels at 28 weeks. At 38 weeks, the mean hemoglobin level in Group B was significantly lower than in Group A and Group C (P = 0.018), but the difference was of no clinical significance. The mean serum ferritin level increased significantly in Group C at 28 weeks’ gestation (P = 0.03). When comparing the final levels at 38 weeks, a significant difference was observed between Group B and the other two groups in this iron status indicator (P = 0.035). This difference was also of marginal clinical significance (19.9 μg/L in Group B).
Figure 3 Geometric means of ferritin level.
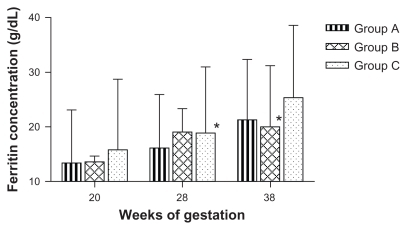
Table 2 Effect of once-weekly, twice-weekly, and daily iron supplementation on hemoglobin and ferritin levels in nonanemic pregnant women
Birth outcome
An overall comparison of average birth parameters for the three treatment groups is summarized in . Infants born to women who were assigned to the different treatment groups showed no significant difference in average birth weight (P = 0.521). The difference in pregnancy termination week was insignificant across the randomization groups (P = 0.13), as was the incidence of cesarean section births, preterm delivery, and low birth weight across the groups (P = 0.31, 0.25, and 0.33, respectively). Two babies (one in Group A and one in Group C) were of low birth weight, and eight babies (Group A, n = 4; Group B, n = 3; Group C, n = 1) were delivered preterm.
Table 3 Pregnancy outcome analysis in randomization groups
Adherence to regimen and side effects
Adherence to the regime was 100% according to data provided in the forms for the participants. No side effects were reported throughout the duration of the study.
Discussion
Low hemoglobin caused most commonly by iron deficiency is highly prevalent in pregnant women, and represents a global clinical problem with considerable impact on public health and health care systems.Citation1 Various routine iron supplementation regimes have been proposed in recent decades to address this issue from the public health perspective, most commonly consisting of daily iron supplementation. Our data suggest that there is no significant benefit of daily iron supplementation over intermittent dosing regimes for maintenance of safe hematologic marker levels and for preventing pregnancy and neonatal complications in pregnant women who are nonanemic at ≤20 weeks. The absence of a placebo control group allows only a comparison between daily, twice-weekly, and once-weekly supplementation groups. However, given that it has been well established by various studies that daily antenatal iron supplementation increases hemoglobin levels in maternal blood both antenatally and postnatally,Citation17 that absence of iron supplementation during pregnancy increases the risk of anemia,Citation18 and that various countries now recommend routine iron supplementation as a conceptual part of their public health care policy (US, France,Citation19 Iran), our goal was not to assess the impact of absence of iron supplementation in comparison with iron supplies, but to compare the effect of various iron supplementation regimens in a matched sample of pregnant women.
In the women who were nonanemic at 20≤weeks’ gestation, weekly supplementation was less effective in preventing hemoglobin levels <11 g/dL compared with twice-weekly and daily supplementation regimes. However, the twice-weekly regime has shown equal effectiveness as a daily supplementation regimen with respect to maintaining safe hemoglobin and ferritin levels throughout pregnancy. In addition to this, based on WHO criteria for the lowest (5th percentile) mid-pregnancy hemoglobin level of 10.5 g/dL,Citation16 also proposed by Milman et al,Citation20 none of the women who were excluded due to hemoglobin levels <11 g/dL at 28 weeks were in fact anemic (10.6, 10.7, and 10.7 g/dL). Moreover, this finding could be explained by the physiologic hemodilution that occurs during this stage of pregnancy. The reason they were transferred to a daily supplementation regimen was based on a cutoff point of 11 g/dL for anemia in pregnant women throughout pregnancy applied in routine Iranian clinical practice in accordance with the Iranian Ministry of Health recommendation.
Although hemoglobin levels were significantly lower in Group B compared with Groups A and C (P = 0.018) at 38 weeks, the difference was not clinically significant (Hb level >11 g/dL). A similar trend was observed for the difference in ferritin levels, in that although daily supplementation led to a significant increase in ferritin at 28 weeks (P = 0.03), this difference was not maintained towards 38 weeks in comparison with the other two regimes. Group B, on the other hand, achieved significantly lower ferritin levels compared with Group A and Group C at 38 weeks, but again this was not clinically significant.
Various studies comparing daily versus intermittent regimens have shown that the intermittent regimen is less effective in anemic pregnant women,Citation21,Citation22 while other studies conducted in anemicCitation23 and nonanemicCitation24 women demonstrate equal efficacy,Citation25 frequently due to poor adherence to the regime in the daily supplementation setting. In addition to equal ability to maintain safe hematologic markers on both regimes, studies also report a possible adverse effect of hemoconcentration on birth outcomeCitation24 and other aspects associated with daily exposure to iron, such as hypertension, in healthy nonanemic women.Citation26
At 38 weeks, 15.7% women in Group C had hemoconcentration, compared with 8.1% and 7.3% in Group A and Group B, respectively. However, the initial hemoglobin levels were higher in Group C (12.9% had hemoconcentration at week 20 compared with 5.3% in Group B), which may account for the considerably higher percentage of women with hemoconcentration in this group at the time of delivery.
It is noteworthy that many studies comparing daily versus intermittent iron supplementation attribute the low effectiveness of routine daily administration to low adherence with the daily regimen,Citation21,Citation27 which is mainly due to the side effects of daily iron supplementation. Given the fact that all women in our study reported full adherence and no side effects, it may be important to study the social characteristics of target study populations to verify this finding.
Another aspect that may have played a role in the significantly high adherence during this study is that all women were informed in detail about the general effects and benefits of iron on the course of their pregnancy and its outcome, and were clearly instructed on how and when to take their tablet(s). This is in accordance with another compliance study demonstrating that this approach increases compliance rates.Citation27
The dietary habits of the study sample were not specifically recorded, but given the relative ethnic, religious, and socioeconomic homogeneity of the participating women, it may be reasonably assumed that there were no significant differences in their diet. None of the participating women were vegetarians, and all were informed regarding proper dietary composition during pregnancy. In accordance with Islamic law, which does not allow pregnant women to fast, none were fasting. Several studies have demonstrated that anemia in pregnancy is associated with a risk of low birth weight or premature delivery.Citation28–Citation30 Our study shows that low birth weight occurred with equal frequency in the daily and weekly supplementation groups (n = 1 in each group), while no low birth weight infants occurred in the twice-weekly group.
Pan-population approaches using global routine iron supplementation, although introduced, eg, in India in the early 70s,Citation21 have proven to be ineffective in reducing the prevalence of anemia during pregnancy. Moreover, such approaches may not be safe in all circumstances, as shown by studies demonstrating an adverse effect on pregnancy outcome in women with higher hemoglobin levels who receive iron supplementation. Currently there is no general solution for this worldwide problem, which rather emphasizes the need for careful evaluation of target populations with respect to social, dietary, and religious customs, and in particular the need for an individual approach in each pregnant woman. Rigid iron supplementation rules based on inaccurate generalizations from studies conducted in different global and political regions in different ethnic populations and sometimes in a different decade may eventually cause harm instead of benefit in a subset of pregnant women and their babies.
In conclusion, our study shows that assessment of hematologic parameters in early pregnancy should be routinely incorporated into prenatal care and, based on this evaluation, appropriate iron supplementation should be proposed for every woman, regardless of location or background. This regimen should be in accordance with local and national population health and the woman’s individual medical history and needs. From a more general perspective, a heated debate concerning daily versus intermittent iron supplementation has developed in recent years. Both approaches have been corroborated with clinical trials, yet no clear conclusion can be reached. Although our results do not provide a definite answer, they do suggest that, in nonanemic women, a twice-weekly iron supplementation regime may represent a reasonable compromise for an initial iron dosing regimen in nonpregnant women that may be adjusted in concordance with the development of iron markers during pregnancy.
Acknowledgment
We would like to thank the Student Research Committee, Urmia University of Medical Sciences, for their support of this research.
Disclosure
The authors report no conflicts of interest in this work.
Reference
- StoltzfusRDefining iron-deficiency anemia in public health terms: a time for reflectionJ Nutr20011312S–2565S567S11160589
- SloanNLJordanEWinikoffBEffects of iron supplementation on maternal hematologic status in pregnancyAm J Public Health200292228829311818308
- LozoffBGeorgieffMKIron deficiency and brain developmentSemin Pediatr Neurol200613315816517101454
- HaramKNilsenSTUlvikRJIron supplementation in pregnancy – evidence and controversiesActa Obstet Gynecol Scand200180868368811531608
- MilmanNIron prophylaxis in pregnancy – general or individual and in which dose?Ann Hematol2006851282182816763841
- LeBlancCPFisetSSuretteMETurgeon O’BrienHRiouxFMMaternal iron deficiency alters essential fatty acid and eicosanoid metabolism and increases locomotion in adult guinea pig offspringJ Nutr200913991653165919640965
- AndrewsNCIron homeostasis: insights from genetics and animal modelsNat Rev Genet20001320821711252750
- Hematologic disorders of pregnancy3rd edFortnerKBSzymanskiLFoxHEWallachEEThe Johns Hopkins Manual of Gynecology and Obstetrics3rd edPhiladelphia, PALippincott Williams and Wilkins2007215230
- DeMaeyerEMDallmanPGurneyJMHallbergLSoodSKSrikantiaSGPreventing and controlling iron deficiency anaemia through primary health careGenevaWorld Health Organization1989
- BeardJLEffectiveness and strategies of iron supplementation during pregnancyAm J Clin Nutr2000715 Suppl1288S1294S10799404
- YektaZAyatollahiHPouraliRFarzinAPredicting factors in iron supplement intake among pregnant women in urban care settingJRHS200881
- BeardJLWeekly iron intervention: the case for intermittent iron supplementationAm J Clin Nutr19986822092129701171
- HahnPFBaleWFRossJFBalfourWMWhippleGHRadioactive iron absorption by gastro-intestinal tract: influence of anemia, anoxia, and antecedent feeding distribution in growing dogsJ Exp Med194378316918819871320
- WrightAJSouthonSThe effectiveness of various iron-supplementation regimens in improving the Fe status of anaemic ratsBr J Nutr19906335795852383534
- ViteriFELiuXTolomeiKMartinATrue absorption and retention of supplemental iron is more efficient when iron is administered every three days rather than daily to iron-normal and iron-deficient ratsJ Nutr1995125182917815180
- Prevention and management of severe anaemia in pregnancyReport of a Technical Working GroupGeneva, SwitzerlandWorld Health Organisation1993
- Pena-RosasJPViteriFEEffects of routine oral iron supplementation with or without folic acid for women during pregnancyCochrane Database Syst Rev20063CD00473616856058
- PreziosiPPrualAGalanPDaoudaHBoureimaHHercbergSEffect of iron supplementation on the iron status of pregnant women: consequences for newbornsAm J Clin Nutr1997665117811829356536
- MakridesMCrowtherCAGibsonRAGibsonRSSkeaffCMEfficacy and tolerability of low-dose iron supplements during pregnancy: a randomized controlled trialAm J Clin Nutr200378114515312816784
- MilmanNBygKEAggerAOHemoglobin and erythrocyte indices during normal pregnancy and postpartum in 206 women with and without iron supplementationActa Obstet Gynecol Scand2000792899810696955
- MukhopadhyayABhatlaNKriplaniAPandeyRMSaxenaRDaily versus intermittent iron supplementation in pregnant women: hematological and pregnancy outcomeJ Obstet Gynaecol Res200430640941715566454
- MumtazZShahabSButtNRabMADeMuynckADaily iron supplementation is more effective than twice weekly iron supplementation in pregnant women in Pakistan in a randomized double-blind clinical trialJ Nutr2000130112697270211053509
- YoungMWLupafyaEKapendaEBobrowEAThe effectiveness of weekly iron supplementation in pregnant women of rural northern MalawiTrop Doct2000302848810842553
- CasanuevaEViteriFEMares-GalindoMWeekly iron as a safe alternative to daily supplementation for nonanemic pregnant womenArch Med Res200637567468216740440
- RidwanESchultinkWDillonDGrossREffects of weekly iron supplementation on pregnant Indonesian women are similar to those of daily supplementationAm J Clin Nutr19966368848908644682
- ZiaeiSNorroziMFaghihzadehSJafarbeglooEA randomised placebo-controlled trial to determine the effect of iron supplementation on pregnancy outcome in pregnant women with haemoglobin > or = 13.2 g/dlBJOG2007114668468817516958
- HabibFAlabdinEHAlenazyMNoohRCompliance to iron supplementation during pregnancyJ Obstet Gynaecol200929648749219697194
- KidantoHLMogrenILindmarkGMassaweSNystromLRisks for preterm delivery and low birth weight are independently increased by severity of maternal anaemiaS Afr Med J20099929810219418670
- LoneFWQureshiRNEmmanuelFMaternal anaemia and its impact on perinatal outcome in a tertiary care hospital in PakistanEast Mediterr Health J200410680180716335767
- ScanlonKSYipRSchieveLACogswellMEHigh and low hemoglobin levels during pregnancy: differential risks for preterm birth and small for gestational ageObstet Gynecol2000965 Pt 174174811042311