
Abstract
Despite the availability of a range of treatment options and management guidelines, a high proportion of adults with asthma remain uncontrolled. The challenge of managing uncontrolled asthma includes providing efficacious treatment while limiting side effects, recognizing situations when a change in asthma therapy is required, and considering patient preferences and satisfaction. In line with the Global Initiative for Asthma report, asthma management is based on a backbone of inhaled corticosteroid (ICS) therapy and use of add-on therapies to achieve disease control. This review considers whether add-on options could be better utilized in clinical practice. A number of long-acting muscarinic antagonists are in development, but tiotropium is the most widely studied for use in asthma. Evidence demonstrating the efficacy of tiotropium as an add-on therapy to at least ICS in adults with symptomatic mild, moderate, and severe asthma is presented from randomized controlled trials and real-world evidence. In addition, the benefit of tiotropium therapy in a wide range of patient phenotypes and disease severities without the need for biomarker assessment is discussed. Additional strategies that complement this approach, such as recognizing and overcoming barriers to adherence, ensuring optimal device use, and education and support to enhance patient–physician communication, are discussed. Physician education can also help raise awareness that additional management options are available for patients with moderate-to-severe asthma who remain uncontrolled on ICS/long-acting β2-agonist treatment.
Video abstract
Point your SmartPhone at the code above. If you have a QR code reader the video abstract will appear. Or use:
Introduction
Despite the availability of a range of treatment options and management guidelines, an unacceptably high proportion of adults with asthma remain poorly controlled.Citation1 Reflective of the situation in a number of countries,Citation2 findings from a web-based survey conducted in over 2,500 Australian adults with asthma indicate poor self-rated symptom control in almost half of the participants, with an urgent need for asthma-related health care in the previous year reported by almost one-third of the participants.Citation3
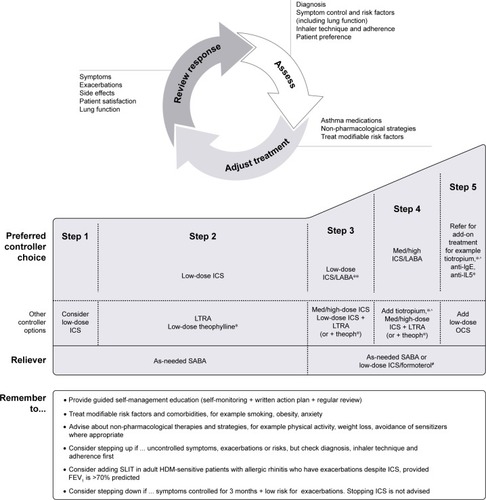
There remains a gap in asthma care worldwide, and effective clinical application of guideline recommendations is lacking.Citation3 The goals of asthma management are to achieve control, minimize the future risk of exacerbations, and reduce fixed airflow limitation, while minimizing treatment side effects.Citation4 In clinical practice, the challenge of managing uncontrolled asthma and achieving these goals should involve the principles outlined in the Global Initiative for Asthma (GINA) global strategy report, namely, a continuous cycle consisting of regular patient assessment, treatment adjustment, and review of the patient response to facilitate treatment decisions (). As part of this cycle, issues that characteristically impact treatment should be addressed, including consideration of whether the diagnosis is correct and an assessment of comorbidities, risk factors, inhaler technique, and adherence. Furthermore, the cycle of management and stepwise approach to care allows for providing treatment that is efficacious and safe according to individual patient needs, recognizing situations when a change in asthma therapy is required, while considering patient preferences and satisfaction.Citation4
Figure 1 Asthma management based on a continuous cycle of patient assessment, treatment, and review.
Abbreviations: HDM, house dust mite; ICS, inhaled corticosteroid; IgE, immunoglobulin E; IL5, interleukin-5; LABA, long-acting β2-agonist; LTRA, leukotriene receptor antagonist; OCS, oral corticosteroids; SABA, short-acting beta2-agonist; SLIT, sublingual immunotherapy.
Scope
In this review, the evidence for asthma management in adults will be discussed in the context of clinical challenges and the GINA management cycle, with consideration of whether add-on options could be better utilized in clinical practice. In particular, this review focuses on the evidence for tiotropium as an add-on to inhaled corticosteroid (ICS) for the treatment of asthma.
Current asthma management strategies
In line with the GINA global strategy report, management of adults with asthma is based on a preferred backbone of ICS therapy and use of add-on therapies, starting with long-acting β2-agonists (LABAs) and stepping up management based on patient needs in order to achieve disease control.Citation4 The GINA report proposes several options for add-on therapy in patients who are uncontrolled despite medium- to high-dose ICS with or without other controllers at GINA Step 4, including tiotropium for individuals with a history of severe exacerbations, or leukotriene receptor antagonists (LTRAs) or theophylline added to high-dose ICS. At GINA Step 5, it recommends that patients with severe asthma are offered add-on treatment with tiotropium and escalation to biologic therapies, such as anti-immunoglobulin E (IgE), anti-interleukin-5 (anti-IL-5), or low-dose oral corticosteroids ().Citation4
Anticholinergics, both long-acting and short-acting, have been used in the management of respiratory disease, particularly COPD, for many years. The short-acting anti-cholinergic ipratropium bromide is a well-established bronchodilator treatment for managing acute exacerbations of asthma in clinical practice.Citation5 Several long-acting muscarinic antagonist (LAMA) treatments are in clinical development and are reviewed elsewhere.Citation6–Citation10 Tiotropium is the most widely studied LAMA and the only one licensed for use in asthma. In addition to a growing body of evidence for use in asthma, tiotropium has the benefit of over 10 years of clinical experience in COPD.Citation11 Anticholinergics are muscarinic (M) receptor antagonists; in the airways, tiotropium binds equally well to M receptors (M1, M2, and M3), but dissociates slowly from the M1 and M3 anticholinergic receptors, resulting in the long duration of bronchodilator effect.Citation12–Citation14 In animal models and in vitro, tiotropium also has effects on inflammation and airway remodeling, although the clinical significance of this is uncertain.Citation15,Citation16 Tiotropium Respimat® is approved in patients with asthma aged 18 years and over in Australia and Singapore, 15 years and over in Japan, and 6 years and over in the US and the European Union. As the recommended dose and specific indication can vary, it is recommended that the indication/label in each country is checked.
Practical considerations for the management of patients with asthma
Each stage of the GINA control-based management strategy (assessment, adjustment, review) involves key principles for clinicians who care for patients with asthma.Citation4 These principles include the importance of recognizing patient preferences and satisfaction, offering support to overcome any barriers to adherence, assessing inhaler use, providing a written asthma action plan, and scheduling regular asthma reviews to optimize control and ensure that ineffective or poorly tolerated treatments are reviewed. A Cochrane review reported that education in asthma self-management, involving self-monitoring by either peak expiratory flow or symptoms, together with regular medical review and a written action plan, led to an improvement in several health outcomes for adults with asthma.Citation17 Regular clinical review can help health care professionals identify a need for a therapeutic change and recognize when an add-on option might be more appropriate than increasing ICS dose, and helps patients understand the important components to achieving good asthma control. Disease education empowers patients; hence, supporting patients to self-monitor symptoms and recognize triggers and disease worsening are valuable aspects of care.Citation18 Regular review opens communication channels between the patient and the health care professional, providing benefits on both sides, both clinically and with respect to patient satisfaction. Review is essential to assess recent asthma control and the benefit of treatment, check inhaler technique, and educate patients in self-management.Citation18 In accordance with the GINA cycle of asthma management, every treatment change should be followed by a scheduled asthma review after at least 2–3 months to assess and optimize control, and to ensure that ineffective or poorly tolerated treatments are reviewed.Citation4
Treatment adherence is a well-known challenge in asthma management. Effective communication regarding asthma management may help increase patients’ adherence, but, in addition to the challenges of time constraints, health care professionals may not be skilled in providing effective adherence assessment and advice. In one study, primary care physicians were provided with 2 hours’ training in delivering brief, motivational, interview-based adherence counseling with asthma-specific counseling support tools.Citation19 Almost all participants found the training very or extremely useful, leading to increased confidence and satisfaction with the quality of their consultations. Continuing to keep abreast of the evolving clinical evidence, new devices and treatment combinations, and support strategies for the care of patients with asthma is also important. It is becoming clear that asthma is a highly heterogeneous disease, and that ascertaining asthma phenotype may also guide therapeutic decisions in suboptimally controlled asthma.Citation20 However, there are very few clinical trials apart from those of targeted monoclonal therapies that examine treatment response in relation to phenotype. At present, monoclonal therapies are expensive, and it behooves clinicians to address all treatable traits – of which adherence is one, before embarking on long-term expensive therapies.
Optimally, health care professionals may look to continually evolve and refine the softer skills required for effective patient care. Participation in communication skills training can improve patient adherence, with the odds of patient adherence being 1.62 times higher than when a physician receives no training.Citation21 This meta-analysis reported a 19% higher risk of nonadherence among patients when their physician communicated poorly than among those who experienced effective physician communication.Citation21 Continuing professional development can also help enhance awareness of the alternative management options available for patients who remain uncontrolled on ICS with or without other controllers.
Counseling and training are also required, so that patients better understand their condition and how to use their inhaler, as even the most user-friendly devices require education and a demonstration.Citation22 In a study by Jahedi et al,Citation23 a total of 87.5% of patients were not able to demonstrate the correct inhaler technique and the majority of patients did not have any degree of involvement with decision-making regarding treatment. This was the case despite a body of evidence across many disease areas (including asthma) demonstrating that shared decision-making and effective patient–physician communication is of benefit to patients.Citation23 Routine checking of inhaler technique and asking patients to demonstrate use is important,Citation24 as patients can revert to an incorrect technique just after a short period.Citation25 Crane et alCitation26 reported that use of tailored education that included observation, verbal instruction, and device demonstration led to a significant improvement in device technique that was sustained at 12 months, while no significant improvement was recorded in those who only received written instructions.Citation26 A physical demonstration of inhaler technique and patient retraining at follow-up appointments is recommended in the GINA report,Citation4 as many studies show a rapid loss of technique after a single demonstration.Citation27,Citation28 A wide range of drug and inhaler device combinations are available; the most commonly used devices include pressurized metered-dose inhalers, dry powder inhalers, and soft mist inhalers.Citation25,Citation29 The soft mist inhaler, of which the Respimat® Soft Mist™ Inhaler (Boehringer Ingelheim, Ingelheim, Germany) for the delivery of tiotropium is an example, was developed to help overcome the limitations of other devices, which include aerosol velocity, limited drug deposition in the lung, and adequate patient coordination for inhalation.Citation29 Use of a number of separate inhalers requiring different inhalation techniques can be confusing for patients with asthma, but training and education can ensure that the benefit of additional controller medication is achieved. Of note, patient preference is recognized as a key factor in device selection, successful drug delivery, and adherence.Citation30
In summary, a number of strategies can be employed to help overcome perceived barriers to good asthma outcomes by offering individualized education and support.
Therapeutic strategies: tiotropium as an add-on therapy to at least ICS
The efficacy and safety of treatment with tiotropium as an add-on to standard ICS maintenance treatment, with or without a LABA, has been demonstrated in a large clinical study program comprising 18 trials with over 6,000 patients aged 1–75 years with symptomatic mild, moderate, or severe asthma.Citation31–Citation40 Six Phase III, double-blind, placebo-controlled, parallel-group trials have been conducted in adults with symptomatic asthma.Citation31–Citation34 The broad-based inclusion criteria required patients to have a documented history of poorly controlled asthma (defined by the seven-question Asthma Control Questionnaire [ACQ-7] score ≥1.5). Those with a significant disease other than asthma were excluded. Patients were also either lifelong nonsmokers or had a smoking history of fewer than 10 pack-years, with no smoking in the year before the study.
In the replicate PrimoTinA-asthma® 1 and 2 studies, tiotropium (5 µg) or placebo was added to high-dose ICS (≥800 µg budesonide or equivalent per day) plus LABA once daily for 48 weeks in 912 patients with symptomatic severe asthma ().Citation31 In patients with uncontrolled asthma despite treatment with ICS/LABA, the use of tiotropium add-on therapy significantly increased the time to first exacerbation and provided a modest sustained bronchodilation.Citation31 At 24 weeks, change in peak forced expiratory volume in 1 s (FEV1) within 3 hours post-dose (FEV1(0–3h)) from baseline was significantly greater with tiotropium in both trials compared with placebo (mean difference in the two studies: 86 mL [95% CI: 20–152 mL; P<0.05] and 154 mL [95% CI: 91–217 mL; P<0.001]). Findings were also significant for trough FEV1 with tiotropium compared with placebo (adjusted mean difference: 88 mL [95% CI: 27–149 mL; P<0.01] and 111 mL [95% CI: 53–169 mL; P<0.001]). Time to the first severe exacerbation was increased in patients treated with tiotropium add-on therapy vs placebo (282 vs 226 days), with a 21% reduction in the risk of a severe exacerbation (P=0.03). Improvements in asthma control and quality of life were observed in both trials between the tiotropium group and the placebo group. At Week 24, the mean difference in ACQ-7 and Asthma Quality of Life Questionnaire scores between groups was significantly improved for tiotropium-treated patients vs placebo in trial 2, but did not achieve the minimal clinically important differences (0.5 units for each questionnaire). The proportion of patients reporting adverse events (AEs) was comparable between placebo and tiotropium ().Citation31
Table 1 Summary of clinical trials and real-world evidence with tio add-on therapy in adult patients with asthma
Table 2 Summary of adverse events in Phase III clinical trials of tio in adults (18–75 years old) with mild, moderate, or severe asthma
MezzoTinA-asthma® 1 and 2, conducted in 2,103 adult patients with symptomatic moderate asthma, also comprised two replicate, randomized, double-blind, placebo-controlled trials. Once-daily tiotropium (5 or 2.5 µg), twice-daily salmeterol 50 µg, or placebo was added to medium-dose ICS (400–800 µg budesonide or equivalent per day) for 24 weeks ().Citation32 Data from the two studies were pooled. Tiotropium 5 and 2.5 µg add-on therapy led to a significant improvement in lung function compared with placebo (peak FEV1: 185 mL [95% CI: 146–223 mL; P<0.0001] with tiotropium 5 µg; 223 mL [95% CI: 185–262 mL; P<0.0001] with tiotropium 2.5 µg). Both doses of tiotropium significantly improved trough FEV1, and results were also numerically higher for tiotropium 2.5 µg. A significant reduction in the risk of first severe exacerbation and of first asthma worsening was reported for tiotropium 2.5 µg. There were also more ACQ-7 responders with tiotropium (5 and 2.5 µg), and salmeterol, compared with placebo (all P<0.05). The proportion of patients reporting AEs was similar across all treatment groups (). Overall, tiotropium added to medium-dose ICS provided significant improvements in lung function and asthma control that were similar to those of salmeterol; as such, it was concluded that tiotropium is a safe and effective bronchodilator and a potential alternative to salmeterol for use as an add-on therapy in this patient population.Citation32
In the GraziaTinA-asthma® study, 464 adults with symptomatic mild-to-moderate asthma received tiotropium (5 or 2.5 µg) or placebo added to low- to medium-dose ICS (200–400 µg budesonide or equivalent per day), as shown in .Citation33 Findings showed that once-daily tiotropium was an efficacious bronchodilator, and that safety and tolerability were comparable with placebo.Citation33 After 12 weeks, lung function was significantly improved with both doses of tiotropium compared with placebo (peak FEV1(0–3h): 128 mL [95% CI: 57–199 mL] with tiotropium 5 µg; 159 mL [95% CI: 88–230 mL] with tiotropium 2.5 µg; both P<0.001). Trough FEV1 was also significantly improved with both doses of tiotropium compared with placebo. This study was not designed to evaluate the effect of tiotropium on asthma exacerbations. Numerical improvements in the adjusted mean ACQ-7 total score were observed across all treatment groups after 12 weeks. The differences between each dose of tiotropium vs placebo were not statistically significant. The proportion of patients reporting AEs was similar across all treatment groups ().Citation33
In addition to the safety findings reported with the use of tiotropium add-on therapy in the Phase III studies described, a Japanese study randomized 285 patients to receive tiotropium (5 or 2.5 µg) or placebo as an add-on therapy to ICS/LABA for 52 weeks.Citation34 At Week 52, the proportion of patients reporting AEs with tiotropium 5 µg, 2.5 µg, and placebo were 88.6%, 86.8%, and 89.5%, respectively. No significant difference in the percentage of patients reporting AEs was observed between the groups (). Dahl et alCitation41 conducted a pooled safety analysis of seven Phase II and III, randomized, double-blind, parallel-group trials of 12–52 weeks’ treatment duration, which investigated once-daily tiotropium add-on therapy vs placebo in adult patients across a range of asthma severities. The proportion of patients with AEs was comparable between treatment groups (tiotropium 5 µg vs placebo 5 µg pool: 60.8% vs 62.5%; tiotropium 2.5 µg vs placebo 2.5 µg pool: 57.1% vs 55.1%). Patients were most commonly reported with asthma, decreased peak expiratory flow rate, and nasopharyngitis. A low proportion of patients reported AEs of special interest, including dry mouth (1.0% and 0.5% with tiotropium 5 µg and placebo, respectively) or cardiac AEs (1.4% with both tiotropium 5 µg and placebo).Citation41
Overall, these studies demonstrate the efficacy and safety of tiotropium in adults with a range of asthma severities. Furthermore, systematic reviews have concluded that a LAMA, such as tiotropium, serves as an effective bronchodilator across varying severities of asthma in patients who remain symptomatic on at least ICS, and particularly as an add-on to ICS/LABA therapy.Citation42–Citation44 In addition, findings from an independent study by Peters et alCitation45 support the use of tiotropium for the treatment of asthma in patients with asthma uncontrolled by ICS alone, demonstrating that the use of tiotropium was superior to doubling the ICS dose, with improvements in symptoms and lung function; tiotropium was also shown to be non-inferior to salmeterol ().
To date, a limited number of real-life studies have investigated the impact of incorporation of add-on tiotropium into clinical practice. A retrospective analysis was conducted of medical records from 633 adult patients with asthma who were admitted to an immunology and allergy diseases clinic between 2003 and 2011.Citation46 A total of 64 patients with severe asthma were followed for at least 1 year and treated with add-on tiotropium for at least 3 months. The mean time for onset of add-on tiotropium treatment was 5.5 months after admission to the outpatient clinic. The authors reported that tiotropium as an add-on to high-dose ICS and LABA therapy resulted in a number of improved endpoints compared with baseline (). These included lung function with a mean FEV1 of 57.5%±1.9% at baseline increasing to 65.5%±1.9% after 12 months of treatment with tiotropium add-on, and improved asthma control, according to GINA-based control assessment (based on daytime symptoms, night waking, need for reliever, and activity limitations), in 42.2% of cases with tiotropium add-on. Furthermore, with tiotropium add-on therapy compared with baseline, there was a reduction in the number of emergency department visits and hospitalizations in 46.9% and 50.0% of patients with severe asthma, respectively (all P<0.05).
In a real-life study conducted by Price et al,Citation47 medical records of adults with asthma who were prescribed tiotropium were obtained from the United Kingdom Optimum Patient Care Research Database for the period 2001–2013. Of the 2,042 study patients, 83% and 68% were receiving an ICS or a LABA, respectively, during the baseline year; 67% of patients were receiving both. When the outcome year, defined as the year after addition of tiotropium, was compared with the baseline year, the percentage of patients having at least one exacerbation decreased from 37% to 27% (P<0.001) and patients experiencing at least one acute respiratory event decreased from 58% to 47% (P<0.001), as shown in . Few real-world studies are available, and evidence to date is consistent with the findings from randomized clinical trials of tiotropium in asthma.Citation46,Citation47
Other add-on therapies for adults with asthma uncontrolled with ICS with or without other controllers
Other add-on therapies are available for adults with asthma that is uncontrolled with ICS. Leukotrienes are lipid mediators produced by inflammatory cells of the airways, and can cause bronchoconstriction, among other pathophysiologic effects. Montelukast is an LTRA that targets an inflammatory cascade mediated by sulfidopeptide leukotrienes, which are involved in the chemoattraction of inflammatory cells (including eosinophils) and possibly the proliferation of mucosal fibroblasts.Citation48 LTRAs disrupt leukotriene-mediated signaling, and can improve lung function and decrease other symptoms across a range of asthma severities in adults and children.Citation49 There are controversies in the clinical evidence supporting the efficacy of LTRAs, particularly in adults; for example, a meta-analysis of six clinical studies assessing montelukast as an add-on therapy in mild-to-moderate asthma showed significantly improved symptom control compared with ICS monotherapy.Citation50 In contrast, other studies of patients treated with ICS (mostly high-dose ICS) and additional therapy such as LABA showed the addition of montelukast produced no improvement in symptoms, lung function, or rescue medication use compared with placebo.Citation51,Citation52 Furthermore, a meta-analysis showed that LABA add-on to ICS is superior to LTRA addition, in terms of risk of exacerbations requiring systemic corticosteroids, and improvements in lung function, asthma symptoms, rescue medication use, and quality of life.Citation53 Overall, LTRAs may be most useful in specific populations, such as asthma in obese patients, in some with exercise-induced asthma, and in viral-induced wheezing episodes with asthma.Citation54
Theophylline is a non-selective phosphodiesterase inhibitor. It has relatively modest bronchodilator effects,Citation55,Citation56 but does have anti-inflammatory properties.Citation57 There is evidence to show that the addition of theophylline to ICS is clinically equivalent to doubling the dose of ICS in terms of improvements in lung function and symptoms in patients with moderate asthma.Citation58 However, theophylline has a narrow therapeutic window, thereby making it less well tolerated than inhaled treatment.Citation57
Biologic therapy has been the focus of more recent research. Omalizumab is a humanized anti-IgE monoclonal antibody approved as an add-on therapy for the treatment of moderate-to-severe allergic asthma inadequately controlled with high-dose ICS, with or without other controller medication.Citation59 Reslizumab (Teva) and mepolizumab (GlaxoSmithKline) are humanized anti-IL-5 monoclonal antibodies, and benralizumab (AstraZeneca) is an anti-IL-5 receptor α monoclonal antibody, which have all recently been approved for the treatment of severe eosinophilic asthma.Citation4,Citation60,Citation61 Dupilumab (Regeneron), which targets the receptors for both IL-4 and IL-13, has also demonstrated improved outcomes, including lung function and exacerbations, in patients with severe asthma.Citation62 Targeted monoclonal therapies show particular effects in reducing exacerbations in severe asthma in patients with eosinophilic inflammation, but are somewhat less effective in improving lung function and optimizing asthma control.Citation63 Biomarkers are usually required to identify patient populations that are most likely to benefit from the different biologic treatments (eg, peripheral eosinophil counts for anti-IL-5 therapies). This additional testing adds to an already costly therapy. Therefore, it may be most beneficial to assess the effects of biologics after the use of ICS/LABA plus additional controller medications, such as tiotropium, ensuring that more cost-effective therapeutic options have been exhausted. Currently, add-on anti-IgE and anti-IL-5 treatment form options at Step 5 of the GINA report recommendations.Citation4
Bronchial thermoplasty is a non-pharmaceutical intervention that uses thermal energy to reduce the amount of smooth muscle in the airway walls, making it less likely that the airways will become narrow in the future.Citation64 This option has shown improvements in quality of life and reduced exacerbations in patients with severe asthma. As it is an expensive intervention requiring several bronchoscopies, more evidence is required on the long-term efficacy and safety of the procedure to accurately assess its role and cost–benefit.Citation65 The GINA report recommends bronchial thermoplasty as a potential treatment option in patients with severe asthma (Step 5), but indicates that it should be performed “in adults with severe asthma only in the context of an independent Institutional Review Board-approved systematic registry or a clinical study, so that further evidence about the effectiveness and safety of the procedure can be accumulated”.Citation4
Incorporation of tiotropium in clinical practice
In the GINA report, tiotropium is recommended as an add-on option to ICS with or without other controller options in adult patients with a history of asthma exacerbations at Steps 4 or 5 (),Citation4 with no requirement for prior phenotyping. Several studies have been conducted to investigate the efficacy and safety of tiotropium, irrespective of baseline characteristics, allergic status, and phenotypic characteristics. In an exploratory analysis from four large asthma trials, pooled data from adults with moderate-to-severe asthma who were treated with once-daily tiotropium 5 or 2.5 µg as an add-on to at least ICS were analyzed.Citation66 Findings suggest that the efficacy of tiotropium is not predicted by a T2high or T2low profile, defined by IgE level, eosinophil count, or clinician judgment of allergic asthma in patients with asthma. Another analysis (in adults with severe asthma) reported that tiotropium 5 µg improved lung function, reduced the risk of exacerbations (time to first severe exacerbation), and improved asthma symptom control independent of several baseline characteristics such as IgE levels, eosinophil counts, age, gender, or baseline demographics compared with placebo.Citation67 Similar findings have been demonstrated in adults with symptomatic moderate asthma.Citation68
Obesity is a common comorbidity in patients with asthma.Citation69 Obese patients have more severe and more frequent respiratory symptoms compared with non-overweight asthma patients,Citation70 and thus may require specific consideration during treatment selection. A post hoc analysis of patients with symptomatic mild, moderate, and severe asthma demonstrated that changes in lung function were consistent across the range of body mass index, suggesting that tiotropium is an effective add-on therapy to ICS, independent of body mass index.Citation71 Thus, tiotropium offers an easy option to implement in clinical practice prior to moving onto other options if necessary.
It has been reported that some African-American patients with asthma may not benefit from LABA treatment to the same degree as individuals in other population subgroups,Citation72 and the use of tiotropium has been investigated as an alternative to LABA add-on therapy.Citation73 Findings suggest that LABA plus ICS did not add any benefit compared with tiotropium plus ICS in this population group. The Arg16/Arg16 β2-adrenergic receptor polymorphism has been reported in both African Americans and white asthma patients,Citation74 with an increased risk of a severe asthma exacerbation requiring hospitalization shown among patients with this polymorphism who are treated with a LABA.Citation74–Citation76 As such, tiotropium may offer an alternative add-on option to LABA in patients with this genotype who are not adequately controlled on ICS alone.Citation77 This was evident in a post hoc analysis of African-American patients (n=155) who participated in the tiotropium clinical trial program that showed the efficacy and safety of tiotropium compared with placebo in this group.Citation78 The proportion of African-American patients treated with tiotropium who experienced an AE leading to discontinuation or a drug-related AE was similar to placebo and to that of the overall population treated with tiotropium.Citation78
Asthma can be a costly disease due to its prevalence, long-term nature, and both direct and indirect health care costs, particularly attributable to patients with poor asthma control. The consequences of poor control, apart from the burden on the patient, include the impact on school and work attendance, work productivity, and health care services.Citation79 Findings from a UK-based analysis of adult patients with symptomatic severe asthma demonstrated that tiotropium Respimat® add-on therapy was a cost-effective management option when added to usual care, despite treatment with high-dose ICS/LABA therapy.Citation80,Citation81 Additionally, a US-based analysis has also shown that addition of tiotropium was cost-effective compared with both standard therapy and add-on omalizumab therapy in patients with uncontrolled allergic asthma.Citation82 In the US analysis, omalizumab resulted in the highest improvement in quality-adjusted life years and reduction in the number of exacerbations, but this came with substantial costs. Clearly, patients need to be trialed on different therapeutic options and all avenues should be explored before stepping up treatment.
In conclusion, tiotropium is a highly effective add-on therapy to ICS/LABA in poorly controlled asthma and the only long-acting anticholinergic therapy currently approved for asthma management. Its efficacy and safety has been demonstrated in a large-scale clinical trial program conducted in adults with symptomatic mild, moderate, or severe asthma. Given that a large proportion of patients with asthma are uncontrolled, health care professionals should continually work to implement the asthma management principles described in the GINA report, which involve a cycle of assessment, treatment adjustment, and regular review. Furthermore, empowering patients to play a role in their own care using tools such as written asthma management plans, developed in collaboration with their health care provider, may help earlier identification of cases where therapy changes or the use of an add-on therapy such as tiotropium is appropriate to help optimize patient outcomes.
Acknowledgments
The author takes full responsibility for the scope, direction, and content of, and editorial decisions relating to the manuscript, was involved at all stages of development, and has approved the submitted manuscript. The author would like to thank Kjeld Hansen, a member of the Patient Ambassador Group for the European Lung Foundation, for his input to the video summary for this manuscript. Medical writing assistance, in the form of preparation and revision of the draft manuscript, was supported financially by Boehringer Ingelheim and provided by Helen Moore, PhD, of MediTech Media, under the author’s conceptual direction and based on feedback from the author. Boehringer Ingelheim was given the opportunity to review the manuscript for factual accuracy only.
Disclosure
CJ is a member of advisory boards and steering committees for Boehringer Ingelheim and for several pharmaceutical companies the drugs of which are mentioned in this review. She has received payments for travel and attending these meetings. She has not received payment for writing this paper. The author reports no other conflicts of interest in this work.
References
- PriceDFletcherMvan der MolenTAsthma control and management in 8,000 European patients: the REcognise Asthma and Link to Symptoms and Experience (REALISE) surveyNPJ Prim Care Respir Med2014241400924921985
- DemolyPPaggiaroPPlazaVPrevalence of asthma control among adults in France, Germany, Italy, Spain and the UKEur Respir Rev20091811210511220956130
- ReddelHKSawyerSMEverettPWFloodPVPetersMJAsthma control in Australia: a cross-sectional web-based survey in a nationally representative populationMed J Aust2015202949249625971575
- Global Initiative for AsthmaGINA report: global strategy for asthma management and prevention Available from: http://ginasthma.org/2018-gina-report-global-strategy-for-asthma-management-and-prevention/Accessed March 8, 2018
- HamelmannESzeflerSJEfficacy and safety of tiotropium in children and adolescentsDrugs201878332733829368127
- D’AmatoMVitaleCMolinoALanzaMD’AmatoGAnticholinergic drugs in asthma therapyCurr Opin Pulm Med201723110310827820743
- CazzolaMOraJRoglianiPMateraMGRole of muscarinic antagonists in asthma therapyExpert Rev Respir Med201711323925328140686
- FerrandoMBagnascoDBraidoFUmeclidinium for the treatment of uncontrolled asthmaExpert Opin Investig Drugs2017266761766
- AlbertsonTEChenowethJAAdamsJYSutterMEMuscarinic antagonists in early stage clinical development for the treatment of asthmaExpert Opin Investig Drugs20172613549
- BusseWWDahlRJenkinsCCruzAALong-acting muscarinic antagonists: a potential add-on therapy in the treatment of asthma?Eur Respir Rev201625139546426929422
- HalpinDMKaplanAGRussellRKWhy choose tiotropium for my patient? A comprehensive review of actions and outcomes versus other bronchodilatorsRespir Med2017128284128610667
- BarnesPJThe pharmacological properties of tiotropiumChest20001172 Suppl63S66S10673478
- DisseBSpeckGARomingerKLWitekTJJrHammerRTiotropium (Spiriva): mechanistical considerations and clinical profile in obstructive lung diseaseLife Sci1999646–745746410069510
- HaddadEBMakJCBarnesPJCharacterization of [3H]Ba 679 BR, a slowly dissociating muscarinic antagonist, in human lung: radioligand binding and autoradiographic mappingMol Pharmacol19944558999078190106
- RadovanovicDSantusPBlasiFManteroMThe evidence on tiotro-pium bromide in asthma: from the rationale to the bedsideMultidiscip Respir Med2017121228484598
- MeursHOenemaTAKistemakerLEGosensRA new perspective on muscarinic receptor antagonism in obstructive airways diseasesCurr Opin Pharmacol201313331632323643733
- GibsonPGPowellHCoughlanJSelf-management education and regular practitioner review for adults with asthmaCochrane Database Syst Rev20021CD001117
- ReddelHKJenkinsCRPartridgeMRSelf-management support and other alternatives to reduce the burden of asthma and chronic obstructive pulmonary diseaseInt J Tuberc Lung Dis201418121396140625517803
- FosterJMSmithLUsherwoodTSawyerSMReddelHKGeneral practitioner-delivered adherence counseling in asthma: feasibility and usefulness of skills, training and support toolsJ Asthma201653331132026365203
- CharriotJVachierIHalimiLFuture treatment for asthmaEur Respir Rev201625139779226929425
- ZolnierekKBDimatteoMRPhysician communication and patient adherence to treatment: a meta-analysisMed Care200947882683419584762
- WesterikJACarterVChrystynHCharacteristics of patients making serious inhaler errors with a dry powder inhaler and association with asthma-related events in a primary care settingJ Asthma201653332132926810934
- JahediLDownieSRSainiBChanHKBosnic-AnticevichSInhaler technique in asthma: how does it relate to patients’ preferences and attitudes toward their inhalers?J Aerosol Med Pulm Drug Deliv2017301425227676193
- CromptonGKBarnesPJBroedersMThe need to improve inhalation technique in Europe: a report from the Aerosol Drug Management Improvement TeamRespir Med200610091479149416495040
- LavoriniFLevyMLCorriganCCromptonGADMIT Working GroupThe ADMIT series – issues in inhalation therapy. 6) Training tools for inhalation devicesPrim Care Respir J201019433534121049263
- CraneMAJenkinsCRGoemanDPDouglassJAInhaler device technique can be improved in older adults through tailored education: findings from a randomised controlled trialNPJ Prim Care Respir Med2014241403425188403
- ResnickDJGoldRLLee-WongMFeldmanBRRamakrishnanRDavisWJPhysicians’ metered dose inhaler technique after a single teaching sessionAnn Allergy Asthma Immunol19967621451488595532
- BashetiIAThe effect of using simulation for training pharmacy students on correct device techniqueAm J Pharm Educ2014781017725657364
- DalbyRNEicherJZierenbergBDevelopment of Respimat(®) Soft Mist™ Inhaler and its clinical utility in respiratory disordersMed Devices (Auckl)2011414515522915941
- Moroni-ZentgrafPImpact of patient needs on design and usage of an inhalation device in respiratory medicineRespir Drug Deliv20131141
- KerstjensHAEngelMDahlRTiotropium in asthma poorly controlled with standard combination therapyN Engl J Med2012367131198120722938706
- KerstjensHACasaleTBBleeckerERTiotropium or salmeterol as add-on therapy to inhaled corticosteroids for patients with moderate symptomatic asthma: two replicate, double-blind, placebo-controlled, parallel-group, active-comparator, randomised trialsLancet Respir Med20153536737625682232
- PaggiaroPHalpinDMBuhlRThe effect of tiotropium in symptomatic asthma despite low- to medium-dose inhaled corticosteroids: a randomized controlled trialJ Allergy Clin Immunol Pract20164110411326563670
- OhtaKIchinoseMTohdaYLong-term once-daily tiotropium Respimat® is well tolerated and maintains efficacy over 52 weeks in patients with symptomatic asthma in Japan: a randomised, placebo-controlled studyPLoS One2015104e012410925894430
- HamelmannEBatemanEDVogelbergCTiotropium add-on therapy in adolescents with moderate asthma: a 1-year randomized controlled trialJ Allergy Clin Immunol2016138244145026960245
- VogelbergCEngelMLakiITiotropium add-on therapy improves lung function in children with symptomatic moderate asthmaJ Allergy Clin Immunol Pract Epub2018508
- HamelmannEBernsteinJAVandewalkerMA randomised controlled trial of tiotropium in adolescents with severe symptomatic asthmaEur Respir J2017491160110027811070
- SzeflerSJMurphyKHarperT3rdA Phase III randomized controlled trial of tiotropium add-on therapy in children with severe symptomatic asthmaJ Allergy Clin Immunol201714051277128728189771
- BisgaardHVandewalkerMGrahamLMSafety of tiotropium in pre-school children with symptomatic persistent asthmaEur Respir J201648Suppl 60PA315
- VogelbergCLakiISchmidtOSafety and tolerability of once-daily tiotropium Respimat® add-on therapy in children with moderate symptomatic asthmaEur Respir J201648Suppl 60PA4399
- DahlREngelMDusserDSafety and tolerability of once-daily tiotropium Respimat(®) as add-on to at least inhaled corticosteroids in adult patients with symptomatic asthma: a pooled safety analysisRespir Med201611810211127578478
- AndersonDEKewKMBoyterACLong-acting muscarinic antagonists (LAMA) added to inhaled corticosteroids (ICS) versus the same dose of ICS alone for adults with asthmaCochrane Database Syst Rev2015248CD011397
- KewKMDahriKLong-acting muscarinic antagonists (LAMA) added to combination long-acting beta2-agonists and inhaled corticosteroids (LABA/ICS) versus LABA/ICS for adults with asthmaCochrane Database Syst Rev2016211CD011721
- RodrigoGJCastro-RodríguezJAWhat is the role of tiotropium in asthma?: a systematic review with meta-analysisChest2015147238839625322075
- PetersSPKunselmanSJIcitovicNTiotropium bromide step-up therapy for adults with uncontrolled asthmaN Engl J Med2010363181715172620979471
- AbadogluOBerkSTiotropium may improve asthma symptoms and lung function in asthmatic patients with irreversible airway obstruction: the real-life dataClin Respir J201610442142725335652
- PriceDKaplanAJonesRLong-acting muscarinic antagonist use in adults with asthma: real-life prescribing and outcomes of add-on therapy with tiotropium bromideJ Asthma Allergy2015811325609985
- PaggiaroPBacciEMontelukast in asthma: a review of its efficacy and place in therapyTher Adv Chronic Dis201121475823251741
- Peters-GoldenMHendersonWRJrLeukotrienesN Engl J Med2007357181841185417978293
- JoosSMikschASzecsenyiJMontelukast as add-on therapy to inhaled corticosteroids in the treatment of mild to moderate asthma: a systematic reviewThorax200863545346218443162
- RobinsonDSCampbellDBarnesPJAddition of leukotriene antagonists to therapy in chronic persistent asthma: a randomised double-blind placebo-controlled trialLancet200135792732007201111438132
- TonelliMZingoniMBacciEShort-term effect of the addition of leukotriene receptor antagonists to the current therapy in severe asthmaticsPulm Pharmacol Ther200316423724012850127
- ChauhanBFDucharmeFMAddition to inhaled corticosteroids of long-acting beta2-agonists versus anti-leukotrienes for chronic asthmaCochrane Database Syst Rev2014241CD003137
- MarcelloCCarloLAsthma phenotypes: the intriguing selective intervention with montelukastAsthma Res Pract201621127965779
- PaggiaroPLGianniniDDi FrancoATestiRComparison of inhaled salmeterol and individually dose-titrated slow-release theophylline in patients with reversible airway obstruction. European Study GroupEur Respir J199698168916958866596
- DahlRLarsenBBVengePEffect of long-term treatment with inhaled budesonide or theophylline on lung function, airway reactivity and asthma symptomsRespir Med200296643243812117043
- BarnesPJTheophyllineAm J Respir Crit Care Med2013188890190623672674
- UkenaDHarnestUSakalauskasRComparison of addition of theophylline to inhaled steroid with doubling of the dose of inhaled steroid in asthmaEur Respir J19971012275427609493656
- LiJKangJWangCOmalizumab improves quality of life and asthma control in Chinese patients with moderate to severe asthma: a randomized Phase III studyAllergy Asthma Immunol Res20168431932827126725
- BjermerLLemiereCMasperoJWeissSZangrilliJGerminaroMReslizumab for inadequately controlled asthma with elevated blood eosinophil levels: a randomized Phase 3 studyChest2016150478979827056586
- OrtegaHGLiuMCPavordIDMepolizumab treatment in patients with severe eosinophilic asthmaN Engl J Med2014371131198120725199059
- WenzelSCastroMCorrenJDupilumab efficacy and safety in adults with uncontrolled persistent asthma despite use of medium-to-high-dose inhaled corticosteroids plus a long-acting β2 agonist: a randomised double-blind placebo-controlled pivotal Phase 2b dose-ranging trialLancet201638810039314427130691
- PavordIDKornSHowarthPMepolizumab for severe eosinophilic asthma (DREAM): a multicentre, double-blind, placebo-controlled trialLancet2012380984265165922901886
- RubinAZelmanovitzSCavalcantiMBronchial thermoplasty in a patient with difficult-to-control asthmaJ Bras Pneumol201642215515627167438
- WahidiMMKraftMBronchial thermoplasty for severe asthmaAm J Respir Crit Care Med2012185770971422077066
- CasaleTBBatemanEDVandewalkerMTiotropium Respimat add-on is efficacious in symptomatic asthma, independent of T2 phenotypeJ Allergy Clin Immunol Pract20186392393529174062
- KerstjensHAMoroni-ZentgrafPTashkinDPTiotropium improves lung function, exacerbation rate, and asthma control, independent of baseline characteristics including age, degree of airway obstruction, and allergic statusRespir Med201611719820627492532
- CasaleTBBatemanEDAalbersROnce-daily tiotropium Respimat add-on therapy improves lung function and asthma control in moderate symptomatic asthma, independent of baseline characteristicsEur Respir J201750PA647
- BouletLPAsthma and obesityClin Exp Allergy201343182123278876
- TaylorBManninoDBrownCCrockerDTwum-BaahNHolguinFBody mass index and asthma severity in the National Asthma SurveyThorax2008631142018156567
- KhuranaSKerstjensHAPaggiaroPOnce-daily tiotropium Respimat® add-on to inhaled corticosteroid maintenance therapy reduces airflow obstruction in patients with symptomatic asthma, independent of body mass index scoreAm J Respir Crit Care Med2017195A6443
- WechslerMECastroMLehmanEImpact of race on asthma treatment failures in the asthma clinical research networkAm J Respir Crit Care Med2011184111247125321885625
- WechslerMEYawnBPFuhlbriggeALAnticholinergic vs long-acting β-agonist in combination with inhaled corticosteroids in black adults with asthma: the BELT randomized clinical trialJAMA2015314161720173026505596
- OrtegaVEHawkinsGAMooreWCEffect of rare variants in ADRB2 on risk of severe exacerbations and symptom control during longacting β agonist treatment in a multiethnic asthma population: a genetic studyLancet Respir Med20142320421324621682
- WechslerMEKunselmanSJChinchilliVMEffect of beta2-adrenergic receptor polymorphism on response to longacting beta2 agonist in asthma (LARGE trial): a genotype-stratified, randomised, placebo-controlled, crossover trialLancet200937497031754176419932356
- PalmerCNLipworthBJLeeSIsmailTMacgregorDFMukhopadhyaySArginine-16 beta2 adrenoceptor genotype predisposes to exacerbations in young asthmatics taking regular salmeterolThorax2006611194094416772309
- BatemanEDKornmannOSchmidtPPivovarovaAEngelMFabbriLMTiotropium is noninferior to salmeterol in maintaining improved lung function in B16-Arg/Arg patients with asthmaJ Allergy Clin Immunol2011128231532221807250
- GrahamLKerstjensHAVogelbergCSafety and tolerability of once-daily tiotropium Respimat® add-on therapy in African-American patients with symptomatic persistent asthma across a range of severitiesAm J Respir Crit Care Med2017195A6445
- NunesCPereiraAMMorais-AlmeidaMAsthma costs and social impactAsthma Res Pract20173128078100
- WillsonJBatemanEDPavordILloydAKrivasiTEsserDCost effectiveness of tiotropium in patients with asthma poorly controlled on inhaled glucocorticosteroids and long-acting β-agonistsAppl Health Econ Health Policy201412444745924974107
- WillsonJBatemanEDPavordILloydAKrivasiTEsserDErratum to: Cost effectiveness of tiotropium in patients with asthma poorly controlled on inhaled glucocorticosteroids and long-acting β-agonistsAppl Health Econ Health Policy201614111912526816028
- ZafariZSadatsafaviMFitzGeraldJMCanadian Respiratory Research NetworkCost-effectiveness of tiotropium versus omalizumab for uncontrolled allergic asthma in USCost Eff Resour Alloc2018161329422778