
Abstract
Background
IL-17-producing CD8+ T (Tc17) cells promote inflammation and have been identified in chronic hepatitis. However, the role of Tc17 cells in patients with hepatitis B virus (HBV)-related acute-on-chronic liver failure (HBV-ACLF) remains unclear.
Methods
The frequency of Tc17 cells in blood samples from 66 patients with HBV-ACLF was determined by flow cytometry. The levels of Tc17 cell-related cytokines were measured by FlowCytomix assays. The prognostic prediction accuracy was evaluated by the receiver operating characteristic (ROC) curve analysis. Survival was analyzed using Kaplan–Meier curves. Mortality predictors were determined by the Cox regression analysis.
Results
The frequency of Tc17 cells was markedly higher in patients with HBV-ACLF than in those with chronic hepatitis B and normal control subjects. Increased frequencies of Tc17 cells may indicate liver injury and were positively correlated with disease severity. The Tc17 cell frequency was significantly higher in non-surviving patients with HBV-ACLF than in surviving patients. The ROC curve analysis showed that Tc17 cell frequency accurately predicted 90-day survival in patients with HBV-ACLF, with an accuracy equivalent to those of the Model for End-Stage Liver Disease (MELD), MELD-Na, and Chronic Liver Failure Consortium ACLF scores. Kaplan–Meier analysis showed an association between the increase in circulating Tc17 cells and poor overall survival in patients with HBV-ACLF. Moreover, the multivariate Cox regression analysis showed that Tc17 cell frequency was an independent predictor of overall survival in patients with HBV-ACLF.
Conclusion
Tc17 cells may play a proinflammatory role in HBV-ACLF pathogenesis. Furthermore, the increased frequency of circulating Tc17 cells could be an independent prognostic biomarker in patients with HBV-ACLF.
Introduction
Acute-on-chronic liver failure (ACLF) is a severe clinical syndrome characterized by the acute deterioration of preexisting chronic liver diseases and is linked with substantial short-term mortality.Citation1 In China, HBV-related ACLF (HBV-ACLF) accounts for most patients because of the high prevalence of HBV infection.Citation2 The lack of knowledge on the mechanism underlying HBV-ACLF and the lack of effective treatment result in extremely high mortality.Citation3 Accumulating evidence has shown that systemic inflammation caused by excessive immune-mediated inflammation plays a central role in the mechanism underlying HBV-ACLF. Moreover, systemic inflammation has been found to be associated with disease progression and mortality in patients with HBV-ACLF.Citation1,Citation2,Citation4,Citation5
IL-17 has been researched intensely since its discovery. IL-17 is a proinflammatory cytokine that participates in both acute and chronic inflammatory responses and is mainly produced by a subset of CD4+ T cells (namely, Th17 cells);Citation6 however, other immune cells, including CD8+ T cells (namely, Tc17 cells), can also express IL-17.Citation7,Citation8 Tc17 cells have been detected in several autoimmune diseases in both humans and mice,Citation9,Citation10 thus confirming their role in inflammatory processes. In addition, the accumulation of Tc17 cells has been observed in several types of human tumors.Citation11 Furthermore, Tc17 cells were found to protect the host against lethal influenza infection.Citation12 Tc17 cells were found to be enriched in the liver of patients with chronic HCV infection, and the frequency of intrahepatic Tc17 cells was significantly higher than that in the peripheral blood.Citation13 Intrahepatic Tc17 cells increased in other chronic liver diseases, including alcoholic liver disease, non-alcoholic steatohepatitis, and autoimmune hepatitis. Moreover, the CXCR3 pathway could promote recruitment of Tc17 cells from the blood into the liver.Citation14 However, less is known about the role and clinical relevance of Tc17 cells in patients with HBV-ACLF.
On the basis of these collective and emerging data, we hypothesized that Tc17 cells may be implicated in the pathogenesis of HBV-ACLF. The main aim of the current study was to evaluate the role and the prognostic value of Tc17 cells in patients with HBV-ACLF.
Methods
Study design and patients
Sixty-six patients with HBV-ACLF admitted to our department between April 2009 and August 2014 were enrolled. HBV-ACLF was diagnosed on the basis of the development of jaundice (a Tbil of ≥171 µmol/L), a PTA of ≤40%, and the presence of at least one of the other criteria (≥ grade 2 hepatic encephalopathy, ascites, spontaneous bacterial peritonitis, or hepatorenal syndrome).Citation15,Citation16 The exclusion criteria were 1) evidence of other liver diseases or cancer; 2) coinfection with other hepatitis viruses or HIV; 3) treatment with artificial liver support or immunomodulatory drugs; 4) drug or alcohol abuse; 5) history of cardiovascular, pulmonary, or renal diseases; and 6) pregnancy. Cirrhosis was clinically diagnosed when a small, nodular liver was observed in imaging tests, including ultrasound, computerized tomography scans, or magnetic resonance imaging.Citation17 Each patient was treated with supportive internal treatment. All patients with HBV-ACLF were followed up for at least 3 months. The patients’ outcomes were recorded as surviving or non-surviving. Thirty patients with CHB and 17 NC during the same period were enrolled as controls. Patients with CHB were defined as those who had showed HBsAg positivity for more than 6 months and exhibited signs of hepatitis and abnormal liver function. A clinical assessment was performed and peripheral blood was collected at admission. Serum was separated and stored at −80°C until analysis. The study was conducted in accordance with the guidelines of the Declaration of Helsinki, and the protocol was approved by the ethics committee of our hospital (The Third Affiliated Hospital of Sun Yat-sen University). Written informed consent was obtained from each participant.
Cell staining and flow cytometry
An APC-conjugated anti-CD8 antibody was purchased from BD Biosciences (San Jose, CA, USA). A PerCP-Cy5.5-conjugated anti-CD3 antibody and a phycoerythrin-conjugated anti-IL-17A antibody were purchased from eBioscience (San Diego, CA, USA). Fresh heparinized peripheral blood was incubated in RPMI 1640 medium supplemented with phorbol 12-myristate 13-acetate (20 ng/mL; Sigma-Aldrich Co., St Louis, MO, USA) and ionomycin (1 µg/mL; Sigma-Aldrich Co.) for 5 hours at 37°C and 5% CO2. Monensin (1.7 µg/mL; Sigma-Aldrich Co.) was added during the first hour of incubation. Intracellular IL-17A staining was performed after fixation and permeabilization using Fix&Perm reagents (Thermo Fisher Scientific, Waltham, MA, USA). Data were collected on a FACSCalibur and analyzed with CELLQUEST software (BD Biosciences).
Cytokine analysis by FlowCytomix
Levels of serum cytokines (IL-17A, IL-22, and IL-23) were quantified using FlowCytomix™ kits (Bender MedSystems, Vienna, Austria) according to the manufacturer’s instructions. Data were collected on a FACSCalibur and analyzed with FlowCytomix Pro software (Bender MedSystems). Standard curves were determined for each cytokine. The detection sensitivity was 2.5 pg/mL for the IL-17A kit, 43.3 pg/mL for the IL-22 kit, and 21.9 pg/mL for the IL-23 kit.
Virological assessment and liver biochemical assays
The levels of serum HBV markers (including HBsAg, HBeAg, HBeAb, and HBcAb) and AFP were measured using an Elecsys system (Hoffman-La Roche Ltd., Basel, Switzerland). HBV-DNA levels were quantitated with RT-PCR using an ABI7300 instrument (Thermo Fisher Scientific). The detection limit of HBV-DNA was 100 IU/mL. Biochemical assays were performed using an autoanalyzer (TBA-30FR; Toshiba, Tokyo, Japan). PTA was measured using an automatic hemostasis/thrombosis analyzer (STA Compact, Holliston, MA, USA).
Disease severity assessment
MELD, MELD-Na, and CLIF-C ACLF scores were used to assess disease severity.Citation18,Citation19 Briefly, these scores were calculated as follows: MELD score=3.8×ln(bilirubin [mg/dL])+ 11.2×ln(INR)+9.6×ln(creatinine [mg/dL])+6.4×(etiology: 0 if cholestatic or alcoholic, 1 otherwise); MELD-Na score=MELD score−Na−0.025×MELD×(140−Na)+140; and CLIF-C ACLF score=10×(0.33×CLIF-OFs+0.04×Age+0.63×ln[WBC count]−2).
Statistical analyses
Data were analyzed using SPSS version 20.0 (IBM Corporation, Armonk, NY, USA) and were expressed as frequencies, medians, and ranges or mean ± standard deviations. Differences in variables were analyzed with ANOVA and Student’s t-tests or with Kruskal–Wallis tests and Mann–Whitney U tests. Correlations were evaluated by Pearson or Spearman tests. ROC curves were used to predict prognosis. Comparisons of ROC curve parameters were performed using the DeLong test. Survival was analyzed using Kaplan–Meier curves. The association between relevant variables and mortality was investigated by the multivariate Cox regression analysis. Two-sided P-values of <0.05 were considered statistically significant.
Results
Patients’ characteristics
The median age of the patients with HBV-ACLF was 41 years (range 18–75). During the follow-up period, 28 patients with HBV-ACLF survived, while 38 died. Thus, the overall mortality rate was 57.6%. Sixteen (24.2%) patients with HBV-ACLF were clinically diagnosed with cirrhosis before enrollment. The mortality rate was lower in patients without cirrhosis (25/50, 50%) than in those with cirrhosis (13/16, 81%, P=0.041). The baseline characteristics of the participants are shown in . No significant differences existed among the three groups in age (P=0.151) or gender (P=0.690).
Table 1 Characteristics of participants enrolled in the study
Tc17 cell frequency was significantly higher in patients with HBV-ACLF independent of HBeAg status
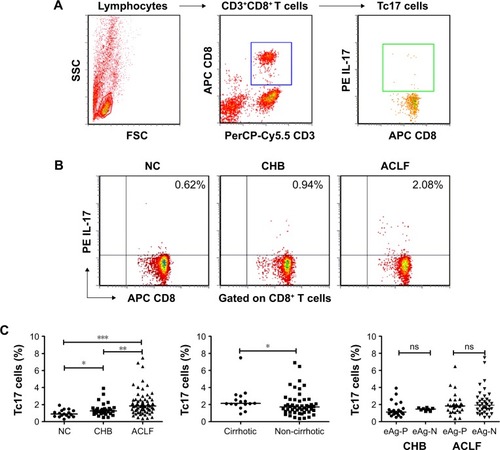
We measured the frequency of Tc17 cells by flow cytometry (). Tc17 cells were significantly higher in patients with HBV-ACLF (median 1.84%, range 0.36%–7.48%) than in either patients with CHB (median 1.26%, range 0.5%–3.91%; P=0.002) or NC subjects (0.96%±0.42%, P<0.001; ). Moreover, the frequency of Tc17 cells was significantly higher in cirrhotic patients with HBV-ACLF (median 2.13%, range 0.91%–7.48%) than in non-cirrhotic patients with HBV-ACLF (median 1.72%, range 0.36%–6.90%; P=0.034; ). We then determined the correlation between HBeAg status and Tc17 cell frequency. The Tc17 cell frequency did not differ between HBeAg-positive and HBeAg-negative patients with either CHB (P=0.097) or HBV-ACLF (P=0.496; ).
Figure 1 Tc17 cell frequency was significantly higher in patients with HBV-ACLF.
Abbreviations: ACLF, acute-on-chronic liver failure; CHB, chronic hepatitis B; eAg-P, HBeAg-positive; FSC, forward scatter; eAg-N, HBeAg-negative; HBV, hepatitis B virus; ns, not significant; NC, normal control; SSC, side scatter; Tc17, IL-17-producing CD8+ T.
Tc17 cells may play a proinflammatory role in the pathogenesis of HBV-ACLF
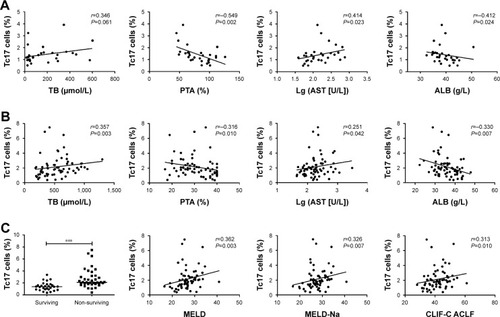
We subsequently analyzed the correlation between Tc17 cell levels and Tbil levels, PTA levels, ALB levels, AST levels, ALT levels, and HBV-DNA loads in patients with CHB and patients with HBV-ACLF. Tc17 cells were found to be associated with Tbil (r=0.346, P=0.061), PTA (r=−0.549, P=0.002), AST (r=0.414, P=0.023), and ALB levels (r=−0.412, P=0.024; ) in patients with CHB. Additionally, significant correlations were found between Tc17 cells and Tbil (r=0.357, P=0.003), PTA (r=−0.316, P=0.010), AST (r=0.251, P=0.042), and ALB levels (r=−0.330, P=0.007; ) in patients with HBV-ACLF. However, no significant correlation was observed between Tc17 levels and either ALT levels or HBV-DNA loads in CHB and HBV-ACLF patients. Next, we examined the correlation between clinical outcome and Tc17 cell frequency at admission. The frequencies of Tc17 cells were significantly higher in non-surviving patients (median 2.11%, range 0.40%–7.48%) than in surviving patients (median 1.38%, range 0.36%–3.35%, P<0.001; ). Moreover, we stratified HBV-ACLF patients into three groups according to their disease severity on the basis of the Asian Pacific Association for the Study of the Liver ACLF Research Consortium grade system.Citation20 Interestingly, Tc17 cells progressively increased from the ACLF-I group (0.88%±0.40%, n=8) to the ACLF-II group (2.12%±1.39%, n=44; vs ACLF-I group, P<0.001) to maximum in the ACLF-III group (3.01%±1.39%, n=14; vs ACLF-II group, P=0.007). MELD, MELD-Na, and CLIF-C ACLF scores are widely used to evaluate disease severity in patients with HBV-ACLF. In this study, these parameters were calculated at admission. The results were 26.89±4.17, 27.97±4.12, and 41.98±6.49 for the MELD score, MELD-Na score, and CLIF-C ACLF score, respectively. Next, correlations between Tc17 cells and these scores were examined. Interestingly, positive correlations were found between Tc17 cell frequency and MELD score (r=0.362, P=0.003), MELD-Na score (r=0.326, P=0.007), and CLIF-C ACLF score (r=0.313, P=0.010; ). Collectively, these findings indicated that Tc17 cells may play a proinflammatory role in the pathogenesis of HBV-ACLF.
Figure 2 Tc17 cells may play a proinflammatory role in the pathogenesis of HBV-ACLF.
Abbreviations: ACLF, acute-on-chronic liver failure; AST, aspartate aminotransferase; ALB, albumin; CHB, chronic hepatitis B; CLIF-C, chronic liver failure consortium; HBV, hepatitis B virus; MELD, model for end-stage liver disease; PTA, prothrombin time activity; TB, total bilirubin; Tc17, IL-17-producing CD8+ T.
Increased Tc17 cell frequency at admission indicated poor prognosis in patients with HBV-ACLF
The ROC curve analysis was used to evaluate the value of Tc17 cells in predicting prognosis. The area under the ROC curve (AUROC) was 0.826 (95% CI: 0.712–0.908, P<0.0001; ). The Youden index was used to identify the optimal cutoff value, defined as the value that maximized the sensitivity and specificity. With a cutoff value of 1.6%, the sensitivity was 86.84% (95% CI: 71.9%–95.6%) and the specificity was 75% (95% CI: 55.1%–89.3%). More importantly, no significant differences were observed between the AUROC values obtained using the Tc17 cell frequency and those obtained with the MELD score (AUROC=0.769, P=0.437), MELD-Na score (AUROC=0.782, P=0.552), or CLIF-C ACLF score (AUROC=0.773, P=0.474; ), indicating that the frequency of Tc17 cells at admission may have a prognostic value equivalent to that of these accepted scores.
Figure 3 Increased Tc17 cell frequency at admission indicated poor prognosis in HBV-ACLF.
Abbreviations: AUC, area under curve; ACLF, acute-on-chronic liver failure; AUROC, area under the ROC curve; CLIF-C, chronic liver failure consortium; Cum, cumulative; HBV, hepatitis B virus; MELD, model for end-stage liver disease; ROC curve, receiver operating characteristic curve; Tc17, IL-17-producing CD8+ T.
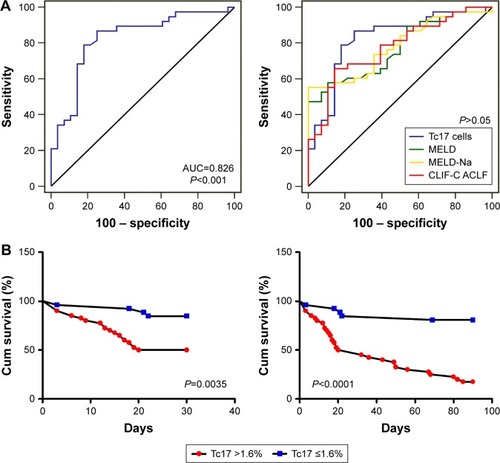
Patients were then divided into two groups, a higher group (Tc17 cell frequency >1.6%, N=40) and a lower group (Tc17 cell frequency ≤1.6%, N=26). The 30-day mortality rate was 15.4% (4/26) in the lower group but 50% (20/40, P=0.008) in the higher group. The 90-day mortality rate was also lower in the lower group (5/26, 19.2%) than in the higher group (33/40, 82.5%, P<0.001). Additionally, survival was examined by the Kaplan–Meier analysis. The log-rank test revealed significant differences between the higher group and the lower group in both the 30-day (chi-square=8.545, P=0.0035) and 90-day (chi-square=23.98, P<0.0001; ) survival rate. Collectively, these data suggested that an increased frequency of Tc17 cells could be a useful predictor of mortality in patients with HBV-ACLF.
Increased Tc17 cell frequency at admission could be an independent predictor of mortality
Baseline clinical and laboratory variables were analyzed as possible predictors of mortality. The basic characteristics of surviving and non-surviving patients with HBV-ACLF are summarized in . Compared with surviving patients, non-surviving patients were older, were more likely to be female, had higher levels of Tc17 cells and Tbil, had lower levels of PTA, and were more likely to be cirrhotic at baseline (). Next, the Cox regression analysis was used to identify predictors for HBV-ACLF. In the univariate analysis, female sex, cirrhosis, Tc17 cell frequency, Tbil levels, PTA levels, MELD score, MELD-Na score, and CLIF-C ACLF score were factors associated with a higher risk of mortality (). Next, we evaluated these significant variables in a multivariate Cox regression analysis by using forward stepwise (likelihood ratio) selection. Only female sex (HR=5.450, P<0.001), Tc17 cell frequency (HR=1.401, P=0.001), and MELD-Na score (HR=1.344, P<0.001) were found to be independent baseline predictors of mortality in patients with HBV-ACLF ().
Table 2 Characteristics of patients with HBV-ACLF according to clinical outcome
Table 3 Factors associated with mortality in patients with HBV-ACLF by using the Cox regression analysis
Tc17 cell frequency was positively correlated with serum IL-17A and IL-22 levels
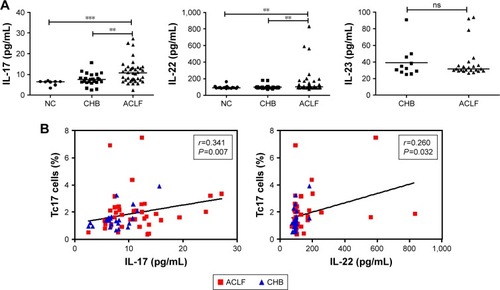
Finally, we determined the serum levels of cytokines (IL-17A, IL-22, and IL-23) in NC subjects (N=17), patients with CHB (N=30), and patients with HBV-ACLF (N=38) by a FlowCytomix assay. IL-22 was detected in all three groups. IL-17A was detected in 38 patients with HBV-ACLF (100%), 23 patients with CHB (77%), and 8 NC subjects (47%). However, only 11 patients with CHB (37%) and 23 patients with HBV-ACLF (60%) had detectable IL-23, while IL-23 was not detectable in the NC subjects. Moreover, IL-17A levels were higher in patients with HBV-ACLF (median 10.81, range 2.50–27.18 pg/mL) than in patients with CHB (7.65±2.95 pg/mL, P=0.004) and NC subjects (median 6.47, range 3.45–7.01 pg/mL, P<0.001). In addition, IL-22 levels were higher in patients with HBV-ACLF (median 101.16, range 73.20–832.31 pg/mL) than in patients with CHB (median 94.68, range 73.20–181.59 pg/mL, P=0.004) and NC subjects (median 91.24, range 82.47–163.8 pg/mL, P=0.002). However, IL-23 levels did not differ between patients with HBV-ACLF (median 31.70, range 26.56–93.92 pg/mL) and patients with CHB (median 32.16, range 25.07–90.74 pg/mL, P=0.892; ). Next, correlations between the expression of Tc17 cells and these cytokines in HBV-infected patients were examined. Interestingly, positive correlations were found between the frequency of Tc17 cells and the levels of both IL-17A (r=0.341, P=0.007) and IL-22 (r=0.260, P=0.032; ). However, no correlation was found between Tc17 cell frequency and IL-23 level (r=0.030, P=0.867). These data indicated that Tc17 cells may represent an additional source of IL-17 in HBV-infected patients.
Figure 4 Tc17 cell frequency was positively correlated with serum IL-17A and IL-22 levels.
Abbreviations: ACLF, acute-on-chronic liver failure; CHB, chronic hepatitis B; HBV, hepatitis B virus; NC, normal control; ns, not significant; Tc17, IL-17-producing CD8+ T.
Discussion
Although the pathogenic role of Tc17 cells has been explored in inflammatory diseases and tumors, much less is known about the role of Tc17 cells in patients with HBV-ACLF. To our knowledge, this study is the first to extensively determine the role of Tc17 cells in patients with HBV-ACLF. We present evidence that Tc17 cells increase in frequency and participate in the pathogenesis of HBV-ACLF. Furthermore, this study is the first to demonstrate that an increased frequency of Tc17 cells predicts poor overall patient survival. Additionally, Tc17 cell frequency is shown to be an independent prognostic factor by the multivariate Cox regression analysis.
Tc17 cells were found to be enriched in patients with chronic hepatitis CCitation13,Citation14 and hepatocellular carcinomas.Citation21 These data indicate that Tc17 cells may contribute to immune-mediated inflammation. Thus, we hypothesized that Tc17 cells may be involved in the process of HBV-induced liver injury. A previous report showed that Tc17 cells were enriched in HBeAg-positive patients with CHB as compared to those in healthy individuals, but the difference was not significant.Citation22 However, we showed that the frequency of Tc17 cells was increased significantly in patients with CHB as compared to that in NC subjects (P=0.019). This discrepancy could be explained by the different disease status of patients enrolled in this study (a greater proportion of HBeAg-negative and deteriorated patients were chosen). Moreover, Tc17 cell frequency was closely correlated with Tbil, PTA, AST, and ALB levels, indicating that Tc17 cells were associated with liver injury.
Knowledge about the implication of Tc17 cells in the pathogenesis of HBV-ACLF is currently limited. Therefore, the role of Tc17 cells in HBV-ACLF was extensively explored. Consistent with our hypothesis, our results indicate that an increased frequency of Tc17 cells is associated with liver injury in patients with HBV-ACLF. Substantial evidence supports this hypothesis. First, we demonstrated that patients with HBV-ACLF had higher levels of Tc17 cells than patients with CHB (P=0.002) and NC subjects (P<0.001) and that Tc17 cell frequency was positively correlated with Tbil and AST levels but was negatively correlated with PTA and ALB levels (all P<0.05), which are often used as markers of liver injury.Citation23 Additionally, the frequency of Tc17 cells was higher in non-surviving patients with HBV-ACLF than in surviving patients (P<0.001). More importantly, Tc17 cell frequency was positively correlated with MELD, MELD-Na, and CLIF-C ACLF scores (all P<0.05). Collectively, these results indicate that Tc17 cells may play a proinflammatory role in the pathogenesis of HBV-ACLF.
Researchers reported that intratumoral Tc17 cells increased with tumor progression and were associated with overall survival time in gastric cancer.Citation24 Additionally, another report showed that peripheral Tc17 cells were negatively correlated with the 5-year survival rate for patients with head and neck cancer.Citation25 These studies indicate a clinical prognostic value of Tc17 cells. This study is the first to demonstrate that Tc17 cell frequency can be used to predict the prognosis of patients with HBV-ACLF. Indeed, we found that higher levels of Tc17 cells were associated with poorer clinical outcomes. Moreover, the ROC curve analysis showed that Tc17 cell frequency predicted 90-day survival with an accuracy equivalent to that of MELD, MELD-Na, and CLIF-C ACLF scores (all P>0.05). The Kaplan–Meier analysis revealed that Tc17 cell enrichment was associated with poor overall survival. Additionally, the multivariate Cox regression analysis suggested that Tc17 cell frequency was an independent predictor of overall survival in patients with HBV-ACLF. Taken together, these data strongly indicated that peripheral Tc17 cells could serve as a prognostic biomarker. Moreover, Tc17 cell frequency was inversely correlated with survival, suggesting that the frequency of circulating Tc17 cells may be an indicative factor to guide further treatment decisions. If validated in the future, Tc17 cell frequency measured by a simple and accessible technique could be a prognostic biomarker to identify patients at risk of death.
IL-17 is a key pathogenic cytokine in liver diseases.Citation26 Although Th17 cells are thought to be the main producer of IL-17, other immune cells can also produce IL-17. Hence, the identification of all potential IL-17 sources in HBV-ACLF is important. Tc17 cells are defined by their ability to produce IL-17; in addition, Tc17 cells coexpress other cytokines, including IFN-gamma and TNF-alpha.Citation10 In our study, IL-17A and IL-22 levels were higher in patients with HBV-ACLF than in patients with CHB and NC subjects. Moreover, the frequencies of Tc17 cells were positively correlated with IL-17A and IL-22 levels (both P<0.05). These data indicate that Tc17 cells may represent an additional source of IL-17 in HBV-infected patients.
The similarity of the cytokine profile of Tc17 cells to that of Th17 cells provides a basis for using Th17 cell differentiation conditions to expand Tc17 cells. For example, IL-23 is often used to expand human Th17 cells.Citation27 In mice, IL-23 induced IL-17 expression only slightly and maintained the Tc17 cell phenotype.Citation28,Citation29 However, the role of IL-23 in human Tc17 cells is not yet clarified. In the present study, no significant correlation was found between Tc17 cell frequency and IL-23 levels, indicating that the role of IL-23 in Tc17 cell differentiation may differ from its role in Th17 cells. Thus, further investigations are required to confirm the role of IL-23 in Tc17 cells in humans.
This study has some limitations. First, our sample size was relatively small. Moreover, the present study was a single-center investigation in China. The findings need to be confirmed in large multicenter and prospective studies.
Conclusion
Our findings demonstrate that Tc17 cells are preferentially enriched in patients with HBV-ACLF and that this increase positively correlates with liver injury and disease severity. Thus, Tc17 cells may play a proinflammatory role in the pathogenesis of HBV-ACLF. Furthermore, our data indicate that an increased frequency of circulating Tc17 cells could be an independent predictor of mortality in patients with HBV-ACLF. Therefore, future therapeutic strategies aimed at interfering with Tc17 cell pathways may benefit patients with HBV-ACLF.
Availability of data
The datasets used or analyzed during the current study are available from the first author (Geng-lin Zhang) on reasonable request.
Author contributions
All authors contributed toward data analysis, drafting and critically revising the paper and agree to be accountable for all aspects of the work.
Abbreviations
| AFP | = | alpha-fetoprotein |
| ACLF | = | acute-on-chronic liver failure |
| ALB | = | albumin |
| ALT | = | alanine aminotransferase |
| AST | = | aspartate aminotransferase |
| AUROC | = | area under the ROC curve |
| CHB | = | chronic hepatitis B |
| CLIF-C | = | chronic liver failure consortium |
| HBV | = | hepatitis B virus |
| HCV | = | hepatitis C virus |
| MELD | = | model for end-stage liver disease |
| NC | = | normal control |
| PTA | = | prothrombin time activity |
| ROC curve | = | receiver operating characteristic curve |
| Tbil | = | total bilirubin |
| Tc17 | = | IL-17-producing CD8+ T |
Acknowledgments
The authors thank all individuals in this study. The manuscript has been edited and proofread by a medical editor, a native English speaker from American Journal Experts. This study was supported by grants from the National Science and Technology Major Project (2018Z × 10302204–002), National Natural Science Foundation of China (81672701), Guangdong Province Medical Research (A2017048), and Guangzhou Science and Technology Project (201508020118, 2014Y2-00544).
Disclosure
The authors report no conflicts of interest in this work.
References
- BernalWJalanRQuagliaASimpsonKWendonJBurroughsAAcute-on-chronic liver failureLancet2015386100031576158726423181
- WangFSZhangZLiver: How can acute-on-chronic liver failure be accurately identified?Nat Rev Gastroenterol Hepatol201310739039123609466
- SetoWKLaiCLYuenMFAcute-on-chronic liver failure in chronic hepatitis BJ Gastroenterol Hepatol201227466266922098452
- ClàriaJStauberRECoenraadMJSystemic inflammation in decompensated cirrhosis: Characterization and role in acute-on-chronic liver failureHepatology20166441249126427483394
- WuWYanHZhaoHCharacteristics of systemic inflammation in hepatitis B-precipitated ACLF: Differentiate it from No-ACLFLiver Int201838224825728646630
- TesmerLALundySKSarkarSFoxDATh17 cells in human diseaseImmunol Rev20082238711318613831
- KondoTTakataHMatsukiFTakiguchiMCutting edge: Phenotypic characterization and differentiation of human CD8+ T cells producing IL-17J Immunol200918241794179819201830
- HuberMHeinkSGrotheHA Th17-like developmental process leads to CD8(+) Tc17 cells with reduced cytotoxic activityEur J Immunol20093971716172519544308
- LiangYPanHFYeDQTc17 Cells in Immunity and Systemic AutoimmunityInt Rev Immunol201534431833125259411
- SrenathanUSteelKTaamsLSIL-17+ CD8+ T cells: Differentiation, phenotype and role in inflammatory diseaseImmunol Lett2016178202627173097
- MajchrzakKNelsonMHBaileySRExploiting IL-17-producing CD4+ and CD8+ T cells to improve cancer immunotherapy in the clinicCancer Immunol Immunother201665324725926825102
- HamadaHGarcia-HernandezMLReomeJBTc17, a unique subset of CD8 T cells that can protect against lethal influenza challengeJ Immunol200918263469348119265125
- BillerbeckEKangYHWalkerLAnalysis of CD161 expression on human CD8+ T cells defines a distinct functional subset with tissue-homing propertiesProc Natl Acad Sci U S A201010773006301120133607
- OoYHBanzVKavanaghDCXCR3-dependent recruitment and CCR6-mediated positioning of Th-17 cells in the inflamed liverJ Hepatol20125751044105122796894
- SarinSKKumarAAlmeidaJAAcute-on-chronic liver failure: consensus recommendations of the Asian Pacific Association for the study of the liver (APASL)Hepatol Int20093126928219669378
- ZhangGLXieDYLinBLImbalance of interleukin-17-producing CD4 T cells/regulatory T cells axis occurs in remission stage of patients with hepatitis B virus-related acute-on-chronic liver failureJ Gastroenterol Hepatol201328351352123215950
- PengLXieDYLinBLAutologous bone marrow mesenchymal stem cell transplantation in liver failure patients caused by hepatitis B: short-term and long-term outcomesHepatology201154382082821608000
- KimWRBigginsSWKremersWKHyponatremia and mortality among patients on the liver-transplant waiting listN Engl J Med2008359101018102618768945
- JalanRSalibaFPavesiMCANONIC study investigators of the EASL-CLIF Consortium. Development and validation of a prognostic score to predict mortality in patients with acute-on-chronic liver failureJ Hepatol20146151038104724950482
- SarinSKChoudhuryAManagement of acute-on-chronic liver failure: an algorithmic approachHepatol Int Epub2018816
- KuangDMPengCZhaoQTumor-activated monocytes promote expansion of IL-17-producing CD8+ T cells in hepatocellular carcinoma patientsJ Immunol201018531544154920581151
- LiJShiJRenWWuWChenZRegulatory role of CD4(+)CD25 (+) Foxp3(+) regulatory T cells on IL-17-secreting T cells in chronic hepatitis B patientsDig Dis Sci20145971475148324442238
- RehermannBNascimbeniMImmunology of hepatitis B virus and hepatitis C virus infectionNat Rev Immunol20055321522915738952
- ZhuangYPengLSZhaoYLCD8(+) T cells that produce interleukin-17 regulate myeloid-derived suppressor cells and are associated with survival time of patients with gastric cancerGastroenterology20121434951962.e822710190
- LeeMHTung-Chieh ChangJLiaoCTChenYSKuoMLShenCRInterleukin 17 and peripheral IL-17-expressing T cells are negatively correlated with the overall survival of head and neck cancer patientsOncotarget20189119825983729515773
- HammerichLHeymannFTackeFRole of IL-17 and Th17 cells in liver diseasesClin Dev Immunol2011201134580321197451
- StockingerBOmenettiSThe dichotomous nature of T helper 17 cellsNat Rev Immunol201717953554428555673
- CurtisMMWaySSWilsonCBIL-23 promotes the production of IL-17 by antigen-specific CD8 T cells in the absence of IL-12 and type-I interferonsJ Immunol2009183138138719542449
- El-BehiMDaiHMagalhaesJGCommitted Tc17 cells are phenotypically and functionally resistant to the effects of IL-27Eur J Immunol201444103003301425070084