
Abstract
Background
Despite great advances in aseptic surgical techniques, surgical site infection (SSI) is still one of the main complications after spine surgery. SSI can bring tremendous physical, psychological, and economic challenges to patients. Intrawound vancomycin application is a much disputed method for the prevention of SSI after spine surgery.
Objective
The aim of this study is to review the current literature for studies on the intra-wound application of vancomycin powder and to analyze its effectiveness in the prevention of postoperative SSI.
Methods
PubMed, Medline, Elsevier, and CNKI were searched for the key words “vancomycin”, “local/intraoperative/topical/intra-wound”, “spine/spinal/lumbar/cervical/thoracolumbar surgery”, “infection”, and “SSI” in published studies on the effectiveness of intrawound vancomycin application to prevent postoperative SSI. RevMan 5.3 was used to compare the data extracted from the studies included.
Results
A total of 27 studies involving 17,321 patients were included in the final analysis. Among those patients, 7,423 patients were treated with vancomycin to prevent SSI, with 9,898 in control groups. SSI incidence after surgery in experimental groups was 0.39 times as high as control groups, and this difference was statistically significant (P<0.01). Among patients who underwent internal fixation, vancomycin application significantly reduced the incidence of postoperative SSI (OR 0.31 95% CI 0.19–0.50; P<0.01). Meanwhile, vancomycin did not affect SSI incidence in patients who did not receive internal fixation (P=0.17) or received deformity correction (P=0.25).
Conclusion
SSI incidence after spinal surgery can be significantly reduced by intrawound application of vancomycin in most circumstances. This method can be applied in various spinal procedures involving instrumentation to prevent postoperative SSI.
Background
Despite highly developed intraoperative aseptic techniques, postoperative surgical site infection (SSI) is still one of the most common complications of spine surgery. In the current literature, SSI incidence after spine surgery ranges 2%–13%.Citation1,Citation2 In US, there are half a million patents with SSI, and the direct cost for treatment is as high as $1.8 billion annually.Citation3 For patients, SSI brings about an average of 2 weeks longer in hospital, higher medical bills, and increased likelihood of disability, mortality, and physical and physiological pressure.Citation4
Now that SSI prevention is one of the main requirements of high-standard medical centers, numerous techniques and guidelines have been developed to avoid it.Citation5,Citation6 After Buchholz et alCitation41 applied antibiotics at the site of surgery to prevent SSI and gained satisfying results, a variety of antibiotics were tried regionally for the same purposes.Citation7,Citation8 In consideration of the fact that the main pathogens in SSI are Staphylococcus aureus and Staphylococcus epidermidis and that vancomycin can eliminate both, its local application may significantly decrease SSI after spinal surgery. In the last decade, there have been numerous studies on the local application of vancomycin powder on the surgical site, but results of those studies are controversial. As such, the current study was carried out to assess the results of those studies and provide guidance for future clinical practice.
Methods
Literature search
Two independent reviewers carried out computerized search of the databases PubMed (2005–2018), Medline (2005–2018), Embase (2005–2018), Elsevier (2005–2018), Cochrane library (2008–2018), and CNKI (2005–2018) with the MeSH words “vancomycin”, “local/intraoperative/topical/intra-wound”, “spine/spinal/lumbar/cervical/thoracolumbar surgery”, “infection”, and “SSI”. Where the two authors disagreed on whether studies had met the inclusion criteria, a neutral scholar was invited to settle the disputes. Two authors independently assessed the quality of the studies included with the Newcastle–Ottawa Scale (NOS).Citation9
Data extraction
Data from the trails were extracted by two independent reviewers. The authors of each study, study design, sample size, patient age, time of study, and intervention methods were extracted as basic demographic data. Overall patient numbers, number of patients who had had vancomycin applied regionally to prevent postoperative SSI, and number of patients with SSI were recorded as outcome parameters. In cases where the same patients were analyzed in more than one study, they were extracted and analyzed as one patient population.
Analysis
Data were analyzed and processed using RevMan 5.3 (Cochrane Collaboration, Oxford, UK). Two authors checked data input to make sure that no errors were made. Studies were considered to have significant heterogeneity if I2>50%, in which case random-effect analysis was performed on the study data. Differences in each study were defined by OR with 95% CI for categorical outcome frequencies in study groups and control groups. ORs for all trials are shown in forest plots.
Results
Study selection
Among a total of 1,715 studies, 27 studiesCitation10–Citation36 comparing the effectiveness of vancomycin in preventing SSI after spine surgery were included in the final analysis. Those studies reported the outcome of 17,321 patients with or without the regional application of vancomycin after spinal surgery. Vancomycin was applied in 7,423 of those patients and not applied in 9,898 patients (; ).
Figure 1 Selection of papers for this research. A total of 27 studies were included in the final analysis.
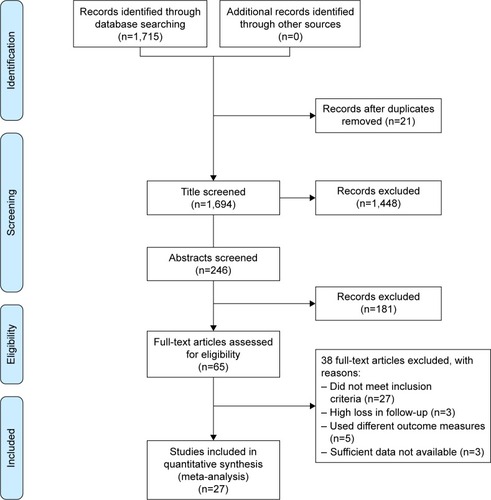
Table 1 Demographic characteristics of included studies
In the 27 studies included, two were randomized controlled trials (RCTs) and the remaining were retrospective cohort studies. They were carried out between 2011 and 2018 and mostly between 2013 and 2015. The level of evidence in studies was 2–3, with NOS scores of 5–7 ().
Overall analysis
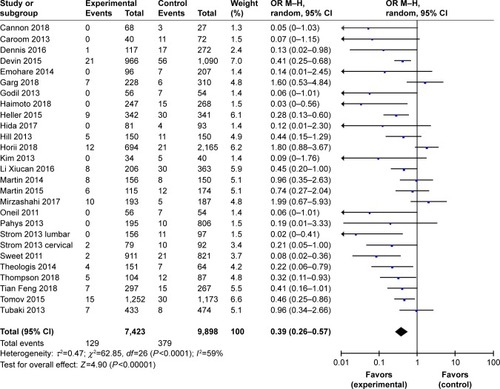
The meta-analysis on the overall effect of vancomycin on SSI included a total number of 17,321 patients. Vancomycin was applied in 7,423 of those patients, while vancomycin was not applied in 9,898 patients. Random-effect analysis was carried out because I2>50%. Results of the meta-analysis indicated that SSI incidence in control groups (no vancomycin) was 2.56 times as high as in experimental groups (vancomycin applied locally during surgery). The difference was significant between the groups (P<0.01; ).
Figure 2 Overall surgical site infection incidence was significantly low when vancomycin was applied locally after surgery (P<0.01).
Subgroup analysis according to the study design
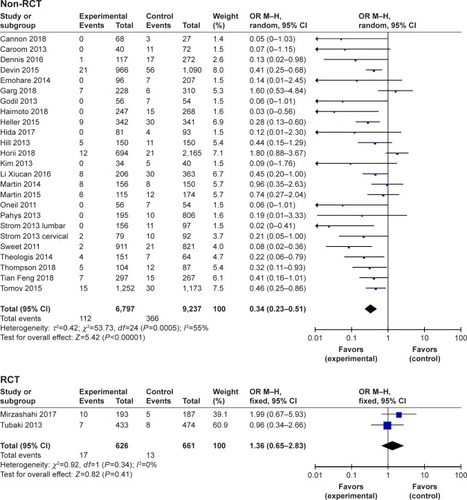
In consideration of the fact that results of RCTs may have less patient selection bias than retrospective studies, here, we meta-analyzed the data by RCTs and retrospective studies separately. In the current literature, there are only two RCTs: studies by Tukabi et al and Mirzashahi et al. Those studies included a total of 1,287 patients, and meta-analysis indicated that SSI incidence in vancomycin groups was 1.36 times as high as in control groups (95% CI 0.65–2.83), but this difference was not significant (P=0.41). Meanwhile, meta-analysis of 25 retrospective studies with 16,034 patients indicated that SSI incidence in vancomycin groups was 0.34 times as high as in the control group (95% CI 0.23–0.51), and this difference was significant (P<0.01; ). Given that neither of the RCTs provided a trial registration number and both were carried out in a single study center, the quality control status of those RCTs may be questionable. More multicenter RCTs with strict quality control are necessary to reach a more reliable result.
Figure 3 Meta-analysis of randomized controlled trials (RCTs) and retrospective studies.
Subgroup analysis according to the application of internal fixation
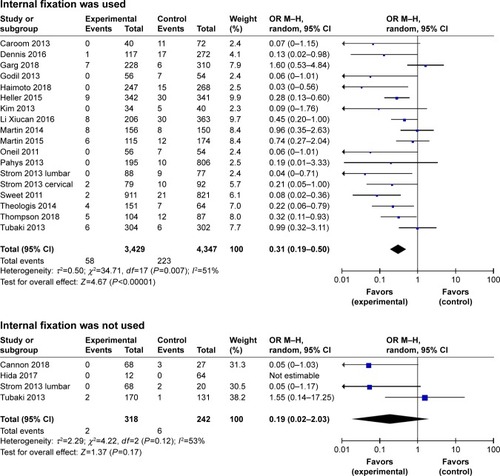
In consideration of the fact that patients with internal fixation may face higher likelihood of SSI after surgery, in the current study, we analyzed patients who underwent internal fixation and those who did not separately. In the 18 studies included in this analysis, 7,776 patients received internal fixation. Meta-analysis indicated that SSI incidence in vancomycin groups is 0.31 times as high as control groups (95% CI 0.19–0.50), and this difference was significant (P<0.01). The analysis of four studies including 560 patients indicated that when no instrumentation was applied, SSI incidence in vancomycin groups was 0.19 times as high as in control groups (95% CI 0.02–2.03), but this difference was not significant (P=0.12). This indicated that the local application of vancomycin may not affect SSI incidence in patients with no internal fixation ().
Figure 4 Local application of vancomycin reduced surgical site infections after surgery irrespective of whether internal fixation was used.
Subgroup analysis of deformity correction or nondeformity correction surgery
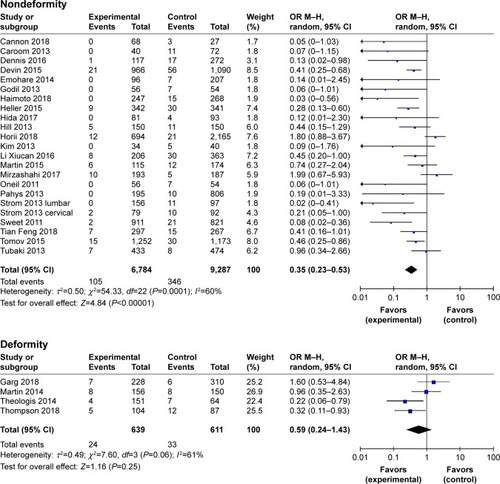
Patients who undergo deformity correction surgery always have to endure longer operations, more intraoperative hemorrhage, and more implants than in conventional spine surgeries. All those factors can increase the possibility of postoperative SSI. In the current study, four studies including 1,250 subjects were on patients who underwent spinal deformity correction. Meta-analysis of these studies showed that in spinal deformity surgeries, the SSI possibility in vancomycin groups was 0.59 times as much as no-vancomycin groups (95% CI 0.24–0.1.43), but this difference was not significant (P=0.06). Meanwhile, meta-analysis of 23 studies with 16,071 patients who did not underwent spinal deformity-correction surgery showed that vancomycin group has 0.35 times as much SSI possibility as no-vancomycin group (95% CI 0.23–0.53). This difference was significant (P<0.01; ).
Figure 5 Local application of vancomycin reduced surgical site infections after surgery in both spinal deformity surgeries and nondeformity surgeries.
Subgroup analysis depending on the site of surgery
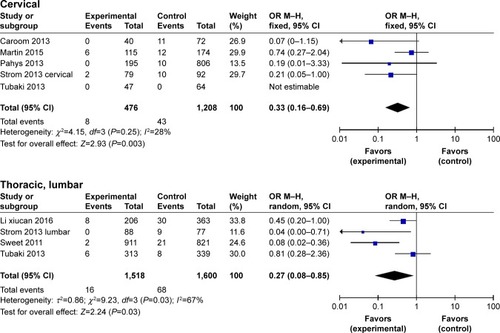
In consideration of the fact that there could be differences in SSI incidence in patients undergoing cervical, thoracic, or lumbar surgery, in the current study, we analyzed patients who received surgical treatment on cervical, thoracic, or lumbar region separately. Given that the studies included did not provide adequate information on patients receiving thoracic spine surgery and that most surgeries carried out on the thoracic region also involve the thoracolumbar junction, in the current study, we analyzed the data of thoracic and lumbar regions as a whole. Among the studies included, five studies with 1,684 patients received surgical treatment in the cervical region. Meta-analysis indicated that SSI incidence in vancomycin groups was 0.33 times as high as control groups (95% CI 0.16–0.69), and this difference was significant (P<0.01). The analysis of four studies including 3,118 patients who received surgical treatment in the thoracic and lumbar regions indicated that SSI incidence in vancomycin groups was 0.27 times as high as control groups (95% CI 0.08–0.85), and this difference was also significant (P=0.03). This indicated that local application of vancomycin can significantly reduce SSI incidence in patients who receive surgical treatment in the cervical, thoracic, or lumbar region ().
Figure 6 Local application of vancomycin significantly reduced surgical site infection incidence in patients who received cervical, thoracic, or lumbar surgical treatment.
Effect of vancomycin on deep and superficial infection after spine surgery
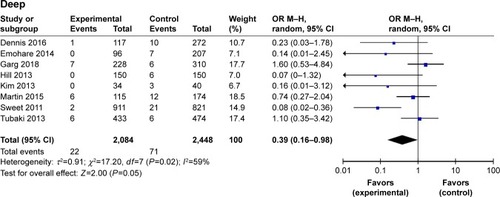
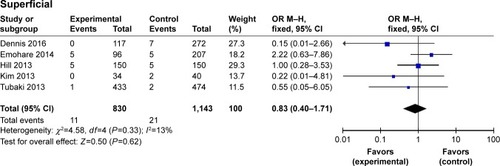
In consideration of the fact that deep and superficial infections after spine surgery require different treatment options and have different outcomes, we analyzed the incidence of deep and superficial infections between the two groups. Eight studies including 4,532 patients analyzed the incidence of deep tissue infection after spinal surgery, which was lower in the vancomycin group than in the no-vancomycin group (OR =0.39, 95% CI 0.16–0.98; P=0.05). In the meanwhile, the analysis of five studies including 1,973 patients revealed that application of vancomycin did not significantly reduce the incidence of superficial wound infection (OR 0.83, 95% CI 0.40–1.71; P=0.62; ).
Figure 7 Subgroup analysis of incidence of deep (upper) and superficial (lower) tissue infections after spinal surgeries.
Discussion
With advances in aseptic surgical techniques, postoperative SSI incidence is gradually decreasing. However, SSI is still one of the most common surgery-related complications. In the current literature, the incidence of SSI is as high as 10%.Citation37 Risk factors for SSI include being overweight, overage, diabetes, smoking, poor overall physical condition, implant application, long surgery, and voluminous hemorrhage.Citation38
Vancomycin has been proven to be effective in reducing postoperative SSI in patients undergoing arthroplasty.Citation39 Intravenous application of vancomycin can affect liver and kidney functions. Compared to intravenous drug delivery, local application of vancomycin powder can reach high doses specific to the surgical region, avoiding injury to healthy organs.Citation40 Therefore, regional application of vancomycin powder may reduce SSI after spine surgery without causing serious harmful effects to vital organs. In the last two decades, vancomycin has been applied in several medical centers. However, the results are controversial. The current research was carried out to assess the published studies and provide more reliable information for future clinical work.
In our literature research, we found 27 studies including 17,321 patients on the effectiveness and safety of vancomycin. This is the meta-analysis with the largest participant base so far. Result of the current meta-analysis showed that the regional application of vancomycin could reduce SSI incidence to approximately one-third (OR 0.39) of that when vancomycin was not applied. The difference between the two groups was significant (P<0.00001).
17,321 patients received a variety of surgical treatments, including spinal deformity surgery and common surgery with or without internal fixation. In consideration of the fact that different treatment measures may react differently to the application of vancomycin, we analyzed patients by the surgical treatment they received. Vancomycin was proven to be effective in reducing SSI after all varieties of spinal surgeries, except when instrumentation was not applied (P=0.17) and in deformity correction surgery (P=0.25). However, because of the vague information in most publications, there were only four studies with 560 patients that reported not using any implants, and only eight of those patients suffered from SSI. On the other hand, there were 7,776 patients in 18 studies in the meta-analysis showing that the application of vancomycin can significantly reduce SSI after spine surgery (OR 0.31, 95% CI 0.19–0.50). These results indicate that in patients with no instrumentation, it may not be necessary to use vancomycin to prevent SSI, but still more data can be used to solidify this conclusion.
Similarly, there were only four studies with 1,250 patients leading to the conclusion that vancomycin may not help to decrease SSI in deformity correction surgery. This result could change with more data from the studies that had strict design and large sample. It can also be seen from the current research that although the incidence of deep wound infection may be influenced by the application of vancomycin (OR 0.39, 95% CI 0.16–0.98; P=0.05), the incidence of superficial wound infection may not be influenced by the application of vancomycin (OR 0.83, 95% CI 0.40–1.71; P=0.62). However, since deep wound infection can be much more harmful to patients and more difficult to treat, it is still plausible to use vancomycin intraoperatively to prevent SSI.
The current study has several disadvantages. Among the 27 included studies, only two studies were RCTs, with the rest being retrospective cohort studies. Most studies included 300–1,000 patients, with four exceptional studies with >1,000 participants. Considering that NOS scores of those studies were mostly 6–7, we included them in the data extraction process and used random-effect analysis when I2>50%. Therefore, we believe the final data are still meaningful for clinical practice. However, due to the study design in most retrospective studies, there were few patients with no-instrumentation treatment. Results of the meta-analysis may change with more RCTs with more strict design and execution.
Conclusion
SSI incidence after spinal surgery can be significantly reduced by intrawound application of vancomycin in most circumstances. This method can be applied with instrumentation in various clinical settings of spine practice, except for no-instrumentation surgery, to prevent postoperative SSI.
Disclosure
The authors alone are responsible for the content and writing of the article. The authors report no conflicts of interest in this work.
References
- BakhsheshianJDahdalehNSLamSKSavageJWSmithZAThe use of vancomycin powder in modern spine surgery: systematic review and meta-analysis of the clinical evidenceWorld Neurosurg201583581682325535069
- KhanNRThompsonCJDeCuypereMA meta-analysis of spinal surgical site infection and vancomycin powderJ Neurosurg Spine201421697498325259555
- AwadSSAdherence to surgical care improvement project measures and post-operative surgical site infectionsSurg Infect (Larchmt)201213423423722913334
- McGirtMJGodilSSReduction of surgical site infection in spine surgery: an opportunity for quality improvement and cost reductionSpine J20131391030103124029137
- OlsenMANeppleJJRiewKDRisk factors for surgical site infection following orthopaedic spinal operationsJ Bone Joint Surg Am20089016269
- SavageJWAndersonPAAn update on modifiable factors to reduce the risk of surgical site infectionsSpine J20131391017102923711958
- KanjWWFlynnJMSpiegelDADormansJPBaldwinKDVancomycin prophylaxis of surgical site infection in clean orthopedic surgeryOrthopedics201336213814623379827
- MohammedSPisimisisGTDaramSPImpact of intraoperative administration of local vancomycin on inguinal wound complicationsJ Vasc Surg20135741079108323313181
- StangACritical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analysesEur J Epidemiol201025960360520652370
- HeyHWThiamDWKohZSIs Intraoperative Local Vancomycin Powder the Answer to Surgical Site Infections in Spine Surgery?Spine (Phila Pa 1976)201742426727428207669
- DevinCJChotaiSMcGirtMJIntrawound vancomycin decreases the risk of surgical site infection after posterior spine surgery: a multicenter analysisSpine (Phila Pa 1976)2018431657126656042
- EmohareOLedonioCGHillBWDavisRAPollyDWJrKangMMCost savings analysis of intrawound vancomycin powder in posterior spinal surgerySpine J201414112710271524650851
- GodilSSParkerSLO’NeillKRDevinCJMcGirtMJComparative effectiveness and cost-benefit analysis of local application of vancomycin powder in posterior spinal fusion for spine trauma: clinical articleJ Neurosurg Spine201319333133523848350
- HaimotoSSchärRTNishimuraYHaraMWakabayashiTGinsbergHJReduction in surgical site infection with suprafascial intrawound application of vancomycin powder in instrumented posterior spinal fusion: a retrospective case-control studyJ Neurosurg Spine201829219319829726801
- HellerAMcIffTELaiSMBurtonDCIntrawound vancomycin powder decreases staphylococcal surgical site infections after posterior instrumented spinal arthrodesisJ Spinal Disord Tech20152810E584E58924189484
- HidaTAndoKKobayashiKIntrawound Vancomycin powder as the prophylaxis of surgical site infection after invasive spine surgery with a high risk of infectionNagoya J Med Sci201779454555029238110
- HillBWEmohareOSongBDavisRKangMMThe use of vancomycin powder reduces surgical reoperation in posterior instrumented and noninstrumented spinal surgeryActa Neurochir (Wien)2014156474975424570187
- HoriiCYamazakiTOkaHDoes intrawound vancomycin powder reduce surgical site infection after posterior instrumented spinal surgery? A propensity score-matched analysisSpine J Epub2018426
- KimHSLeeSGKimWKParkCWSonSProphylactic intrawound application of vancomycin powder in instrumented spinal fusion surgeryKorean J Spine201310312112524757472
- MartinJRAdogwaOBrownCRExperience with intrawound vancomycin powder for posterior cervical fusion surgeryJ Neurosurg Spine2015221263325380539
- MartinJRAdogwaOBrownCRExperience with intrawound vancomycin powder for spinal deformity surgerySpine (Phila Pa 1976)201439217718424158179
- O’NeillKRSmithJGAbtahiAMReduced surgical site infections in patients undergoing posterior spinal stabilization of traumatic injuries using vancomycin powderSpine J201111764164621600853
- PahysJMPahysJRChoSKMethods to decrease postoperative infections following posterior cervical spine surgeryJ Bone Joint Surg Am201395654955423515990
- StromRGPacioneDKalhornSPFrempong-BoaduAKLumbar laminectomy and fusion with routine local application of vancomycin powder: decreased infection rate in instrumented and non-instrumented casesClin Neurol Neurosurg201311591766176923622935
- StromRGPacioneDKalhornSPFrempong-BoaduAKDecreased risk of wound infection after posterior cervical fusion with routine local application of vancomycin powderSpine (Phila Pa 1976)2013381299199423324930
- SweetFARohMSlivaCIntrawound application of vancomycin for prophylaxis in instrumented thoracolumbar fusions: efficacy, drug levels, and patient outcomesSpine (Phila Pa 1976)201136242084208821304438
- TheologisAADemirkiranGCallahanMPekmezciMAmesCDevirenVLocal intrawound vancomycin powder decreases the risk of surgical site infections in complex adult deformity reconstruction: a cost analysisSpine (Phila Pa 1976)201439221875188025077909
- ThompsonGHPoe-KochertCHardestyCKSon-HingJMistovichRJDoes Vancomycin Powder Decrease Surgical Site Infections in Growing Spine Surgery?: A Preliminary StudyJ Bone Joint Surg Am2018100646647129557862
- TomovMMitsunagaLDurbin-JohnsonBNallurDRobertoRReducing surgical site infection in spinal surgery with betadine irrigation and intrawound vancomycin powderSpine (Phila Pa 1976)201540749149925608241
- TubakiVRRajasekaranSShettyAPEffects of using intravenous antibiotic only versus local intrawound vancomycin antibiotic powder application in addition to intravenous antibiotics on postoperative infection in spine surgery in 907 patientsSpine (Phila Pa 1976)201338252149215524048091
- CaroomCTullarJMBentonEGJrJonesJRChaputCDIntrawound vancomycin powder reduces surgical site infections in posterior cervical fusionSpine (Phila Pa 1976)201338141183118723474597
- MirzashahiBChehrassanMMortazaviSMJIntrawound application of vancomycin changes the responsible germ in elective spine surgery without significant effect on the rate of infection: a randomized prospective studyMusculoskelet Surg201810213539
- LiXCQinYXuxuanWWangXXThe effect of local application of vancomycin powder after posterior lumbar interbody fusion surgery on prevention of surgical site infection and fusion rateChin J Spine Spinal Cord2016261211091114
- FengTYangYEffects observation of local intrawound application vancomycin in prevention surgical site infection after the spine surgeriesJ Clin Orthop2018212157159
- CannonJGDHoALMoholeJTopical vancomycin for surgical prophylaxis in non-instrumented pediatric spinal surgeriesChilds Nerv Syst2018515
- GargSBlochNPotterMTopical vancomycin in pediatric spine surgery does not reduce surgical site infection: a retrospective cohort studySpine Deform20186552352830122387
- SassoRCGarridoBJPostoperative spinal wound infectionsJ Am Acad Orthop Surg200816633033718524984
- GeromettaARodriguez OlaverriJCBitanFInfections in spinal instrumentationInt Orthop201236245746422218913
- SalehAKhannaAChaginKMKlikaAKJohnstonDBarsoumWKGlycopeptides versus β-lactams for the prevention of surgical site infections in cardiovascular and orthopedic surgery: a meta-analysisAnn Surg20152611728025119119
- EvaniewNKhanMDrewBPetersonDBhandariMGhertMIntrawound vancomycin to prevent infections after spine surgery: a systematic review and meta-analysisEur Spine J201524353354224838506
- BuchholzHWElsonRAEngelbrechtEManagement of deep infection of total hip replacementJ Bone Joint Surg Br19816333423537021561