
Abstract
Objective
This study analyzed metabolic factors associated with lymphovascular space invasion (LVSI) and compared the difference between type 1 and type 2 endometrial cancer (EC).
Methods
Four hundred patients primarily diagnosed with EC who underwent hysterectomy with pathological results at Fujian Medical University Cancer Hospital from January 2019 to January 2021 were included. Demographic variable data were collected as well as pathological results. Laboratory evaluations included fasting blood glucose (FBG), serum cholesterol (TC), triglyceride (TG), high-density lipoprotein (HDL), low-density lipoprotein (LDL), apolipoprotein A (Apo A) and apolipoprotein B (Apo B). Characterization of binary logistic regression models was used to test the odds ratios (ORs) between LVSI and its metabolic parameters with different subtypes of EC.
Results
The results indicated that CA125, ROMA, Ki67 score, FBG and TC were higher in EC patients with LVSI (all p<0.05). Negative ER and PR expression was positively associated with LVSI (P<0.05). CA125, ROMA, FBG, TC and ER were found to be independent risk factors for LVSI. CA125, ROMA and FBG were significantly elevated in type 1 EC patients with LVSI compared with those without LVSI (all p<0.05). TC and Ki67 scores were much higher in type 2 EC patients with vs without LVSI (all p<0.05). Negative PR expression was positively related to both type 1 and type 2 EC patients with LVSI. Consequently, CA125, ROMA, FBG and Apo B were found to be independent risk factors for LVSI in type 1 EC, and TC was found to be an independent risk factor for LVSI in type 2 EC.
Conclusion
FBG and TC were both independent risk factors for LVSI in EC. FBG and Apo B were independent risk factors for LVSI in type 1 EC. TC was an independent risk factor for LVSI in type 2 EC.
Introduction
Endometrial cancer (EC) is one of the most common obesity-related tumors in women. In 2022, the incidence and mortality of EC in the USA ranked first and second, respectively, among female reproductive system tumors.Citation1 In the past two decades, the incidence of EC in China has also shown a gradual increase.Citation2 With the development of the economy, obesity and diabetes have become important public health problems in China.Citation3 Obesity, diabetes and overweight are also reported to be adverse factors for the invasion and metastasis of EC.Citation4 Recently, metabolic syndrome was reported to be an adverse prognostic factor for EC. A meta-analysis showed that metabolic syndrome was strongly associated with an increased risk of EC in women (relative risk: 1.89, 95% confidence interval: 1.34–2.67).Citation5 Kitson et al suggested that EC patients were more likely to have obesity, high blood sugar, and a total cholesterol (TC)/high-density lipoprotein cholesterol (HDL) ratio >4.5 than those without EC.Citation6 According to the diagnostic criteria of metabolic syndrome proposed by the Diabetes Society of Chinese Medical Association in 2004,Citation7 accumulated studies have shown that glucolipid metabolism is closely associated with poor prognosis of EC. In a hyperglycemic environment, Drp1 impaired the mitochondrial function of EC cells to increase GLUT4 and VEGF expression, which promoted EMT and upregulated estrogen to accelerate the development of EC.Citation8,Citation9 Wang et al found that four metabolic subtypes based on the glucose-cholesterol synthesis axis could predict EC patient clinical outcomes by RNA sequencing. A total of 1204 samples, including endometrial cancer, were divided into four metabolic subtypes (quiescent, glycolysis, cholesterol, and mixed). In terms of survival analysis, the prognosis of the cholesterol subtype was better than that of the quiescent subtype.Citation10
Lymph-vascular space invasion (LVSI) is a poor prognostic factor for EC. EC patients with LVSI are more likely to relapseCitation11 and experience lymph node metastasis (LNM) and invasion.Citation12,Citation13 A cohort study based on prospectively recorded data identified LVSI as the strongest independent risk factor for LNM and reduced survival in EC patients.Citation14 Clinical studies suggest that adjuvant external irradiation and/or chemotherapy should be considered for stage I EC with a large amount of LVSI.Citation15 It has been reported that metabolic syndrome can increase the risk of EC, which is more prone to myometrium invasion and LNM.Citation16–18 However, it has not been reported whether obesity, diabetes and other metabolic disorders are related to the LVSI of EC.
We aimed to evaluate whether these metabolic indices were independent risk factors for LVSI in EC and compared the differences in metabolic risk factors among different subtypes of EC to improve the stratified management of metabolic risk in EC.
Patients and Methods
Subjects
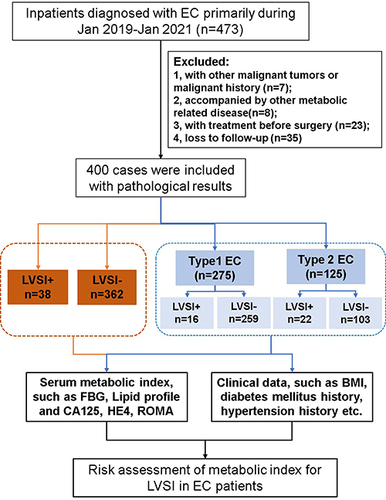
The current study retrospectively included patients who were diagnosed with EC primarily at Fujian Medical University Cancer Hospital, Fujian Cancer Hospital from January 2019 to January 2021 and those who had immunohistochemical pathological results (n=473). The exclusion criteria included the following: 1) other malignant tumors or a history of other malignant tumors (n=7); 2) accompanied by other diseases related to metabolic disease, such as liver diseases, nephrotic syndrome, and thyroid diseases. (n=8); 3) preoperative chemotherapy, radiotherapy or hormone therapy (n=23); and 4) loss to follow-up (n=35). A total of 400 patients were included. We obtained informed consent from all included patients. The Ethics Committee of Fujian Medical University Cancer Hospital, Fujian Cancer Hospital approved the study, which was conducted according to the principles of the Declaration of Helsinki (no. K2022-026-01).
Study Design and Data Collection
Data on demographic and clinical indicators were collected from the Fujian Medical University Cancer Hospital, Fujian Cancer Hospital information system. We performed the study as shown in . The collected data included age, menopausal status, body mass index (BMI), cancer antigen 125 (CA125), human epididymis protein 4 (HE4), risk ovarian malignancy algorithm (ROMA), fasting blood glucose (FBG), triglyceride (TG), total cholesterol (TC), low density lipoprotein (LDL), high density lipoprotein (HDL), apolipoprotein A (Apo A), apolipoprotein B (Apo B), history of diabetes and hypertension, International Federation of Gynecology and Obstetrics (FIGO) stage, pathology grade, lymphovascular space invasion (LVSI) and the expression levels of estrogen receptor (ER), progesterone receptor (PR), and Ki67 in EC tissue. Pretreatment lipid profiles were measured in 8-hour and above fasting blood samples within a week before any intervention. Tumor staging was classified in accordance with the 2009 International Federation of Gynecology and Obstetrics (FIGO) classification.Citation19 Tumor grade and histological classification were assigned based on the 2003 WHO classification of tumors.Citation20 The types of endometrial cancer were identified based on Bokhman.Citation21
Figure 1 The flowchart of inclusion and exclusion criteria of the study population.
Statistical Analysis
Statistical analysis was performed with SPSS 22.0 (IBM Corp., Armonk, NY, USA). Variables with approximately normal distributions are presented as the mean ± SD, and those with skewed distributions are presented as the median and interquartile range (25th–75th percentile). Categorical variables are presented as percentages (numbers). Continuous variables were analyzed by Student’s t-tests or Mann–Whitney U-tests. Chi-square tests or Fisher’s exact tests were used to analyze the categorical variables. A receiver operating characteristic (ROC) curve was generated for the cutoff point of the continuous data. The significance of the obtained cutoff values associated with LVSI was tested by performing both univariate and multivariate binary logistic regression analyses. Associations between the significant index and LVSI were studied by using multivariate logistic regression analysis. The odds ratios (ORs) and 95% confidence intervals (95% CIs) were adjusted for age, FIGO and tumor grade at diagnosis. Statistical significance was inferred from two-sided P values <0.05.
Results
Baseline Characteristics of EC Patients with or Without LVSI
Clinical data of EC patients with LVSI are shown in . In total, 38 (9.5%) of the 400 EC patients were diagnosed with LVSI. The incidence of LVSI in EC patients was not related to age, BMI, pregnancy and menopause status, diabetes, hypertension or HE4. (all p > 0.05). However, tumor biomarkers, such as CA125 and ROMA, were obviously higher in patients with LVSI than in those without LVSI (p<0.001, p=0.029). HE4 was not significantly elevated, and ROMA rose remarkably, which was most likely caused by CA125. Thus, CA125 is an important tumor biomarker associated with LVSI in EC. The expression levels of immunohistochemical indicators, such as ER and PR, were significantly higher in patients without LVSI than in those with LVSI (p<0.001). Conversely, Ki67 scores were much higher in those with LVSI (p=0.038, ).
Table 1 Clinicopathological Characteristics in EC Patients with LVSI or Not
Independent Risk Factors for LVSI in EC Patients
To evaluate the relationship between metabolic indices and LVSI, serum FBG and lipid profiles were analyzed. FBG and TC were higher in patients with LVSI than those without LVSI (all p<0.05). Apo B was also included because it was nearly significantly associated with LVSI (p=0.089, ). The continuous data were dichotomized for subsequent analyses using ROC curve analysis and the Youden Index. The cutoff values for statistically significant LVSI-related indicators, including CA125, HE4, ROMA, Ki67, FBG, TC, Apo B, ER and PR, were identified. Then, significant factors from the univariate analysis were included in the multivariate analysis. After adjusting for age, FIGO stage, tumor grade, CA125 odds ratio (OR) = 5.176, 95% CI: 2.234–11.989, p = 0.001], ROMA (OR = 12.67, 95% CI: 2.147–74.494, p = 0.005), FBG (OR = 3.095, 95% CI: 1.139–8.414, p = 0.027), TC (OR = 3.729, 95% CI: 1.413–9.840, p = 0.008), and positive ER expression (OR=0.349, 95% CI: 0.154–0.792, p=0.012) were independent risk factors for LVSI in EC patients ().
Table 2 Characteristics of Serum Metabolic Indexes in EC Patients by LVSI or Not
Table 3 Logistic Regression Analysis Independent Risk Factors of LVSI in EC
Metabolic Characteristics in Different Subtypes of EC Patients with or Without LVSI
To further explore the clinical application value of the LVSI, we analyzed EC patients according to the expression level of ER. Based on the Bokhman criterion, 275 (61.75%) of the 400 EC patients were diagnosed with ER+ and thus had type 1 EC. The results showed that the LVSI was closely related to CA125, ROMA, FBG and PR positivity in EC patients with ER+ (all p < 0.05, ). In EC patients with ER-, who had type 2 EC, the LVSI was associated with TC, Ki67 and PR positivity (all p < 0.05, ). Compared with type 1 EC, LVSI is more common in type 2 EC. Generally, LVSI in type 1 EC is related to FBG in addition to tumor biomarkers, including CA125 and ROMA, which are mainly affected by CA125. LVSI in type 2 EC was associated with TC in addition to the Ki67 score. These results indicated that CA125, as a serum tumor biomarker, may play a role in detecting LVSI in type 1 EC. Importantly, the difference in metabolic phenotype may affect the LVSI of different subtypes of EC.
Table 4 Clinicopathological and Metabolic Characteristics in Different Subtype of EC Patients with LVSI or Not
Independent Risk Factors for LVSI in Type 1 and Type 2 EC
The significant factors with p<0.100, such as CA125, ROMA, FBG, Apo B and PR expression related to type 1 EC, and the significant indicators, such as TC, Ki67 score and PR expression related to type 2 EC, were included in univariate and multivariate logistic regression analyses. The continuous data were dichotomized for subsequent analyses using ROC curve analysis and the Youden Index. The cutoff values for statistically significant LVSI-related indicators, including CA125, ROMA, FBG, Apo B, TC, Ki67 and PR, were reidentified, as shown in . After adjusting for age, FIGO stage, and tumor grade, CA125 (OR = 11.257, 95% CI: 2.375–53.363, p = 0.002), ROMA (OR = 16.777, 95% CI: 1.405–200.289, p = 0.026), FBG (OR = 3.608, 95% CI: 1.150–11.323, p = 0.028) and Apo B (OR = 3.969, 95% CI: 1.044–15.083, p = 0.043) were independent risk factors for type 1 EC, while TC (OR = 5.791, 95% CI: 1.376–24.364, p = 0.017) was an independent risk factor for type 2 EC.
Table 5 Logistic Regression Analysis Independent Risk Factors for LVSI in Different Subtype of EC
Discussion
The prognosis of early EC is generally good, but the prognosis of those with invasion and metastasis is poor.Citation22 LVSI is a clinicopathological feature closely related to LNM, progression-free survival and overall survival of EC.Citation23 At the same time, studies have shown that metabolic disorders can increase the risk of EC and tumor progression. Case–control studies in China showed that EC was positively associated with total serum cholesterol, triglycerides (TGs), low-density lipoprotein cholesterol, and dyslipidemia but negatively associated with HDL. They also observed an increased risk of type 1 EC women with BMI≥24.58 compared with those with BMI<24.58.Citation24 Significant increases in lipid biosynthesis and lipid peroxidation were found in obese individuals, and obese status promoted tumor invasiveness in EC mouse models.Citation25 Yang et al cultured Ishikawa cells with high glucose and found that high glucose promoted the progression of EC.Citation26 Simon et al suggested that lowering the burden of cardiovascular risk factors (including high cholesterol) may help intervene in the incidence of EC by a 10-year follow-up.Citation27 In this study, significant differences in FBG and TC were found in EC patients with and without LVSI. The relationship between glucose metabolism disorder and EC LVSI has not been reported before. This study is the first to suggest that blood glucose and dyslipidemia are associated with LVSI and that both are independent risk factors for LVSI in EC. In addition to metabolic risk factors, we identified CA125, ROMA, and ER as independent risk factors for EC with LVSI. A study has shown that CA125 and HE4 are independent risk factors for LVSI in postmenopausal stage 1 EC.Citation28 Consistent with this finding, we found that CA125 was more effective in predicting LVSI in type 1 EC. However, ROMA was a risk score calculated by CA125 and HE4. Here, ROMA was shown to be an independent risk factor for LVSI in type 1 EC, mainly resulting from the effect of CA125.
ER, as an important prognostic factor of hormone-dependent tumors, is closely related to LVSI.Citation29 Positive ER expression was the advantageous factor for LVSI of EC, which inspired us to classify EC according to the expression of ER. In our research, the incidence of LVSI in type 2 EC was higher (17.60%) than that in type 1 EC (6.18%). Similarly, Jaishankar et al claimed that substantial LVSI had a high incidence in type 2 EC and predicted LNM and worse clinical outcomes.Citation30 Interestingly, we found that the independent risk factors for LVSI were diverse in type 1 and 2 EC. FBG and Apo B were independent risk factors for LVSI in type 1 EC, while TC was an independent risk factor for LVSI in type 2 EC. These results indicated that glycol metabolism played a vital role in the LVSI of type 1 EC that was dominated by endometrioid adenocarcinoma. Dai et al found that diabetes was more common in LVSI-positive patients with endometrial adenocarcinoma.Citation31 Excess body weight was associated with both type 1 and type 2 EC in a weight-dependent manner, and the association was significantly stronger in type 1 EC.Citation32
On the other hand, lipid metabolism played an important role in the LVSI of type 2 EC, mainly consisting of nonendometrioid adenocarcinoma. Many studies have shown that cholesterol is closely related to the metastasis of hormone-dependent tumors, such as prostate cancer,Citation33 breast cancer,Citation34 and EC.Citation35 In addition, Kho et al performed a bidirectional, two-sample Mendelian randomization analysis to investigate the relationship between levels of three blood lipids and EC risk in a large population. They suggested that an increase in serum LDL reduced the risk of nonendometrioid adenocarcinoma, whereas an increase in serum HDL increased the risk of nonendometrioid adenocarcinoma. Importantly, LDL and HDL also play an important role in the progression of nonendometrioid adenocarcinoma.Citation36 Although we did not find such differences in HDL and LDL in type 2 EC, this was probably owing to our small sample size. In a retrospective review of 816 consecutive EC cases was conducted by Yale University, there was no association between type 2 EC and diabetes mellitus or the use of HRT.Citation37
This metabolic heterogeneity was probably related to excess estrogen. Estrogen-mediated regulation of diabetes mellitus has already been reported in vitro and in vivo.Citation38 Gregorio et al investigated whether estrogen not only decreased blood glucose but also induced insulin resistance. The opposite effects were mainly dependent on the previous circulating estrogenic (low or high) levels, which demonstrated a direct effect of estrogen upon glycemic homeostasis.Citation39 Therefore, in contrast to Type 2 EC, FBG was an independent risk factor for LVSI in Type 1 EC patients.
Strengths and Limitations
Our study evaluated the prognosis of different types of EC using clinically available metabolic markers, such as serum lipid profile and glucose. Moreover, the classification of EC by ER and PR is an economical and conventional method in clinical practice. A strength of the study is that the results are more easily applied to the clinic and beneficial to the individual management of EC patients. However, the ESTRO/ESGO/ESP guidelines for the management of EC proposed a novel risk stratification model including molecular TCGA molecular groups to assess the prognosis of EC, and the role of these molecular subtypes of EC as prognostic factors independent from classic, well-known, clinicopathologic ones in EC (such as myometrial invasion, histotype or LVSI) is a hot topic in the literature to date.Citation40 A limitation of this study is that the evaluation of molecular TCGA subtypes of EC is absent. Recently, Antonio et al claimed that LVSI was a prognostic factor of EC independent from molecular prognostic factors,Citation41 which also showed the importance of looking for independent risk factors for LVSI. A prospective study on the molecular markers of EC based on four molecular subtypes of EC found that ER/PR was associated with molecular typing, and PR negative was significant in P53 type.Citation42 P53mt patients had the worst prognosis and higher incidence of LVSI.Citation43 The relationship between LVSI and metabolism in TCGA molecular subtypes of EC remains to be explored. In future, we will continue to focus on metabolic risk factors to contribute to managing EC patients.
Conclusion
In general, glucose and lipid metabolism are inextricably linked in EC. FBG and TC were both independent risk factors for LVSI in EC. Importantly, different subtypes of EC have diverse metabolic phenotype characteristics, which is beneficial for risk management of different subtypes of EC. In summary, we should focus on managing blood glucose in type 1 EC and pay more attention to controlling serum cholesterol in type 2 EC to prevent LVSI in EC.
Ethical Approval
This study was approved by the ethical committee of the Fujian Medical University Cancer Hospital, Fujian Cancer Hospital (no. K2022-026-01). Informed consents were waived by the Ethic Committee as all clinical data were extracted from the medical system and personal information of any patient was masked. Patients’ personal information and medication information were recorded while maintaining patient confidentiality and omitting their names and addresses. This study was performed in accordance with the Helsinki Declaration.
Disclosure
The authors declare that they have no conflicts of interest.
Additional information
Funding
References
- Siegel RL, Miller KD, Fuchs HE, et al. Cancer statistics, 2022. CA. 2022;72(1):7–33. doi:10.3322/caac.21708
- Chen W, Zheng R, Baade PD, et al. Cancer statistics in China, 2015. CA. 2016;66(2):115–132. doi:10.3322/caac.21338
- Chen W, Sun K, Zheng R, et al. Cancer incidence and mortality in China, 2014. Chin J Cancer Res. 2018;30(1):1–12. doi:10.21147/j.issn.1000-9604.2018.01.01
- Mili N, Paschou SA, Goulis DG, et al. Obesity, metabolic syndrome, and cancer: pathophysiological and therapeutic associations. Endocrine. 2021;74(3):478–497. doi:10.1007/s12020-021-02884-x
- Esposito K, Chiodini P, Capuano A, et al. Metabolic syndrome and endometrial cancer: a meta-analysis. Endocrine. 2014;45(1):28–36. doi:10.1007/s12020-013-9973-3
- Kitson SJ, Lindsay J, Sivalingam VN, et al. The unrecognized burden of cardiovascular risk factors in women newly diagnosed with endometrial cancer: a prospective case control study. Gynecol Oncol. 2018;148(1):154–160. doi:10.1016/j.ygyno.2017.11.019
- Chinese Medical Association. The Suggestion on Chinese Metabolic Syndrome. Shanghai, China: Chinese Medical Association; 2004.
- Guo J, Ye F, Jiang X, et al. Drp1 mediates high glucose-induced mitochondrial dysfunction and epithelial-mesenchymal transition in endometrial cancer cells. Exp Cell Res. 2020;389(1):111880. doi:10.1016/j.yexcr.2020.111880
- Gu CJ, Xie F, Zhang B, et al. High glucose promotes epithelial-mesenchymal transition of uterus endometrial cancer cells by increasing ER/GLUT4-mediated VEGF secretion. Cell Physiol Biochem. 2018;50(2):706–720. doi:10.1159/000494237
- Wang G, Liu X, Wang D, et al. Identification and development of subtypes with poor prognosis in pan-gynecological cancer based on gene expression in the glycolysis-cholesterol synthesis axis. Front Oncol. 2021;11:636565. doi:10.3389/fonc.2021.636565
- Tortorella L, Restaino S, Zannoni GF, et al. Substantial lymph-vascular space invasion (LVSI) as predictor of distant relapse and poor prognosis in low-risk early-stage endometrial cancer. J Gynecol Oncol. 2021;32(2):e11. doi:10.3802/jgo.2021.32.e11
- Restaino S, Tortorella L, Dinoi G, et al. Semiquantitative evaluation of lymph-vascular space invasion in patients affected by endometrial cancer: prognostic and clinical implications. Eur J Cancer. 2021;142:29–37. doi:10.1016/j.ejca.2020.10.011
- Kim SI, Yoon JH, Lee SJ, et al. Prediction of lymphovascular space invasion in patients with endometrial cancer. Int J Med Sci. 2021;18(13):2828–2834. doi:10.7150/ijms.60718
- Stålberg K, Bjurberg M, Borgfeldt C, et al. Lymphovascular space invasion as a predictive factor for lymph node metastases and survival in endometrioid endometrial cancer - A Swedish Gynecologic Cancer Group (SweGCG) study. Acta Oncol. 2019;58(11):1628–1633. doi:10.1080/0284186X.2019.1643036
- Bosse T, Peters EE, Creutzberg CL, et al. Substantial lymph-vascular space invasion (LVSI) is a significant risk factor for recurrence in endometrial cancer–A pooled analysis of PORTEC 1 and 2 trials. Eur J Cancer. 2015;51(13):1742–1750. doi:10.1016/j.ejca.2015.05.015
- Kokts-Porietis RL, McNeil J, Nelson G, et al. Prospective cohort study of metabolic syndrome and endometrial cancer survival. Gynecol Oncol. 2020;158(3):727–733. doi:10.1016/j.ygyno.2020.06.488
- Tong Y, Xie X, Mao X, et al. Low red blood cell count as an early indicator for myometrial invasion in women with endometrioid endometrial carcinoma with metabolic syndrome. Cancer Manag Res. 2020;12:10849–10859. doi:10.2147/CMAR.S271078
- Yang X, Li X, Dong Y, et al. Effects of metabolic syndrome and its components on the prognosis of endometrial cancer. Front Endocrinol. 2021;12:780769. doi:10.3389/fendo.2021.780769
- Creasman W. Revised FIGO staging for carcinoma of the endometrium. Int J Gynecol Obstet. 2009;105(2):109. doi:10.1016/j.ijgo.2009.02.010
- Rutgers JK. Update on pathology, staging and molecular pathology of endometrial (uterine corpus) adenocarcinoma. Future Oncol. 2015;11(23):3207–3218. doi:10.2217/fon.15.262
- Bokhman JV. Two pathogenetic types of endometrial carcinoma. Gynecol Oncol. 1983;15(1):10–17. doi:10.1016/0090-8258(83)90111-7
- Giannone G, Attademo L, Scotto G, et al. Endometrial cancer stem cells: role, characterization and therapeutic implications. Cancers. 2019;11(11):1820. doi:10.3390/cancers11111820
- Perrone E, De Felice F, Capasso I, et al. The immunohistochemical molecular risk classification in endometrial cancer: a pragmatic and high-reproducibility method. Gynecol Oncol. 2022;165(3):585–593. doi:10.1016/j.ygyno.2022.03.009
- Zhang Y, Liu Z, Yu X, et al. The association between metabolic abnormality and endometrial cancer: a large case-control study in China. Gynecol Oncol. 2010;117(1):41–46. doi:10.1016/j.ygyno.2009.12.029
- Guo H, Kong W, Zhang L, et al. Reversal of obesity-driven aggressiveness of endometrial cancer by metformin. Am J Cancer Res. 2019;9(10):2170–2193.
- Yang X, Cheng Y, Zhou J, et al. Targeting cancer metabolism plasticity with JX06 nanoparticles via inhibiting PDK1 combined with metformin for endometrial cancer patients with diabetes. Adv Sci. 2022;9(8):e2104472. doi:10.1002/advs.202104472
- Simon MS, Hastert TA, Barac A, et al. Cardiometabolic risk factors and survival after cancer in the Women’s Health Initiative. Cancer. 2021;127(4):598–608. doi:10.1002/cncr.33295
- Panyavaranant P, Manchana T. Preoperative markers for the prediction of high-risk features in endometrial cancer. World J Clin Oncol. 2020;11(6):378–388. doi:10.5306/wjco.v11.i6.378
- Majid S, Rydén L, Manjer J. Predictive factors for sentinel node metastases in primary invasive breast cancer: a population-based cohort study of 2552 consecutive patients. World J Surg Oncol. 2018;16(1):54. doi:10.1186/s12957-018-1353-2
- Jaishankar S, Pifer PM, Bhargava R, et al. Is substantial lymphovascular space invasion prognostic for clinical outcomes in type ii endometrial cancer? Clin Oncol. 2022;34(7):452–458. doi:10.1016/j.clon.2022.02.018
- Dai Y, Dong Y, Cheng Y, et al. Prognostic significance of lymphovascular space invasion in patients with endometrioid endometrial cancer: a retrospective study from a single center. J Gynecol Oncol. 2020;31(3):e27. doi:10.3802/jgo.2020.31.e27
- Sollberger TL, Gavrilyuk O, Rylander C. Excess body weight and incidence of type 1 and type 2 endometrial cancer: the Norwegian women and cancer study. Clin Epidemiol. 2020;12:815–824. doi:10.2147/CLEP.S253866
- Marín-Aguilera M, Pereira MV, Jiménez N, et al. Glutamine and cholesterol plasma levels and clinical outcomes of patients with metastatic castration-resistant prostate cancer treated with taxanes. Cancers. 2021;13(19):4960. doi:10.3390/cancers13194960
- Baek AE, Yu YA, He S, et al. The cholesterol metabolite 27 hydroxycholesterol facilitates breast cancer metastasis through its actions on immune cells. Nat Commun. 2017;8(1):864. doi:10.1038/s41467-017-00910-z
- Chen Y, Lee K, Liang Y, et al. A cholesterol homeostasis-related gene signature predicts prognosis of endometrial cancer and correlates with immune infiltration. Front Genet. 2021;12:763537. doi:10.3389/fgene.2021.763537
- Kho PF, Amant F, Annibali D, et al. Mendelian randomization analyses suggest a role for cholesterol in the development of endometrial cancer. Int J Cancer. 2021;148(2):307–319. doi:10.1002/ijc.33206
- Feinberg J, Albright B, Black J, et al. Ten-year comparison study of type 1 and 2 endometrial cancers: risk factors and outcomes. Gynecol Obstet Invest. 2019;84(3):290–297. doi:10.1159/000493132
- Barnes BO, Regan JF, Nelson WO. Improvement in experimental diabetes following the administration of amniotin. JAMA. 1933;101(12):926–927. doi:10.1001/jama.1933.02740370030008
- Gregorio KCR, Laurindo CP, Machado UF. Estrogen and glycemic homeostasis: the fundamental role of nuclear estrogen receptors ESR1/ESR2 in glucose transporter GLUT4 regulation. Cells. 2021;10(1):99. doi:10.3390/cells10010099
- Concin N, Matias-Guiu X, Vergote I, et al. ESGO/ESTRO/ESP guidelines for the management of patients with endometrial carcinoma. Int J Gynecol Cancer. 2021;31(1):12–39. doi:10.1136/ijgc-2020-002230
- Antonio R, Antonio T, Diego R, et al. Lymphovascular space invasion in endometrial carcinoma: a prognostic factor independent from molecular signature. Gynecol Oncol. 2022;165(1):192–197. doi:10.1016/j.ygyno.2022.01.013
- Karnezis AN, Leung S, Magrill J, et al. Evaluation of endometrial carcinoma prognostic immunohistochemistry markers in the context of molecular classification. J Pathol Clin Res. 2017;3(4):279–293. doi:10.1002/cjp2.82
- Bayramoglu D, Seçilmiş Kerimoğlu Ö, Bayramoğlu Z, et al. Classification of high-grade endometrium carcinomas using molecular and immunohistochemical methods. Ginekol Pol. 2022. doi:10.5603/GP.a2021.0177