 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Objectives:
The purpose of this study was to analyze the relationship of airborne chemicals and the physical work environment risk element on the indoor air symptoms of nonindustrial workers.
Design:
A cross-sectional study consisting of 200 office workers. A random selection of 200 buildings was analyzed for exposure and indoor air symptoms based on a pilot study in the Klang Valley, Malaysia.
Methods:
A set of modified published questionnaires by the Department of Occupational Safety and Health (DOSH), Malaysia and a previous study (MM040NA questionnaire) pertaining to indoor air symptoms was used in the evaluation process of the indoor air symptoms. Statistical analyses involving logistic regression and linear regression were used to determine the relationship between exposure and indoor air symptoms for use in the development of an indoor risk matrix.
Results:
The results indicate that some indoor air pollutants (carbon monoxide, formaldehyde, total volatile organic compound, and dust) are related to indoor air symptoms of men and women. Temperature and relative humidity showed a positive association with complaints related to the perceived indoor environmental condition (drafts and inconsistency of temperature). Men predominantly reported general symptoms when stratification of gender involved exposure to formaldehyde. Women reported high levels of complaints related to mucosal and general symptoms from exposure to the dust level indoors.
Conclusion:
Exposure to pollutants (total volatile organic compounds, carbon monoxide, and formaldehyde) and physical stressors (air temperature and relative humidity) influence reported symptoms of office workers. These parameters should be focused upon and graded as one of the important elements in the grading procedure when qualitatively evaluating the indoor environment.
Video abstract
Point your SmartPhone at the code above. If you have a QR code reader the video abstract will appear. Or use: http://dvpr.es/KAo2dY
Point your SmartPhone at the code above. If you have a QR code reader the video abstract will appear. Or use:
Introduction
The indoor environment has been a growing focus for environmental and public health professionals including occupational safety and health professionals. Due to the implementation of the current Code of Practice in Malaysia in 2010,Citation1 many employers and building managers have taken a positive response towards determining, monitoring, and quantifying the risk of indoor air pollutants existing in their premises or buildings.
In a tropical climate country like Malaysia, industrial hygienists and indoor air quality assessors have been extensively involved in indoor air quality (IAQ) diagnosis and remediation in occupational environments for the past 5 years.Citation2 Professionals in air pollution, ventilation, engineering, microbiology, architecture, and other fields are called upon to respond to resolve IAQ problems.
No matter how extensive or bad the situation of the indoor environment that negatively influences the health condition of the occupants is, a multidisciplinary approach from skilled professionals with knowledge on the maintenance, construction, ventilation system, and sources of biological or chemical contaminants and their potential health effects, together with the perception of the building occupants, IAQ guidelines, standards, and Codes of Practice, should be able to address the problems.Citation1–Citation4
The development of Malaysia has led to the major construction of buildings, which fully depend on air conditioning systems to control the perceived environmental factors related to thermal comfort; however, certain other parameters have frequently been neglected by the building owner until a problem strikes.Citation4
A lack of information regarding the influence of gender differences, chemicals, and physical indoor pollutants that can influence health symptoms of Malaysians has presented scientists with a challenge to identify and mitigate the IAQ issues before they become catastrophic. Therefore, an extensive study regarding these issues should be conducted to provide indoor air scientists and the indoor air industry with information concerning the effects of pollutants and their relationship with common indoor air symptoms.
IAQ is one of the big issues being addressed in Malaysia. Concerns about health have led workers (nonindustrial) to participate in most of the activities concerning awareness of health-related issues in the workplace.Citation3 Good IAQ is desired by most workers and visitors, especially in public offices such as government offices.
The current Code of Practice has been updated and focuses on eleven main parameters that are suspected of influencing pollution of the indoor air environment.Citation2 Previous studies suggest that a checklist is one of the preliminary tools needed to evaluate the condition of the indoor environment in the workplace.Citation5 Hitherto, scientists have suggested that ventilation influences most of the indoor environmental issues in tropical climates, which are most likely related to the high number of cases of sick building syndrome being reported after exposure to poor ventilation and also thermal comfort issues.Citation3
In addition, the indoor environment is considered by most engineers to be challenging because of the need to design in the tight space above the ceiling to ensure sufficient fresh air and efficient ventilation that is able to provide a sufficient level of comfort and dilute pollutants that have already been introduced from air handling units.
Working in a healthy environment is important to the individual as the environment, especially indoors, is perceived through individual appraisal.Citation6,Citation7 Some mediating factors between the work environment and physiological reactions and the individual’s perception are related to the process of establishing an individual appraisal of environmental functions. Various negative effects on health can be caused by a combination of mental factors including low job control, low job support, and high demand or workload.Citation8 Serious health problems – anxiety, mental distress, high rate of absence, multiple sickness, high mortality rate,Citation9 and high turnoverCitation10 – can occur due to multifactorial problems related to working indoors.
Recently, there has been an interest in multidisciplinary research to identify health problems related to the indoor environment.Citation5 Nonspecific symptoms that affect the skin, eyes, nose, and throat and nervous symptoms such as headache, dizziness, tiredness, and feeling heavy-headed have been previously reported as being due to poor IAQ in the workplace. Collectively, these have been termed as the sick building syndrome.Citation11,Citation12
Exposure to various indoor air pollutants has been suggested as being the cause of such symptoms. These include dampness,Citation13 inconsistency of temperature and thermal comfort issues,Citation3,Citation14,Citation15 and indoor particle pollutants.Citation16 In addition, other factors that significantly influence the symptoms reported among occupants include chemical dispersion and chemical reaction indoors,Citation17 thermal condition (which involves the temperature and relative humidity [RH] in the workplace),Citation18–Citation20 ventilation rate issues,Citation3 ergonomic issues (eg, video terminal display), working with the photocopier,Citation21 environmental tobacco smoke, total volatile organic compounds (TVOCs), formaldehyde, material containing aldehydes, and combustion products.Citation22
Many researchers suggest that indoor environmental problems seem to be multifactorial, which are probably caused by mental stress at work,Citation3,Citation5,Citation23,Citation24 the psychosocial work environment, and the relationship between physical and mental factors.Citation8 Gender differences in reporting indoor air-related symptoms has been debated but discussion pertaining to tropical climate regions is lacking.Citation5 Many four-season countries have conducted numerous studies that focused on observing subjective health symptoms.Citation25 Population and general studies in other countries also show similar results relating to gender differences as well as organ-specific symptoms from exposure to the indoor environment.Citation26,Citation27 Previous clinical studies of airway symptoms, airway caliber, bronchial hyperreactivity, and factors such as hormonal fluctuations suggest possible causes of gender differences.Citation28 However, scientists are still unable to identify the real causes of these differences, thus several studies have suggested certain elements and factors that need to be considered when studying gender differences in indoor air symptoms.Citation29
This study aimed to evaluate the relationship and association between reported health symptoms, subjectively evaluate the physical indoor environmental stressors, as well as objectively evaluate the chemical airborne and physical indoor environment. Gender differences were also evaluated.
Materials and methods
Study design
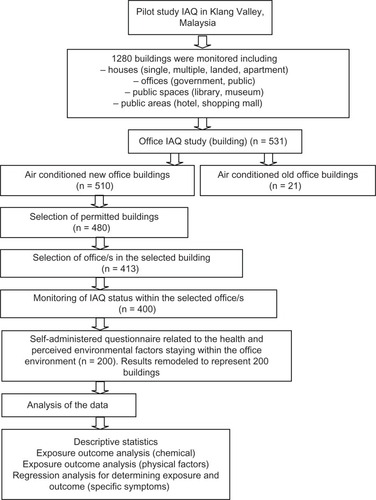
A cross-sectional study was performed on 200 buildings (in 25 different postcodes) that had been selected from a pilot IAQ study in the Klang Valley, Malaysia. Employees in each of these buildings during the study period were invited to participate (data had been modeled to spatially represent 200 buildings due to insufficient complete questionnaires gathered by the end of the study period). They were all informed in a general meeting and briefed by the building owners, safety and health officers, or building management who were present. Both written and oral information was given and all participants gave written informed consent. The study was conducted between March and June 2012, after the monsoon season and before the fasting season. All participants were questioned at their own workplace. A summary of the data collection process is described in .
Figure 1 Flow diagram of the study related to exposure and outcome of indoor air pollutants.
Questionnaire
The participants were asked to complete a modified extended MM040NA questionnaire that has frequently been used for the investigation of indoor air symptoms.Citation30 The questionnaire also contains items similar to those published by the Department of Occupational Safety and Health (DOSH), Malaysia in their Code of Practice on IAQ for Malaysian use.Citation2 This questionnaire contains twelve questions concerning sick building symptoms that are known to be related to indoor air problems and twelve other questions about perceived factors in the physical work environment over the previous 3 months. Symptoms and environmental factors were recorded in statistical analysis as “yes, often (more than once a week)” = two, “yes, sometimes (once a week)” = one, and “no, never” = zero. These were then totaled, giving scores for symptoms (zero to 24) and perceived physical work environment (zero to 24), respectively. The symptoms asked in this questionnaire included five questions on general symptoms (fatigue; feeling heavy-headed; headache; nausea or dizziness; and difficulty concentrating), four questions on mucosal irritation (itching, burning, or irritation of the eyes; irritated, stuffy or runny nose; hoarse, dry throat; and cough), and three on skin symptoms (dry or flushed facial skin; scaling or itching scalp or ears; and dry, itching, red skin). These were totaled, giving three additional scores for general (zero to ten), mucosal (zero to eight), and dermal symptoms (zero to six), respectively.
The participants also answered questions about gender, age, race, marital status, job category (private or government), workstation, smoking (yes/no), working hours in a week (hours), and working days in a week (days). Additional questions also included the perception of the indoor environment in their office, such as using chemicals with strong odor (yes/no), workstation covered with carpet (yes/no), new carpet (yes/no), new furniture (yes/no), new partition (yes/no), new wall covering (yes/no), new water damage (yes/no), and using office equipment such as photocopier, fax machine, glue, and chemicals with strong odor (yes/no).
Based on a previous study conducted using a checklist,Citation5 some remarks were made by trained occupational hygienists from the National Institute of Occupational Safety and Health, Malaysia and Universiti Putra Malaysia to give the score for five to six important elements (with 14 key questions) in the indoor investigation using the environmetric technique.Citation5 These items included the general condition of the indoor environment (fungal index; blockage ventilation index; hazardous substances index), health effect (radiant heat index; air dead index; occupant change index), source of pollutants (furniture index; off gassing index), ventilation (outside air index; air conditioning schedule index), IAQ perception (noise index), and industry Code of Practice on IAQ (general index; conduct IAQ test index; IAQ interest index). This checklist is scored from zero to five for each index in which the highest number indicates the higher risk available indoors based on subjective perception. The scores were totaled and divided by the overall scores, giving scores in the form of the index from zero to one. The evaluation will be discussed and analyzed elsewhere. The checklist item is registered as an evaluation variable with the quantitative airborne and physical work environment measurements.
Objective indoor environmental exposure monitoring (chemical and physical)
Indoor climate was assessed in 200 buildings in different postcodes (25 postcodes): 73 small offices (approximately 3000–10,000 sq ft), 54 medium-sized offices (10,000–20,000 sq ft), and 73 large offices (>20,000 sq ft). The offices were randomly selected from the available rooms/permitted areas provided by the building owner of the buildings. Measurements were performed at a logging point in each office, close to the worker, 110 cm from the floor. To obtain representative samples, a number of points per floor were selected based on the suggested standard published by DOSH.Citation2 below shows the recommended minimum number of sampling points for IAQ assessments suggested by DOSH.Citation2
Table 1 Suggested minimum number of sampling points according to the floor area served by mechanical ventilation and air conditioning system
Air temperature (°C), RH (%), and air movement (m/second) were used for physical work environment monitoring. Carbon dioxide (CO2; ppm), carbon monoxide (CO; ppm), TVOCs (ppm), formaldehyde (ppm), ozone (ppm), and airborne dust – assessed as particulate matter with an aerodynamic diameter of 10 μg/m3 (PM10; μg/m3) – were monitored. Data were logged according to the occupational hygiene technique, namely surrogate partial period grab samples.Citation3 The samples were collected in 30 minutes at four time slots (morning, afternoon, evening, and late evening) to avoid spatial temporal differences in the data collection process (making the data more representative). Data were logged continuously using the following instruments:
Temperature (air): AQ 200 air quality monitoring with Data Logger-10 software (KIMO, Montpon, France).
RH (air): AQ 200 air quality monitoring with Data Logger-10 software (KIMO).
CO2 and CO (air): AQ 200 air quality monitoring with Data Logger-10 software (KIMO) with multifunction probe (SCO2T and SCOT; KIMO) for temperature, humidity, and CO2 (with measuring range of approximately −20°C to 80°C for temperature, 5%–95% RH for humidity, and 0–5000 ppm for CO2).
Air velocity and draft: VT 200 draft sensor (hot wire) with Data Logger-10 software (KIMO) (measuring range of air velocity 0.01–3.00 m/second).
Airborne dust (PM10; μg/m3): DustTrak™ II Aerosol Monitor 8532 with TrakPro™ software (TSI Inc, Shoreview, MN, USA).
Chemical airborne monitoring (direct reading): YESAIR 8-Channel IAQ Monitor with multiple sensors (formaldehyde, ozone, and TVOCs) with YES Viewer software version 7.0 (Critical Environment Technologies Canada Inc, Delta, BC, Canada).
The instruments were calibrated according to the stated procedures from the instrument suppliers and manufacturers’ specification. For real-time monitoring, a special sensor – photoionization detector – was used in the YESAIR monitoring devices. Precautions were taken when using the real-time photoionization detector instrument as the readings could be affected by the presence of other non-VOCs, such as anesthetic or disinfecting gases. For calibration of the real-time monitors, isobutylene (2-methylpropene) was used as the reference calibration gas.Citation2
Measurements were registered as 5-minute averages throughout the monitoring period. The results for each room were calculated as mean figures (8-hour time-weighted average) from the work hours defined as between 8:00 AM and 5:00 PM for monitoring days. Because not all offices in the buildings were monitored, the results were modeled according to the building and office size or dimensions to assign data for the worksite for all participants. The concentrations of the airborne chemicals were calculated using the following equation:
In this equation, C represents the concentration of contaminant during an incremental exposure time and T represents the incremental exposure time.
Statistical procedure
Categorical values were compared in the groups using Pearson’s chi-squared test, and continuous variables were compared using Student’s t-test. As the dust levels (PM10), formaldehyde, and TVOCs were highly skewed in the material, log-transformed data for this variable were used in the analysis. Linear regression analysis was performed using scores as dependent variables, adjusting for smoking, chronic illness, age, gender, job category, new furniture, new partition, and workstation. Unadjusted and adjusted betas (partial regression coefficient) were calculated.
Logistic regression was performed for dichotomized responses concerning symptoms and perceived indoor environments, univariate and controlling for gender, smoking, chronic illness, age, gender, job category, new furniture, new partition, and workstation. Analysis was also stratified by gender. SPSS version 13.0 (SPSS Inc, Chicago, IL, USA) was used for the analysis, and the significance level was set at 0.05. The potential cofounders found in the analysis were controlled statistically.
Ethics
The Universiti Putra Malaysia Medical and Health Sciences Research Committee (under the Faculty of Medicine and Health Sciences) approved the study (reference item: UPM/FPSK/PADS/T7-MJKEtikaPer/F01[LEC[JKK]_OOGOS[10]03]; dated February 10, 2011).
Results
Questionnaire
A total of 200 (80%) of the invited workers participated in the study (out of 531 office buildings), which included 81 men and 119 women who were mostly aged 21–40 years (). The women recorded a higher number of Malay workers than the men, but this was not statistically significant. A significantly higher percentage of women worked in the government sector compared to the men. More men had managerial positions, whereas more women were employed as administrative/supporting staff, with corresponding workstation differences leading to different complaints. The genders did not differ significantly for working hours in a week and working days in a week.
Table 2 Sociodemographic and office environment status of respondents
Men registered exposure to potential chemical dispersion items in the indoor environment more often than women. The differences were significant for the reporting of new furniture and new partition (). Women had more complaints concerning clinically diagnosed illness by a medical doctor than men. The differences were significant for asthma, migraine, and eczema ().
Table 3 Percentage (%) of reported (yes) perception of indoor office environment between men and women
Table 4 Percentage (%) of reported illness by doctor
Exposure and building characteristics
The indoor chemistry of the air, described in , are classified by the age and exposure level of the building. Buildings were categorized based on an age of 5 years to describe whether they were old or new (ie, >5 years occupancy considered old).Citation3 The differences in indoor parameters were higher in new buildings compared to old for RH and ventilation rate. Due to the nature of the data collected and based on the focus of the study objectives, new buildings in the Klang Valley with an air conditioning system were focused on and a sample of 200 respondents from these building was further analyzed.
Table 5 Airborne chemical data between old and new buildings (from pilot study)
Airborne pollutants and reported indoor symptoms
Men were exposed to significantly higher concentrations of airborne chemicals compared to women, namely TVOCs and CO. The physical parameters, namely air movement, were recorded more often by men compared to the women (). The temperature, RH, and dust (PM10) were reported less by men compared to the women; however, the level was not significant.
Table 6 Airborne chemical and physical data between men and women in selected exposure building (results were taken for n = 200 modeled exposure)Table Footnote$
All registered symptoms were reported more often by women than men. The differences were significant for feeling heavy-headed and difficulty in concentrating (). More women complained of these two general symptoms.
Table 7 Differences in reported air symptoms of men and women in buildings in the Klang Valley, Malaysia (200 randomly assigned buildings)
Women complained more frequently about the physical work environment, namely draft, temperature too high, varying temperature, temperature too low, dry air, and dusty environment. Men reported more complaints about unpleasant odor, static electricity, passive smoking, noise, and inadequate lighting. The differences were not statistically significant for all registered complaints ().
Table 8 Number and percentage of men and women working in office environments in the Klang Valley, Malaysia who answered “yes, often” or “yes, sometimes” to questions about perceived environments related to twelve physical indoor climate factors pertaining to the previous 3 weeks (n = 200)
Relationships between symptoms score, chemical exposure, and subjectively perceived physical work environment
shows the results from the linear regression analysis, with the symptom score as the dependent variable, and CO2, CO, dust (PM10), formaldehyde, and TVOCs (ie, IAQ chemical parameters), and the score for perceived physical indoor air environment as independent variables. The analysis was adjusted for smoking, chronic illness, age, gender, job category, new furniture, new partition, and workstation.
Table 9 Linear regression study of workers in office areas in the Klang Valley, Malaysia (subjective work environment)
The results show that the subjective physical environment was significantly associated with the total, general, and mucosal symptom score. The dermal symptom score was not associated with the subjective physical environment. CO showed the most significant association with the total, general, and mucosal symptom scores (), while other parameters did not show a significant association.
When analyzing men and women separately, the findings were not similar and were stronger for the men between the total symptom score and the subjective physical environment score and TVOC concentration (β = 2.819, 95% confidence interval [CI] 0.234–5.404, standardized β = 0.698, P = 0.034). The association with TVOCs was not significant for women (β = −0.364, 95% CI = −11.004–10.275, standardized β = −0.038, P = 0.942).
Using the three subscores for general, mucosal, and dermal symptoms for both genders together in the adjusted analysis, males showed that the score for general symptoms was significantly associated with CO and TVOC concentration (β = −0.963, 95% CI = −1.887 to −0.038, standardized β = −0.714, P = 0.042 and β = 1.224, 95% CI = 0.054–2.393, standardized β = 0.636, P = 0.041, respectively). However, no association was observed among the female respondents.
The mucosal score only showed a significant association with TVOC concentration among male respondents (β = 0.721, 95% CI = 0.088–2.129, standardized β = 0.481, P = 0.035), while females only showed an association in the dermal score with the perceived work environment score (β = 0.307, 95% CI = 0.032–0.581, standardized β = 0.862, P = 0.031).
Relationship between symptom scores, chemical exposure, and objectively assessed physical work environment
The next step was to replace the perceived physical environments (subjective perception score) with objective assessments (airborne physical parameters such as air movement, air temperature, and RH). The total symptom score was analyzed as a dependent variable with five IAQ chemical parameters and three objective physical environmental factors (air temperature, RH, and air movement) in the model at the same time.
A similar pattern of observations was gathered in the analyses in which the total, general, and mucosal symptom scores were significantly related to the CO level (). CO was the only factor significantly associated with the symptom score (total, general, and mucosal) when also adjusting for smoking, chronic illness, age, gender, job category, new furniture, new partition, and workstation.
Table 10 Linear regression study of workers in office areas in the Klang Valley, Malaysia (objectively measured physical work environment)
Men and women were then analyzed separately, and this finding (total symptoms score) was not significantly associated with the objective measurement (chemical and physical parameters) for men and women (β = −2.380, 95% CI = −5.009–0.249, standardized β = −0.841, P = 0.073 and β = −1.999, 95% CI = −5.831–1.833, standardized β = −0.718, P = 0.278, respectively).
Using the three subscores for symptoms (general, mucosal, and dermal) in the adjusted analysis for all workers, the scores for general, mucosal, and dermal symptoms were not significantly associated with the exposure to the chemical or physical objective parameters. Males showed a higher result for exposure to CO; however, it was not statistically significant (β = −1.104, 95% CI = −2.311−0.102, standardized β = −0.819, P = 0.070). Analyzing men and women separately showed no significant association with general, mucosal, or dermal symptoms for men with exposure to CO. No associations were found for women for all exposures and symptoms.
Additional analysis was performed by changing the illness (asthma, migraine, and eczema) diagnosed by the doctor in the dependent variable section (stratified by gender). Only male respondents showed a significant relationship with migraine complaint (β = −0.762, 95% CI = −1.386 to −0.138, standardized β = −0.663, P = 0.020). There was no significant relationship with the complaints of asthma and eczema among men and women.
Relationship between individual symptoms and objectively assessed physical work environment
Among the general symptoms, the three most prevalent symptoms were fatigue, feeling heavy-headed, and headache (). The relationship between each of these symptoms and the objectively assessed physical work environment was analyzed by logistic regression adjusting for smoking, chronic illness, age, gender, job category, new furniture, new partition, and workstation. Formaldehyde concentration was significantly associated with feeling heavy-headed and headache (odds ratio 0.474, CI 0.236–0.953 and odds ratio 0.430, CI 0.212–0.872, respectively), but no other relationships were significant. Gender differences were not studied due to the low numbers of people experiencing several of the symptoms.
Among the complaints, the three most prevalent (draft, varying temperature, and passive smoking) were chosen. The relationship between each of these and objectively assessed physical work environment was analyzed by logistic regression adjusting for smoking, chronic illness, age, gender, job category, new furniture, new partition, and workstation (). Perceiving the temperature as being too inconsistent was associated with lower RH or higher RH and consistency of the supplied air temperature. Only the association with RH and air temperature were significant after adjustment. Perception of draft and passive smoking showed no association with lower RH/higher RH and higher/lower air temperature in univariate analysis and the results indicate no statistical significance after adjustment.
Table 11 Relationship between subjective perception and objective assessment (temperature, relative humidity, air movement, and dust measurement) by logistic regression
Relationship between subjective perceptions and objectively assessed physical work environment
The results stratified by gender () reveal that the total and general symptom scores were highly significant among male respondents. The concentration of CO caused a high number of complaints related to total and general symptoms (fatigue, feeling heavy-headed, and headache) among male respondents. Exposure to TVOCs influenced the overall condition of men compared to women. Men reported having all types of complaint (total, general, mucosal, and dermal) after exposure to TVOCs or aldehyde content while women only reported having mucosal discomfort from exposure to this chemical. The most common complaints related to the exposure of TVOCs were fatigue and cough (). Dust exposure influenced the total symptoms reported by women while no significant association was observed among the men. Symptoms from exposure to dust caused complaints of headache and feeling heavy-headed.
Table 12 Results stratified for gender: regression analyses of total, general symptoms, mucosal, dermal, and perceived physical complaint
Table 13 Result stratified for gender: regression analyses of individual complaints (12 symptoms)Table Footnote*
The physical indoor climate condition showed that male workers suffered from mucosal symptoms due to exposure to inconsistent air temperature while women showed a significant association with the perceived physical subjective complaint from exposure to air temperature and air movement (). RH showed a significant effect on the subjective perceived physical symptoms between both genders but there was no association between stratified genders. Air movement influenced the mucosal symptoms for both men and women.
The overall condition showed that temperature and RH strongly influenced the reported symptoms (total, general, mucosal, dermal, and subjective perceived indoor air climate) for both genders. Women showed more sensitivity to different air temperature conditions compared to men (). No association or relationship was observed for other conditions between exposure and complaints.
Discussion
This study shows an association between symptoms and chemical exposure in the indoor environment of nonindustrial workplaces (office buildings) in one of the busiest locations in Malaysia (Klang Valley). In addition, the physical work environment was found to be related to these symptoms for both the perceived physical environment and objective assessment, such as air temperature, air movement, and RH. Men had more symptoms and complaints than women although women’s symptoms and complaints had stronger associations to air temperature, air movement, and RH.
Generally, women’s but not men’s complaints about varying temperature of air were significantly associated with lower changes of air temperature. A lower RH was associated with the perception of too many changes of air temperature for both genders.
Gender differences
This study shows a different pattern of complaints between genders, in which men had a higher prevalence of symptoms compared to women.Citation8,Citation23,Citation31 Men reported the effect of chemical exposure on indoor air symptoms more than women and similarly in respect to perceived physical factors. This study indicates that men are more sensitive to environmental factors, they tend to perceive their health problems more intensely, and tend to report them more frequently than women.Citation32 However, a previous study indicated that women were more sensitive than men.Citation8 This might be due to the differences in hormonal levels, which could result in a different physiological threshold for observed symptoms.Citation26 The other possible explanation is the multiple exposure of chemical pollutants elsewhere (outdoors/other places/outdoor intense exposure). Men usually ride motorbikes to the office or use public transport, whereas most women prefer to use a personal car. In addition, the difference in reported complaints might be caused by a reporting tradition between the genders.Citation33 It is suggested that men have a more health seeking behavior and technical understanding in respect to IAQ issues for perceiving and reporting health problems. Previous research indicated that women reported more frequently than men due to progesterone and estradiol, which, although postulated as being linked to asthmatic symptoms,Citation32 is not in keeping with the findings of this study.
However, the differences found might also be due to the actual gender difference in the physical or cultural work environment, as supported by the spatial exposure data (200 separate buildings). In the current study population, the men undertook different types of work to the women, as more men had scientific positions (based on the type of workstation). This means that the men spent more of their work time in their offices, because of their higher position in the company, and, in addition, they also participated in activities outside the office buildings more than the women. A previous study suggests that the different hierarchical positions in the office certainly influences the physical indoor environment and thus affects the reporting of symptoms by workers.Citation25
Previous studies suggest that women report symptoms more frequently.Citation23,Citation31 Although men and women similarly reported psychosocial work factors, their perceived physical factors were quite different. This study’s findings contradicted those of a previous study in Europe.Citation34 The differences in reporting symptoms might be influenced by an understanding of the IAQ issues in the workplace. Men tend to have more knowledge, awareness, and alertness compared to women as the the IAQ codes have been embedded in the Occupational Safety and Health Act in Malaysia since 2005.Citation1,Citation2
Although the association between RH, air velocity, and symptoms as well as complaints was more prominent among men than women, women had more sick building syndrome symptoms and complaints than men. Few studies have stratified for gender in the analyses of the association between exposure and effects. This study suggests that the high number of symptoms and exposure to environmental parameters, including temperature, CO, aldehydes, and particulates, are similar to the findings for men in US commercial office buildings.Citation35
Air temperature was the only parameter associated to mucosal symptoms among men and associated with perceived physical symptoms among women. RH was the only parameter associated with perceived physical symptoms in both genders.
This study’s findings differ to a previous study conducted by Scandinavian researchers who found a strong association between the increased number of symptoms scales for women, but not for men.Citation8 The current results might support the hypothesis that the differences in illness perception or reported symptoms may be due to a reporting bias in which men are more likely to perceive and report symptoms more freely than women, who possibly underreport symptoms. In future studies, it is suggested that the influence of gender on exposure, symptoms, and perception of the indoor environment should be differentiated and should be specific to the separate targets of the investigation.
Stratifying for gender analysis reveals that there were some major differences in reporting symptoms and exposure to the chemical or physical condition of the working environment. Men had a positive association of mucosal complaints while women did not. TVOCs, however, had a positive association among men for all types of complaint (whether general, mucosal, dermal, or total symptoms) compared to women who only reported general symptoms (probably related to the difficulty in concentration and feeling heavy-headed). This symptom’s prominence among men may be due to the fact that the exposure of such pollutants is prominent among men compared to women.
Among women, dust is highly associated with the general reported symptoms, with dust levels > 0.071 mg/m3 having a very high positive relationship with the general symptoms reported by women. However, there was no association among men. This indicates that the risk of exposure is greater among women (due to the fact that their workstations had more particulates than men).Citation36
Relationship between symptoms and indoor climate factors
In the current study, exposure to factors in both the airborne chemical and physical work environments seem to be important for symptoms to occur. This may fit a theoretical model postulating that occupational exposure to chemical or physical stressors may function as a modifying factor between the environmental factors and symptoms, increasing the individual’s sensitivity to factors in the physical work environment.Citation37,Citation38
As the study design was cross-sectional, the causality or cause and effect cannot be determined. Nevertheless, this study helps to provide some indication that certain aspects of this theory (exposure to chemical airborne pollutants and their effect on health) might be present even in the exposure of low chemical dispersion (as demonstrated in the stratified gender analyses), which is supported by findings from a previous study in Finland.Citation39
Improvement to this study can be made by evaluating the personality factor by inserting it into the model of indoor air symptom development.Citation40 This has been suggested by numerous researchers who have observed that high occurrences of indoor air symptoms are related to personality factors.Citation41
The current study does not evaluate the psychosocial effects, such as strain, demand, and control, as described previously by Scandinavian researchers.Citation8 In addition, this study had no information concerning the personality of workers, and could not evaluate this aspect. The authors would like to suggest that future researchers include psychosocial aspects by using appropriate tools for assessing strain, demand, and control among workers, which probably have some effect on the health of workers (mental/psychological aspects). Previous studies have examined physical environmental factors, psychosocial factors, and indoor air symptoms at the same time, which successfully addressed certain problems related to sick building syndrome.Citation2,Citation5,Citation8,Citation42 This is important as a previous study of buildings in Finland, which examined aspects of the psychosocial work environment by an interview and questionnaire with three types of indoor environmental problems, showed that psychosocial factors can be used to determine mental strain and stress at work, which might influence the perceived symptoms.Citation43
A previous study in Sweden proved their hypothesis that psychosocial work factors, such as work stress, work cooperation, and work satisfaction, are important in studying symptoms related to indoor environment problems.Citation23 This is supported by another study, which suggested that the physical environment appeared to be less important than the psychosocial work environment in comparing the prevalence of symptoms.Citation24
Even though the psychosocial effect was not measured, the current study has strength in terms of showing the relative exposure to indoor air pollutants (including the physical indoor climate) and their effect on general or specific sick building syndrome symptoms. This is supported by previous findings in which measuring the exposure of airborne chemicals and physical indoor climate at the same time is important to predict the prevalence of sick building syndrome and perceived symptoms.Citation42 The present study also has other strengths in that the comprehensive investigation included the evaluation of quantitative airborne chemical dispersion, subjective measurement, qualitative assessment (described elsewhere), and objective measurement of physical work indoor climate (especially in a tropical climate country), unlike a previous study.Citation8
Air temperature had a positive association with the mucosal complaints among men and perceived complaints among women. This difference might be due to the hormonal changes in women, which make them more sensitive than men.Citation32 Stratified regression showed no association between gender and the RH changes for all types of complaint except for total complaints in respect to perceived environmental condition. This suggests that neither men nor women perceived differently in reporting RH. Gender might not be an important aspect when predicting RH problems in an indoor environment. A previous study showed that RH is one of the important parameters that influence reported symptoms, chemical dispersion, and indoor climate.Citation14
The air movement and indoor climate showed a positive association among men and women for mucosal symptoms. This is supported by a previous study that suggests that the olfactory gland is easily affected by the effect of air, whether strong or low.Citation18 Low air movement leads to a stagnant air effect and creates “dead air spaces,” while high air movement leads to dryness of the nose and dry skin. Women tend to complain more compared to men in respect to thermal comfort issues. This study is supported by previous findings.Citation44
Prevalence of symptoms
Most of the general symptoms, such as fatigue, feeling heavy-headed, headache, nausea/dizziness, and difficulty concentrating, were more prevalent in the current study population compared with a reference population from nine “healthy buildings” in Sweden.Citation30 In addition, the current study recorded a greater prevalence of symptoms when compared to a large study in Finland.Citation45 The best explanation for this might be due to the reporting culture, climate factors, understanding of IAQ issues, building design,Citation46 health awareness, and personality traits.Citation23,Citation47 Furthermore, the materials used for indoor furnishings might also contribute to the indoor air symptoms as well as the real problem of the indoor environment, as several responses to the questions about sick building symptoms problems had a high prevalence. It has been demonstrated that the current study recorded a 20% higher prevalence of sick building syndrome in the workplace than previous studies on buildings in four-season countries,Citation45 and 15% higher than for previous studies on buildings in tropical countries.Citation3,Citation5
Physical work environment
As CO2 is used as the standard in Malaysia to identify ventilation efficiency, the parameter is considered as a physical work environment factor.Citation2 The daily temperature and CO2 level were similar among men and women. The CO2 level was low, which shows that the offices were well ventilated even though air movement/velocity was low and clearly below the recommended level of 0.15–0.5 m/second, as suggested by DOSH. The air temperature (mean 24.35°C, range 19.60°C–32.30°C) was not within the levels recommended in the Malaysia Occupational Safety and Health guidelines.Citation2 Complaints about air velocity were low, but significantly higher among men than among women. The RH was low (mean 57.71%, range 30.0%–78.6%) due to the high outdoor temperature combined with a low ventilation rate. This study recorded higher RH compared to other four-season countries (mean 21.9%, range 15%–35%).Citation8 The sensation of the temperature being perceived as too low was associated with low RH, as demonstrated by researchers in Finland in their experimental study.Citation48
Humidification of the air resulted in the RH increasing from 12% to 39%, which then led to fewer complaints about thermal discomfort at temperature settings below 22.0°C. Data from this study suggest that RH was negatively associated with the sensation of dryness when RH was in the 30.0%–78.6% range, but might lead to complaints of stuffiness/excessive sweating in accordance with the experimental humidification field studies.Citation14,Citation15,Citation49 The high RH in tropical countries causes the evaporative mechanism of the sweat from the skin to be less efficient as the water vapor composition indoors is too great (which cannot “pick up” the excess water vapor from the sweat). If the RH setting is above the level recommended by DOSH (70%), possible thermal discomfort will occur as suggested in previous indoor air studies using a checklist.Citation4,Citation5
It was also found that a higher RH that exceeds the recommended range by DOSH might increase the perception of stuffiness. Complaints about air velocity were higher for men than for women, and women complained more about drafts, inconsistent temperature, and temperature being too low. The air velocity was always lower than the recommended maximum values of 0.15 m/second (DOSH),Citation2 and was not associated with the symptoms or complaints about perceived drafts. This physical unstable indoor climate can influence the dispersion of chemicals, and imbalances in the ventilation can create a localized episode of sick building syndrome. A previous study in commercial buildings suggests that the ventilation rate together with poor thermal comfort balance influence the sick building syndrome in office workers.Citation3
The current study shows that air movement was associated with complaints about varying temperature indoors. With sedentary lifestyles and activities, occupants generally feel thermally neutral or cooler, with air movement being perceived as unacceptable at a temperature of up to 26°C–32°C, even at low air movement, as suggested by previous researchers.Citation50 This study shows a similar pattern with a previous study, in which a cool overall thermal sensation influenced the subjective perception of air movement in a backward condition (negative influence).Citation8 However, another report showed that women tend to report feeling cooler and are more sensitive than men. Unfortunately, this study did not identify any effect of gender on perception of drafts similar to a previous study.Citation50 This situation suggests that when air movement was set to a lower level, it could help to remediate action for feeling too cold among office workers.
Chemical airborne work environment (modifiable agent potentially influences health symptoms)
Complaints about dust (PM10) were significantly higher among women than among men. This suggests that women are more responsive than men, which indicates the fatigue/general symptoms are associated with the exposure of PM10 among women rather than men. Women tend to be more reactive/sensitive to smoking activities, which might be associated with higher concentrations of PM10 in their workstation. The reaction of positive symptoms among women suggests that PM10 can easily cause women to complain, especially in respect to symptoms pertaining to the upper respiratory condition and other related sick building syndrome symptoms. This is supported by previous findings which reported that women are more likely to complain than men in indoor environments with higher particulate matter levels.Citation16
The relationship of CO to the symptoms suggests that the infiltration of the air conditioning system highly influences the reported symptoms of workers, especially those related to general and mucosal symptoms. This hypothesis is supported by a previous theory concerning the heating, ventilation, and air conditioning system industry and other mechanical engineers, which suggests that the infiltration of CO influences the efficiency of the heating, ventilation, and air conditioning system, thus indicating the ability of the indoor climate to remove pollutants and dilute pollutants indoors.Citation47 The mixture of phenol and dust is probably caused by smoking/passive smoking activity.Citation3 A significant amount of CO infiltration indicates poor arrangement of the fresh air intake and a significant amount of outdoor air being introduced indoors. These gases (CO2, CO, and particulate) are modifying factors (based on the fact that these pollutants can be controlled and managed properly) that can be managed by engineers, architects, and building management prior to development, maintenance, and occupancy. Therefore, this building health-related information should be stringent and considered by building professionals before the design and development begins, especially in a humid and temperate climate such as Malaysia.
TVOCs, which are from the aldehyde group, indicate formaldehyde dispersion. The temperature and RH influence the dispersion of formaldehyde and other aldehyde compounds, as demonstrated by a formaldehyde study conducted previously.Citation36 The aldehyde group of chemicals can be successfully controlled and managed by the proper selection of chemical-related products. The sensible selection of coating materials on the furniture, wall, and office equipment will make a considerable difference.
Temperature is related to chemical dispersion indoors. Based on the results shown, the temperature in new buildings is slightly lower at 26.4°C compared to old buildings (based on the pilot study data). This might be due to the poor efficiency of the maintenance on the mechanical ventilation and air conditioning (MVAC) system. This temperature issue might lead to chemical dispersion of formaldehyde or other aldehydes containing material, as suggested by previous researchers.Citation51,Citation52 Many possible formaldehyde dispersion models have been suggested by researchers. The dispersion and exposure may depend on the potency of the formaldehyde-emitting products present, the extent of their use, and the loading factor (m2/m3), which is described by the surface area (m2) of formaldehyde-emitting materials relative to the volume (m3) of interior spaces.Citation53 Other reasons might include environmental factors (formaldehyde emissions and their level increase with increasing temperature and RH) and material age (formaldehyde emissions and their level decrease with time).Citation54 Other factors include the interaction effects, which suggest the formaldehyde sources will interact or react with the most potent source suppressing emissions from less potent sources. Other explanations concerning formaldehyde emissions may be due to the ventilation condition where the lowest levels are experienced in cold conditions and the possible infiltration rates are high on warm days when occupants open windows.Citation3,Citation52,Citation54 The most important source in this developing country is probably the effect of smokers, who are exposed to significant formaldehyde concentrations.Citation3,Citation5
This study shows that formaldehyde and TVOCs are prominent in triggering mucosal- and general-related indoor air symptoms, which suggests that exposure to TVOCs leads to headaches, fatigue, and other neurological disorders and symptoms. This is supported by a previous study.Citation36 Therefore, the management of exposure to indoor air pollutants within tropical climate buildings is important to reduce such symptoms that may lead to chronic health effects and prominent repeated mucosal and general symptoms within the building community.
Due to the limitations of the study design, the causality shown between exposure to TVOCs in respect to neurological disorders or associated chronic diseases cannot be established; however, the pattern of recognition of the important sources could help epidemiologists or IAQ professionals predict the future effect of TVOCs and aldehyde contents on the health of workers. Current technology, such as interior design for healthy living and green buildings, should be integrated to improve the quality of air indoors. Chemical dispersion coming from interior surfaces, such as paint, wallpaper, and ventilation,Citation3,Citation36 should be considered by engineers, architects, and industrial hygienists to ensure that air quality issues can be maintained to higher standards.
TVOCs or formaldehyde are believed to be associated with neurological symptoms such as fatigue. This is supported by previous findings.Citation36 Dust is positively associated with neurological symptoms among women, which indicates that women are more susceptible and sensitive to dust than men. Proper management of filters in the MVAC system should be improved in order to reduce the number of complaint-related symptoms among women, as suggested by Syazwan et al.Citation4,Citation5
Consideration of the use of low emitting VOCs, especially on coated wall areas can prevent over accumulation of the VOCs material indoors. Suitable air movement, air temperature, and RH can help maintain the indoor environment in a healthy condition. The coated/material that reflects heat (especially radiant heat, ie, from outdoor sun) needs to be well planned so that the heat is not introduced indoors, preventing the effect of chemical dispersion of the indoor furniture, especially in tropical climate countries.
Stratification of gender and related symptoms revealed that some symptoms were associated with exposure to chemicals indoors. CO2 is associated with reported cough symptoms among men and women. This reflects the efficiency of the MVAC maintenance, which in turn influences the ventilation of the indoor climate.Citation3,Citation18,Citation19 In addition, men reported feeling heavy-headed when CO2 is a prominent indicator. CO showed the highest reported symptoms in the exposure symptoms analysis. This is supported by previous researchers who linked CO with infiltration problems, which constitute the main indicator of MVAC efficiency and pertain to the location of its fresh air intake.Citation5,Citation37
From analysis of the exposure symptoms, there are a few parameters that should be focused on in the development of the IAQ index as the main indicators of problematic buildings.Citation54,Citation55 Temperature and RH should be the best evaluation in predicting the quality of the air being served by mechanical ventilation. Air movement should be monitored on a periodic basis to identify potential dead space, which can accumulate chemicals indoors. CO2 should be an indicator of the efficiency of the ventilation. CO should be monitored as the main sign of outdoor air intrusion or smoking activities. TVOCs, formaldehyde, or chemical-based materials should be evaluated, especially in strong odor areas, which are suspected of being responsible for more complaints of fatigue or neurological-related complaints. Dust should be evaluated more stringently in areas used by women as they appear to be more sensitive, as demonstrated by the 20% reporting of symptoms.
Methodological considerations
This study was performed in an office setting, and some bias might be present as information on the symptoms and perception of the work environment was collected using the same questionnaire. However, the study has a major strong point in that the perceived physical work environment and airborne chemical monitoring with perception on odor was supplemented with objective measures. This study also has other major strengths in that it monitored the main indoor environmental factors (gases, chemical and physical indoor environment) for the analysis, which probably reflects the main possible problems in an indoor work environment (psychological factors, microbiological agents, and stress level). Further, the participation rate was high, reducing the probability of selection bias. This study was performed in a population of office staff. The results are probably representative of other offices (new buildings and air conditioned offices) in the Klang Valley (Malaysia as a tropical climate country) and similar workplaces in any tropical region that has a similar pattern of high humidity and temperature. However, other types of workplaces may have different challenges, such as the psychosocial work environment, different outdoor climate, different building design, ventilation, interaction of different races, and different gender–environment interactions. In this study, the statistical evaluation considered some confounders, which were controlled statistically during the data analysis process.Citation56 The confounders included workstation status, prescribed activities, and chronic diseases reported by the occupants.
This study had certain limitations in terms of the chemical monitoring, due to the use of surrogate measurements in the partial period grab sampling method. Overall changes in the temporal patterns of the chemical and physical parameters may exist.
Conclusion
The physical work environment, such as air temperature and RH, assessed as a combination of chemical dispersion of TVOCs, formaldehyde, and outdoor intrusion of CO, can be associated with symptoms and perceptions of indoor environments. Moreover, objectively assessed indoor environments might differ between genders in office buildings. The higher prevalence of environmental symptoms and complaints among men does not necessarily indicate a stronger association with climate factors. Chemical airborne dispersion (CO, formaldehyde, and TVOCs) factors and physical environmental factors as well as gender differences should be considered when evaluating an indoor environment. A holistic approach, which should consider other elements, such as psychological factors and personality factors is advisable in dealing with indoor occupational environments.
Recommendations/suggestions
In order to maintain or create a suitable indoor environment to prevent the occurrence of severe indoor, repeated symptoms that will reduce productivity, some important recommendations should be considered by the facility managers, maintenance workers, building designers, architects, and interior designers. New buildings should be using low-emitting VOC paint. Improvement of the fresh air intake should be considered during the planning stage of the building construction to avoid infiltration of CO within the facilities.
From this study, a model of exposure symptoms can be established in which temperature, RH, and air movement should be modeled as primary indicators. Any changes to the range suggested by the current standard are likely to cause IAQ problems. Due to the nature of the chemicals/gases, TVOCs and formaldehyde should be treated as secondary parameters to be evaluated and scored. Others include CO2, CO, dust, and microbial contaminants.
Acknowledgements
The project was made possible thanks to a collaborative effort from Nippon Paint (Malaysia) Sdn Bhd (NPM) under the main research programme entitled “Indoor air TVOCs and formaldehyde monitoring programme and its impact on respiratory health, allergies, and asthma among building occupants” in addition to a scholarship from the Research Management Center (RMC), Universiti Putra Malaysia, and Ministry of Higher Education (MOHE) and support from the private sectors in indoor air industries (Kim Chew Communication Sdn Bhd). Special thanks to the indoor air scientists and indoor air quality assessors (JKKP HIE 127/171 – 4[18]) registered under the Department of Occupational Safety and Health, Malaysia (DOSH, Malaysia). The authors would like to thank Maznah Ab Jamal for her guidance concerning the publication of this article. Special thanks also go to Ismail Musa, Mohd Khairi Ismail, Zulfadhli Ismail, and Hasanul Manzar Ismail for their ideas and critical evaluation of this article.
Disclosure
The authors report no conflicts of interest in this work.
References
- Department of Occupational Safety and Health, MalaysiaIndustry Code of Practice on Indoor Air QualityPutrajayaMinistry of Human Resources2010
- Department of Occupational Safety and Health, MalaysiaCode of Practice on Indoor Air QualityPutrajayaMinistry of Human Resources2005
- SyazwanAIJulianaJNorhafizalinaOAzmanZAKamaruzamanJIndoor air quality and sick building syndrome in Malaysian buildingsGlob J Health Sci200912126135
- SyazwanAIRafeeBMHafizanJDevelopment of an indoor air quality checklist for risk assessment of indoor air pollutants by semi-quantitative score in nonindustrial workplacesRisk Manag Healthc Policy201251172322570579
- SyazwanAIRafeeBMHafizanJAnalysis of indoor air pollutants checklist using environmetric technique for health risk assessment of sick building complaint in nonindustrial workplaceDrug Healthc Patient Saf2012410712623055779
- LazarusRSPsychological Stress and the Coping ProcessNew York, NYMcGraw-Hill1966
- CoxTStress, coping and problem solvingWork Stress19871514
- BakkeJVMoenBEWieslanderGNorbackDGender and the physical and psychosocial work environments are related to indoor air symptomsJ Occup Environ Med200749664165017563607
- KivimakiMLeino-ArjasPLuukkonenRRiihimakiHVahteraJKirjonenJWork stress and risk of cardiovascular mortality: prospective cohort study of industrial employeesBMJ2002325736985712386034
- MichieSWilliamsSReducing work related psychological ill health and sickness absence: a systematic literature reviewOccup Environ Med20036013912499449
- BurgePSHedgeAWilsonSBassJHRobertsonASick building syndrome: a study of 4373 office workersAnn Occup Hyg1987314A4935043439759
- SkovPValbjornOPedersenBVInfluence of personal characteristics, job-related factors and psychosocial factors on the sick building syndromeScand J Work Environ Health19891542862952772583
- BornehagCGSundellJBoniniSDampness in buildings as a risk factor for health effects, EUROEXPO: a multidisciplinary review of the literature (1998–2000) on dampness and mite exposure in buildings and health effectsIndoor Air200414424325715217478
- ReinikainenLMJaakkolaJJSignificance of humidity and temperature on skin and upper airway symptomsIndoor Air200313434435214636228
- ReinikainenLMJaakkolaJJEffects of temperature and humidification in the office environmentArch Environ Health200156436536811572281
- GyntelbergFSuadicaniPNielsenJWDust and the sick building syndromeIndoor Air199444223238
- WolkoffPClausenPAJensenBNielsenGDWilkinsCKAre we measuring the relevant indoor pollutants?Indoor Air19977292106
- FangLClausenGFangerPOImpact of temperature and humidity on chemical and sensory emissions from building materialsIndoor Air19999319320110439557
- FangLWyonDPClausenGFangerPOImpact of indoor air temperature and humidity in an office on perceived air quality, SBS symptoms and performanceIndoor Air200414Suppl 7748115330775
- WyonDPThe effects of indoor air quality on performance and productivityIndoor Air200414Suppl 79210115330777
- JaakkolaMSJaakkolaJJOffice equipment and supplies: a modern occupational health concern?Am J Epidemiol1999150111223122810588083
- World Health OrganizationAir Quality Guidelines for Europe2nd edGenevaWorld Health Organization2000 Available from: http://www.euro.who.int/document/e71922.pdf. Accessed December 1, 2012.
- RunesonRNorbackDKlintebergBEdlingCThe influence of personality, measured by the Karolinska Scales of Personality (KSP) on symptoms among subjects in suspected sick buildingsIndoor Air200414639440415500632
- MarmotAFEleyJStaffordMStansfeldSAWarwickEMarmotMGBuilding health: an epidemiological study of “sick building syndrome” in the Whitehall II studyOccup Environ Med200663428328916556750
- StenbergBWallSWhy do women report “sick building symptoms” more often than men?Soc Sci Med19954044915027725123
- IhlebaekCEriksenHRUrsinHPrevalence of subjective health complaints (SHC) in NorwayScand J Public Health2002301202911928829
- AnderssonHRPottierACStrachanDPAsthma from birth to age 23: incidence and relation to prior and concurrent atopic diseaseThorax19924775375421412098
- TollefsenELanghammerARomundstadPBjermerLJohnsenRHolmenTLFemale gender is associated with higher incidence and more stable respiratory symptoms during adolescenceRespir Med2007101589690217084607
- MessingKDumaisLCourvilleJSeifertAMBoucherMEvaluation of exposure data from men and women with the same job titleJ Occup Med19943689139177807275
- AnderssonKEpidemiological approach to indoor air problemsIndoor Air19988Suppl 43239
- BrascheSBullingerMMorfieldMGebhardtHJBischofWWhy do women suffer from sick building syndrome more often than men? Subjective higher sensitivity versus objective causesIndoor Air200111421722211761596
- ZimmermannJLWoodruffPGClarkSCamargoCARelation between phase of menstrual cycle and emergency department visits for acute asthmaAm J Respir Crit Care Med20001622 Pt 151251510934079
- Mendoza-SassiRABeriaJUGender differences in self-reported morbidity: evidence from a population-based study in southern BrazilCad Saude Publica200723234134617221083
- VerbruggeLMGender and health: an update on hypotheses and evidenceJ Health Soc Behav19852631561823905939
- ReynoldsSJBlackDWBorinSSIndoor environmental quality in six commercial office buildings in the midwest United StatesAppl Occup Environ Hyg200116111065107711757903
- NorbackDSubjective indoor air quality in schools – the influence of high room temperature, carpeting, fleecy wall materials and volatile organic compounds (VOC)Indoor Air199554237246
- BakerDBSocial and organizational factors in the office building-associated illnessOccup Med1989446076242690377
- RollinsVSwiftGHPsychological issues: a multifaceted problem, a multidimensional approachRostronJSick Building Syndrome: Concepts, Issues and PracticeLondonE and FN Spon19976984
- LahtinenMSundman-DigertCReijulaKPsychosocial work environment and indoor air problems: a questionnaire as a means of problem diagnosisOccup Environ Med200461214314914739380
- CrawfordJOBolasSMSick building syndrome, work factors and occupational stressScand J Work Environ Health19962242432508881012
- RunesonRNorbackDAssociations among sick building syndrome, psychosocial factors, and personality traitsPercept Mot Skills20051003 Pt 174775916060437
- OoiPLGohKTSick building syndrome: an emerging stress-related disorder?Int J Epidemiol1997266124312499447404
- LahtinenMHuuhtanenPKahkonenEReijulaKPsychosocial dimensions of solving an indoor air problemIndoor Air2002121334611951709
- FangLWyonDPClausenGFangerPOImpact of indoor air temperature and humidity in an office on perceived air quality, SBS symptoms and performanceIndoor Air200414Suppl 7748115330775
- ReijulaKSundman-DigertCAssessment of indoor air problems at work with a questionnaireOccup Environ Med2004611333814691270
- SkybergKSkulbergKREduardWSkaretELevyFKjuusHSymptoms prevalence among office employees and associations to building characteristicsIndoor Air200313324625212950587
- International Organization for StandardizationModerate Thermal Environments – Determination of the PMV and PPD Indices and Specification of the Conditions for Thermal ComfortGenevaInternational Organization for Standardization1994
- PalonenJSeppanenOJaakkolaJJKThe effects of air temperature and relative humidity on thermal comfort in the office environmentIndoor Air199334391397
- NorbackDWieslanderGNordstromKWalinderRVengePThe effect of air humidification on symptoms and nasal patency, tear film stability, and biomarkers in nasal lavage: a 6 weeks’ longitudinal studyIndoor Built Environ200092834
- ToftumJAir movement – good or bad?Indoor Air200414Suppl 7404515330770
- GodishTIndoor Air Pollution ControlChelsea, MILewis Publishers1989
- GodishTResidential formaldehyde contamination: sources and levelsComments Toxicol19882115134
- GodishTIndoor contamination problem in school buildingsPaper presented at: 89th Annual Meeting of the Air and Waste Management AssociationJune 23–28, 1996Nashville, TN
- GodishTZollingerTWKonopinskiVResidential formaldehyde: increased exposure levels aggravate adverse health effectsJ Environ Health1990533437
- LooCKFotyRGWheelerAJDo questions reflecting indoor air pollutant exposure from a questionnaire predict direct measure of exposure in owner-occupied houses?Int J Environ Res Public Health2010783270329720948960
- SalamehPKhayatGWakedMCould symptoms and risk factors diagnose COPD? Development of a diagnosis score for COPDClin Epidemiol2012424725523071403