
Abstract
Erectile dysfunction (ED) is often perceived by both patients and sexual partners as a serious problem that can jeopardize quality of life, psychosocial or emotional well-being, and the partnership in the long term. Since their introduction, oral phosphodiesterase type 5 inhibitors (PDE5Is) have been found to be highly effective and well tolerated, and are available as the first-line therapy for the treatment of ED. Udenafil is one of the selective PDE5Is made available in recent years for the treatment of ED. Udenafil has clinical properties of both relatively rapid onset and long duration of action due to its pharmacokinetic profile, thereby providing an additional treatment option for ED men to better suit individual needs. There is positive evidence that udenafil is effective and well tolerated in the treatment of ED of a broad spectrum of etiologies or severity. Udenafil is as effective in the treatment of diabetes mellitus-associated ED as other PDE5Is. Due to the clinical property of relatively long duration of action, udenafil may be another option in daily dosing treatment for ED, as suggested by its favorable efficacy and safety profile. Most adverse effects reported from clinical trials are mild or moderate in severity, without any serious adverse event, with headache and flushing being the most common. Also, the concomitant use of anti-hypertensive drugs or alpha-1-blockers does not significantly affect the efficacy and safety profile of udenafil. However, additional studies with larger cohorts including prospective, multicenter, comparative studies with patients of different ethnicities are needed to further validate the favorable findings of udenafil in the treatment of ED.
Video abstract
Point your SmartPhone at the code above. If you have a QR code reader the video abstract will appear. Or use:
Keywords:
Introduction
Erectile dysfunction (ED) is defined by the inability to achieve or maintain an erection sufficient for satisfactory sexual performance and is a common clinical entity that primarily affects men older than 40 years of age.Citation1,Citation2 ED is associated with various comorbidities or conditions, including advanced age, hypertension, hyperlipidemia, metabolic syndrome, lower urinary tract symptoms (LUTS) of benign prostatic hyperplasia (BPH), cardiovascular disease, central neuropathologic conditions, psychological factors, diabetes mellitus (DM), a result of radical prostatectomy, and the use of medications prescribed for the treatment of depression and hypertension.Citation3–Citation10 Furthermore, recent studies have suggested that ED can be a strong predictor of cardiovascular disease and that the development of symptomatic ED may precede the occurrence of a cardiovascular event by 2–3 years.Citation11–Citation15
Many treatment modalities have been introduced to address ED due to its considerable impact on overall quality of life and psychosocial aspects, such as emotional well-being or interpersonal relationships. Currently, treatment options available for ED include vacuum pump devices, intracavernosal injection of vasoactive agents, intraurethral suppositories, penile prosthesis, vascular surgery, hormones, and phosphodiesterase (PDE) type 5 inhibitors (PDE5Is).Citation16,Citation17 Among these, the advent of PDE5Is, which offer advantages over other treatment modalities in terms of ease of administration and costs, has revolutionized the medical treatment for ED.Citation18,Citation19 PDE5Is are considered to be the first-line therapy for most men with ED across a broad spectrum of underlying diseases and severity. To date, there are four PDE5Is (sildenafil, vardenafil, tadalafil, and avanafil) approved for the treatment of ED worldwide, and udenafil has been approved in 13 countries, including Korea.Citation20,Citation21 Mirodenafil has been approved only in Korea, and lodenafil and SLx-2101, new PDE5Is, are still under investigation.Citation22–Citation25
Udenafil (Zydena; Dong-A Pharmaceutical, Seoul, Korea), one of the selective PDE5Is, was developed in Korea and approved for the treatment of ED in 2005. Its pharmacokinetic profiles include a time to maximum drug plasma concentration (tmax) of 0.8–1.3 hours and a half-life (t1/2) of 9.9–12.1 hours, which would confer clinical properties of both relatively rapid onset and long duration of action.Citation26 Its molecular structure is similar to that of sildenafil citrate (Viagra; Pfizer Inc, New York, NY, USA), and the isoenzyme selectivity profile of udenafil is comparable to that of sildenafil.Citation26 Clinical efficacy and safety of udenafil have been evaluated in men with ED of a broad spectrum of etiologies or severity in several randomized, controlled trials;Citation27–Citation33 thus, the availability of a variety of PDE5Is, including udenafil, can assist clinicians in tailoring treatment regimens to the specific needs of each patient with ED and in prescribing the PDE5I that has the highest efficacy for erection or satisfaction and the least overall adverse effects in a given patient. In this review, we highlight the preclinical and clinical evidence for the efficacy and safety of udenafil in the treatment of ED.
Physiologic basis for effects and adverse effects
PDEs comprise a family of metallophosphohydrolases that cleave the 3′,5′-cyclic phosphate moiety of cyclic adenosine monophosphate (cAMP) and/or cyclic guanosine monophosphate (cGMP) to produce the corresponding 5′ nucleotide.Citation34 PDE5 selectively cleaves cGMP, a key intracellular secondary messenger in penile erection, by which the effect of nitric oxide (NO) on relaxation of cavernous smooth muscles and dilation of helicine arterioles is mediated.Citation34,Citation35 PDE5I has a similar structure to cGMP and inhibits the breakdown of NO-derived cGMP by competitively binding the catalytic site of PDE5, thereby allowing the accumulation of cGMP in the cytoplasm of cavernosal and vascular smooth muscle cells for continuous activation of the NO/cGMP mechanism, which can lead to increased penile blood flow during sexual stimulation and, ultimately, enhanced penile erection.Citation36
Given this physiologic background, therapeutic effects of PDE5Is such as udenafil depend on their specificity for PDE5 and their pharmacokinetics, as well as on the distribution of different PDE isoforms in the cavernous tissue. As different PDE isoforms are distributed throughout a variety of tissues and PDE5 is present in high concentration in the cavernous smooth muscle, the selectivity of PDE5Is for PDE5 over the other PDE isoforms is a prerequisite for an increased therapeutic window.Citation34 Further, the selectivity for PDE5 over the other PDE isoforms and degree of inhibition of PDE5 in tissues other than corpora cavernosa are key factors determining the safety and tolerability of PDE5Is. If PDE5Is have a large enough difference in the affinity to PDE5 compared to other PDE isoforms, there is less likely to be a significant inhibition of the other PDE isoforms and, thereby, less likelihood of unwanted adverse effects at therapeutic plasma concentrations.
A preclinical study showed that an inhibitory concentration for PDE5 of udenafil was approximately 150-, 17-, 9- and 10-fold lower than those for PDE1, PDE2, PDE3, and PDE6, respectively.Citation26 Moreover, with regard to PDE1 associated with vasodilation and flushing, PDE1 selectivity of udenafil (selectivity ratio of 149) is similar to that of sildenafil (selectivity ratio of 111).Citation26 Also, the selectivity data of udenafil for PDE5 over PDE2, PDE3, and PDE6 are comparable to those of sildenafil.Citation26 As for PDE11, udenafil (selectivity ratio of 96) has higher selectivity than tadalafil (selectivity ratio of 7.1), but the clinical significance of PDE11 inhibition has not yet been established.Citation31,Citation37 Thus, udenafil is one of the selective PDE5Is, based on its low affinity for the other PDE isoforms.
Chemistry
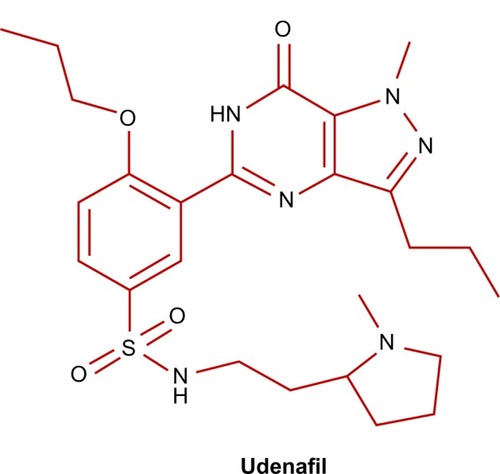
Udenafil (5-[2-propyloxy-5-(1-methyl-2-pyrollidinylethylamidosulphonyl)phenhyl]-1-methyl-3-propyl-1,6-dihydro-7H-pyrazolo(4,3-d)-pyrimidin-7-one) is a pyrazolopyrimidine derivative and has a molecular structure similar to that of cGMP, like sildenafil ().Citation37,Citation38 Udenafil has a molecular mass of 516.657 g/mol and its product is available in tablet formulation of 100 mg and 200 mg.
Figure 1 Structural formula of udenafil.
Pharmacological profile
Pharmacokinetics
A recent Phase I clinical trial has demonstrated that udenafil is rapidly absorbed, reaching peak plasma concentrations at 0.8–1.3 hours, then declining monoexponentially with a t1/2 from 9.9 to 12.1 hours, which can confer clinical properties of both relatively rapid onset and long duration of action.Citation38 Also, the area under the time–concentration curve and the maximum concentrations in plasma (Cmax) of udenafil increased supraproportionally with increasing dose on single administration.Citation38 Udenafil reached steady state by day 5 of regular repeated administrations, without significant drug accumulation.Citation38 According to a previous preclinical study using rats, absolute oral bioavailability of udenafil was only 38% in rats, which was similar to that of sildenafil (23%–44%).Citation39,Citation40 This low oral bioavailability of udenafil appears to be mainly due to a considerable intestinal first-pass effect.Citation39 On the other hand, according to a model of interspecies scale-up of pharmacokinetics of udenafil, it was predicted that its volume of distribution in humans was large, as extrapolated from data on other species.Citation41 The time to Cmax of udenafil is delayed under a fat-fed condition;Citation42 however, although the Cmax can be reduced by approximately 21% in a low-fat-fed state, overall bioavailability is not affected when taken with food.Citation42
Pharmacodynamics
PDE5 is mainly found in the corpora cavernosa, the vascular and visceral smooth muscles, and platelets.Citation43,Citation44 Udenafil exhibits its inhibitory effect by binding competitively to the catalytic site of PDE5, thereby promoting the accumulation of cGMP in the smooth muscle cells of corpora cavernosa. The inhibition of various PDEs by udenafil was evaluated in comparison to that of sildenafil.Citation26 The half-maximal inhibitory concentration (IC50) for PDE5 of udenafil is 8.25±2.90 nM, which is similar to that of sildenafil (8.50±2.05 nM).Citation26,Citation38 PDE1 inhibition is associated with vasodilation, flushing, and tachycardia. The inhibitory effect of udenafil on PDE5 is about 150-fold greater than that on PDE1 (selectivity ratio of 149), which is similar to the PDE1 selectivity of sildenafil (selectivity ratio of 111).Citation26 Furthermore, PDE11 selectivity of udenafil (selectivity ratio of 96) is relatively high, indicating a very low probability of inhibition of PDE11 at therapeutic doses of udenafil.Citation31,Citation37 PDE11 is present in a variety of organs, including skeletal muscle, prostate, testis, corpora cavernosa, heart, and anterior pituitary, and its functions are not clearly known. On the other hand, the IC50 values for PDE2, PDE3, and PDE6 of udenafil were 101±15.1 nM, 52.0±3.53 nM, and 53.3±2.47 nM, which was similar to those of sildenafil (111±25.0 nM, 30.6±1.65 nM, and 72.4±2.94 nM), suggesting the selectivity ratios for PDE2, PDE3, and PDE6 were roughly 10 in both udenafil and sildenafil.Citation26 PDE3 hydrolyzes cAMP and is mainly found in cardiomyocytes, as well as in the corpora cavernosa. Cross-reactions with PDE3 by udenafil might increase the level of cAMP in the heart, thereby inducing an increase in heart rate with a positive inotropic effect.Citation32,Citation45 Also, udenafil could cross-react with PDE6, as sildenafil does, and might partially inhibit it at therapeutic doses. As inhibition of PDE6, which controls levels of cGMP in the retina, may cause visual adverse effects, such as chromatopsia and blurred vision, reported in a minority of patients taking udenafil, attention should be paid to PDE6, which is predominantly expressed in the cones and rods of retina.Citation31,Citation32,Citation38,Citation45,Citation46
Metabolism
Udenafil is mainly metabolized by cytochrome P450 3A4 (CYP3A4), and CYP3A5 partly contributes to its metabolism.Citation37,Citation47 There are three metabolites produced by the metabolism: DA-8164, M1 (hydroxyl DA-8159), and M2 (N-demethyl DA-819).Citation39,Citation48 Among these, DA8164 is known as the major active metabolite of udenafil.Citation48,Citation49 CYP3A4 is predominantly responsible for the formation of DA-8164 from udenafil.Citation48 DA-8164 has a half in vitro potency for inhibition of PDE5 compared to that of udenafil, and t1/2 of DA-8164 is nearly similar to that of udenafil (12 hours).Citation50 Udenafil appears to be mainly excreted into the feces, although this has not been conclusively proven, due to limited data on the pharmacological properties of udenafil.Citation37,Citation50 Urinary excretion of udenafil was low (<12%), and DA-8164 was extremely low (0.2%), suggesting both udenafil and DA-8164 are subject to nonrenal elimination.Citation50
Efficacy of udenafil in ED
The current American Urological Association and European Association of Urology guidelines recommend oral PDE5Is as a first-line treatment option for ED.Citation17,Citation51 Initially, the efficacy of udenafil was documented in a preclinical study using rat and dog models, which reported that oral or intravenous administration of udenafil increased the number of penile erections with increasing dosages, indicating significant therapeutic potential in the treatment of ED.Citation52 In a Phase I trial, udenafil was found to be safe, well tolerated, and rapidly absorbed, and systemic exposure to udenafil increased in a dose-proportional manner with both single and multiple doses.Citation50 A Phase II, double-blind, placebo-controlled, multi-center, parallel-group clinical trial showed that udenafil produced a highly significant improvement in erectile function, with an up to 91% vaginal penetration success rate.Citation53 The clinical efficacy of udenafil in patients with ED of a variety of underlying etiologies, severities, and ages of the patients has been suggested in several randomized, placebo-controlled trials.Citation27–Citation29,Citation31–Citation33 Patient characteristics, outcome measures, and results of these trials are summarized in and .
Table 1 Patient characteristics and outcome measures of six randomized, placebo-controlled trials
Table 2 Summary of efficacy of udenafil in six randomized, placebo-controlled trials
A Phase III, 12-week, multicenter, double-blind, randomized, placebo-controlled, parallel-group study by Paick et al evaluated the efficacy and safety of udenafil at two doses (100 mg and 200 mg) in 167 Korean men aged 19 to 70 years with at least a 6-month history of ED from organic, psychogenic, or mixed etiology.Citation27 The primary efficacy variable was the change from baseline in the erectile function domain (EF) scores of the International Index of Erectile Function (IIEF) questionnaire. Secondary efficacy variables included changes from baseline in scores on the IIEF for question 3 (penetration ability) and question 4 (maintenance frequency); changes from baseline in all domain scores of the IIEF; and patients’ responses to questions 2 and 3 of the Sexual Encounter Profile (SEP) (SEP2: successful vaginal penetration; SEP3: the ability to successfully complete intercourse). Patients’ responses to the Global Assessment Question (GAQ) were also assessed after 12 weeks of treatment. After 12 weeks of treatment, the patients treated with udenafil showed significantly greater change from baseline in the IIEF-EF scores compared with placebo (placebo: 0.20; 100 mg udenafil: 7.52; 200 mg udenafil: 9.93). Furthermore, the proportion of subjects exhibiting normal erection based on the IIEF-EF score after the 12-week period was 3.7%, 35%, and 48% in the placebo, 100 mg udenafil, and 200 mg udenafil treatment groups, respectively. Compared with placebo, udenafil significantly enhanced the rates of successful penetration (SEP2) (placebo: 53.38%; 100 mg udenafil: 88.83%; 200 mg udenafil: 92.40%) and maintenance of erection (SEP3) (placebo: 15.44%; 100 mg udenafil: 70.08%; 200 mg udenafil: 75.70%). Furthermore, significantly greater proportions of udenafil treatment groups responded positively to the GAQ compared with the placebo group (placebo: 25.9%; 100 mg udenafil: 81.5%; 200 mg udenafil: 88.5%). Thus, udenafil treatment resulted in a numerically dose-dependent increase in all efficacy variables, with mild-to-moderate treatment-related adverse events, indicating that udenafil may well be a reliable treatment option for ED of broad-spectrum etiology and severity.
A recent multicenter, randomized, double-blind, placebo-controlled, parallel-group study assessed the efficacy and safety of 8-week 100 mg udenafil treatment in 118 Turkish men aged 19 to 70 years with ED of organic or psychogenic etiology.Citation33 The primary efficacy variable was change from baseline in IIEF-EF scores. The secondary efficacy variables included changes from baseline in the other domain scores of the IIEF, in SEP2 and SEP3, and in the patients’ responses to GAQ. The udenafil group showed significantly higher increase in the IIEF-EF score compared to the placebo group (placebo: 3.8; 100 mg udenafil: 7.7). Similarly, greater improvements were observed for SEP2, SEP3, and two other IIEF domains (sexual desire and overall sexual satisfaction). The proportion of positive responses to GAQ was significantly greater in the udenafil group than in the placebo group (72.2% versus 49.1%). All adverse events observed during the study period were of mild or moderate severity.
Recently, a randomized, double-blind, placebo-controlled, parallel-group, fixed-dose-design, multicenter study by Park et al showed that the effectiveness of udenafil to improve erectile function of the subjects could be sustained for up to 12 hours after a single dosage of 100 mg, indicating that flexibility and spontaneity in the sex-life could be achieved.Citation28 In the study, participants were requested to attempt sexual intercourse at 12 hours after udenafil or placebo dosing, taken as needed, during the 4-week treatment period. The primary efficacy variable was response to SEP3. The secondary efficacy variables were response to SEP2 and change from baseline in IIEF-EF scores. Udenafil significantly enhanced the rate of maintenance of erection (placebo: 28.3% versus udenafil: 54.7% [SEP3]). Compared with the placebo, signifi-cant change in the IIEF-EF score was observed in the udenafil group (placebo: −0.58±0.67; 100 mg udenafil: 4.40±0.84). For SEP2, however, there was no difference from baseline, and no difference between the udenafil and placebo groups. Park et al concluded that udenafil could be a reliable treatment option in patients who are in need of a spontaneous recovery of erectile function and who desire sexual intercourse without concerns about the duration of efficacy.Citation28
According to a recent meta-analysis of five randomized, placebo-controlled trials by Ding et al, the pooled analysis showed that udenafil treatment provided an average increase in change from baseline in the IIEF-EF score of 5.65 points compared with placebo, which was statistically significant.Citation54 Similar results were observed in the comparison of SEP2 and SEP3, GAQ, and the proportion of shift to normal erection based on the IIEF-EF score (≥26). The pooled results showed average increases of 22.14% and 31.22% in positive responses to SEP2 and SEP3 respectively after the udenafil treatment compared with placebo. Also, the udenafil group showed greater increases in positive responses to GAQ and the proportion of shift to normal erection compared to placebo (risk ratios: 3.44 and 2.37, respectively).
Efficacy in ED patients with DM
The neurologic and vascular consequences of DM are considered to be a significant comorbidity for development of ED. DM contributes to ED through a complex interplay of elevated advanced glycation end-products; increased levels of oxygen free radicals; impaired NO synthesis; increased endothelin B receptor binding sites; upregulation of RhoA/Rho-kinase pathway; neuropathic damage; and impaired cGMP-dependent protein kinase-1, indicating that DM-associated ED is multifactorial.Citation55 Despite considerable progress in the knowledge and understanding of pathophysiology of ED, the treatment of DM-associated ED is often difficult due to its multifactorial etiology.
Several preclinical studies using animal models of DM-associated ED have provided a rationale for the use of udenafil as treatment for diabetic ED.Citation56–Citation58 Also, in a rat model of DM-associated ED, chronic administration of udenafil was shown be a potential therapeutic strategy to prevent the progression of diabetic ED by enhancing gene and protein expression levels of neuronal NO synthase and endothelial NO synthase in diabetic corpora cavernosa.Citation59 Interestingly, a recent study using a rat model of streptozotocin-induced diabetic ED has demonstrated that a time-dependent deterioration of erectile function during the course of diabetes was followed by decreased responsiveness to udenafil and severe ED refractory to udenafil, suggesting the necessity of early preventive treatment for DM-associated ED.Citation60
A Phase III, 12-week, multicenter, placebo-controlled, randomized, double-blind, double-dummy, parallel-group-design, fixed-dose trial by Moon et al evaluated the efficacy and safety of udenafil at two doses (100 mg and 200 mg) in 174 Korean men with ED.Citation29 The primary efficacy variable was change in the IIEF-EF score from baseline. The secondary parameters were IIEF questions 3 and 4, SEP2 and SEP3, rate of achieving normal erectile function, and patient response to GAQ. Both udenafil groups showed significantly greater change from baseline in the IIEF-EF score compared with placebo (placebo: 1.20; 100 mg udenafil: 7.00; 200 mg udenafil: 8.21). Similar results were observed in the comparison of IIEF questions 3 and 4, SEP2 and SEP3, and GAQ between the udenafil and placebo groups.
Efficacy in ED patients with hypertension
Hypertension is a prevalent condition in men with ED as well as a risk factor for the development of ED.Citation2 ED can also occur as an adverse effect of several antihypertensive drugs such as beta-blockers and thiazide.Citation2 Thus, given the close association between ED and hypertension, the issues of efficacy and safety of PDE5Is for treatment of ED in this patient population has assumed considerable importance.
A Phase III, 12-week, multicenter, double-blind, randomized, placebo-controlled, parallel-group study by Paick et al was performed to determine the efficacy and safety of udenafil of fixed doses (100 mg or 200 mg) in 165 Korean men with at least a 6-month history of ED who took one or more antihypertensive agents in a stable dose for arteriogenic hypertension.Citation32 The primary efficacy variable was change from baseline in IIEF-EF scores. The secondary efficacy variables included change from baseline in scores on the IIEF question 3 and question 4, changes in SEP2 and SEP3, and patient responses to GAQ. The udenafil groups showed significantly greater increase in the IIEF-EF score (placebo: 1.98; 100 mg udenafil: 8.71; 200 mg udenafil: 10.04) and scores on the IIEF question 3 (placebo: 0.1; 100 mg udenafil: 1.3; 200 mg udenafil: 1.4) and question 4 (placebo: 0.7; 100 mg udenafil: 2.0; 200 mg udenafil: 2.5) compared with placebo group. Similarly, greater improvements were observed for changes from baseline in the SEP2 (placebo: 3.13%; 100 mg udenafil: 25.85%; 200 mg udenafil: 29.82%) and SEP3 (placebo: 12.55%; 100 mg udenafil: 57.86%; 200 mg udenafil: 71.82%). Compared to the placebo group, the proportion of positive responses to GAQ (placebo: 41.2%; 100 mg udenafil: 78.8%; 200 mg udenafil: 85.2%) and that of subjects who returned to normal erection (placebo: 15.7%; 100 mg udenafil: 44.2%; 200 mg udenafil: 54.5%) were significantly greater for the udenafil groups. The efficacy was maintained irrespective of baseline ED severity, the number of antihypertensive agents, and prior experience with PDE5Is. Udenafil was well tolerated with a low incidence of treatment-emergent adverse events.
Efficacy in ED patients with LUTS
A large body of epidemiologic evidence supports a causal relationship between ED and LUTS.Citation61 Although the underlying mechanisms for the relationship between LUTS and ED in men with BPH are not fully understood, common links, such as the NO/cGMP pathway, RhoA/Rho-kinase signaling, pelvic atherosclerosis, and autonomic adrenergic hyperactivity, can be potential targets for PDE5Is.Citation62 Thus, a recent meta-analysis of available randomized, placebo-controlled trials investigating the efficacy and safety of PDE5Is alone or in combination with alpha-blocker in men with LUTS/BPH showed favorable outcomes in terms of both erectile function and LUTS.Citation62
An open, prospective, non-comparative study by Chung et al assessed the efficacy and safety of coadministered 100 mg udenafil and alpha-1-blockers in 120 patients with both LUTS/BPH and ED, who were already receiving stable alpha-1-blocker therapy.Citation30 At the end of the treatment period (8 weeks), mean international prostatic symptom score (IPSS) significantly decreased from 14.3 at baseline to 11.5, and mean IIEF-5 score significantly increased from 11.9 at baseline to 19.3, without any additional adverse effects related to coadministration.
Chronic dosing of udenafil for ED
Several preclinical and clinical studies have demonstrated that chronic or daily use of PDE5Is in the treatment of ED can significantly improve endothelial dysfunction, suggesting a promising therapeutic potential.Citation63–Citation65 Potential benefits of chronic PDE5I dosing are as follows: 1) a natural and spontaneous sex-life as it used to be when erectile function was not impaired; 2) salvage treatment of nonresponder to on-demand use of PDE5Is; 3) endothelial and penile rehabilitation, especially in complicated cases; and 4) combined treatment of LUTS/BPH.Citation2,Citation19,Citation66 Given the pharmacokinetic profiles of udenafil with tmax of 0.8–1.3 hours and t1/2 of 9.9–12.1 hours, udenafil may be a candidate for chronic dosing.
A Phase II, multicenter, randomized, double-blind, placebo-controlled, fix-dosed clinical trial evaluated the efficacy and safety of a once-daily low dose of udenafil (25 mg or 50 mg or 75 mg) in the treatment of ED and aimed to determine the optimal clinical dose and dosing schedule.Citation31 The primary efficacy variable was change from baseline in IIEF-EF scores. The secondary efficacy variables included patient responses to SEP2, SEP3, and GAQ, and the percentage of patients exhibiting a “shift to normal.” Compared with placebo, patients who took 50 mg or 75 mg of udenafil had significantly greater increase in their IIEF-EF score, but those who took 25 mg of udenafil did not (placebo: 3.61; 25 mg udenafil: 5.75; 50 mg udenafil: 6.55; 75 mg udenafil: 8.71). A similar finding was observed when comparing change from baseline in patient response of SEP2 (placebo: 11.95%; 25 mg udenafil: 22.10%; 50 mg udenafil: 27.9%, 75 mg udenafil: 39.11%); however, compared to placebo, all udenafil groups showed significantly greater increases in patient response of SEP3 (placebo: 23.46%; 25 mg udenafil: 42.09%; 50 mg udenafil: 51.41%, 75 mg udenafil: 73.5%) and in the percentage of patients achieving normal IIEF-EF scores (placebo: 13.6%; 25 mg udenafil: 30.5%; 50 mg udenafil: 40.0%; 75 mg udenafil: 44.1%). Also, with respect to the proportion of positive responses to GAQ, all udenafil groups showed a significant difference compared with the placebo group (placebo: 35.6%; 25 mg udenafil: 69.5%; 50 mg udenafil: 75.0%, 75 mg udenafil: 88.1%). In general, udenafil was well tolerated, and all treatment-related adverse effects were mild or moderate in severity.
Efficacy in other populations with ED
Dyslipidemia, one component of metabolic syndrome, is an independent risk factor for endothelial dysfunction, which is believed to be a major contributor to the development of ED.Citation67 Several clinical trials have demonstrated favorable outcomes of vardenafil and tadalafil in the treatment of ED patients with dyslipidemia.Citation68,Citation69 A preclinical study using a rat model of hypercholesterolemic ED showed that chronic udenafil treatment restored the erectile function, providing a rationale for the potential use of udenafil for treating ED secondary to hypercholesterolemia.Citation70 To date, however, no clinical data on the efficacy of udenafil for treatment of ED patients with dyslipidemia have been published.
The role of PDE5Is in penile rehabilitation following radical prostatectomy has been an active area of debate ever since several preclinical studies suggested the protective role of PDE5Is in the prevention of endothelial damage due to vascular ischemic and cavernous nerve (CN) injuries.Citation71 A few experimental studies using animal models of CN injury have shown that chronic administration of udenafil can preserve erectile function through amelioration of penile hypoxia and fibrosis induced by CN injury, indicating the beneficial role against the pathophysiological consequences of CN injury.Citation72,Citation73 There have, however, been no human data published on the protective role of udenafil in men with post-radical prostatectomy ED.
Safety and tolerability of udenafil in ED
Udenafil is well tolerated with few treatment-related adverse events. Most clinical investigations of udenafil for ED report that no adverse effects were shown in electrocardiogram or laboratory tests or on vital signs such as blood pressure (BP) and pulse rate in men with ED.Citation27–Citation29,Citation31,Citation32
Treatment-related adverse effects
All clinical trials evaluating the efficacy and safety of udenafil in men with ED reported that most adverse effects were mild-to-moderate in severity, without any serious adverse event during the study period.Citation27–Citation33 The most common udenafil-related adverse effects include flushing and headache.Citation19 Common adverse effects are summarized in . The adverse effects are generally related to the vasodilatory effect, a known pharmacology of PDE5Is, and the safety profile of udenafil is largely a function of inhibition of PDE5 expressed in non-penile tissue or cross-reactivity with the other PDEs. Although there has been a report of a case of anterior ischemic optic neuropathy associated with the use of udenafil,Citation74 the overall frequencies of visual adverse effects related to udenafil were very low (0.0%–0.6%).Citation27–Citation33 Udenafil appears not to be associated with adverse effects such as myalgia and back pain. Although a single case of nonaneurysmal subarachnoid hemorrhage has been reported in a patient after taking 50 mg udenafil,Citation75 it is not clear that there was a causal relationship between intake of udenafil and the hemorrhage.
Table 3 Summary of treatment-related adverse effects caused by udenafil
Safety and tolerability in ED patients with hypertension
Given the vasodilatory effect of PDE5Is, special attention has been paid to the safety and tolerability of udenafil in patients who took concomitant antihypertensive agents. In patients with ED who took concomitant antihypertensive drugs, significant decrease in diastolic BP was observed in both 100 mg (standing only: from 85.3 mmHg to 81.9 mmHg) and 200 mg (both standing and sitting: from 83.7 and 85.9 mm Hg to 81.1 and 83.0 mmHg, respectively) udenafil treatment groups, without a significant change in systolic BP.Citation32 Interestingly, a significant reduction of diastolic BP was noted in both sitting and standing positions after the treatment with placebo; thus, there were no statistically significant differences in the sitting or standing BP profiles between the groups. Furthermore, concomitant use of udenafil with antihypertensive medication did not lead to increases in the frequency of udenafil-related adverse events, such as vasodilatory symptoms (headache, flushing) or significant hypotensive symptoms (dizziness, faintness, vertigo).Citation32
Another class of drug requiring special caution, when taken in combination with udenafil, is alpha-blocker, which can be used for treatment of BPH or hypertension. It may induce significant hypotension when administered in combination with udenafil. A recent Phase I, randomized, double-blind, double-dummy, placebo-controlled trial showed that the coadministration of udenafil and tamsulosin was not associated with clinically significant hemodynamic changes such as systolic or diastolic BP in healthy volunteers.Citation76 There have however, been no clinical data on safety and tolerability of udenafil when administered in combination with nonselective alpha-blockers, such as doxazosin and terazosin.
Discussion
Since their introduction in the treatment of ED, PDE5Is have rapidly gained wide acceptance among clinicians and patients due to several factors, such as reliable efficacy and tolerability, an apparently favorable safety profile, and ease of use. PDE5Is improve erectile function by increasing cGMP in corpora cavernosa, leading to relaxation of cavernosal smooth muscle cells. Clinical differences among these PDE5Is are mainly related to their different pharmacokinetics, particularly time to onset and duration of action. Thus, the advent of a variety of PDE5Is and other potential agents now under clinical development with varying pharmacokinetic and other properties can provide additional options for patients and thus better suit their individual needs. In this regard, because udenafil has clinical properties of both relatively rapid onset and long duration of action, it may be a better treatment option for ED according to patient-specific sex-life profiles.
There is positive evidence that udenafil is an effective, safe, and well-tolerated treatment option in the management of ED.Citation27–Citation29,Citation31,Citation32 The recent meta-analysis by Ding et al showed that 100 mg and 200 mg udenafil could increase IIEF-EF scores by 6.69 and 8.62 points, respectively.Citation54 These are similar to the results of the pooled analyses of 100 mg sildenafil, 20–25 mg tadalafil, and 20 mg vardenafil (9.65, 8.52, and 7.50 points, respectively), although it may be difficult to directly compare the efficacy of different PDE5Is due to limited data on comparative analyses of their efficacy in the treatment of ED.Citation77 Also, udenafil showed increases in SEP2 and SEP3 by 28.09% and 40.23%, respectively, which was similar to the results of the pooled analysis for sildenafil (10.48% and 29.10%, respectively), tadalafil (29.70% and 48.07%, respectively) and vardenafil (29.22% and 48.13%, respectively).Citation21,Citation54 In terms of GAQ, udenafil showed approximately twice the positive response to GAQ compared to placebo as the other PDE5Is have shown (placebo: 24%; udenafil: 69%; sildenafil: 73%; tadalafil: 75%; vardenafil: 73%).Citation21 In addition, the effect of udenafil on improving erectile function was maintained for up to 12 hours after a single dosage of 100 mg udenafil, suggesting the potential of allowing spontaneity in the sex-lives of patients.Citation28
Although the response to PDE5I in ED men is lower in those with DM than in those without DM, PDE5I is a helpful treatment option for the management of ED in diabetic men. According to a recent Cochrane Review, treatment with sildenafil resulted in a 7.19-point improvement in IIEF-EF score compared to placebo.Citation78 A multicenter, randomized, double-blind, placebo-controlled, parallel-group trial by Sáenz de Tejada et al showed that 10 mg and 20 mg tadalafil improved the IIEF-EF score by 6.3 and 7.2 points compared with placebo, respectively.Citation79 Also, treatment with 10 mg and 20 mg tadalafil significantly increased the positive response to SEP2 (10 mg and 20 mg tadalafil: 22.2% and 22.6%, respectively) and SEP3 (10 mg and 20 mg tadalafil: 28.4% and 29.1%, respectively) compared to baseline. A Phase III, multicenter, randomized, double-blind, fixed-dose, parallel-group trial by Goldstein et al demonstrated that 10 mg and 20 mg vardenafil improved the IIEF-EF score by 4.5 and 6.4 points compared with placebo, respectively.Citation80 Furthermore, treatment with 10 mg and 20 mg vardenafil significantly increased the positive response to SEP2 (10 mg and 20 mg vardenafil: 30.0% and 23.0%, respectively) and SEP3 (10 mg and 20 mg vardenafil: 41.0% and 39.0%, respectively) compared to baseline. In accordance with these findings, 100 mg and 200 mg udenafil showed greater increase in the IIEF-EF score by 5.8 and 7.01 points compared with placebo, respectively.Citation29 As for the positive response to SEP2, treatment with 100 mg and 200 mg udenafil demonstrated increases of 23.84% and 31.07% compared to baseline, respectively. As for the positive response to SEP3, treatment with 100 mg and 200 mg udenafil showed increases of 45.97% and 55.56% compared to baseline, respectively. Taken together, despite the differences in the pharmacokinetics and pharmacodynamics among different PDE5Is, the clinical efficacy of udenafil is comparable to that of other PDE5Is.
Udenafil can be an effective and well-tolerated treatment option for ED men with underlying HTN who take antihypertensive drugs. According to the recent data by Paick et al,Citation32 100 mg and 200 mg udenafil showed a greater increase in the IIEF-EF score by 6.73 and 8.06 points compared with placebo, respectively, which was comparable to the results obtained with 25–100 mg sildenafil (6.2 points), 20 mg tadalafil (8.1 points), and 5–20 mg vardenafil (8.9 points).Citation81–Citation83 In terms of the positive response to SEP2 and SEP3, treatment with 100 mg and 200 mg udenafil showed increases of 25.85% and 57.88% and 29.82% and 71.11% compared to baseline, respectively, which were comparable to the results obtained with 20 mg tadalafil (34.3% and 45.1%) and 5–20 mg vardenafil (32.4% and 38.0%).Citation32,Citation81–Citation83 Thus, although previous studies for other PDE5Is used different primary efficacy variables, thereby making direct comparison among different PDE5Is difficult, the body of evidence suggests that the clinical efficacy of udenafil is similar to that of other PDE5Is. Also, the results of udenafil for the treatment of ED in hypertensive men on antihypertensive drugs appear to be similar to those results found for the all-comer population with ED.Citation27,Citation32 In terms of safety and tolerability, the treatment with udenafil in ED men on concomitant antihypertensive medication did not result in any significant changes in the BP profiles or increases in the frequency of treatment-related adverse events, such as clinically significant vasodilatory symptoms or hypotensive symptoms, compared with placebo, which was similar to the results of other PDE5Is.Citation32,Citation84,Citation85
Recent evidence indicates that ED men may prefer daily use of PDE5I to on-demand use, due to greater improvements in sexual self-confidence, time concerns, and spontaneity.Citation86 The on-demand use of PDE5I requires scheduled sexual activities, which may not be favored either by ED men or their sexual partners. Several studies have shown that chronic administration of PDE5Is in the treatment of ED can significantly improve endothelial dysfunction and structural alteration in penis.Citation63–Citation65 Thus, daily use of PDEIs may have the advantage of potentially curing ED by interfering with pathophysiological factors of both psychogenic (anxiety due to scheduled sexual activity) and organic (endothelial dysfunction and penile structural alteration) origin, although further studies are needed. In this context, prolonged duration of action provides an ideal pharmacokinetic profile for daily dosing of PDE5I, thereby allowing constant steady-state concentrations of the drug. Tadalafil, the only drug currently approved for daily dosing in the treatment of ED, has a t1/2 of 17.5 hours, which is longer than that of sildenafil (3–4 hours) or vardenafil (4–5 hours).Citation19 Although the t1/2 of udenafil (9.–12.1 hours) is shorter than that of tadalafil, udenafil appears to be have a pharmacokinetic property of relatively longer t1/2 compared to sildenafil or vardenafil.Citation19,Citation25 Thus, udenafil may be considered another potential option for chronic dosing of PDE5I in the treatment of ED. According to the recent study by Zhao et al,Citation31 daily dosing of 50 mg and 75 mg udenafil for 12 weeks showed significantly greater increase in the IIEF-EF score, by 3.45 and 5.20 points, compared with placebo, respectively, which was similar to the results of daily dosing of 2.5–10 mg tadalafil for 12–24 weeks (4.9–8.8 points).Citation64,Citation87 In terms of the positive response to SEP2 and SEP3, treatment with 50 mg and 75 mg udenafil showed increases of 27.9% and 51.41% and 39.11% and 73.5% compared to baseline, respectively, which was similar to the data obtained for 2.5–10 mg tadalafil (24.3%–39.4% for SEP2 and 31.2%–50.1% for SEP3).
Several randomized, placebo-controlled trials have investigated the efficacy and safety of PDE5I alone or in combination with alpha-blocker in the treatment of LUTS/BPH. According to a recent meta-analysis, the use of PDE5Is alone in patients with LUTS/BPH was associated with a significant improvement of the IIEF score (+5.487) and IPSS (−2.852), but not the maximum flow rate (Qmax) compared with placebo.Citation62 The combined use of PDE5I and alpha-1-blocker significantly improved the IIEF score (+3.6), IPSS score (−1.8), and Qmax (+1.5) compared to alpha-1-blocker alone, without an increase in significant adverse effects. Consistent with these findings, Chung et al demonstrated that combination of 100 mg udenafil with alpha-1-blockers in patients with both LUTS/BPH and ED significantly improved the IPSS (−2.8) and IIEF-5 score (+7.4), without any additional adverse effects related to coadministration.Citation30
There has been a scarcity of studies devoted specifically to the clinical properties (onset or duration of action) of udenafil. In the study by Park et al, however, participants were requested to attempt sexual intercourse at 12 hours after udenafil or placebo dosing to evaluate the duration of action of udenafil.Citation28 The study showed that udenafil significantly enhanced the rate of maintenance of erection and improved the IIEF-EF score compared with the placebo, indicating that the effectiveness of udenafil could be sustained for up to 12 hours after a single dosage of 100 mg. For sildenafil, several studies have suggested its sustained efficacy of 4–12 hours after dosing.Citation88–Citation91 Also, a prospective randomized controlled trial showed the extended duration of action of flexibly dosed vardenafil in men with ED when taken 8 hours before intercourse.Citation92 The t1/2 of udenafil (9.9–12.1 hours) is longer than that of sildenafil (3–4 hours) or vardenafil (4–5 hours), but shorter than that of tadalafil (17.5 hours). Thus, given the difference in t1/2 among the PDE5Is, it is possible that the effectiveness of udenafil to improve erectile function may persist even longer than 12 hours after dosing. Because there has been no study directly comparing the duration of action among the various PDE5Is, further studies are warranted.
A recent systemic review and meta-analysis for oral PDE5Is in the treatment of ED demonstrated that the adverse events caused by PDE5Is were generally mild and that there were no major differences in safety profiles among various PDE5Is.Citation21 The adverse effects of udenafil are usually similar to those of sildenafil. The frequency of myalgia and back pain caused by udenafil is substantially low. Although some publications have suggested that PDE11 inhibition could account for the back pain and myalgia reported by some men taking tadalafil,Citation46,Citation93 the physiological significance of PDE11 and the possible consequences of its inhibition have not yet been established. Results from most studies on udenafil support the conclusion that, when used as recommended, udenafil is safe in a broad range of patient populations, including those with hypertension.Citation27–Citation33
Patient preference studies on various PDE5Is may be helpful in better suiting individual needs and increasing patient satisfaction. Although most of the currently available patient preference studies have reported preference rates favorable to tadalafil, mainly because of longer duration of action that increases the patient’s freedom in their sexual life, there are some possible sources of bias.Citation94,Citation95 To date, there have been no data on patient preference between udenafil and the other PDE5Is. Thus, although it is very difficult to evaluate an individual preference in an objective way in daily clinical practice, the results of preference studies on various PDE5Is, including udenafil, can be useful in determining the best tailored therapy.Citation94
To date, there have been no data on long-term efficacy and tolerability of udenafil for the treatment of ED. Also, there have been sparse data on efficacy and safety of udenafil for the treatment of ED in other ethnic populations, since all studies, with the exception of a study by Ortaç et al,Citation33 have been performed in East Asian countries. Additionally, further research is needed to evaluate the efficacy of udenafil for ED management in difficult-to-treat populations, such as nonresponders to other PDE5Is or post-radical prostatectomy ED men. Further studies devoted specifically to clinical properties such as onset of action are needed. Although not published yet, a recent Phase III, multicenter, randomized, placebo-controlled study reported the favorable efficacy and safety of udenafil at three doses (50 mg, 100 mg, and 150 mg) in the United States.Citation96 Thus, research on ED treatment using udenafil is still ongoing.Citation97 Therefore, further clinical trials are needed to confirm long-term efficacy and safety of udenafil for the treatment of ED in various ethnic populations other than East Asian.
Conclusion
Udenafil has proven to have high efficacy and a favorable safety profile for a broad spectrum of ED patients, which are comparable to those of other PDE5Is. Due to the clinical properties of relatively rapid onset and long duration of action, udenafil may be a better option for ED treatment according to patient-specific sex-life patterns. Udenafil is as effective in the treatment of DM-associated ED as other PDE5Is. Recent data suggest that the concomitant use of anti-hypertensive drugs does not significantly affect the efficacy and safety profile. Also, due to its clinical properties, udenafil can be a daily-dosing option for the treatment of ED, as suggested by its favorable efficacy and safety profile. Further studies are still required to validate the efficacy and safety of udenafil and to complement the scientific basis for rationale, evidence-based prescription, and dosing decisions.
Disclosure
Jae-Seung Paick has served as a consultant of Mezzion Pharma Co, Ltd, since 2012. The authors report no other conflicts of interest in this work.
References
- [No authors listed]Consensus development conference statement. Impotence. December 7–9, 1992Int J Impot Res1993541812848173631
- ShamloulRGhanemHErectile dysfunctionLancet2013381986115316523040455
- KubinMWagnerGFugl-MeyerAREpidemiology of erectile dysfunctionInt J Impot Res2003151637112605242
- KupelianVShabsighRAraujoABO’DonnellABMcKinlayJBErectile dysfunction as a predictor of the metabolic syndrome in aging men: results from the Massachusetts Male Aging StudyJ Urol2006176122222616753405
- McVaryKTErectile dysfunction and lower urinary tract symptoms secondary to BPHEur Urol200547683884515925081
- RosenRAltweinJBoylePLower urinary tract symptoms and male sexual dysfunction: the multinational survey of the aging male (MSAM-7)Eur Urol200344663764914644114
- BillupsKLSexual dysfunction and cardiovascular disease: integrative concepts and strategiesAm J Cardiol20059612B57M61M
- McVaryKTCarrierSWessellsHSubcommittee on Smoking and Erectile Dysfunction Socioeconomic Committee, Sexual Medicine Society of North AmericaSmoking and erectile dysfunction: evidence based analysisJ Urol200116651624163211586190
- BrownJSWessellsHChancellorMBUrologic complications of diabetesDiabetes Care200528117718515616253
- McVaryKTClinical practice. Erectile dysfunctionN Engl J Med2007357242472248118077811
- KapurVChienCVFuessJESchwarzERThe relationship between erectile dysfunction and cardiovascular disease. Part II: The role of PDE-5 inhibition in sexual dysfunction and cardiovascular diseaseRev Cardiovasc Med20089318719518953278
- MinerMMErectile dysfunction and the “window of curability”: a harbinger of cardiovascular eventsMayo Clin Proc200984210210419181641
- ShabsighRShahMSandMErectile dysfunction and men’s health: developing a comorbidity risk calculatorJ Sex Med2008551237124318439154
- MontorsiPRavagnaniPMGalliSAssociation between erectile dysfunction and coronary artery disease. Role of coronary clinical presentation and extent of coronary vessels involvement: the COBRA trialEur Heart J200627222632263916854949
- HodgesLDKirbyMSolankiJO’DonnellJBrodieDAThe temporal relationship between erectile dysfunction and cardiovascular diseaseInt J Clin Pract200761122019202517997808
- WessellsHJoyceGFWiseMWiltTJErectile dysfunctionJ Urol200717751675168117437781
- MontagueDJarowJBroderickGErectile Dysfunction Guideline Update PanelChapter 1: The management of erectile dysfunction: an AUA updateJ Urol2005174123023915947645
- MontorsiFAdaikanGBecherESummary of the recommendations on sexual dysfunctions in menJ Sex Med20107113572358821040491
- BruzzichesRFrancomanoDGareriPLenziAAversaAAn update on pharmacological treatment of erectile dysfunction with phosphodiesterase type 5 inhibitorsExpert Opin Pharmacother201314101333134423675780
- BellASPalmerMJNovel phosphodiesterase type 5 modulators: a patent survey (2008–2010)Expert Opin Ther Pat201121101631164121905762
- YuanJZhangRYangZComparative effectiveness and safety of oral phosphodiesterase type 5 inhibitors for erectile dysfunction: a systematic review and network meta-analysisEur Urol201363590291223395275
- GlinaSToscanoIGomatzkyCEfficacy and tolerability of lodenafil carbonate for oral therapy in erectile dysfunction: a phase II clinical trialJ Sex Med20096255355719040623
- GlinaSFonsecaGNBerteroEBEfficacy and tolerability of lodenafil carbonate for oral therapy of erectile dysfunction: a phase III clinical trialJ Sex Med2010751928193620214718
- HatzimouratidisKHatzichristouDGLooking to the future for erectile dysfunction therapiesDrugs200868223125018197727
- PalitVEardleyIAn update on new oral PDE5 inhibitors for the treatment of erectile dysfunctionNat Rev Urol201071160360921068761
- DohHShinCYSonMMechanism of erectogenic effect of the selective phosphodiesterase type 5 inhibitor, DA-8159Arch Pharm Res200225687387812510841
- PaickJSKimSWYangDYThe efficacy and safety of udenafil, a new selective phosphodiesterase type 5 inhibitor, in patients with erectile dysfunctionJ Sex Med20085494695318221288
- ParkHJParkJKParkKMinKParkNCEfficacy of udenafil for the treatment of erectile dysfunction up to 12 hours after dosing: a randomized placebo-controlled trialJ Sex Med2010762209221620412426
- MoonDGYangDYLeeCHA therapeutic confirmatory study to assess the safety and efficacy of Zydena (udenafil) for the treatment of erectile dysfunction in male patients with diabetes mellitusJ Sex Med2011872048206121554549
- ChungBHLeeJYLeeSHYooSJLeeSWOhCYSafety and efficacy of the simultaneous administration of udenafil and an alpha-blocker in men with erectile dysfunction concomitant with BPH/LUTSInt J Impot Res200921212212819194451
- ZhaoCKimSWYangDYEfficacy and safety of once-daily dosing of udenafil in the treatment of erectile dysfunction: results of a multicenter, randomized, double-blind, placebo-controlled trialEur Urol201160238038721458153
- PaickJSKimSWParkYKThe efficacy and safety of udenafil [Zydena] for the treatment of erectile dysfunction in hypertensive men taking concomitant antihypertensive agentsJ Sex Med20096113166317619694927
- OrtaçMÇayanSÇalis¸kanMKEfficacy and tolerability of udenafil in Turkish men with erectile dysfunction of psychogenic and organic aetiology: a randomized, double-blind, placebo-controlled studyAndrology20131454955523785019
- CorbinJDFrancisSHPharmacology of phosphodiesterase-5 inhibitorsInt J Clin Pract200256645345912166544
- LueTFErectile dysfunctionN Engl J Med2000342241802181310853004
- KimNNPhosphodiesterase type 5 inhibitors: a biochemical and clinical correlation surveyInt J Impot Res200315Suppl 5S13S1914551572
- KouvelasDGoulasAPapazisisGSardeliCPourzitakiCPDE5 inhibitors: in vitro and in vivo pharmacological profileCurr Pharm Des200915303464347519860692
- KimBHLimHSChungJYSafety, tolerability and pharmacokinetics of udenafil, a novel PDE-5 inhibitor, in healthy young Korean subjectsBr J Clin Pharmacol200865684885418318773
- ShimHJKimYCParkKJPharmacokinetics of DA-8159, a new erectogenic, after intravenous and oral administration to rats: hepatic and intestinal first-pass effectsJ Pharm Sci200392112185219514603504
- WalkerDKAcklandMJJamesGCPharmacokinetics and metabolism of sildenafil in mouse, rat, rabbit, dog and manXenobiotica199929329731010219969
- ShimHJKimYCLeeJHInterspecies pharmacokinetic scaling of DA-8159, a new erectogenic, in mice, rats, rabbits and dogs, and prediction of human pharmacokineticsBiopharm Drug Dispos200526726927715991256
- KimTEKimBHKimJREffect of food on the pharmacokinetics of the oral phosphodiesterase 5 inhibitor udenafil for the treatment of erectile dysfunctionBr J Clin Pharmacol2009681434619660002
- WallisRMCorbinJDFrancisSHEllisPTissue distribution of phosphodiesterase families and the effect of sildenafil on tissue cyclic nucleotides, platelet function, and the contractile responses of trabeculae carneae and aortic rings in vitroAm J Cardiol1999835A3C12C
- FrancisSHTurkoIVCorbinJDCyclic nucleotide phosphodiesterases: relating structure and functionProg Nucleic Acid Res Mol Biol20016515211008484
- BischoffEPotency, selectivity, and consequences of nonselectivity of PDE inhibitionInt J Impot Res200416Suppl 1S11S1415224129
- GresserUGleiterCHErectile dysfunction: comparison of efficacy and side effects of the PDE-5 inhibitors sildenafil, vardenafil and tadalafil – review of the literatureEur J Med Res200271043544612435622
- KuHYAhnHJSeoKAThe contributions of cytochromes P450 3A4 and 3A5 to the metabolism of the phosphodiesterase type 5 inhibitors sildenafil, udenafil, and vardenafilDrug Metab Dispos200836698699018308836
- JiHYLeeHWKimHHRole of human cytochrome P450 3A4 in the metabolism of DA-8159, a new erectogenicXenobiotica20043411–1297398215801542
- KimJKimSJJiHYSimultaneous determination of a new phosphodiesterase-5 inhibitor DA-8159 and its active metabolite in human plasma by high performance liquid chromatography with tandem mass spectrometryChromatographia2003577–8447450
- AmakyeDWardJBrysonSHanKDA-8159-phase I studies to investigate the safety and pharmacokinetics in healthy male Caucasian subjectsClin Pharmacol Ther20047586
- HatzichristouDAmarEEardleyIGuidelines on male sexual dysfunction: erectile dysfunction and premature ejaculationEur Urol201057580481420189712
- OhTYKangKKAhnBOYooMKimWBErectogenic effect of the selective phosphodiesterase type 5 inhibitor, DA-8159Arch Pharm Res200023547147611059826
- SalemEAKendirciMHellstromWJUdenafil, a long-acting PDE5 inhibitor for erectile dysfunctionCurr Opin Investig Drugs200677661669
- DingHDuWWangHEfficacy and safety of udenafil for erectile dysfunction: a meta-analysis of randomized controlled trialsUrology201280113413922497982
- ThorveVSKshirsagarADVyawahareNSJoshiVSIngaleKGMohiteRJDiabetes-induced erectile dysfunction: epidemiology, pathophysiology and managementJ Diabetes Complications201125212913620462773
- KangKKChoiSMAhnGJKwonJWKimWBThe effect of DA-8159 on corpus cavernosal smooth muscle relaxation and penile erection in diabetic rabbitsUrol Res200432210711115024530
- AhnGJSohnYSKangKKThe effect of PDE5 inhibition on the erectile function in streptozotocin-induced diabetic ratsInt J Impot Res200517213414115578039
- AhnGJYuJYChoiSMChronic administration of phosphodi-esterase 5 inhibitor improves erectile and endothelial function in a rat model of diabetesInt J Androl200528526026616128985
- AhnGJChungHKLeeCHKangKKAhnBOIncreased expression of the nitric oxide synthase gene and protein in corpus cavernosum by repeated dosing of udenafil in a rat model of chemical diabetogenesisAsian J Androl200911443544219465935
- ChoSYParkKPaickJSKimSWChange of erectile function and responsiveness to phosphodiesterase type 5 inhibitors at different stages of streptozotocin-induced diabetes in ratsJ Sex Med2011851352136121054802
- Martínez-SalamancaJICarballidoJEardleyIPhosphodiesterase type 5 inhibitors in the management of non-neurogenic male lower urinary tract symptoms: critical analysis of current evidenceEur Urol201160352753521684677
- GacciMCoronaGSalviMA systematic review and meta-analysis on the use of phosphodiesterase 5 inhibitors alone or in combination with α-blockers for lower urinary tract symptoms due to benign prostatic hyperplasiaEur Urol2012615994100322405510
- Behr-RousselDGornyDMevelKChronic sildenafil improves erectile function and endothelium-dependent cavernosal relaxations in rats: lack of tachyphylaxisEur Urol2005471879115582254
- PorstHGiulianoFGlinaSEvaluation of the efficacy and safety of once-a-day dosing of tadalafil 5 mg and 10 mg in the treatment of erectile dysfunction: results of a multicenter, randomized, double-blind, placebo-controlled trialEur Urol200650235135916766116
- PorstHRajferJCasabéALong-term safety and efficacy of tadalafil 5 mg dosed once daily in men with erectile dysfunctionJ Sex Med2008592160216918557812
- BellaAJDeyoungLXAl-NumiMBrockGBDaily administration of phosphodiesterase type 5 inhibitors for urological and nonurological indicationsEur Urol2007524990100517646047
- MinerMBillupsKLErectile dysfunction and dyslipidemia: relevance and role of phosphodiesterase type-5 inhibitors and statinsJ Sex Med2008551066107818331271
- LewisRWSadovskyREardleyIThe efficacy of tadalafil in clinical populationsJ Sex Med20052451753116422847
- MinerMGildermanLBailenJVardenafil in men with stable statin therapy and dyslipidemiaJ Sex Med2008561455146718373526
- KangKKYuJYYooMKwonJWThe effect of DA-8159, a novel PDE5 inhibitor, on erectile function in the rat model of hypercholesterolemic erectile dysfunctionInt J Impot Res200517540941615920460
- HatzimouratidisKBurnettALHatzichristouDMcCulloughARMontorsiFMulhallJPPhosphodiesterase type 5 inhibitors in postprostatectomy erectile dysfunction: a critical analysis of the basic science rationale and clinical applicationEur Urol200955233434718986755
- LeeCHKimHSGooMJChronic administration of udenafil, a selective phosphodiesterase type 5 inhibitor, promotes erectile function recovery in an animal model of bilateral cavernous nerve crush injuryJ Sex Med2011851330134021366883
- LeeCHShinJHAhnGJKangKKAhnBOYooMUdenafil enhances the recovery of erectile function and ameliorates the pathophysiological consequences of cavernous nerve resectionJ Sex Med2010772564257120524975
- KimIKimDAnterior ischemic optic neuropathy associated with udenafilKorean J Ophthalmol201226323523822670084
- BaeEKAhnJHParkJJNonaneurysmal subarachnoid hemorrhage after udenafil intakeJ Stroke Cerebrovasc Dis Epub522013
- KimMGKimJRKimBHThe effect of udenafil on the hemodynamics of healthy male volunteers administered tamsulosinCurr Med Res Opin201329668569323557068
- BernerMMKristonLHarmsAEfficacy of PDE-5-inhibitors for erectile dysfunction. A comparative meta-analysis of fixed-dose regimen randomized controlled trials administering the International Index of Erectile Function in broad-spectrum populationsInt J Impot Res200618322923516239897
- VardiMNiniAPhosphodiesterase inhibitors for erectile dysfunction in patients with diabetes mellitusCochrane Database Syst Rev20071CD00218717253475
- Sáenz de TejadaIAnglinGKnightJREmmickJTEffects of tadalafil on erectile dysfunction in men with diabetesDiabetes Care200225122159216412453954
- GoldsteinIYoungJMFischerJBangerterKSegersonTTaylorTVardenafil, a new phosphodiesterase type 5 inhibitor, in the treatment of erectile dysfunction in men with diabetes: a multicenter double-blind placebo-controlled fixed-dose studyDiabetes Care200326377778312610037
- BlondeLSildenafil citrate for erectile dysfunction in men with diabetes and cardiovascular risk factors: a retrospective analysis of pooled data from placebo-controlled trialsCurr Med Res Opin200622112111212017076971
- KlonerRASadovskyRJohnsonEGMoDAhujaSEfficacy of tadalafil in the treatment of erectile dysfunction in hypertensive men on concomitant thiazide diuretic therapyInt J Impot Res200517545045416015377
- ShabsighRDuvalSShahMReganTSJuhaszMVeltryLGEfficacy of vardenafil for the treatment of erectile dysfunction in men with hypertension: a meta-analysis of clinical trial dataCurr Med Res Opin200723102453246017727740
- KlonerRABrownMPrisantLMCollinsMEffect of sildenafil in patients with erectile dysfunction taking antihypertensive therapy. Sildenafil Study GroupAm J Hypertens2001141707311206684
- van AhlenHWahleKKupperWYassinAReblinTNeureitherMSafety and efficacy of vardenafil, a selective phosphodiesterase 5 inhibitor, in patients with erectile dysfunction and arterial hypertension treated with multiple antihypertensivesJ Sex Med20052685686416422810
- Rubio-AuriolesEPorstHKimEDA randomized open-label trial with a crossover comparison of sexual self-confidence and other treatment outcomes following tadalafil once a day vs tadalafil or sildenafil on-demand in men with erectile dysfunctionJ Sex Med2012951418142922429760
- RajferJAliottaPJSteidleCPFitchWP3rdZhaoYYuATadalafil dosed once a day in men with erectile dysfunction: a randomized, double-blind, placebo-controlled study in the USInt J Impot Res20071919510316871272
- GiulianoFVicautEJeanpetitYImpact of the pharmacokinetic properties of PDE5 inhibitors on the dose/sexual intercourse intervalProg Urol20081853654218760744
- EardleyIEllisPBoolellMWulffMOnset and duration of action of sildenafil for the treatment of erectile dysfunctionBr J Clin Pharmacol200253Suppl 161S65S11879261
- ZinnerNDo food and dose timing affect the efficacy of sildenafil? A randomized placebo-controlled studyJ Sex Med2007413714417233779
- MoncadaIJaraJSubiráDCastañoIHernándezCEfficacy of sildenafil citrate at 12 hours after dosing: Re-exploring the therapeutic windowEur Urol20044635736015306108
- PorstHSharlipIDHatzichristouDExtended duration of efficacy of vardenafil when taken 8 hours before intercourse: a randomized, double-blind, placebo-controlled studyEur Urol2006501086109516820261
- MeulemanEJReview of tadalafil in the treatment of erectile dysfunctionExpert Opin Pharmacother200342049205614596658
- CoronaGMondainiNUngarARazzoliERossiAFuscoFPhosphodiesterase type 5 (PDE5) inhibitors in erectile dysfunction: the proper drug for the proper patientJ Sex Med201183418343221995676
- MironeVFuscoFRossiASicuteriRMontorsiFTadalafil and vardenafil vs sildenafil: a review of patient-preference studiesBJU Int20091031212121719154480
- Warner ChilcottTreatment of Erectile Dysfunction II Available from: http://clinicaltrials.gov/ct2/show/NCT01037218. NLM identifier:NCT01037218Accessed November 18, 2013
- Warner ChilcottTreatment of Erectile Dysfunction - Long Term Safety and Efficacy Available from: http://clinicaltrials.gov/ct2/show/NCT01065012. NLM identifier:NCT01065012Accessed November 18, 2013