
Abstract
Objective
Hip ankylosis is a prevalent condition in patients with Ankylosing spondylitis (AS) that can significantly impact their psychological well-being. This study aimed to investigate the impact of Total Hip Arthroplasty (THA) on anxiety and depression among AS patients.
Methods
62 AS patients undergoing primary THA were recruited and separated into two groups based on preoperative hip motion. The 40 patients with hip mobility of 0° were assigned to group A, and others were assigned to group NA. Self-rating Anxiety Scale (SAS), Self-rating Depression scale (SDS), Harris hip scores (HHS) and 36-Item Short Form Survey (SF-36) were obtained one week before and there, six and twelve months after THA.
Results
The study found that AS patients in group A had significantly higher levels of anxiety and depression (SAS score = 75.05±2.79, SDS index score = 0.74±0.02) compared to group B (SAS score = 54.58±3.35, SDS index score= 0.64±0.03, P=0.01). However, both groups showed significant improvements in anxiety and depression scores from there to twelve months after THA (P<0.001). Correlation analyses revealed that the improvement in group NA was associated with hip pain relief (p<0.001), while the improvement in group A was related to joint function, disease duration, age at THA and spine imaging lesions (p<0.001).
Conclusion
Some degree of anxiety and depression was present in both groups of AS patients. Levels of depression and anxiety were higher in patients with combined hip ankylosis. And their improvement was associated with improved hip function and quality of life after THA. Hip pain relief played a significant role in patients without hip joint ankylosis. The impact of the degree of lesion on spinal imaging on psychological status needs to be considered in both groups.
Introduction
Ankylosing spondylitis (AS) is a chronic inflammatory disease characterized by inflammation and fusion of the axial sacroiliac, spinal, and hip joints.Citation1 About 80% of patients first develop symptoms before the age of 30 years,Citation2 and most often in young males. Currently, the mean global prevalence of AS is around 0.1–0.3% in Europe and the US and 0.3% in China,Citation3,Citation4 with hip joint involvement seen in 30–50% of cases, and bilateral hip involvement in up to 80–90%.Citation5 Total hip arthroplasty is now acknowledged as the most effective therapy for AS patients in terms of pain reduction and hip function restoration.Citation6
With the occurrence of hip joint ankylosis, patients’ psychological state and daily life would be greatly affected due to progressive hip motion limitation and pain. Günaydin et alCitation7 reported that more than one-third of AS patients had depressive symptoms and high depression scores, and Martindale et alCitation8 found that AS patients with depression and anxiety were 15% and 25%, respectively. Meanwhile, abnormal psychological status can also worsen the patient’s condition,Citation9 and AS patients with depression or anxiety had more severe pain and limited joint function.Citation10 However, the majority of surgeons were concerned with the outcomes of their patients’ operations, and few studies have quantitatively examined the impact of hip replacement for AS patients’ mental health. In particular, the effect of surgeries on anxiety, depression, and overall quality of life (QoL) need to be assessed.
The goal of this study was to compare pre-and post-operative mental status, hip function scores and QoL in AS patients with varying degrees of joint motion. Questionnaires were used to measure changes in AS patients’ mental health and QoL after surgery. This provided a theoretical basis for evaluating the short-term effects of surgery and providing more effective interventions.
Patients and Methods
Study Participants
This was a prospective cohort study including participants from two major hospitals (The Second Hospital Affiliated to Medical College, Xi’an Jiaotong University; and Hong-Hui Hospital, Medical College, Xi’an Jiaotong University). AS patients who received primary THA from April 2020 to June 2021 were recruited. Persistent joint pain or limited joint movement was the main indication for THA. The inclusion criteria were as follows: 1) Patients aged ≥ 18 years with AS diagnosed according to the Modified New York criteria,Citation11 with hip involvement confirmed radiographically; 2) Underwent primary THA; and 3) persistent hip pain for at least 3–6 months, VAS score at rest ≥ 3, and the bath ankylosing spondylitis radiology index (BASRI-hip) grade ≥2 (mild hip injury on x-ray with hip gap >2mm)Citation12,Citation13 (shown in ).
Table 1 BASRI-Hip Standard Grading
The following were exclusion criteria: previous hip, spinal, or other surgery, and rely on anti-anxiety or depression medications. Eligible patients were invited to participate, all of whom underwent cementless joint prosthesis replacement. The research was authorized by two local medical ethics committees (No. XJSH2020013; No. HH2020021), and all participants completed an informed consent form before the procedure. It was followed the 2013 Revised Declaration of Helsinki, stating that each participant signed an informed consent form.
Study Design
After admission, baseline clinical and psychometric assessments were completed immediately before arthroplasty. Total passive mobility of the hip joint was measured, including flexion, extension, abduction, adduction, internal rotation and external rotation. The total passive range of motion was 0°, which is defined as joint fusion. Based on hip mobility, patients were classified into joint ankylosis (passive joint mobility of 0°) and without hip joint ankylosis groups. In patients with bilateral joint involvement, mobility is measured as the mean of the joint mobility values on both sides. In both group, mental health score, Harris hip scores and quality of life scores were reevaluated 1 week before, and 3, 6 and 12 months after THA. Height, weight, age of onset, disease course, duration of cure, and morning stiffness time were obtained using a self-report questionnaire.
Tools for Assessing Anxiety, Depression and Quality of Life
Psychological status was measured using two questionnaires provided as a pamphlet. Zung’s Self-rating Anxiety Scale (SAS) and Self-rating Depression Scale (SDS; Zung, 1965)Citation14 both use 20 items, to assess anxiety and depression, respectively. Each item is rated on a four-point scale from 1 to 4, respectively. The SAS has a maximum possible score of 100 (adjusted standard score = original score*1.25), and the SDS (scored separately) has a maximum possible score of 1 (adjusted standard score = original score/80); higher scores (cutoff = 50; 0.5 points) indicate more severe anxiety or depression.
SF-36 was used to assess the AS patients’ quality of life.Citation15,Citation16 It includes eight dimensions of physical functioning, role physical, mental health, role emotional, social functioning, energy/vitality, pain, and general health perception. For different dimension, item scores are coded, summed, and converted to a scale of 0–100, and the higher the score means the better the quality of life.
Hip Function and Spinal Lesion Assessment Scale
The hip function associated with THA outcomes was measured by the Harris hip score (HHS),Citation17 which uses a 100-point rating scale and includes pain, function, activity, deformity, and mobility domains; the higher the score, the better the joint function.Citation18 The HHS has been widely used as a valid and reliable instrument to evaluate the outcome of hip replacement surgery.Citation19,Citation20 Regarding the measurement of joint mobility, the patient’s passive hip mobility, such as the angles of forward flexion, back extension, internal rotation, external rotation, internal retraction and abduction, was measured by using a goniometer, and the total sum was the patient’s total passive hip mobility. The Bath Ankylosing Spondylitis Radiology Index spine (BASRI-s) was applied to grade radiographic severity in the anterior-posterior and lateral spine.Citation21 A visual analogue scale (VAS) was used to assess hip and sacroiliac joint pain intensity (0 = no pain, 10 = severest pain possible). Furthermore, the Bath Ankylosing Spondylitis Functional Index (BASFI) is a scale used to assess the overall level of functional impairment in AS patients.Citation22 The BASFI comprises ten questions that cover physical activities and functional activities commonly encountered in daily life, such as getting up, walking, lifting weights, dressing, and self-care. Each question is rated on a scale of 0–10, with a total score ranging from 0–100. The scoring criterion is obtained by dividing the total score by 10, resulting in a final score ranging from 0–10, with higher values indicating a worse functional status. The BASFI has demonstrated high reliability and validity in assessing functional impairment in AS patients.
The main assessment regarding disease activity in AS patients uses the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI), a simple and validated self-assessment scale.Citation23 The BASDAI consists of six questions that address spinal pain, fatigue, joint swelling, joint pain, and local pressure pain. Patients are asked to rate the severity of their symptoms on each question based on the most recent week, on a scale ranging from 0 to 10 (in conjunction with a visual analog assessment method), where 0 indicates no disease activity and 10 indicates extremely active disease.
Statistical Analysis
The study focused on the changes in anxiety and depression scores of patients after total hip arthroplasty at different time points, and the sample estimators were designed using repeated measures ANOVA, the arithmetic process of which was done with the help of the software G-power.Citation24 The software correlation was set with the following parameters: effect size f=0.25, α=0.05, test efficacy Power value=0.8, number of groups=1 (usually 1 when there are multiple repeated measurement points), number of measurements=4, intra-major correlation=0, spherical hypothesis=0.35.
The normality of the data was checked by using the Kolmogorov–Smirnov test. Nonparametric tests analyzed non-normally distributed data, and parametric tests analyzed normally distributed data. A paired t-test was applied to compare the difference between pre-operative and final follow-up results. The two groups were compared using the independent samples t-test. Changes in each outcome measure were analyzed using repeated-measures ANOVA (two-tailed tests).Citation25 P-values were calculated using the Huynh–Feldt correction for non-sphericity.Citation26 The impact of pain, hip function, and QoL on psychological factors was examined using Pearson correlation analysis. P values <0.05 were considered statistically significant. All statistical analyses were computed by SPSS 23.0 software (SPSS Inc, Chicago, IL, USA).
Results
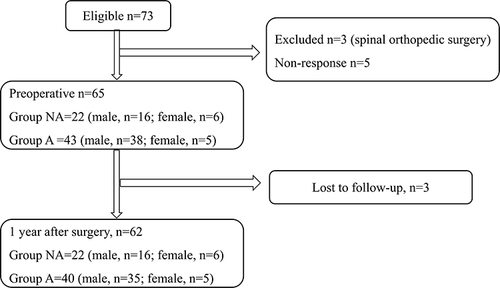
In total, 62 patients (left hip, n = 11; right hip, n = 10; both hips, n = 41) were included in the final analysis. The research procedures and population are depicted in . The 40 patients were assigned to group A, and the remaining 22 were assigned to group NA. The research procedures and population are presented in . Of the total patients, 40 were assigned to group A, and the remaining 22 were assigned to group NA. Based on the preoperative baseline questionnaire, significant differences were observed in bilateral surgery, age at THA, disease duration, preoperative range of motion (ROM) and hip flexion, morning stiffness time, BASFI and BASRI-s between the two groups (P<0.05) (shown in ). All patients’ surgical wounds healed at stage I, and no cases of superficial or periprosthetic infection were reported. During surgery, two patients sustained sciatic nerve injuries resulting in decreased muscle strength, which returned to normal after three months. No other post-operative complications were recorded at the end of the final follow-up.
Table 2 Pre-Operative Baseline Patient Demographics, Clinical, and Laboratory Parameters of as Patients
Figure 1 Flow chart for patient recruitment and follow-up.
Harris Hip, Mental Status and QOL Scores During the Study Period
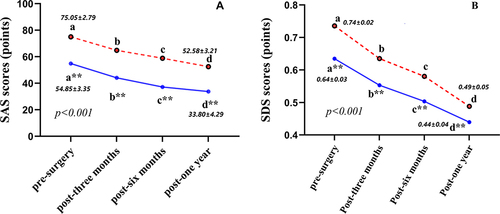
Group A had lower preoperative HHS and hip motion compared to group NA (p<0.001). One year after THA, both groups showed significant improvements in joint function and mobility (p<0.001). Although there was no significant difference in joint mobility between the two groups at the last follow-up (p=0.604), group A had lower HHS scores than group NA (p<0.001) (shown in ). Preoperatively, group A (SAS=75.05±2.79, SDS=0.74±0.02) had higher anxiety and depression levels than group NA (SAS=54.58±3.35, SDS=0.64±0.03, P=0.01). At the final follow-up, anxiety and depression levels significantly improved in both groups, with group NA (SAS=33.80±4.29, SDS=0.44±0.04; p<0.001) almost reaching normal levels (shown in ). However, anxiety and depression levels in group A (SAS=52.58±3.21, SDS=0.49±0.05, p<0.001) remained significantly higher than in group NA. But the Group NA exhibited higher preoperative VAS scores for hip pain than Group A (p<0.001), yet both groups achieved significant pain reduction postoperatively.
Table 3 Comparisons of VAS Score, Harris Score, and Total Hip ROM Between at Pre- and Post-Operation
Figure 2 Impact of Hip arthroplasty on Hip function and psychological status.
The preoperative SF-36 scores of the two groups were significantly different. All patients in group A had significantly lower mental health, general health, and physical function scores than those in group NA (p<0.05). One year after surgery, although the psychological and general health scores were significantly better in both groups (p<0.05), there were still significant differences between the groups (p<0.001). The other items of SF-36 showed no significant differences within or between groups in the research (p>0.05) (results not shown in the ). Patients with preoperative comorbidities had lower SF-36 scores and higher SAS/SDS scores over the course of the study, compared to the mean within the group.
Table 4 Preoperative and Postoperative the Quality of Life (SF-36) Scores
Correlation of SAS/SDS with SF-36 and Hip Joint Function Scores
Based on the results of the last follow-up, Pearson correlation analysis showed that the last postoperative anxiety and depression levels in patients without hip ankylosis were associated with hip pain, being undergoing bilateral arthroplasty, and the degree of spinal imaging lesions (P<0.05); however, in patients with hip ankylosis, last follow-up anxiety and depression levels were associated with the patient’s disease duration, age at the time of surgery, improvement in hip function, the passive hip mobility, unilateral or bilateral surgery, the degree of spinal imaging lesions, and improvement in quality of life were also associated (P<0.05) (Shown in ).
Table 5 Correlations Among Mental Status, Quality of Life, Joint Scores and Passive Mobility of the Hip at the Last Follow-Up
Discussion
Preoperative Depression and Anxiety
Our research has shown that AS patients with hip stiffness experience more severe psychological disorders, which can be divided into two aspects. Firstly, most AS patients are vulnerable to excessive stress, psychological burden, and hypersensitivity due to a lack of understanding of the disease’s characteristics, including its prolonged duration, and to conservative treatment outcomes not meeting their expectations.Citation27 Secondly, AS patients with severe hip lesion are typically affected by inflammatory pain and partial hip involvement during the early stages of hip involvement. As the condition progresses, the fusion of the hip joints and lesions in the spine can cause further physical deformity and body image disturbance (BID).Citation28 Our study found that significantly more patients in the ankylosis group received bilateral joint replacements than in the without hip joint ankylosis group.
Mental Health with Pain and Hip Function
Additionally, our study revealed an interesting finding: hip pain symptoms were relieved when hip involvement developed joint ankylosis, and those without ankylosis reported more severe hip pain than those with ankylosis. This difference in pain severity may be attributed to impaired hip motion and decreased intra-articular capsule pressure in the middle and late stages of joint ankylosis. Chronic body pain (lower back pain and hip pain) and disability caused by musculoskeletal system disorders might be associated with anxiety and depression.Citation29–31 The benefits of pain relief were particularly apparent in group A patients, and the reconstruction of joint function played an important role in group NA. However, psychological status differed between the groups in different disease stages. In group NA, psychological status improved significantly and continuously; group A patients needed more time to recover and still had higher anxiety scores at 1 year after surgery. The reason was that they experienced prolonged pain and physical hip dysfunction. In addition, compared to the NA group, patients in the ankylosis group tended to have bilateral hip ankylosis and severe contracture of the surrounding local muscle tissue. The above factors may explain why people with ankylosing joints have difficulty returning to a healthy psychological state after surgery. Therefore, treatment should not only be aimed at pain reduction and a return to function, but also relief of psychological sequelae.Citation32
In addition to lesions in the hip joint, patients with AS commonly experience damage in multiple organ systems, which results in a comorbid state.Citation33 While total hip arthroplasty can effectively address the issue of limited hip motion, it does not tackle other systemic diseases that can substantially affect patients’ long-term outlook. Bekhuis et alCitation34,Citation35 suggested that psychological disorders are strongly correlated with somatic symptoms. Therefore, providing early multidisciplinary treatment to such patients may enhance their long-term prognosis and alleviate their pain.
Postoperative QoL and Psychological State
Our study found that THA surgery can lead to improvements in psychological well-being and overall quality of life in patients with AS. These positive effects may be attributed to an increase in satisfaction and a shift in the perception of the disease, as seen in cases of developmental dysplasia of the hip.Citation36 The significant improvements in range of motion and hip function post-surgery are believed to bolster patients’ confidence and satisfaction, ultimately contributing to a better psychological state and improved quality of life. According to current research on crowd anxiety, there are two forms of human anxiety, namely trait anxiety and state anxiety.Citation14 Trait anxiety reflects interindividual changes in response to a negative or threatening event. State anxiety relates to current anxiety and may improve with other changes. Although these two kinds of anxiety were not rated separately in this study, the improvement of postoperative anxiety in both groups may have been related to the improvement in state anxiety, because state anxiety decreased with the relief of pain and improvement of hip function (while the change in trait anxiety was relatively insignificant). Further research is needed to confirm this, which would also provide a theoretical basis for perioperative psychological support. The long-term psychological and physical rehabilitation of postoperative patients still requires more effort from clinicians, especially for the patients with joint ankylosis.
We note some limitations of this study. First, AS is a systemic disease, and patients often have other systemic diseases during disease onset and development. Moreover, the control of postoperative disease activity, time invested in rehabilitation, and treatment of other systemic diseases differed among patients, which greatly affected the outcomes. Second, we could not draw any conclusions about gender differences in depression and anxiety disorders due to the low incidence of female patients. Potential gender differences should be addressed in a future study. Finally, the research results were limited by the relatively short follow-up period. Although this study found a positive effect of THA on the psychological health of AS patients, large sample sizes and long follow-up are needed to validate the results.
In conclusion, anxiety and depression were observed in both groups before surgery, but they were worse in the group with joint stiffness. After THA, the patients’ psychological function improved significantly due to the enhanced mobility and joint function of the hip. Pain relief is even more important in patients with a non-ankylosis hip. For patients with joint ankylosis, preoperative and postoperative psychological support should be offered.
Ethics Approval and Consent to Participate
The study process was reviewed and approved by the Ethical Approval Committee of the Second Affiliated Hospital of Xi’an Jiaotong University and Honghui Hospital. It was followed the 2013 Revised Declaration of Helsinki, stating that each participant signed an informed consent form (guardian signature required if under 18 years of age). Participants were not involved in vulnerable groups (eg vegetative), at risk of being coerced (eg prisoners) or signing the consent form without being reunited and informed. Both offline paper questionnaires and online electronic questionnaires were used for the study surveys, and data were compiled and tallied by a separate person. The research was authorized by two local medical ethics committees (No. XJSH2020013; No. HH2020021), and all participants completed an informed consent form before the procedure. All methods used in the research survey were carried out in accordance with relevant guidelines and regulations, with respect to the full protection of individual privacy as the overriding principle.
Disclosure
The authors declare that they have no competing interests for this work.
Acknowledgments
The authors would like to thank all the patients who participated, as well as the medical institutions and colleagues who have provided help with this study.
Data Sharing Statement
The datasets used and analysed during the current study available from the corresponding author on reasonable request.
Additional information
Funding
References
- Kubiak EN, Moskovich R, Errico TJ, Cesare PED. Orthopaedic management of ankylosing spondylitis. J Am Acad Orthop Surg. 2005;13(4):12. doi:10.5435/00124635-200507000-00006
- Feldtkeller E, Khan M, van der Heijde D, van der Linden S, Braun J. Age at disease onset and diagnosis delay in HLA-B27 negative vs. positive patients with ankylosing spondylitis. Rheumatol Int. 2003;23(2):61–66. doi:10.1007/s00296-002-0237-4
- Dean LE, Jones GT, MacDonald AG, Downham C, Sturrock RD, Macfarlane GJ. Global prevalence of ankylosing spondylitis. Rheumatology. 2014;53(4):650–657. doi:10.1093/rheumatology/ket387
- Ho -H-H, Chen J-Y. Ankylosing spondylitis: Chinese perspective, clinical phenotypes, and associated extra-articular systemic features. Curr Rheumatol Rep. 2013;15(8):344. doi:10.1007/s11926-013-0344-0
- Joshi AB, Markovic L, Hardinge K, Murphy JCM. Total hip arthroplasty in ankylosing spondylitis: an analysis of 181 hips. J Arthroplasty. 2002;17(4):427–433. doi:10.1054/arth.2002.32170
- Bukowski BR, Clark NJ, Taunton MJ, Freedman BA, Berry DJ, Abdel MP. Primary total hip arthroplasty in patients with ankylosing spondylitis. J Arthroplasty. 2021;36(7):S282–S289. doi:10.1016/j.arth.2021.01.054
- Günaydin R, Göksel Karatepe A, Çeşmeli N, Kaya T. Fatigue in patients with ankylosing spondylitis: relationships with disease-specific variables, depression, and sleep disturbance. Clin Rheumatol. 2009;28(9):1045–1051. doi:10.1007/s10067-009-1204-1
- Martindale J, Smith J, Sutton CJ, Grennan D, Goodacre L, Goodacre JA. Disease and psychological status in ankylosing spondylitis. Rheumatology. 2006;45(10):1288–1293. doi:10.1093/rheumatology/kel115
- Brionez TF, Assassi S, Reveille JD, et al. Psychological correlates of self-reported functional limitation in patients with ankylosing spondylitis. Arthritis Res Ther. 2009;11(6):R182. doi:10.1186/ar2874
- Baysal Ö, Durmuş B, Ersoy Y, et al. Relationship between psychological status and disease activity and quality of life in ankylosing spondylitis. Rheumatol Int. 2011;31(6):795–800. doi:10.1007/s00296-010-1381-x
- Raychaudhuri SP, Deodhar A. The classification and diagnostic criteria of ankylosing spondylitis. J Autoimmun. 2014;48–49:128–133. doi:10.1016/j.jaut.2014.01.015
- MacKay K, Brophy S, Mack C, Doran M, Calin A. The development and validation of a radiographic grading system for the hip in ankylosing spondylitis: the bath ankylosing spondylitis radiology hip index. J Rheumatol. 2000;27(12):2866–2872.
- Braun J, van der Heijde D. Imaging and scoring in ankylosing spondylitis. Best Pract Res Clin Rheumatol. 2002;16(4):573–604. doi:10.1053/berh.2002.0250
- Knight RG, Waal-Manning HJ, Spears GF. Some norms and reliability data for the state-trait anxiety inventory and the zung self-rating depression scale. Br J Clin Psychol. 1983;22(4):245–249. doi:10.1111/j.2044-8260.1983.tb00610.x
- Ware JE, Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care. 1992;30(6):473–483. doi:10.1097/00005650-199206000-00002
- Doward LC, Spoorenberg A, Cook SA, et al. Development of the ASQoL: a quality of life instrument specific to ankylosing spondylitis. Ann Rheum Dis. 2003;62(1):20–26. doi:10.1136/ard.62.1.20
- Harris WH. Traumatic arthritis of the hip after dislocation and acetabular fractures: treatment by mold arthroplasty. An end-result study using a new method of result evaluation. J Bone Joint Surg Am. 1969;51(4):737–755. doi:10.2106/00004623-196951040-00012
- Nilsdotter A, Bremander A. Measures of hip function and symptoms: Harris Hip Score (HHS), Hip Disability and Osteoarthritis Outcome Score (HOOS), Oxford Hip Score (OHS), Lequesne Index of Severity for Osteoarthritis of the Hip (LISOH), and American Academy of Orthopedic Surgeons (AAOS). Arthritis Care Res. 2011;63(S11):S200–S207. doi:10.1002/acr.20549
- Singh JA, Schleck C, Harmsen S, Lewallen D. Clinically important improvement thresholds for Harris Hip Score and its ability to predict revision risk after primary total hip arthroplasty. BMC Musculoskelet Disord. 2016;17(1):256. doi:10.1186/s12891-016-1106-8
- Söderman P, Malchau H. Is the Harris Hip score system useful to study the outcome of total hip replacement? Clin Orthop Relat Res. 2001;384(384):189–197. doi:10.1097/00003086-200103000-00022
- MacKay K, Mack C, Brophy S, Calin A. The bath ankylosing spondylitis radiology index (BASRI): a new, validated approach to disease assessment. Arthritis Rheum. 1998;41(12):2263–2270. doi:10.1002/1529-0131(199812)41:12<2263::AID-ART23>3.0.CO;2-I
- Calin A, Garrett S, Whitelock H, et al. A new approach to defining functional ability in ankylosing spondylitis: the development of the bath ankylosing spondylitis functional index. J Rheumatol. 1994;21(12):2281–2285.
- A new approach to defining disease status in ankylosing spondylitis: the bath ankylosing spondylitis disease activity index – PubMed. Available from: https://pubmed.ncbi.nlm.nih.gov/7699630/. Accessed June 07, 2023.
- Faul F, Erdfelder E, Lang A-G, Buchner A. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007;39(2):175–191. doi:10.3758/bf03193146
- Diggle P, Liang K, Zeger S. The Analysis of Longitudinal Data. USA: Oxford Science Publications; 1994.
- Huynh H, Feldt LS. Estimation of the box correction for degrees of freedom from sample data in randomized block and split-plot designs. J Educ Stat. 1976;1(1):69. doi:10.2307/1164736
- Webers C, Vanhoof L, Leue C, Boonen A, Köhler S. Depression in ankylosing spondylitis and the role of disease-related and contextual factors: a structural equation modeling approach. J Psychosom Res. 2019;121:130. doi:10.1016/j.jpsychores.2019.03.092
- Shen B, Zhang A, Liu J, et al. Body image disturbance and quality of life in Chinese patients with ankylosing spondylitis. Psychol Psychother. 2014;87(3):324–337. doi:10.1111/papt.12016
- Rode S, Salkovskis P, Dowd H, Hanna M. Health anxiety levels in chronic pain clinic attenders. J Psychosom Res. 2006;60(2):155–161. doi:10.1016/j.jpsychores.2005.07.005
- Ho PT, Li CF, Ng YK, Tsui SL, Ng KFJ. Prevalence of and factors associated with psychiatric morbidity in chronic pain patients. J Psychosom Res. 2011;70(6):541–547. doi:10.1016/j.jpsychores.2010.10.006
- Blackburn J, Qureshi A, Amirfeyz R, Bannister G. Does preoperative anxiety and depression predict satisfaction after total knee replacement? Knee. 2012;19(5):522–524. doi:10.1016/j.knee.2011.07.008
- Badura-Brzoza K, Zajac P, Brzoza Z, et al. Psychological and psychiatric factors related to health-related quality of life after total hip replacement - preliminary report. Eur Psychiatry. 2009;24(2):119–124. doi:10.1016/j.eurpsy.2008.06.009
- Zhao SS, Robertson S, Reich T, Harrison NL, Moots RJ, Goodson NJ. Prevalence and impact of comorbidities in axial spondyloarthritis: systematic review and meta-analysis. Rheumatology. 2020;59(Suppl4):iv47–iv57. doi:10.1093/rheumatology/keaa246
- Bekhuis E, Boschloo L, Rosmalen JGM, Schoevers RA. Differential associations of specific depressive and anxiety disorders with somatic symptoms. J Psychosom Res. 2015;78(2):116–122. doi:10.1016/j.jpsychores.2014.11.007
- Garcia-Cebrian A, Gandhi P, Demyttenaere K, Peveler R. The association of depression and painful physical symptoms–a review of the European literature. Eur Psychiatry. 2006;21(6):379–388. doi:10.1016/j.eurpsy.2005.12.003
- Liu R, Li Y, Fan L, Mu M, Wang K, Song W. Depression and anxiety before and after limb length discrepancy correction in patients with unilateral developmental dysplasia of the Hip. J Psychosom Res. 2015;79(6):574–579. doi:10.1016/j.jpsychores.2015.08.002