
Abstract
Background
The purpose of this study was to evaluate changes in subfoveal choroidal thickness after photodynamic therapy in patients with acute idiopathic central serous chorioretinopathy (ICSCR).
Methods
This was a retrospective observational study conducted in 63 participants. The primary outcome measure was subfoveal choroidal thickness at baseline and 3 days, one week, 4 weeks, and 12 weeks after photodynamic therapy. The secondary outcome measure was indocyanine green angiography at baseline and 4 weeks and 12 weeks after photodynamic therapy.
Results
Four weeks after photodynamic therapy, 20 (64.51%) symptomatic eyes showed hypofluorescence corresponding to the area of photodynamic therapy irradiation at the posterior pole. The mean subfoveal choroidal thickness increased significantly from 422±132 μm at baseline to 478±163 μm at day 3 after treatment (P=0.022) and then decreased to 362±113 μm at week 4 (P<0.001) and 339±135 μm at week 12 (P<0.001).
Conclusion
The subfoveal choroid in patients with acute ICSCR is thicker than in the normal population, and in symptomatic eyes is significantly thicker than in fellow eyes. Photodynamic therapy using a one third dose of verteporfin may decrease choroidal vascular hyperpermeability and choroidal thickness in patients with acute ICSCR.
Introduction
Idiopathic central serous chorioretinopathy (ICSCR), first described by von Graefe in 1866, is characterized by idiopathic exudative detachment of the neurosensory retina in the posterior pole and one or more leaks from the retinal pigment epithelium. The precise pathophysiology of ICSCR is still unclear. Impairment in resorptive capacity and barrier function in retinal pigment epithelium was once considered to be an important contributing factor. However, Negi et alCitation1,Citation2 reported that simple dysfunction of retinal pigment epithelium could not lead to retinal detachment. GassCitation3 postulated that hyperpermeability of the choriocapillaris resulted in exudation of fluid into the subretinal space. Studies using indocyanine green angiography (ICGA) revealed that abnormalities of the choroidal vasculature, including hyperpermeabilityCitation4–Citation10 and venous congestion,Citation10–Citation12 may be the essential elements of ICSCR.Citation10,Citation11 Other studiesCitation13 using high-resolution ultrasonography have also shown hyperdynamic circulation within the choroid of eyes with ICSCR.Citation14,Citation15
Focal laser photocoagulation is a classic treatment for acute ICSCR, and can shorten the duration by about 2 months.Citation16 However, whether it would reduce recurrence rates is controversial. A prospective, randomized clinical trialCitation17 found that the final recurrence rate in a laser photocoagulation group was unchanged. Recurrent attacks always lead to widespread decompensation of retinal pigment epithelium and permanent vision loss. Photodynamic therapy can decrease hyperpermeability in the choroid and reduce leakage from retinal pigment epithelium, hence reducing the recurrence rate.Citation18–Citation22 Several studiesCitation23–Citation25 have reported that photodynamic therapy has a dose-dependent effect, and that reducing the dose of verteporfin could diminish the adverse effects in the retina and choroid. Zhao et alCitation26 demonstrated that a 30% dose of verteporfin is safe and effective for acute ICSCR in Chinese patients.
The rapid development of imaging techniques has improved our understanding of the pathogenesis of ICSCR. Optical coherence tomography, which was invented in the late 1990s, has become an indispensible technique in evaluating and managing many ocular disorders. However, due to the signal loss occurring in the image path and the wavelength-dependent light scattering, conventional optical coherence tomography could not image the choroid clearly. Recently, Spaide et alCitation27 described commercially available enhanced depth imaging spectral-domain optical coherence tomography (EDI-OCT) which enables quantitative measurement of choroidal thickness and topographyCitation27–Citation32 in various diseases, such as ICSCR,Citation33 myopia,Citation34 age-related macular degeneration,Citation28,Citation35 diabetes,Citation36 and glaucoma.Citation37
Maruko et alCitation38 reported that subfoveal choroidal thickness could be decreased using a half dose of photodynamic therapy in patients with ICSCR. In the current study, we performed EDI-OCT and ICGA in symptomatic eyes and fellow eyes of patients with acute ICSCR and evaluated the potential changes in subfoveal choroidal thickness after a 1/2 dose of photodynamic therapy in Chinese patients.
Materials and methods
Study design and patient recruitment
This retrospective observational study was performed in consecutive patients diagnosed with unilateral acute ICSCR at the Department of Ophthalmology, Yellow River Hospital, Henan University of Science and Technology, Sanmenxia, Henan Province, People’s Republic of China, from July 2011 to March 2013. The study received approval from the institutional review board of Yellow River Hospital (approval number 2011-07-03). Written informed consent was obtained from all patients, and the procedures used followed the tenets of the Declaration of Helsinki. For the comparative study, a group of healthy sex-matched and age-matched (±5 years) subjects were recruited from our students, hospital staff, and families.
Diagnosis of acute ICSCR
All participants underwent the following clinical examination: best-corrected visual acuity, slit-lamp biomicroscopy, indirect ophthalmoscopy, fluorescein angiography, and ICGA (TRC-50DX/IMAGEnet 2000; Topcon Medical Systems Inc, Tokyo, Japan). Acute ICSCR was diagnosed if patients had: subretinal fluid involving the macula associated with idiopathic leaks from the retinal pigment epithelium seen on fluorescein angiography; subretinal fluid confirmed by optical coherence tomography; and persistent serous retinal detachment for less than 6 months without widespread decompensation of the retinal pigment epithelium.
Inclusion and exclusion criteria
Inclusion criteria were: acute ICSCR; only a single eye with neurosensory retina or pigment epithelial detachment; age 20–70 years; and no spontaneous resolution after 3 months of conservative management. Exclusion criteria were: chronic ICSCR; a history of ocular disease, such as polypoidal choroidal vasculopathy, myopia, or age-related macular degeneration; a history of ocular surgery or photocoagulation; pregnancy; steroid use; and any other systemic disease.
Photodynamic therapy in acute ICSCR
The photodynamic therapy protocol was performed using a one third dose (2 mg/m2) of verteporfin (Visudine®; Novartis, Basel, Switzerland) to treat patients with acute ICSCR.Citation20 After intravenous administration of the 1/3 dose of verteporfin for 10 minutes, we then used a 689 nm laser system (Carl Zeiss, Dublin, CA, USA) to deliver an activating laser (dose 50 J/cm2) to the fundus of each patient. The exposure time was 83 seconds. The laser spot size was the diameter of the hyperpermeability region of ICGA plus 500 μm.
Examination of subfoveal choroidal thickness
Subfoveal choroidal thickness was evaluated in the patients with acute ICSCR at baseline and 3 days, one week, 4 weeks, and 12 weeks after photodynamic therapy. The choroid was observed by EDI-OCT (Spectralis HRA + OCT, Heidelberg Engineering, Heidelberg, Germany). The device was positioned close to the eye to obtain inverted images of the fundus, but the images were reinverted for display. Eye tracking was used during measurement. Seven sections, each containing 25 averaged raw scans, were obtained within a 5–30 degree rectangle centered on the fovea. Choroidal thickness (defined as the zonal area between the inner scleral surface and the outer retinal pigment epithelium surface) was measured subfoveally on the transfoveolar scan using the manufacturer’s software (Heidelberg Eye Explorer version 1.6.1.0). Although the thickest section of the choroid might not be at the subfoveal region, in this study we measured the subfoveal choroidal thickness as an indicator to avoid selection bias. All measurements were performed independently by two experienced examiners. If the measurements differed by more than 15%, the examiners performed the measurement together twice.
Statistical analyses
All data was analyzed by PASW statistics version 18.0 (SPSS Inc, Chicago, IL, USA). The independent t-test, paired t-test, or least significant difference t-test was used to evaluate subfoveal choroidal thickness. Fisher’s Exact tests were used to compare the difference in other clinical data. Results were considered to be statistically significant at P-values of 0.05.
Results
Baseline demographic characteristics
A total of 63 patients were finally enrolled ie, 31 patients in the photodynamic therapy group and 32 patients in the control group. There was no statistically significant difference between the two groups with regard to mean age and sex (P=0.68 and P=0.78, respectively). The mean spherical equivalent refractive error in the photodynamic therapy group was −1.69±2.24 diopters compared with −2.54±1.96 diopters in the control group; the difference was statistically significant (P=0.02). The mean interval between onset of symptoms and treatment in the photodynamic therapy group was 45.74±22.85 weeks ().
Table 1 Baseline demographic characteristics
Characteristics of ICGA
Of the 64 eyes from the 32 patients in the control group, ten (15.63%) had hyperfluorescence defined as choroidal vascular hyperpermeability in the middle phase of ICGA and 54 eyes (84.37%) did not have hyperfluorescence.
In the photodynamic therapy group, before treatment, 30 (96.78%) symptomatic eyes and 23 (74.19%) fellow eyes from 31 patients showed a mottling hyperfluorescence in the middle phase of ICGA. Four weeks after treatment, we found that 20 (64.51%) symptomatic eyes showed hypofluorescence corresponding to the area of photodynamic therapy irradiation at the posterior pole. The rate of choroidal vascular hyperpermeability in the fellow eye remained unchanged. This phenomenon persisted throughout the study.
Changes in subfoveal choroidal thickness
The mean subfoveal choroid thickness changes at baseline and follow-up are summarized in , and . At baseline, the mean subfoveal choroid thickness in symptomatic eyes was significantly greater than in fellow eyes (422±132 μm and 367±114 μm, respectively, P=0.036). Mean subfoveal choroid thickness in the fellow eyes was significantly greater than in the control group (367±114 μm and 274±53 μm, respectively, P<0.001).
Figure 1 The changes of subfoveal choroidal thickness after photodynamic therapy.
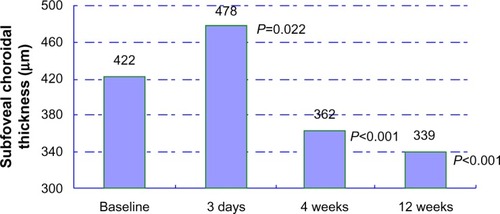
Table 2 Subfoveal choroidal thickness at baseline
Table 3 Subfoveal choroidal thickness during follow-up
Based on the ICGA, the mean subfoveal choroid thickness of fellow eyes with hyperfluorescence was significantly greater than those without hyperpermeability (446±105 μm versus 279±115 μm, P<0.001). When comparing the difference between subfoveal choroidal thickness in the fellow eyes without hyperfluorescence and that in the control group, we found a negative result (279±115 μm versus 274±53 μm, P=0.520).
After photodynamic therapy, the mean subfoveal choroidal thickness increased significantly from 422±132 μm at baseline to 478±163 μm at day 3 (P=0.022) and then decreased to 362±113 μm at week 4 (P<0.001 versus baseline) and to 339±135 μm at week 12 (P<0.001 versus baseline, ). During follow-up, an interesting case occurred in the photodynamic therapy group ().
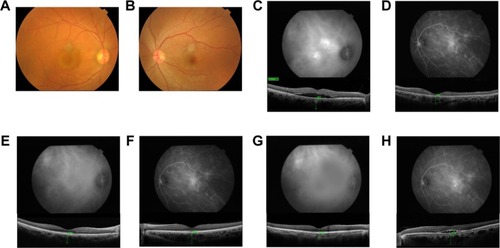
Figure 2 Case 1, a 36-year-old man with blurred vision in his right eye. (A) A fundus photograph of the right eye showing a serous retinal detachment at the fovea. (B) Fundus photograph of the left eye is normal. (C and D) ICGA showed bilateral choroidal vascular hyperpermeability in middle-phase. The subfoveal choroidal thickness at the baseline was 452 μm in the right eye and 351 μm in the left eye. (E and F) After PDT, the subfoveal choroidal thickness in his right eye decreased to 370 μm at week 4. However, the subfoveal choroidal thickness in the left eye increased to 494 μm, with ICGA indicating aggravation of his choroidal vascular hyperpermeability. (G and H) At week 11, in his left eye, ICGA showed aggravation of choroidal vascular hyperpermeability in middle-phase, with a subfoveal choroidal thickness of 470 μm.
Absorption of subretinal fluid
At successive follow-ups, the subretinal fluid in 19 patients decreased significantly at 4 weeks after photodynamic therapy, but not at day 3 and week 1. After 12 weeks of follow-up, the subretinal fluid in 25 patients was already fully absorbed.
Safety
During follow-up, no adverse systemic or ocular events occurred.
Discussion
In the current study, we used EDI-OCT to evaluate changes in subfoveal choroid thickness after photodynamic therapy in patients with acute ICSCR. Our findings support the view that photodynamic therapy can decrease choroidal vascular hyperpermeability and choroidal thickness. Our findings also showed that the subfoveal choroid in patients with acute ICSCR was thicker than in healthy subjects, with the subfoveal choroid in symptomatic eyes being significantly thicker than in the fellow eyes. To our knowledge, this is the first study using EDI-OCT to quantitatively assess changes in subfoveal choroidal thickness after a one third dose of photodynamic therapy in a relatively large sample of patients with acute ICSCR.
Subfoveal choroidal thickness in healthy subjects has been reported to be between 261 μm and 354 μm.Citation29,Citation30,Citation39–Citation42 Our study showed that mean subfoveal choroidal thickness in the control group was 274 μm. The variation in results from the different studies may be attributable to variations in patient age, sex, axial length, and refractive condition, as well as the optical coherence tomography device used. Patient ageCitation28,Citation30,Citation40,Citation43 has been recognized as the most influential factor in choroidal thickness. An EDI-OCT-based study undertaken by Margolis and SpaideCitation30 reported mean decreases in choroidal thickness of 15.6 μm per year in normal eyes. Ikuno et alCitation40 confirmed this finding. However, this theory might not suit for ICSCR patients. Imamura et alCitation33 reported that choroidal thickness did not correlate with age in ICSCR patients (r=0.15, P=0.43). Axial length is another important influencing factor. Li et alCitation42 reported that subfoveal choroidal thickness decreased by 58.2 μm per mm increase in axial length adjusted for age and sex. Esmaeelpour et alCitation44 agreed with this view, and found that axial length was the most important determinant of choroidal thickness. Further, sex has been reported as another influential factor in choroidal thinning. In a multiple regression model,Citation42 after adjustment for age and axial length, subfoveal choroidal thickness was on average 62 μm thicker in men than in women (95% confidence interval 21–104; P=0.0039). In contrast, Park and OhCitation45 analyzed the association between sex and choroidal thickness, and found that the mean subfoveal thickness in males was 9 μm thicker than in females, but the difference was not significantly different (P>0.05). Moreover, an association between refractive condition and subfoveal choroidal thickness has also been reported. Ho et alCitation46 suggested that subfoveal choroidal thickness decreased by 6.205 μm for each diopter in patients with myopia. However, ICSCR patients are often hyperopic. In the current study, the mean spherical equivalent refractive error in the photodynamic therapy group was −1.69±2.24 diopters compared with −2.54±1.96 diopters in the control group; this difference reached statistical significance (P=0.02). This might be one reason why the subfoveal choroid in patients with ICSCR is thicker than in the normal population.
Most acute ICSCR is actually bilateral, even if subretinal fluid is active in one eye. Choroidal vascular hyperpermeability might have a crucial role in ICSCR. In an ICGA study, Iida et alCitation10 found that the incidence of choroidal vascular hyperpermeability was 62% in fellow eyes compared with 95% in symptomatic eyes. In the current study, 96.78% of symptomatic eyes and 74.19% of fellow eyes showed hyperfluorescence in the middle phase of ICGA in the photodynamic therapy group. This is similar to the findings of a study reported by Maruko et al.Citation47 Choroidal vascular hyperpermeability is always accompanied by choroid thickening in ICSCR patients. Imamura et alCitation33 reported that the choroid in patients with ICSCR was thicker bilaterally (including for symptomatic eyes and fellow eyes) than in normal eyes. In our study, the subfoveal choroid in symptomatic eyes was significantly thicker than in fellow eyes (P=0.036), and the subfoveal choroid in fellow eyes was significantly thicker than in age-matched and sex-matched control eyes (P<0.001). The subfoveal choroid thickness of the fellow eyes with hyperfluorescence in ICGA was significantly higher than that in those without hyperpermeability (P<0.001). When we compared the difference between subfoveal choroidal thickness in the fellow eyes without hyperfluorescence and the control eyes, we found a negative result (P=0.520). These findings indicate that choroidal vascular hyperpermeability plays an important role in pathophysiology of ICSCR.
Photodynamic therapy with verteporfin, which has an occlusive effect in the choriocapillary layers, could decrease choroidal vascular hyperpermeability and subsequently choroidal thickness.Citation18,Citation21 Schlotzer-Schrehardt et alCitation24 and Schmidt-Erfurth et alCitation25 reported that photodynamic therapy has a dose-dependent profile. Increasing the dose of verteporfin or laser irradiation would increase the risk of vascular damage or cytotoxicity to the retina and choroid. It is important to balance the maximum therapeutic effect and the minimum complications. Half-dose photodynamic therapyCitation38 has been used widely to treat ICSCR, but might not be suitable for Chinese patients. Zhao et alCitation26 used photodynamic therapy with various doses of verteporfin (70%, 60%, 50%, 40%, 30%, 20%, and 10% of the full dose) to manage ICSCR patients, and their results showed that 30% of the full dose of verteporfin was the lowest effective dose. In our study, following the recommendation of Zhao et al, we chose the 30% dose of verteporfin to manage our ICSCR patients. To our surprise, the mean choroidal thickness increased significantly from 422±132 μm at baseline to 478±163 μm at day 3. This transient increase in choroidal thickness may be a sign of increased exudation in the choroid. Eventually, after impairment of the choriocapillaris and vascular remodeling in the underlying choroid the choroidal thickness decreased to 362±113 μm at week 4 and to 339±135 μm at week 12. Accompanying the changes in choroidal thickness, at week 4, we found that 64.51% of symptomatic eyes showed hypofluorescence corresponding to the area of photodynamic therapy irradiation at the posterior pole. Maruko et alCitation38 reported similar findings, ie, mean choroidal thickness increased from 389±106 μm at baseline to 462±124 μm (P=0.008) on day 2 after treatment, then reduced to 360±100 μm at week 1 and to 330±103 μm at week 4, with ICGA also showing decreased hyperpermeability Maruko et alCitation38 used photodynamic therapy with a half dose (3 mg/m2) of verteporfin, which was higher than that (2 mg/m2) used in our study, but with similar efficacy Recently, a prospective, nonrandomized consecutive, open-label case series conducted by Uetani et alCitation48 reported an opposite outcome. In that study, Uetani et al compared the effects of a half-dose of verteporfin with those of a one-third dose of verteporfin for ICSCR. In the half-dose photodynamic therapy group, choroidal thickness reduced significantly from baseline. However, in the 1/3 dose photodynamic therapy group, choroidal thickness decreased in two eyes in which subretinal fluid disappeared but did not change in the other eyes. However, only six patients were assigned to the photodynamic therapy group in that study, so the sample size was relatively small which might have led to bias.
Our retrospective study has some limitations. Acute ICSCR is well known to recur in some cases, so 3 months of follow-up seems to be short. A long-term study to evaluate the changes in subfoveal choroidal thickness and recurrence rate after photodynamic therapy is necessary. Additionally, the current EDI-OCT does not have automatic choroid segmentation software. Manual operation might lead to inaccuracy in some cases, so automatic choroid segmentation software is needed in future research. Moreover, the relationship between severity of hyperpermeability in ICGA and choroidal thickening should be investigated.
In conclusion, our findings revealed that: the subfoveal choroid in patients with acute ICSCR was thicker than in the normal population, with symptomatic eyes being significantly thicker than in fellow eyes; compared with half-dose or full-dose photodynamic therapy, a one-third dose of verteporfin could decrease choroidal vascular hyperpermeability and choroidal thickness in patients with acute ICSCR.
Disclosure
The authors report no conflicts of interests in this work.
References
- NegiAMarmorMFExperimental serous retinal detachment and focal pigment epithelial damageArch Ophthalmol198410234454496703994
- NegiAMarmorMFThe resorption of subretinal fluid after diffuse damage to the retinal pigment epitheliumInvest Ophthalmol Vis Sci19832411147514796642927
- GassJDPathogenesis of disciform detachment of the neuroepitheliumAm J Ophthalmol196763Suppl 311396019308
- SpaideRFGoldbaumMWongDWTangKCIidaTSerous detachment of the retinaRetina200323682084614707834
- HayashiKHasegawaYTokoroTIndocyanine green angiography of central serous chorioretinopathyInt Ophthalmol19869137413721709
- GuyerDRYannuzziLASlakterJSSorensonJAHoAOrlockDDigital indocyanine green videoangiography of central serous chorioretinopathyArch Ophthalmol19941128105710628053819
- SpaideRFHallLHaasAIndocyanine green videoangiography of older patients with central serous chorioretinopathyRetina19961632032138789858
- SpaideRFCampeasLHaasACentral serous chorioretinopathy in younger and older adultsOphthalmology199610312207020799003341
- ShirakiKMoriwakiMMatsumotoMYanagiharaNYasunariTMikiTLong-term follow-up of severe central serous chorioretinopathy using indocyanine green angiographyInt Ophthalmol19971998215245253
- IidaTKishiSHagimuraNShimizuKPersistent and bilateral choroidal vascular abnormalities in central serous chorioretinopathyRetina199919650851210606450
- PrunteCFlammerJChoroidal capillary and venous congestion in central serous chorioretinopathyAm J Ophthalmol1996121126348554078
- GiovanniniAScassellati-SforzoliniBD’AltobrandoEMariottiCRutiliTTittarelliRChoroidal findings in the course of idiopathic serous pigment epithelium detachment detected by indocyanine green videoangiographyRetina19971742862939279943
- DoroDVisentinSMaimonePEPilottoEHigh-resolution ultrasonography in central serous chorioretinopathyAm J Ophthalmol2005139355055215767075
- TittlMPolskaEKircherKTopical fundus pulsation measurement in patients with active central serous chorioretinopathyArch Ophthalmol2003121797597812860800
- TittlMMaarNPolskaEWeigertGSturMSchmettererLChoroidal hemodynamic changes during isometric exercise in patients with inactive central serous chorioretinopathyInvest Ophthalmol Vis Sci200546124717472116303970
- RobertsonDMIlstrupDDirect, indirect, and sham laser photocoagulation in the management of central serous chorioretinopathyAm J Ophthalmol19839544574666682293
- FickerLVafidisGWhileALeaverPLong-term follow-up of a prospective trial of argon laser photocoagulation in the treatment of central serous retinopathyBr J Ophthalmol198872118298343061449
- YannuzziLASlakterJSGrossNEIndocyanine green angiography guided photodynamic therapy for treatment of chronic central serous chorioretinopathy: a pilot studyRetina200323328829812824827
- Cardillo PiccolinoFEandiCMVentreLRigault de la LongraisRCGrignoloFMPhotodynamic therapy for chronic central serous chorioretinopathyRetina200323675276314707823
- ChanWMLaiTYLaiRYTangEWLiuDTLamDSSafety enhanced photodynamic therapy for chronic central serous chorioretinopathy: one-year results of a prospective studyRetina2008281859318185143
- ChanWMLaiTYLaiRYLiuDTLamDSHalf-dose verteporfin photodynamic therapy for acute central serous chorioretinopathy: one-year results of a randomized controlled trialOphthalmology2008115101756176518538401
- ShinJYWooSJYuHGParkKHComparison of efficacy and safety between half-fluence and full-fluence photodynamic therapy for chronic central serous chorioretinopathyRetina201131111912620890242
- Schmidt-ErfurthULaquaHSchlötzer-SchrehardUViestenzANaumannGOHistopathological changes following photodynamic therapy in human eyesArch Ophthalmol2002120683584412049594
- Schlotzer-SchrehardtUViestenzANaumannGOLaquaHMichelsSSchmidt-ErfurthUDose-related structural effects of photodynamic therapy on choroidal and retinal structures of human eyesGraefes Arch Clin Exp Ophthalmol2002240974875712271373
- Schmidt-ErfurthUMichelsSBarbazettoILaquaHPhotodynamic effects on choroidal neovascularization and physiological choroidInvest Ophthalmol Vis Sci200243383084111867605
- ZhaoMWZhouPXiaoHXPhotodynamic therapy for acute central serous chorioretinopathy: the safe effective lowest dose of verteporfinRetina20092981155116119629018
- SpaideRFKoizumiHPozzoniMCEnhanced depth imaging spectral-domain optical coherence tomographyAm J Ophthalmol2008146449650018639219
- SpaideRFAge-related choroidal atrophyAm J Ophthalmol2009147580181019232561
- BranchiniLRegatieriCVFlores-MorenoIBaumannBFujimotoJGDukerJSReproducibility of choroidal thickness measurements across three spectral domain optical coherence tomography systemsOphthalmology2012119111912321943786
- MargolisRSpaideRFA pilot study of enhanced depth imaging optical coherenceAm J Ophthalmol2009147581181519232559
- BarteselliGChhablaniJEl-EmamSChoroidal volume variations with age, axial length, and sex in healthy subjects: a three-dimensional analysisOphthalmology2012119122572257822921388
- ChhablaniJBarteselliGWangHRepeatability and reproducibility of manual choroidal volume measurements using enhanced depth imaging optical coherence tomographyInvest Ophthalmol Vis Sci20125342274228022427584
- ImamuraYFujiwaraTMargolisRSpaideRFEnhanced depth imaging optical coherence tomography of the choroid in central serous chorioretinopathyRetina200929101469147319898183
- FujiwaraTImamuraYMargolisRSlakterJSSpaideRFEnhanced depth imaging optical coherence tomography of the choroid in highly myopic eyesAm J Ophthalmol2009148344545019541286
- KoizumiHYamagishiTYamazakiTKawasakiRKinoshitaSSubfoveal choroidal thickness in typical age-related macular degeneration and polypoidal choroidal vasculopathyGraefes Arch Clin Exp Ophthalmol201124981123112821274555
- EsmaeelpourMPovazayBHermannBMapping choroidal and retinal thickness variation in type 2 diabetes using three-dimensional 1060-nm optical coherence tomographyInvest Ophthalmol Vis Sci20115285311531621508108
- MaulEAFriedmanDSChangDSChoroidal thickness measured by spectral domain optical coherence tomography: factors affecting thickness in glaucoma patientsOphthalmology201111881571157921492939
- MarukoIIidaTSuganoYOjimaAOgasawaraMSpaideRFSubfoveal choroidal thickness after treatment of central serous chorioretinopathyOphthalmology201011791792179920472289
- DingXLiJZengJChoroidal thickness in healthy Chinese subjectsInvest Ophthalmol Vis Sci201152139555956022058342
- IkunoYKawaguchiKNouchiTYasunoYChoroidal thickness in healthy Japanese subjectsInvest Ophthalmol Vis Sci20105142173217619892874
- ManjunathVTahaMFujimotoJGDukerJSChoroidal thickness in normal eyes measured using Cirrus HD optical coherence tomographyAm J Ophthalmol2010150332532920591395
- LiXQLarsenMMunchICSubfoveal choroidal thickness in relation to sex and axial length in 93 Danish university studentsInvest Ophthalmol Vis Sci201152118438844121917938
- RamrattanRSvan der SchaftTLMooyCMde BruijnWCMulderPGde JongPTMorphometric analysis of Bruch’s membrane, the choriocapillaris, and the choroid in agingInvest Ophthalmol Vis Sci1994356285728648188481
- EsmaeelpourMPovazayBHermannBThree-dimensional 1060-nm OCT: choroidal thickness maps in normal subjects and improved posterior segment visualization in cataract patientsInvest Ophthalmol Vis Sci201051105260526620445110
- ParkKAOhSYChoroidal thickness in healthy childrenRetina20133391971197623644561
- HoMLiuDTChanVCLamDSChoroidal thickness measurement in myopic eyes by enhanced depth optical coherence tomographyOphthalmology201312091909191423683921
- MarukoIIidaTSuganoYOjimaASekiryuTSubfoveal choroidal thickness in fellow eyes of patients with central serous chorioretinopathyRetina20113181603160821487334
- UetaniRItoYOiwaKIshikawaKTerasakiHHalf-dose vs one-third-dose photodynamic therapy for chronic central serous chorioretinopathyEye (Lond)201226564064922573069