
Abstract
Duchenne muscular dystrophy (DMD) is an X-linked myopathy resulting in progressive weakness and wasting of all the striated muscles including the respiratory muscles. The consequences are loss of ambulation before teen ages, cardiac involvement and breathing difficulties, the main cause of death. A cure for DMD is not currently available. In the last decades the survival of patients with DMD has improved because the natural history of the disease can be changed thanks to a more comprehensive therapeutic approach. This comprises interventions targeted to the manifestations and complications of the disease, particularly in the respiratory care. These include: 1) pharmacological intervention, namely corticosteroids and idebenone that significantly reduce the decline of spirometric parameters; 2) rehabilitative intervention, namely lung volume recruitment techniques that help prevent atelectasis and slows the rate of decline of pulmonary function; 3) scoliosis treatment, namely steroid therapy that is used to reduce muscle inflammation/degeneration and prolong ambulation in order to delay the onset of scoliosis, being an additional contribution to the restrictive lung pattern; 4) cough assisted devices that improve airway clearance thus reducing the risk of pulmonary infections; and 5) non-invasive mechanical ventilation that is essential to treat nocturnal hypoventilation, sleep disordered breathing, and ultimately respiratory failure. Without any intervention death occurs within the first 2 decades, however, thanks to this multidisciplinary therapeutic approach life expectancy of a newborn with DMD nowadays can be significantly prolonged up to his fourth decade. This review is aimed at providing state-of-the-art methods and techniques for the assessment and management of respiratory function in DMD patients.
Introduction
Duchenne muscular dystrophy (DMD) is an X-linked myopathy that affects one out of 3,600–6,000 male births.Citation1–Citation3 It is caused by mutations in the dystrophin gene leading to a defect in the protein dystrophin which results in progressive weakness and wasting of all the striated muscles. At the beginning, the proximal lower limb muscles are affected followed by the shoulder muscles, by the distal limb muscle, and ultimately by the respiratory muscles. The consequences are progressive impairment of motor skills, loss of ambulation before teen ages, orthopedic complications, cardiac involvement, and breathing difficulties. Without any intervention, death occurs around the age of 19 due to cardiac and respiratory failure.Citation4–Citation7 At the moment therapy is not available, but in the last decades the survival of these patients improved and a newborn with DMD now has a life expectancy into the fourth decade.Citation3,Citation8–Citation10 The natural history of the disease can now be changed thanks to a more comprehensive therapeutic approach comprising interventions targeted to the manifestations and complications of the disease, particularly in respiratory care.Citation7,Citation11–Citation14 ACE-inhibitions are used to prevent or improve cardiomyopathy. Corticosteroids are used to reduce muscle inflammation, minimize later complications, and prolong ambulation.Citation3,Citation15,Citation16 When the patient becomes non-ambulatory, treatments aim to reduce the risk of progressive scoliosis and stabilizing pulmonary function. According to the internationally recognized guidelines, a structured approach to respiratory management of DMD during the progression of the disease comprises: 1) the monitoring of respiratory function to deal with respiratory complications timely; 2) lung volume recruitment (LVR) techniques to open the lung and reduce atelectasis; 3) the use of a cough assisted device to improve airway clearance and to reduce the risk of pulmonary infections; and 4) the use of non-invasive ventilation (NIV) to deal with nocturnal hypoventilation, sleep disordered breathing, and ultimately respiratory failure.Citation8,Citation11,Citation13,Citation14
The genetic therapy represents hope for the future to develop a definitive cure for DMD. Many promising researches on skeletal muscles are currently under development although not specifically addressed to respiratory muscles.Citation17,Citation18
The present review article is thought to provide a state-of-the-art methods and techniques for the assessment and management of respiratory function in DMD patients. In particular, the techniques currently used for respiratory functional evaluation are illustrated, indicating limits, advantages, and usefulness for assessing the effects of different possible kinds of intervention.
Assessment of respiratory function
The causes of death in DMD patients are both respiratory and cardiac, with the former being the main cause until the 1980s to 1990s. More recently, the structured approach to respiratory problems and, in particular, the institution of nocturnal NIV, had a major effect on survival. Since respiratory failure, however, is still among the main causes of death in patients affected by DMD,Citation3,Citation5–Citation7,Citation12 it is extremely important to measure lung and respiratory muscle function in order to monitor the progression of the disease, identify early signs of respiratory failure, and therefore plan optimal interventions to improve the quality of life and longevity in these patients. The assessment of respiratory function is also important to quantify the possible effects of innovative therapeutic trials.
According to their invasiveness and to the collaboration required to the patients, lung and respiratory muscle function tests are classified as non-invasive/non-volitional, non-invasive/volitional, invasive/non-volitional, and invasive/volitional. These tests can be “specific” or “global” according to whether they allow to distinguish between the contribution and the relative involvement of the different respiratory muscles, namely the diaphragm, the intercostal muscles, the abdominal muscles, and the accessory inspiratory muscles. These tests can assess: i) the level of muscle activation by measuring the electrical activity of the muscle (electromyography [EMG]); ii) the force developed by the muscles by measuring the pressure developed; iii) the resulting action of the contraction of the muscles by measuring flow and/or volume; or iv) the morphology of the muscles with different imaging techniques.Citation19
Non-invasive/non-volitional tests
The electrical activity of each respiratory muscle can be non-invasively measured by transcutaneous EMG using surface electrodes. Unfortunately, at rest the signal/noise ratio is very poor, particularly in weak muscles, because of the “crosstalk” of other muscles, including cardiac activity.Citation20,Citation21
The ventilatory pattern during quiet breathing at rest can be measured at the mouth on a breath-by-breath base by a pneumotachograph preferable using a mask rather than a mouthpiece in order to avoid possible leakage due to weakness of cheek muscle and macroglossia, which are common characteristics in the advanced stages of the disease. The face mask connection to the lung function device is a valid alternative; however, it is important to choose the appropriate prediction equations, depending on subject-instrument interface.Citation22 From the integration of the flow signal, tidal volume (VT) and breathing frequency (fR) are measured and minute ventilation (VE = VT*fR) and rapid and shallow breathing index (RSBi = fR/VT) derived.Citation23 These are global respiratory indexes that can be performed at any age and in different postures: standing, seated, and supine.
Measurements of thoraco-abdominal motion do not require the use of mouthpiece or mask and can be divided into three groups:
– those recording the anteroposterior variations of chest wall diameters, such as the magnetometers (ie, coils placed anteriorly and posteriorly on the ribcage and the abdomen);Citation24
– those measuring variations of ribcage and abdominal cross-sectional areas, such as respiratory inductive plethysmography (ie, coils sewn in belts or wearable garments placed below the axillary line and above the umbilicus);Citation19,Citation25
– those measuring total and compartmental chest wall volumes, such as opto-electronic plethysmography that detects the 3D displacement of a large set of reflective markers placed on the thoraco-abdominal surface of the subject.Citation26–Citation29
Although the shape of the diaphragm can be reconstructed with an excellent resolution by using magnetic resonance imaging (MRI), its clinical use is still limited because of the high cost. Moreover, patients are not always able to maintain the supine posture for the prolonged time required for the acquisition.Citation30
On the other hand, ultrasound (US) imaging is increasingly used since it allows to non-invasively study the diaphragm at rest from three different views: 1) the displacement of the diaphragm dome by positioning the US probe on the anterior abdominal wall; 2) the length of apposition of the diaphragm by positioning the US probe on the lateral ribcage; and 3) the thickness of the diaphragm by positioning the US probe in the intercostal space around the eighth rib.Citation31–Citation33
Non-invasive/volitional tests
All non-invasive/volitional tests require repetition of maximal efforts to get reliable results that can fatigue the weak muscles of DMD patients. They also require full cooperation and are difficult for children to perform. Cooperative children over the age of 7 are considered able to perform reproducible and therefore reliable maneuvers.
Maximal static inspiratory (MIP) and expiratory (MEP) pressures measured at the mouth provide a global index of inspiratory and expiratory muscle strength, respectively. Being MIP and MEP influenced by respiratory muscle length that in turn depends on lung volume, it is crucially important to control the lung volume at which the maneuver is performed. MIP has to be performed at residual volume (RV) and MEP at total lung capacity (TLC), respectively when inspiratory and expiratory muscles are maximally stretched.Citation19,Citation34
Sniff nasal inspiratory pressure (SNIP) measured at the nostril is generally easier to perform, since the requested maneuvers is more natural. If performed correctly (ie, with an outward movement of the belly), it can be considered a specific index of the strength of the diaphragm, although in presence of nasal obstruction it underestimates the real pressure.Citation19,Citation35,Citation36
Inspiratory muscle fatigue can be assessed by the tension time index (TTI) that is calculated as P0.1/MIP· duty cycle, where P0.1 is the pressure measured during the first 100 milliseconds of occlusion while breathing quietly and the duty cycle is the ratio between inspiratory time and the total time duration of the breath. High values of TTI indicate that inspiratory muscles are at risk of fatigue.Citation37–Citation40
Peak expiratory flow (PEF) and cough peak flow (CPF) are measured at the mouth respectively during a maximal exhalation and cough. They provide information on the expiratory muscles.Citation41
Traditional spirometric parameters such as forced vital capacity (FVC) and forced expiratory volume in 1 second (FEV1) are global indexes of the respiratory function. Values above 80% of their ratio (FEV1/FVC), the Tiffenau index, can indicate the presence of restrictive lung disease. The diagnosis has to be confirmed by reduced values of TLC. A drop in FVC (>20%), when the patient goes from sitting to supine position, is a more specific sign of diaphragmatic weakness.Citation42
TLC, functional residual capacity, and RV are absolute lung volumes that cannot be measured by simple spirometry. They require either nitrogen washout technique or body plethysmography. Wheel-chair bound DMD patients can meet great difficulties in entering a body plethysmograph.Citation19,Citation43–Citation46
Invasive/non-volitional tests
Invasive/non-volitional tests imply the use of esophageal and/or gastric unpleasant balloon-catheter systems. They provide specific indexes of the different respiratory muscles. The use of the catheters is not recommended in very severe DMD patients with difficulties in swallowing to avoid regurgitation and aspiration.Citation19 An additional caution of pressure measurements by esophageal and gastric balloons is represented by the possible bradycardia mediated by the stimulation of the vagal nerve. They can be used during quiet breathing at rest without requiring any manouvers.Citation47
The measurement of esophageal pressure (POES), based on transducer-catheter-balloon system placed in the lower third of the esophagus, is considered a useful surrogate of pleural pressure while abdominal gastric pressure (PGA) is measured by placing the transducer-catheter-balloon system in the stomach. The trans-diaphragmatic pressure (PDI) is calculated as PGA–POES and represents the force generated by the diaphragm.Citation19 The ratio between swings of PGA and PDI (ΔPGA/ΔPDI) during spontaneous quiet breathing is able to provide an assessment of paradoxical breathing.Citation48
Peak PDI during magnetic stimulation of the phrenic nerve tests the strength of the diaphragm in non-cooperative patients.Citation49
Volumetric computed tomography imaging can be used to obtain 3D reconstruction of the diaphragm with an excellent resolution, but the radiation exposure limits the clinical use of this technique in DMD patients.Citation50
Invasive/volitional tests
Invasive/volitional tests include the measurements of POES, PGA, and PDI during maximal maneuvers like sniff and cough.Citation51,Citation52 Maximal POES and PDI during sniff maneuvers represent reliable indexes of the strength of global inspiratory muscles and of the diaphragm, respectively;Citation36,Citation53,Citation54 while PGA during maximal cough is an index of the strength of expiratory muscles.Citation51,Citation55 Because cough efficacy depends on the inspiratory volume preceding the maneuver, lung volume is a source of variability and should be controlled.Citation56
summarizes the different techniques, categorized into invasive/non-invasive, and volitional/non-volitional, which are used to evaluate different ventilatory functional parameters in DMD patients, as reported in the literature.
Table 1 Assessment of ventilatory function in DMD
Respiratory function in DMD
Respiratory function assessed by non-invasive non-volitional tests
During spontaneous quiet breathing at rest in supine position, VE decreases because of the reduction of VT with preserved respiratory rate, particularly in older DMD patients.Citation57 In seated position VE does not change significantly because respiratory rate increases to compensate for the fall of VT.Citation37,Citation58,Citation59
The abdominal contribution to VT in supine position during inspiration is an index of the action of the diaphragm. It progressively decreases with age and it is an important predictor of nocturnal hypoexemiaCitation57,Citation60 and inefficient cough.Citation61
Quantitative muscle US is a non-invasive child-friendly tool able to measure DMD muscle changes in terms of both echo intensity and muscle thickness.Citation62 DMD patients are characterized by poor spirometry, reduced inspiratory muscle force (lower MIP), and higher diaphragmatic thickness, measured at its appositional zone by B-mode ultrasonography, compared to healthy controls. This may indicate pseudo-hypertrophy of the diaphragm secondary to infiltration of connective tissue and fat deposition as occurs in limb muscles.Citation63
Recent studies investigating MRI measurements of T2 relaxation time (MRI-T2) on lower limb muscles in patients and on canine model confirm the feasibility of MRI to objectively and non-invasively measure muscle pathology in DMD.Citation64–Citation67 MRI-T2 of the sternocleidomastoid muscle of DMD patients are significantly lower than an age-matched control group indicating altered tissue composition.Citation68 MRI, therefore, represents a potentially promising technique for early detection of disease progression not only of limb muscles but also of the diaphragm and other respiratory muscles in DMD. It can also be used to assess the efficacy of therapeutic interventions on the muscles.
Respiratory function assessed by non-invasive volitional tests
The absolute value of FVC follows a pathognomonic pattern characterized by an ascending phase, a peak approximately at 12–14 years, and a plateau followed by a descending phase.Citation59,Citation69–Citation74 The absolute value reached at the plateau correlates with life expectancy in these patients.Citation75 Values of FVC lower than 2.1 L are associated to lower CPF and represent important thresholds to start with techniques that improve airway clearance.Citation76 FVC below 1 L is a suitable indicator to consider starting more intensive patient support,Citation69 being a good predictor of severe oxygen desaturation, uncontrolled hypercapnia, and impending death within 12 months.Citation69,Citation77,Citation78 The decline in FVC has recently been shown to be associated with ventilation inhomogeneity assessed by lung clearance index measured with the multiple-breath washout technique.Citation58 The maximal percentage postural difference of FVC in DMD patients is approximately 9%. It tends to decrease with age like MIP values. This can indicate that a global weakness of both inspiratory and expiratory muscles is not able to compensate for the diaphragmatic impairment.Citation79
In DMD, FVC expressed as percentage of the predicted values (FVC%) starts approximately 80% at the age of 10 and then it linearly declines with age as shown by different authors indicating a progressive respiratory muscles weakness.Citation59,Citation69,Citation70,Citation72–Citation74,Citation80–Citation83 FVC% and its decline are prognostic markers in DMD.Citation69
Inspiratory flow reserve volume is defined as the ratio between the maximal inspiratory flow during tidal breathing and during FVC. This ratio is higher in DMD compared to controls indicating a reduction in inspiratory flow reserve in DMD.Citation84
When listed as a function of age, the absolute values of FEV1, functional residual capacity, TLC, RV, inspiratory and expiratory reserve volumes reveal ascending, plateau, and descending phases like FVC.Citation70,Citation73,Citation74 Between the ages of 8 and 12 the restrictive pattern is mainly due to reduced expiratory reserve volumes and increased RV. This can indicate an early deterioration of expiratory muscles. After the age of 16, the decline of lung volumes is associated with reduced inspiratory reserve volumes and TLC and therefore with inspiratory muscles’ impairment.Citation70
MIP and MEP in Duchenne patients are reduced compared to normal values and they decrease with age, with MEP being globally lower than MIP. Expiratory muscles, therefore, seem to be more compromised while inspiratory muscles seem to be relatively preserved.Citation59,Citation70,Citation81 MIP predicts the extent of hypercapniaCitation70 and starts to decline from the age of 10 years onward. Because FVC decay starts a bit later, MIP maneuver seems to be affected earlier than spirometry.Citation72 The mean decline with age of MIP varies from 4% to 6.9%.Citation59,Citation70,Citation72
MEP is associated with cough efficiency: if MEP is higher than 60 cm H2O, DMD patient is expected to have an adequate cough; while MEP below 45 cm H2O is an indicator to start cough-assisting techniques.Citation8,Citation85,Citation86
SNIP increases until the age of 10.5 and decreases thereafter with a mean decline of 4.8 cm H2O (5.2% predicted) per year. Because it declines earlier than FVC, it can be considered an early sign of inspiratory muscle strength. Reliable values of SNIP can be obtained from the age of 5 and therefore its measure should be initiated early in the course of the disease.Citation59,Citation71
With the progression of DMD, fatigue index (TTI) increasesCitation37,Citation87 and consequently, without any intervention, older patients are likely to approach respiratory muscle fatigue.
Respiratory function assessed by invasive non-volitional tests
As indicated earlier, ΔPGA/ΔPDI ratio measured at rest during spontaneous quiet breathing is a non-volitional marker that reflects the relative contribution of the diaphragm to VT. In teenagers with DMD, ΔPGA/ΔPDI is negative indicating that the diaphragm is weaker than the other inspiratory muscles and it paradoxically moves upward. PDI secondary to magnetic stimulation of the phrenic nerve is lower in DMD patients than patients with spinal muscle atrophy and congenital myopathy indicating that Duchenne patients are characterized by the weakest diaphragm.Citation51
Respiratory function assessed by invasive volitional tests
Trans-diaphragmatic and POES during sniff are low and progressively decrease after the age of 10 years. The evolution of gastric pressure during cough follows a similar decrement pattern, being significantly reduced by the age of 8 years.Citation51,Citation59
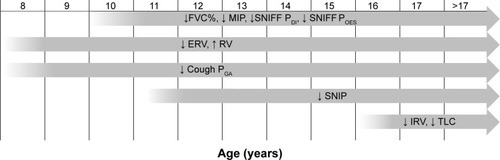
shows a schematic diagram summarizing the natural course of the different respiratory functional parameters over time according to what has been reported in the up-to-date literature.
Figure 1 Schematic diagram summarizing the natural course of the different respiratory functional parameters in DMD.
Abbreviations: FVC, forced vital capacity; MIP, maximal static inspiratory; PDI, trans-diaphragmatic pressure; POES, esophageal pressure; RV, residual volume; PGA, abdominal gastric pressure; SNIP, sniff nasal inspiratory pressure; TLC, total lung capacity; ERV, expiratory reserve volume; IRV, inspiratory reserve volume; DMD, Duchenne muscular dystrophy.
Pharmacological intervention
There is no current curative treatment for DMD and the only medications available and used are glucocorticoid steroids.Citation3,Citation88 The main effects of corticosteroids on skeletal muscles are inflammation reduction, mass increment and deterioration delay. Steroid therapy delays the motor impairment of DMD children by improving muscular strength leading to prolonged ambulation for up to 2–3 years longer.Citation16,Citation89–Citation95 At the beginning, steroid therapy was prescribed to improve motor function. Successively some authors suggested prolonging the treatment also after patients are wheelchair bound for its potential effect in preventing scoliosis and respiratory deterioration. There are studies showing no effect of steroid therapy on the respiratory function in treated DMD patients.Citation80,Citation83 A stabilization of FVC and FEV1 after 2 years of treatment has been describedCitation96 while another study reports a significant increase of MEP and cough peak flow (CPF) after treatment without FVC improvement/stabilization.Citation97 Many authors have found the effectiveness of steroid treatment in improving spirometry in their cohort of DMD patients.Citation98–Citation100 Two reasons can explain such a discrepancy in the role of steroid therapy on lung function in DMD: the lack of standardization in steroid administration and/or the binary subdivision (steroid vs non-steroid) according to the use of therapy. The non-steroid group includes not only young patients, but also old patients who never took the therapy (because its introduction in the clinical management of DMD is relatively new) together with patients who chronically took steroids but in a discontinuous way. As already pointed out by Mayer et alCitation80 the authors believe that the heterogeneity of the two groups can introduce a bias effect on the results since old and therefore more compromised patients can worsen the overall lung function of the group, while the discontinuous-users can contribute in a positive way thanks to the possible beneficial effect of the therapy. The cooperative international neuromuscular research group Duchenne natural history studyCitation15,Citation16 groups 340 DMD patients according to age and to the use of steroids as follows: 1) naïve patients: never used steroids or treated <1 month total and not currently under medication; 2) current recipients; and 3) past users: treated in the past for >1 month and not currently under medication. An overall improved lung function in terms of FVC, FEV1, PEF, MIP, and MEP has been found in the current steroid users across the age groups 10–12 and 13–15 years old.Citation15,Citation16 This demonstrates how crucial it is to properly subdivide patients while testing the efficacy of new therapy in order to avoid possible bias due to the patients’ heterogeneity in their clinical conditions because of the progressive nature of the disease.
Since the use of corticosteroids has well-known side effects, such as weight gain, cataract, osteopenia, behavioral changes, increased insulin resistance, and delayed puberty, there is a high medical need for new effective, safe, and well-tolerated pharmacological therapy able to slow the impairment or even ameliorate the respiratory function in DMD. In a preclinical placebo-controlled study in the mdx mouse idebenone, a potent antioxidant shows cardio-protective effect and improvement in exercise performance.Citation101 A 12-month Phase 2 randomized placebo-controlled trial on a small group of DMD patients shows a significant treatment effect not only on cardiac markers, but also on PEF, as absolute values and as percentage of the predicted values. The beneficial effect of idebenone on PEF is more pronounced in naïve steroid patients rather than in current users, suggesting an inhibitory effect of glucocorticoid steroids.Citation98 Finally, the trial reaches Phase 3 by studying the efficacy of idebenone on respiratory function in DMD patients not on concomitant steroid therapy. Idebenone significantly reduces the decline of different parameters of the respiratory function, namely PEF, FVC, and FEV1, and results have shown it to be safe and well tolerated by patients therefore representing a new therapeutic approach for DMD.Citation102
The goal for future pharmacological therapy is to have at least equal efficacy than glucocorticosteroids but with lower side effect profile. Multiple new treatment approaches have emerged ranging from molecular based therapies aimed to reduce muscle fibrosis or to promote muscle blood flow. It seems more likely that a combination of different approaches, targeting more than one pathway, may be more satisfactory.Citation17,Citation18 Alternative approaches including mutation-specific therapy (gene replacement or repair and stem cell therapy) represent the future possibility to find a definite cure for DMD. There have been genetic-based treatment experiments in the last few years in clinical trials, ie, ataluren for non-sense mutation in the dystrophin gene and antisense oligonucleotide induced exon skipping.Citation103,Citation104 The promising results of some of these studies still have to face the lack of accurate clinical and biological outcome measures able to discriminate between and describe modifications in the disease history.
The ongoing clinical trials are not specifically addressed to study new therapeutic effects on respiratory muscles and consequently do not have respiratory function measures as primary outcomes. The following trials consider respiratory variables as secondary outcome in addition to other clinical and functional measures: a) evaluating the long-term safety of ACE-031 in subjects with DMD;Citation105 b) long-term safety trial of ataluren to treat Becker and Duchenne muscular dystrophies;Citation105 c) NCT02286947;Citation106 d) NCT00264888;Citation106 e) NCT00759876;Citation106 f) NCT01009294;Citation106 g) NCT01239758;Citation106 h) NCT01099761;Citation106 and i) NCT01462292.Citation106
Respiratory muscle training (RMT) and physiotherapy intervention
Respiratory muscles are morphologically and functionally skeletal muscles and therefore RMT can be a possible treatment to improve their strength and endurance and to try to counteract the progressive weakness induced by DMD. The role of RMT in neuromuscular patients is still controversial being potentially dangerous since it may accelerate muscle fatigue by overwork. Beneficial effects of RMT have been shown in DMD. These comprise increased strength of expiratory muscle,Citation107 improved muscle endurance,Citation108 and augmented MIP.Citation109 Another study demonstrates that inspiratory muscle training (IMT) through resistive breathing and/or efforts against a variable inspiratory resistance allows diaphragmatic training in terms of strength and endurance. Peak esophageal and PDI during sniff maneuvers have been measured before and after 6 months of training. In ten out of 15 patients, respiratory muscle function parameters improved and the effect has remained even 6 months after the end of training. RMT is not effective in patients with FVC lower than 25% predicted and/or PaCO2 higher than 45 mmHg. It seems that RMT is not applicable in the most compromised patients, maybe because they do not have enough functional muscle mass left or because their respiratory muscles are so impaired and thus more susceptible to damage.Citation110
IMT is strongly recommended preoperatively in case of spinal surgery in order to prevent pulmonary complication secondary to anesthesia.Citation111 IMT improves the functionality of respiratory muscles by increasing FVC to 26.2% before surgery and by reducing postoperative risks.Citation112
RMT can be simply implemented within video games with the possibility to control all the training processes. Improvements in respiratory performance correlate positively with the actual amount of training and negatively with baseline lung function test. This implies that RMT seems to be more effective in DMD patients who have moderate respiratory impairment.Citation113
The main limitations of these studies are the reduced number of patients and the lack of standardized protocols. RMT therapeutic effects rely on two factors: the amount of training and the relatively good condition of the patient.Citation13
LVR, also known as “breath stacking”, is a method to inflate and recruit the lung. It consists of an inspiratory pressure applied to the airways, the hold of the delivered volume of air by glottic closure, followed by a spontaneous or assisted forced expiratory maneuver. In DMD patients, the progressive impairment of the ventilatory pump reduces the range of motion of the chest wall and therefore the ribcage becomes stiff with reduced compliance of the chest wall and of the lung. The main consequence is the formation of areas of atelectasis. These lead to reduced oxygenation of the blood and to impaired CO2 elimination due to the imbalance between alveolar ventilation and blood perfusion of the capillary. LVR helps to prevent atelectasis, to limit contractures of the thoracic muscles, to maintain the motion of the chest wall particularly of the costovertebral joints, and to improve lung compliance. It can be used also in uncooperative and in very weak patients who cannot hold a mouthpiece and therefore it is applicable to DMD patients.Citation114,Citation115 LVR has been shown to slow the rate of decline of pulmonary function compared to the decline before the start. The values of FVC and peak cough flow improve after LVR.Citation114,Citation116 Because LVR can reach higher pressure compared to in-exsufflator, great care should be taken to avoid barotrauma.Citation114 Failure to successfully stack the breath may occur in very sick patients whose VT is lower than the dead space of the mask and whose inspiratory effort is not enough to trigger the valve. In such a case, it is recommendable to use a supported breath stacking device in which a resuscitator bag helps to augment VT and to open the valve.Citation115
Glossopharyngeal breathing (GPB) represents an autonomous lung-inflation maneuver that these patients should be taught, practiced and encouraged particularly in the last stage of the disease. GPB has been proven to increase lung volume by inflating one gulp at a time and to delay the onset of daytime ventilator use. It can be performed in the event of ventilator failure and during the inspiratory cough phase, since cough flow correlates with pre-cough volume.Citation116
Recently, a 10-month program of yoga breathing exercises has been shown to ameliorate the pulmonary function in DMD patients in terms of significant improvement of FVC and FEV1.Citation117
Finally, very severe DMD patients use a spontaneous movement called the “row-a-boat phenomenon”, ie, swing of the torso back and front rhythmically synchronized with fR, to compensate for the atrophied respiratory muscles. By simply allowing the row-a-boat movement, FVC increases up to 50.8% compared to the values reached when the movement is prevented.Citation118
Management of scoliosis and spinal fusion
In the natural history of DMD, the development of scoliosis is a frequent complication that impacts on respiratory function, seating, and comfort. Ninety percent of untreated DMD boys develop scoliosis, secondary to muscle weakness, pelvic imbalance,Citation119 and after becoming wheelchair bound full-time.Citation120 For this reason, prolonging ambulation in DMD patients is one of the main strategies to delay the onset of scoliosis.Citation121 Other strategies include physiotherapy (passive stretching) to maintain lower limb range of motion, night splints or serial casting.Citation3,Citation122 Moreover, surgery can release contractures of lower limbs and then rehabilitation with “KAFO” (knee ankle foot orthoses) may prolong standing and walking for 2 years.Citation3,Citation119,Citation122–Citation125 There is level III-2 evidence that the use of corticosteroids delays the onset of scoliosis by extending independent ambulation. Steroid therapy has been shown to reduce the need for surgical treatment to reduce scoliosis in DMD from 90% to 15%.Citation88,Citation100,Citation119,Citation126,Citation127 Long-term corticosteroid treatment, however, carries important side effects including worsened bone fragility and the risk of vertebral fractures.
When the scoliosis curvature exceeds the 40° of Cobb angle, scoliosis rapidly progresses and may impair breathing by reducing lung capacity on both the convex and the concave sides.Citation128 Since spinal orthoses seem to have minimal effects on preventing, delaying or minimally correcting the curve progression, surgical correction becomes the indication.Citation129 Because of the cardiopulmonary impairment of DMD, spinal surgery is better when performed during early adolescence in order to avoid the high risk of developing postoperative pneumonia, prolonging ventilatory dependence, cardiac failure, and eventually death.Citation130 In the literature, there are conflicting reports about the effect of surgical spine stabilization on pulmonary function. They all consider the evolution of FVC. There are studies reporting positive effects of spinal fusion in terms of stabilization of FVCCitation131,Citation132 or slightly slowing FVC deterioration with respect to a control non-operative group or to pre-operative patients.Citation128,Citation133–Citation135 It should be noted that in these papers there was a continuous reduction in FVC after surgery, although to a lesser extent. Other studies have found no ameliorative effects on the decline of pulmonary function.Citation83,Citation136–Citation141
The decision to have surgical fixation of the spine therefore has to be considered mainly to improve the general well-being of the patient (maintenance of comfortable sitting balance, release of pain due to muscle contractures, and improvement of quality of life) rather than to improve his respiratory function which will continue to decline anyway. Nevertheless, in DMD patients the combination of spinal fusion with nocturnal ventilation prolongs median survival to 30 years.Citation141
Cough assisted devices
The main causes that require intubation for DMD patients are episodes of pneumonia and acute respiratory failure secondary to benign upper-respiratory infection. This is a consequence of retained secretion due to inability to cough effectively.Citation142 In DMD, cough is considered adequate when CPF >270 L/min and ineffective if CPF <160 L/min and therefore cough augmentation is required. When CPF is between 160 and 270 L/min cough is considered effective when the patient is in good and stable condition, but it becomes inadequate in case of viral illness when secretions increase.Citation111,Citation143,Citation144 Once assisted coughing is recommended, it should be used not only when the patient is ill, but once or twice-per-day as maintenance therapy to improve airway clearance and reduce atelectasis. Since CPF strongly depends on the volume of air inspired pre-coughing,Citation56 the first goal of cough assisted techniques is to maximally inflate the lungs. This can be achieved autonomously by GPB, manually through the use of an inflating Ambu bag or mechanically assisted. The expulsive cough phase can be spontaneous, when the patient is still able to generate sufficient intrathoracic pressures, manually assisted by abdominal compression or mechanically forced by a cough assisted device. The combination of inspiratory volume support with manual assisted expiratory cough phase is more efficacious than the single intervention per se.Citation145,Citation146 The use of mechanical in-exsufflator is effective in preventing pulmonary complications like pneumonia and respiratory failure and in decreasing the number of hospitalizations due to respiratory illness.Citation4 The addition of intrapulmonary percussive ventilation to assist mucus clearance techniques is a safe method to augment the efficacy of these methods to keep the airways of tracheotomized DMD patients clear.Citation147 Care must be taken to adequately pre-set the timing and the levels of pressure in order to be well tolerated by the patient, to maximize cough effectiveness, and to avoid possible complications like pneumothorax, gastroesophageal reflux, and pulmonary hemorrhage.
CPF correlates with MIP and MEPCitation97,Citation146 and all the three parameters improve after long-term steroid therapy. Therefore the steroid-induced preservation of both inspiratory and expiratory muscle strength translates to better cough efficiency.Citation97
The combination of cough assisted devices with NIV before surgery helps in easy extubation after surgery without postoperative respiratory complications.Citation148
NIV
The onset or chronic respiratory insufficiency is a fatal inevitable complication of DMD. Patients not treated with mechanical ventilation die by the end of the second decade of life.Citation7,Citation37,Citation75,Citation77 The use of NIV combined with adequate airway clearance prolongs survival up to the third decade of life in DMD patients.Citation7,Citation9,Citation10,Citation77 In these patients, nocturnal NIV helps to reduce the fatigue of respiratory muscles by lowering TTI. As a result dyspnea reduces, as indicated by lower Borg scale values. After nocturnal NIV, vital capacity slightly increases while MIP does not change. Two additional hours of diurnal NIV improves the respiratory condition of severe DMD patients who present with nocturnal hypoventilation symptoms like breathlessness in the evening. In these patients, the benefits of nocturnal NIV last 6 hours. The same levels of lower TTI and reduced dyspnea are restored and maintained after the 2 additional hours of diurnal NIV that represents a good tool to reduce the load on the respiratory muscles rising from morning to evening.Citation37 This is an important therapeutic intervention for DMD patients who are dyspneic during diurnal unassisted breathing.
Moreover, intermittent positive-pressure breathing (IPPB) shows positive effects on regional lung ventilation. A session of 30 consecutive breaths up to 30 cm H2O performed in different positions (supine, left and right lateral position) increases the regional ventilation of the lungs. Such increment is maintained also 3 hours after the end of IPPB if the patient wears an abdominal belt. The supine position is characterized by the greatest improvement in lung ventilation particularly in the anterior regions. In order to reduce risks of hyperinflation in only one part of the lung, it is recommended to use several positions for the IPPB protocol.Citation149
With the progression of the clinical course of the disease, DMD patients develop respiratory failure characterized by daytime hypercapnia, hypoxia, and impairment in swallowing. The traditional approach to deal with this last stage of the disease would be to introduce tracheostomy ventilation.Citation150 Twenty-four hours’ NIV represents a safe and non-invasive alternative to tracheostomy.Citation9,Citation143,Citation151 The advantage of 24-hour NIV compared to invasive ventilation is the possibility to engage normal verbal communication, to eat, to breath-stack as desired, and to avoid the clinical complications of tracheotomized patients. Dysphagia also benefits from 24 hours of NIV maybe because oropharyngeal muscles improve their strength and endurance associated with the reduced work of breathing. The swallowing mechanism may improve and therefore it can support better nutrition.Citation152
Tracheostomy ventilation becomes necessary in case of severe aspiration risk, severe respiratory infection, and after onset of severe bulbar weakness that is rarely developed in patients with DMD. The combined use of NIV and mechanically assisted cough allows the decannulation and extubation even for unweanable DMD patients.Citation9,Citation153
Animal studies
DMD animal models, both mice and canine, are important reliable models for a physiological study of the disease and/or to test new pharmacological treatment efficacy, particularly for the diaphragm, the most important respiratory muscle. Exposure to episodic hypoxia mocks the sleep disorder breathing of DMD patients and it results in a 30% reduction in diaphragmatic strength in mdx mice.Citation154 Fourteen weeks’ treatment with phosphodiesterase 5 inhibitors reduced the dysfunction of the diaphragm in mdx mice by enhancing the contractility of the diaphragm, by slowing muscle fibrosis, and by normalizing the expression of pro-inflammatory cytokine.Citation155 Improvement in diaphragmatic health, in terms of muscle mass normalization and reduced fiber necrosis, can be obtained in neonatal mdx mice with the combination of antisense therapy with dystrophin restoration and myostatin inhibition.Citation156 Reduction of the oxidative damage and of the inflammatory response in the mdx mouse diaphragm can be achieved using deferoxamine, a potent iron chelating agent.Citation157 It is very important to restore diaphragmatic function not only from a respiratory point of view but also since the rescue of the diaphragm in mdx mice, by increasing its UTRN or dystrophin expression, prevented heart dysfunction. The decline in lung function secondary to respiratory muscles’ impairment increases pulmonary vascular pressure therefore leading to pulmonary hypertension.Citation158 In DMD patients, pulmonary hypertension increases right atrial pressure with possible right ventricular failure.Citation159 An early component of the hypercapnic ventilatory reflex has been revealed in mdx mice, demonstrating a malfunction in the peripheral chemosensory drive. This is supposed to be a further contributor to the respiratory failure in mdx mice. Therefore the monitoring of peripheral chemosensory drive function may be useful to better manage DMD patients with respiratory failure.Citation160 The DMD mdx mouse model with haploinsufficiency of the UTRN gene is characterized by more severe diaphragmatic fibrosis and may improve when testing antifibrotic therapies, especially in the most severe stage.Citation161
Golden Retriever muscular dystrophy (GRMD) is a canine model of DMD. GRMD dogs guarantee an adequate level of ventilation at rest by increasing their respiratory rate in order to compensate for a lower VT compared to normal dogs. GRMD does not show abdominal paradox. When the respiratory drive is stimulated by doxapram, abdominal expiratory muscles are recruited early to compensate for the loss of diaphragmatic function. The diaphragm in GRMD is weaker, shorter, thicker, and severely fibrotic compared to the other respiratory and locomotor muscles.Citation162
Conclusion
Until now clinical trials have not considered respiratory function variables as primary outcomes. This, however, would be highly recommended, as respiratory problems are among the main causes of death in DMD patients. The non-invasive and non-volitional methods and techniques for respiratory functional assessment which are nowadays available should be considered as a tool not only for experimental trials, but also for clinical monitoring starting during the very early stages of the disease.
Disclosure
The authors have no conflict of interest to declare.
References
- EmeryAEPopulation frequencies of inherited neuromuscular diseases – a world surveyNeuromuscul Disord19911119291822774
- GriggsRCBushbyKContinued need for caution in the diagnosis of Duchenne muscular dystrophyNeurology20056491498149915883307
- BushbyKFinkelRBirnkrantDJDiagnosis and management of Duchenne muscular dystrophy, part 1: diagnosis, and pharmacological and psychosocial managementLancet Neurol201091779319945913
- Gomez-MerinoEBachJRDuchenne muscular dystrophy: prolongation of life by noninvasive ventilation and mechanically assisted coughingAm J Phys Med Rehabil200281641141512023596
- EagleMBaudouinSVChandlerCGiddingsDRBullockRBushbyKSurvival in Duchenne muscular dystrophy: improvements in life expectancy since 1967 and the impact of home nocturnal ventilationNeuromuscul Disord2002121092692912467747
- SaitoTTataraKDatabase of Wards for Patients with Muscular Dystrophy in Japan2012 Available from: http://cdn.intechopen.com/pdfs/36737/InTech-Database_of_wards_for_patients_with_muscular_dystrophy_in_japan.pdfAccessed July 16, 2015
- PassamanoLTagliaAPalladinoAImprovement of survival in Duchenne Muscular Dystrophy: Retrospective analysis of 835 patientsActa Myol201231212112523097603
- FinderJDBirnkrantDCarlJRespiratory care of the patient with Duchenne muscular dystrophy: ATS consensus statementAm J Respir Crit Care Med2004170445646515302625
- BachJRMartinezDDuchenne muscular dystrophy: continuous noninvasive ventilatory support prolongs survivalRespir Care201156674475021333078
- IshikawaYMiuraTIshikawaYDuchenne muscular dystrophy: survival by cardio-respiratory interventionsNeuromuscul Disord2011211475121144751
- BirnkrantDJBushbyKMAminRSThe respiratory management of patients with Duchenne muscular dystrophy: A DMD care considerations working group specialty articlePediatr Pulmonol201045873974820597083
- BushbyKFinkelRBirnkrantDJDiagnosis and management of Duchenne muscular dystrophy, part 2: implementation of multidisciplinary careLancet Neurol20109217718919945914
- FinstererJCardiopulmonary support in Duchenne muscular dystrophyLung2006184420521517006747
- WagnerKRLechtzinNJudgeDPCurrent treatment of adult Duchenne muscular dystrophyBiochim Biophys Acta20071772222923716887341
- McDonaldCMHenricsonEKAbreschRTThe cooperative international neuromuscular research group Duchenne natural history study – a longitudinal investigation in the era of glucocorticoid therapy: design of protocol and the methods usedMuscle Nerve2013481325423677550
- HenricsonEKAbreschRTCnaanAThe cooperative international neuromuscular research group Duchenne natural history study: glucocorticoid treatment preserves clinically meaningful functional milestones and reduces rate of disease progression as measured by manual muscle testing and otheMuscle Nerve2013481556723649481
- MalikVRodino-KlapacLRMendellJREmerging drugs for Duchenne muscular dystrophyExpert Opin Emerg Drugs201217226127722632414
- Beytía MdeLVryJKirschnerJDrug treatment of Duchenne muscular dystrophy: available evidence and perspectivesActa Myol20123114822655510
- American Thoracic Society/European Respiratory SocietyATS/ERS Statement on respiratory muscle testingAm J Respir Crit Care Med2002166451862412186831
- DuivermanMLvan EykernLAVennikPWKoëterGHMaarsinghEJWijkstraPJReproducibility and responsiveness of a noninvasive EMG technique of the respiratory muscles in COPD patients and in healthy subjectsJ Appl Physiol (1985)20049651723172914660508
- BeckJSinderbyCWeinbergJGrassinoAEffects of muscle-to-electrode distance on the human diaphragm electromyogramJ Appl Physiol (1985)19957939759858567542
- WohlgemuthMvan der KooiELHendriksJCPadbergGWFolgeringHTFace mask spirometry and respiratory pressures in normal subjectsEur Respir J20032261001100614680093
- TobinMJPerezWGuentherSMThe pattern of breathing during successful and unsuccessful trials of weaning from mechanical ventilationAm Rev Respir Dis19861346111111183789513
- MeadJPetersonNGrimbyGMeadJPulmonary ventilation measured from body surface movementsScience19671563780138313844886899
- ChadhaTSWatsonHBirchSValidation of respiratory inductive plethysmography using different calibration proceduresAm Rev Respir Dis198212566446497091869
- CalaSJKenyonCMFerrignoGChest wall and lung volume estimation by optical reflectance motion analysisJ Appl Physiol (1985)1996816268026899018522
- AlivertiADellacàRPelosiPChiumelloDGatihnoniLPedotiACompartmental analysis of breathing in the supine and prone positions by optoelectronic plethysmographyAnn Biomed Eng2001291607011219508
- RomeiMLoMauro AD’AngeloMGEffects of gender and posture on thoraco-abdominal kinematics during quiet breathing in healthy adultsRespir Physiol Neurobiol2010172318419120510388
- BoudarhamJPradonDPrigentHOptoelectronic plethysmography as an alternative method for the diagnosis of unilateral diaphragmatic weaknessChest2013144388789523519378
- CluzelPSimilowskiTChartrand-LefebvreCZelterMDerenneJPGrenierPADiaphragm and chest wall: assessment of the inspiratory pump with MR imaging-preliminary observationsRadiology2000215257458310796942
- GauthierAPVerbanckSEstenneMSegebarthCMacklemPTPaivaMThree-dimensional reconstruction of the in vivo human diaphragm shape at different lung volumesJ Appl Physiol (1985)19947624955068175555
- UekiJDe BruinPFPrideNBIn vivo assessment of diaphragm contraction by ultrasound in normal subjectsThorax19955011115711618553271
- TestaASoldatiGGiannuzziRUltrasound M-mode assessment of diaphragmatic kinetics by anterior transverse scanning in healthy subjectsUltrasound Med Biol2011371445221144957
- EvansJAWhitelawWAThe assessment of maximal respiratory mouth pressures in adultsRespir Care200954101348135919796415
- StefanuttiDFittingJWSniff nasal inspiratory pressure. Reference values in Caucasian childrenAm J Respir Crit Care Med199915911071119872826
- FaurouxBAubertinGCohenEClémentALofasoFSniff nasal inspiratory pressure in children with muscular, chest wall or lung diseaseEur Respir J200933111311718799509
- ToussaintMSoudonPKinnearWEffect of non-invasive ventilation on respiratory muscle loading and endurance in patients with Duchenne muscular dystrophyThorax200863543043418057095
- HayotMRamonatxoMMateckiSMilic-EmiliJPrefautCNoninvasive assessment of inspiratory muscle function during exerciseAm J Respir Crit Care Med200016262201220711112138
- HussainSNPardyRLInspiratory muscle function with restrictive chest wall loading during exercise in normal humansJ Appl Physiol (1985)1985586202720323159717
- MulreanyLTWeinerDJMcDonoughJMPanitchHBAllenJLNoninvasive measurement of the tension-time index in children with neuromuscular diseaseJ Appl Physiol (1985)200395393193712909595
- BianchiCBaiardiPCough peak flows: standard values for children and adolescentsAm J Phys Med Rehabil200887646146718496248
- FromageotCLofasoFAnnaneDSupine fall in lung volumes in the assessment of diaphragmatic weakness in neuromuscular disordersArch Phys Med Rehabil200182112312811239298
- MillerMRCrapoRHankinsonJGeneral considerations for lung function testingEur Respir J200526115316115994402
- MillerMRHankinsonJBrusascoVStandardisation of spirometryEur Respir J200526231933816055882
- WangerJClausenJLCoatesAStandardisation of the measurement of lung volumesEur Respir J200526351152216135736
- PellegrinoRViegiGBrusascoVInterpretative strategies for lung function testsEur Respir J200526594896816264058
- HillmanDRFinucaneKERespiratory pressure partitioning during quiet inspiration in unilateral and bilateral diaphragmatic weaknessAm Rev Respir Dis19881376140114053202378
- GilbertRAuchinclossJHPeppiDRelationship of rib cage and abdomen motion to diaphragm function during quiet breathingChest19818056076127297153
- MillsGHKyroussisDHamnegardCHPolkeyMIGreenMMoxhamJBilateral magnetic stimulation of the phrenic nerves from an anterolateral approachAm J Respir Crit Care Med19961544 Pt 1109911058887614
- PettiauxNCassartMPaivaMEstenneMThree-dimensional reconstruction of human diaphragm with the use of spiral computed tomographyJ Appl Physiol (1985)199782399810029074993
- NicotFHartNForinVRespiratory muscle testing: a valuable tool for children with neuromuscular disordersAm J Respir Crit Care Med20061741677416574932
- FaurouxBQuijano-RoySDesguerreIKhiraniSThe value of respiratory muscle testing in children with neuromuscular diseaseChest2015147255255925644908
- HéritierFRahmFPaschePFittingJWSniff nasal inspiratory pressure. A noninvasive assessment of inspiratory muscle strengthAm J Respir Crit Care Med19941506 Pt 1167816837952632
- LarocheCMMierAKMoxhamJGreenMThe value of sniff esophageal pressures in the assessment of global inspiratory muscle strengthAm Rev Respir Dis198813835986033202414
- ManWDKyroussisDFlemingTACough gastric pressure and maximum expiratory mouth pressure in humansAm J Respir Crit Care Med2003168671471712857722
- SmithJAAlivertiAQuarantaMChest wall dynamics during voluntary and induced cough in healthy volunteersJ Physiol2012590Pt 356357422144580
- Lo MauroAD’AngeloMGRomeiMAbdominal volume contribution to tidal volume as an early indicator of respiratory impairment in Duchenne muscular dystrophyEur Respir J20103551118112519840972
- StehlingFDohna-SchwakeCMelliesUGrosse-OnnebrinkJDecline in Lung Volume With Duchenne Muscular Dystrophy Is Associated With Ventilation InhomogeneityRespir Care Epub201555
- KhiraniSRamirezAAubertinGRespiratory muscle decline in Duchenne muscular dystrophyPediatr Pulmonol201449547348123836708
- RomeiMD’AngeloMGLoMauroALow abdominal contribution to breathing as daytime predictor of nocturnal desaturation in adolescents and young adults with Duchenne Muscular DystrophyRespir Med2012106227628322083092
- LomauroARomeiMD’AngeloMGAlivertiADeterminants of cough efficiency in Duchenne muscular dystrophyPediatr Pulmonol201449435736523852963
- JansenMvan AlfenNNijhuis van der SandenMWvan DijkJPPillenSde GrootIJQuantitative muscle ultrasound is a promising longitudinal follow-up tool in Duchenne muscular dystrophyNeuromuscul Disord201222430631722133654
- De BruinPFUekiJBushAKhanYWatsonAPrideNBDiaphragm thickness and inspiratory strength in patients with Duchenne muscular dystrophyThorax19975254724759176541
- WangJFanZVandenborneKA computerized MRI biomarker quantification scheme for a canine model of Duchenne muscular dystrophyInt J Comput Assist Radiol Surg20138576377423299128
- HollingsworthKGGarroodPEagleMBushbyKStraubVMagnetic resonance imaging in Duchenne muscular dystrophy: longitudinal assessment of natural history over 18 monthsMuscle Nerve201348458658823620230
- SenesacCRLottDJForbesSCLongitudinal Evaluation of Muscle Composition Using Magnetic Resonance in 4 Boys With Duchenne Muscular Dystrophy: Case SeriesPhys Ther201595797898825592189
- WillcocksRJArpanIAForbesSCLongitudinal measurements of MRI-T2 in boys with Duchenne muscular dystrophy: effects of age and disease progressionNeuromuscul Disord201424539340124491484
- MavrogeniSTzelepisGEAthanasopoulosGCardiac and sternocleidomastoid muscle involvement in Duchenne muscular dystrophy: an MRI studyChest2005127114314815653975
- PhillipsMFQuinlivanRCEdwardsRHCalverleyPMChanges in spirometry over time as a prognostic marker in patients with duchenne muscular dystrophyAm J Respir Crit Care Med2002164122191219411751186
- HahnABachJRDelaubierARenardel-IraniAGuillouCRideauYClinical implications of maximal respiratory pressure determinations for individuals with Duchenne muscular dystrophyArch Phys Med Rehabil1997781169014949
- NèveVCuissetJMEdméJLSniff nasal inspiratory pressure in the longitudinal assessment of young Duchenne muscular dystrophy childrenEur Respir J201342367168023258781
- GayraudJRamonatxoMRivierFHumberclaudeVPetrofBMateckiSVentilatory parameters and maximal respiratory pressure changes with age in Duchenne muscular dystrophy patientsPediatr Pulmonol201045655255920503279
- TangsrudSPetersenILLødrup CarlsenKCCarlsenKHLung function in children with Duchenne’s muscular dystrophyRespir Med2001951189890311716204
- HumbertclaudeVHamrounDBezzouKMotor and respiratory heterogeneity in Duchenne patients: implication for clinical trialsEur J Paediatr Neurol201216214916021920787
- RideauYJankowskiLWGrelletJRespiratory function in the muscular dystrophiesMuscle Nerve1981421551647207506
- GauldLMBoyntonARelationship between peak cough flow and spirometry in Duchenne muscular dystrophyPediatr Pulmonol200539545746015765540
- ToussaintMChatwinMSoudonPMechanical ventilation in Duchenne patients with chronic respiratory insufficiency: clinical implications of 20 years published experienceChron Respir Dis20074316717717711917
- PhillipsMFSmithPECarrollNEdwardsRHCalverleyPMNocturnal oxygenation and prognosis in Duchenne muscular dystrophyAm J Respir Crit Care Med1999160119820210390400
- WonYHChoiWAKimDHKangSWPostural Vital Capacity Difference with Aging in Duchenne Muscular DystrophyMuscle Nerve Epub2015227
- MayerOHFinkelRSRummeyCCharacterization of pulmonary function in Duchenne Muscular DystrophyPediatr Pulmonol201550548749425755201
- McDonaldCMAbreschRTCarterGTProfiles of neuromuscular diseases. Duchenne muscular dystrophyAm J Phys Med Rehabil1995745 SupplS70S927576424
- SteffensenBFLyagerSWergeBRahbekJMattssonEPhysical capacity in non-ambulatory people with Duchenne muscular dystrophy or spinal muscular atrophy: a longitudinal studyDev Med Child Neurol200244962363212227617
- RobertoRFritzAHagarYThe natural history of cardiac and pulmonary function decline in patients with duchenne muscular dystrophySpine (Phila Pa 1976)20113615E1009E101721289561
- De BruinPFUekiJBushAY ManzurAWatsonAPrideNBInspiratory flow reserve in boys with Duchenne muscular dystrophyPediatr Pulmonol200131645145711389578
- BoitanoLJManagement of airway clearance in neuromuscular diseaseRespir Care200651891392216867201
- PanitchHBRespiratory issues in the management of children with neuromuscular diseaseRespir Care200651888589316867199
- MateckiSTopinNHayotMA standardized method for the evaluation of respiratory muscle endurance in patients with Duchenne muscular dystrophyNeuromuscul Disord200111217117711257474
- BushbyKMuntoniFUrtizbereaAHughesRGriggsRReport on the 124th ENMC International Workshop. Treatment of Duchenne muscular dystrophy; defining the gold standards of management in the use of corticosteroids. 2–4 April 2004, Naarden, The NetherlandsNeuromuscul Disord2004148–952653415336694
- YilmazOKaradumanATopaloğluHPrednisolone therapy in Duchenne muscular dystrophy prolongs ambulation and prevents scoliosisEur J Neurol200411854154415272899
- MendellJRMoxleyRTGriggsRCRandomized, double-blind six-month trial of prednisone in Duchenne’s muscular dystrophyN Engl J Med198932024159215972657428
- FenichelGMFlorenceJMPestronkALong-term benefit from prednisone therapy in Duchenne muscular dystrophyNeurology19914112187418771745340
- FenichelGMMendellJRMoxleyRTA comparison of daily and alternate-day prednisone therapy in the treatment of Duchenne muscular dystrophyArch Neurol19914865755792039377
- GriggsRCMoxleyRT3rdMendellJRPrednisone in Duchenne dystrophy. A randomized, controlled trial defining the time course and dose response. Clinical Investigation of Duchenne Dystrophy GroupArch Neurol19914843833882012511
- ConnollyAMSchierbeckerJRennaRFlorenceJHigh dose weekly oral prednisone improves strength in boys with Duchenne muscular dystrophyNeuromuscul Disord2002121091792512467746
- EscolarDMHacheLPClemensPRRandomized, blinded trial of weekend vs daily prednisone in Duchenne muscular dystrophyNeurology201177544445221753160
- MachadoDLSilvaECResendeMBCarvalhoCRZanoteliEReedUCLung function monitoring in patients with duchenne muscular dystrophy on steroid therapyBMC Res Notes20125143522889007
- DaftaryASCrisantiMKalraMWongBAminREffect of long-term steroids on cough efficiency and respiratory muscle strength in patients with Duchenne muscular dystrophyPediatrics20071192e320e32417272595
- BuyseGMGoemansNVan Den HauweMMeierTEffects of glucocorticoids and idebenone on respiratory function in patients with duchenne muscular dystrophyPediatr Pulmonol201348991292023129412
- BiggarWDGingrasMFehlingsDLHarrisVASteeleCADeflazacort treatment of Duchenne muscular dystrophyJ Pediatr20011381455011148511
- BiggarWDHarrisVAEliasophLAlmanBLong-term benefits of deflazacort treatment for boys with Duchenne muscular dystrophy in their second decadeNeuromuscul Disord200616424925516545568
- BuyseGMVan der MierenGErbMLong-term blinded placebo-controlled study of SNT-MC17/idebenone in the dystrophin deficient mdx mouse: cardiac protection and improved exercise performanceEur Heart J200930111612418784063
- BuyseGMVoitTScharaUEfficacy of idebenone on respiratory function in patients with Duchenne muscular dystrophy not using glucocorticoids (DELOS): a double-blind randomised placebo-controlled phase 3 trialLancet20153851748175725907158
- WiltonSDVeeduRNFletcherSThe emperor’s new dystrophin: finding sense in the noiseTrends Mol Med201521741742626051381
- BushbyKFinkelRWongBAtaluren treatment of patients with nonsense mutation dystrophinopathyMuscle Nerve201450447748725042182
- Muscular Dystrophy UK [homepage on the Internet]Find a clinical trial Available from: http://www.musculardystrophyuk.org/progress-in-research/patient-registries-and-clinical-trials/clinical-trials/find-a-clinical-trial/page/2/?mdcore_clinicaltrial_region_tag=-1&mdcore_clinicaltrial_condition=duchenne-muscular-dystrophyAccessed July 20, 2015
- ClinicalTrials.govDuchenne search results Available from: https://clinicaltrials.gov/ct2/results?term=duchenne&pg=5Accessed July 20, 2015
- GozalDThirietPRespiratory muscle training in neuromuscular disease: long-term effects on strength and load perceptionMed Sci Sports Exerc199931111522152710589852
- TopinNMateckiSLe BrisSDose-dependent effect of individualized respiratory muscle training in children with Duchenne muscular dystrophyNeuromuscul Disord200212657658312117483
- WinklerGZifkoUNaderADose-dependent effects of inspiratory muscle training in neuromuscular disordersMuscle Nerve20002381257126010918264
- WankeTToiflKMerkleMFormanekDLahrmannHZwickHInspiratory muscle training in patients with Duchenne muscular dystrophyChest199410524754828306750
- BirnkrantDJPanitchHBBendittJOAmerican College of Chest Physicians consensus statement on the respiratory and related management of patients with Duchenne muscular dystrophy undergoing anesthesia or sedationChest200713261977198618079231
- TakasoMNakazawaTOkadaTSurgical management of severe scoliosis with high risk pulmonary dysfunction in Duchenne muscular dystrophy: Patient function, quality of life and satisfactionInt Orthop201034569570220155495
- VilozniDBar-YishayEGurIShapiraYMeyerSGodfreySComputerized Respiratory Muscle Training in Children with Duchenne Muscular DystrophyNeuromuscul Disord1994432492557919973
- McKimDAKatzSLBarrowmanNNiALeBlancCLung volume recruitment slows pulmonary function decline in duchenne muscular dystrophyArch Phys Med Rehabil20129371117112222421625
- JenkinsHMStockiAKriellaarsDPasterkampHBreath stacking in children with neuromuscular disordersPediatr Pulmonol201449654455323956183
- BachJRBianchiCVidigal-LopesMTuriSFelisariGLung inflation by glossopharyngeal breathing and “air stacking” in Duchenne muscular dystrophyAm J Phys Med Rehabil200786429530017413542
- RodriguesMRCarvalhoCRSantaellaDFLorenzi-FilhoGMarieSKEffects of yoga breathing exercises on pulmonary function in patients with Duchenne muscular dystrophy: an exploratory analysisJ Bras Pneumol201440212813324831396
- YasumaFKatoTMatsuokaYKonagayaMRow-a-boat phenomenon: Respiratory compensation in advanced Duchenne muscular dystrophyChest200111961836183911399712
- HsuJDQuinlivanRScoliosis in Duchenne muscular dystrophy (DMD)Neuromuscul Disord201323861161723746543
- ShapiroFZurakowskiDBuiTDarrasBTProgression of spinal deformity in wheelchair-dependent patients with Duchenne muscular dystrophy who are not treated with steroids: coronal plane (scoliosis) and sagittal plane (kyphosis, lordosis) deformityBone Joint J201496–B1100105
- HsuJDThe development of current approaches to the management of spinal deformity for patients with neuromuscular diseaseSemin Neurol199515124287638454
- ScottOMHydeSAGoddardCDubowitzVPrevention of deformity in Duchenne muscular dystrophy. A prospective study of passive stretching and splintagePhysiotherapy19816761771807301976
- KinaliMMainMEliahooJPredictive factors for the development of scoliosis in Duchenne muscular dystrophyEur J Paediatr Neurol200711316016617257866
- HydeSAScottOMGoddardCMDubowitzVProlongation of ambulation in Duchenne muscular dystrophy by appropriate orthosesPhysiotherapy19826841051087111464
- RodilloEBFernandez-BermejoEHeckmattJZDubowitzVPrevention of rapidly progressive scoliosis in Duchenne muscular dystrophy by prolongation of walking with orthosesJ Child Neurol1988342692743198893
- LebelDECorstonJAMcAdamLCBiggarWDAlmanBAGlucocorticoid treatment for the prevention of scoliosis in children with Duchenne muscular dystrophy: long-term follow-upJ Bone Joint Surg Am201395121057106123783200
- ManzurAYKuntzerTPikeMSwanAGlucocorticoid corticosteroids for Duchenne muscular dystrophyCochrane Database Syst Rev20081CD00372518254031
- KurzLTMubarakSJSchultzPParkSMLeachJCorrelation of scoliosis and pulmonary function in Duchenne muscular dystrophyJ Pediatr Orthop1983333473536874933
- HarveyABakerLWilliamsKNon-surgical prevention and management of scoliosis for children with Duchenne muscular dystrophy: what is the evidence?J Paediatr Child Health20145010E3E923560735
- DuckworthADMitchellMJTsirikosAIIncidence and risk factors for post-operative complications after scoliosis surgery in patients with Duchenne muscular dystrophy : a comparison with other neuromuscular conditionsBone Joint J201496–B7943949
- VelascoMVColinAAZurakowskiDDarrasBTShapiroFPosterior spinal fusion for scoliosis in duchenne muscular dystrophy diminishes the rate of respiratory declineSpine (Phila Pa 1976)200732445946517304138
- GalaskoCSDelaneyCMorrisPSpinal stabilisation in Duchenne muscular dystrophyJ Bone Joint Surg Br19927422102141544954
- TakasoMNakazawaTImuraTSurgical management of severe scoliosis with high-risk pulmonary dysfunction in Duchenne muscular dystrophyInt Orthop201034340140619340426
- CervellatiSBettiniNMoscatoMGusellaADemaEMaresiRSurgical treatment of spinal deformities in Duchenne muscular dystrophy: a long term follow-up studyEur Spine J200413544144815108098
- GalaskoCSWilliamsonJBDelaneyCMLung function in Duchenne muscular dystrophyEur Spine J1995452632678581525
- AlexanderWMSmithMFreemanBJCSutherlandLMKennedyJDCundyPJThe effect of posterior spinal fusion on respiratory function in Duchenne muscular dystrophyEur Spine J201322241141623179984
- JenkinsJGBohnDEdmondsJFLevisonHBarkerGAEvaluation of pulmonary function in muscular dystrophy patients requiring spinal surgeryCrit Care Med198210106456497116884
- KennedyJDStaplesAJBrookPDEffect of spinal surgery on lung function in Duchenne muscular dystrophyThorax19955011117311788553273
- MillerRGChalmersACDaoHFiller-KatzAHolmanDBostFThe effect of spine fusion on respiratory function in Duchenne muscular dystrophyNeurology199141138401985293
- Van OpstalNVerlindenCMynckeJGoemansNMoensPThe effect of Luque-Galveston fusion on curve, respiratory function and quality of life in Duchenne muscular dystrophyActa Orthop Belg201177565966522187843
- EagleMBourkeJBullockRManaging Duchenne muscular dystrophy – the additive effect of spinal surgery and home nocturnal ventilation in improving survivalNeuromuscul Disord200717647047517490881
- BachJRRajaramanRBallangerFNeuromuscular ventilatory insufficiency: effect of home mechanical ventilator use v oxygen therapy on pneumonia and hospitalization ratesAm J Phys Med Rehabil19987718199482374
- BachJRIshikawaYKimHPrevention of pulmonary morbidity for patients with Duchenne muscular dystrophyChest19971124102410289377912
- BachJRSaporitoLRCriteria for extubation and tracheostomy tube removal for patients with ventilatory failure. A different approach to weaningChest19961106156615718989078
- IshikawaYBachJRKomaroffEMiuraTJackson-ParekhRCough Augmentation in Duchenne Muscular DystrophyAm J Phys Med Rehabil200887972673018716484
- KangSWKangYSSohnHSParkJHMoonJHRespiratory muscle strength and cough capacity in patients with Duchenne muscular dystrophyYonsei Med J200647218419016642546
- ToussaintMDe WinHSteensMSoudonPEffect of intrapulmonary percussive ventilation on mucus clearance in duchenne muscular dystrophy patients: a preliminary reportRespir Care2003481094094714525630
- MillsBBachJRZhaoCSaporitoLSabharwalSPosterior spinal fusion in children with flaccid neuromuscular scoliosis: the role of noninvasive positive pressure ventilatory supportJ Pediatr Orthop201333548849323752144
- GuérinCVincentBPetitjeanTThe short-term effects of intermittent positive pressure breathing treatments on ventilation in patients with neuromuscular diseaseRespir Care201055786687220587098
- LofasoFOrlikowskiDRaphaelJCVentilatory assistance in patients with Duchenne muscular dystrophyEur Respir J200628346846916946091
- BachJRGonçalvesMRHonAChanging trends in the management of end-stage neuromuscular respiratory muscle failure: recommendations of an international consensusAm J Phys Med Rehabil201392326727723051760
- McKimDAGrillerNLeBlancCWoolnoughAKingJTwenty-four hour noninvasive ventilation in Duchenne muscular dystrophy: A safe alternative to tracheostomyCan Respir J2013201e5e923457679
- BachJRGonçalvesMRHamdaniIWinckJCExtubation of patients with neuromuscular weakness: a new management paradigmChest201013751033103920040608
- FarkasGAMcCormickKMGosselinLEEpisodic hypoxia exacerbates respiratory muscle dysfunction in DMD(mdx) miceMuscle Nerve200736570871017654561
- PercivalJMWhiteheadNPAdamsMEAdamoCMBeavoJAFroehnerSCSildenafil reduces respiratory muscle weakness and fibrosis in the mdx mouse model of Duchenne muscular dystrophyJ Pathol20122281778722653783
- Lu-NguyenNBJarminSASalehAFPopplewellLGaitMJDicksonGCombination antisense treatment for destructive exon skipping of myostatin and open reading frame rescue of dystrophin in neonatal mdx miceMol Ther20152381341134825959011
- MoraesLHde BurgosRRMacedoABde Almeida HermesTde FariaFMMinatelEReduction of Oxidative Damage and Inflammatory Response in the Diaphragm Muscle of mdx Mice Using Iron Chelator DeferoxamineBiol Trace Elem Res2015167111512025762099
- CrispAYinHGoyenvalleADiaphragm rescue alone prevents heart dysfunction in dystrophic mice in vitroHum Mol Genet201120341342121062902
- YotsukuraMMiyagawaMTsuyaTIshiharaTIshikawaKPulmonary hypertension in progressive muscular dystrophy of the Duchenne typeJpn Circ J19885243213263385914
- MosqueiraMBabySMLahiriSKhuranaTSVentilatory chemosensory drive is blunted in the mdx mouse model of Duchenne Muscular Dystrophy (DMD)PLoS One201387e6956723922741
- HuangPChengGLuHAronicaMRansohoffRMZhouLImpaired respiratory function in mdx and mdx/utrn(+/−) miceMuscle Nerve201143226326721254093
- MeadAFPetrovMMalikASDiaphragm Remodeling and Compensatory Respiratory Mechanics in a Canine Model of Duchenne Muscular DystrophyJ Appl Physiol (1985)2014116780781524408990