
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Background
To date, the decision to treat multilevel cervical spondylotic myelopathy (CSM) with anterior cervical discectomy and fusion (ACDF) or anterior cervical corpectomy and fusion (ACCF) remains controversial. Therefore, we conducted a meta-analysis to quantitatively determine the efficacy of ACDF and ACCF in the treatment of multilevel CSM.
Methods
We searched several databases for related research articles published in English or Chinese. We extracted and assessed the data independently. We determined the pooled data, data heterogeneity, and overall effect, respectively.
Results
We identified 15 eligible studies with 1,368 patients. We found that blood loss and numbers of complications during surgery in ACDF were significantly less that in ACCF; however, other clinical outcomes, such as operation time, bone fusion failure, post Japanese Orthopedic Association scores, recovery rates, and visual analog scale scores between ACDF and ACCF with multilevel CSM were not significantly different.
Conclusion
Our results strongly suggest that surgical treatments of multilevel CSM are similar in terms of most clinical outcomes using ACDF or ACCF.
Introduction
Cervical spondylotic myelopathy (CSM) is a common spinal disease caused by narrowing of the cervical spinal canal as a result of degenerative and congenital changes, and leads to significant neurological disability.Citation1–Citation3 Except major cause of spinal degeneration, cervical congenital malformations that result in progressive scoliosis, such as developmental stenosis, may predispose to CSM. In addition to congenital cervical spinal stenosis, spontaneous fusion of the cervical vertebrae is a further type of congenital malformation that is also a known cause of CSM.Citation4 Surgeries involving anterior and posterior approaches, including anterior cervical discectomy with fusion (ACDF),Citation5–Citation11 anterior cervical corpectomy with fusion (ACCF),Citation6–Citation8,Citation10–Citation13 laminoplasty,Citation14–Citation21 laminectomy,Citation19,Citation21–Citation25 and laminectomy with fusion (class III),Citation26–Citation30 have been developed, and the functional outcome is improved after surgical treatment for CSM.Citation31–Citation35 The surgical choice of an anterior, posterior, or combined approach for CSM should be based on the location and extent of compressive pathology, previous surgery, and the presence of preoperative neck pain, as well as the patient’s age and overall health conditions.Citation36–Citation38 Among the anterior approaches, ACCF has demonstrated relatively good fusion rates,Citation39–Citation41 but is associated with high morbidity of nonunion due to multiple graft-host interfaces,Citation42–Citation45 a higher incidence of complications including vertebral artery injury,Citation36,Citation46 dural tears, and cerebrospinal fluid leakage.Citation47 ACDF is safe and effective for managing multilevel CSM, with a low prevalence of graft extrusion or migration;Citation37,Citation48 however, ACDF may have a high risk of incomplete decompression, limited visual exposure, and injury to the cord, as well as a high rate of pseudarthrosis secondary to an increase in the number of fusion surfaces.Citation36,Citation46,Citation49 Therefore, to date, the decision to treat CSM, especially multilevel CSM, with ACDF or ACCF remains controversial.Citation50 In the present study, we conducted a meta-analysis to quantitatively determine the efficacy of ACDF and ACCF in the treatment of multilevel CSM.
Materials and methods
We performed the meta-analysis according to Preferred Reporting Items for Systematic Reviews and Meta-AnalysesCitation51 and the recommendations of the Cochrane Collaboration.Citation52
Data source and search
We searched and identified all published studies that compared the efficacy of ACDF and ACCF in the treatment of multilevel CSM. An extensive search of the literature was performed in Embase (1974 to July 2014), PubMed (1966 to July 2014) and the Cochrane Library, Biological Abstracts, Science Citation Index, Chinese BioMedical Literature Database, and China National Knowledge Infrastructure (1980 to July 2014). Medical Subject Headings were used to search in both the Chinese and English languages. We used the following keywords: cervical spondylotic myelopathy (CSM), anterior cervical discectomy and fusion (ACDF), anterior cervical corpectomy and fusion (ACCF). The full search strategy is available upon request from the corresponding authors. Relevant reviews and meta-analysis of surgeries in the treatment of CSM were also checked for inclusive studies.
Study selection
This meta-analysis included studies primarily evaluating the efficacy of ACDF and ACCF in the treatment of multilevel CSM. The bibliographies of the search results were independently reviewed by two authors (ZW and JD) to identify relevant articles that met the inclusion criteria (full text or abstract). The quality of the studies was independently assessed, and the level of agreement between them was recorded. The decision on whether to include an article was made by manual screening of titles and abstracts, followed by full-text screening by the same reviewers. If additional data or clarification were necessary, we contacted the study authors. Any disagreements between initial reviewers were resolved by discussion with another reviewer until agreement was reached.
Data extraction
The data were extracted independently by two reviewers (ZL and HX). Data for publication information (name of first author, year of publication), study information (sample size and distributions of age and sex), and the effect of ACDF and ACCF in the treatment of multilevel CSM were collected using standard data extraction forms. The preoperative and postoperative Japanese Orthopedic Association (JOA) score, operation time, blood loss, surgical complications, neurological recovery rate, reoperation rate, as well as the recovery rates and the arm pain visual analog scale (VAS) scores were checked and extracted by the other two reviewers (GL and XL). The recovery rate was determined by the following equation:
Disagreement was checked again by a third reviewer (DL). Exclusion criteria were combined surgery, non-controlled studies, follow-up less than 1 year, and CSM caused by ossification of the posterior longitudinal ligament.
Statistical analysis
All statistical analyses were performed using RevMan version 5 from the Cochrane Collaboration.
Odds ratios were calculated for binary outcomes and weighted mean differences for continuous outcomes, along with 95% confidence intervals. The pooled relative risks were combined by the Mantel–Haenszel method. The Peto method was used when there were trials with no events in one or both arms.Citation52,Citation53 Heterogeneity was evaluated using the χ2 test and I2 statistics (considered significant when the P-value for χ2 test was <0.10 or I2 was >50%). The level of significance was set at P<0.05. Fixed-effect models were applied unless statistical heterogeneity was significant, in which case random-effect models were used. We also assessed the probability of publication bias with funnel plotsCitation54 and the Egger’s test.Citation55 We investigated the influence of study design (randomized controlled trial or quasi-randomized controlled trial) and fixed levels (short or long segment fixation) on pooled estimates using subgroup analysis.
Results
Study selection and characteristics
Five hundred and eleven relevant citations were selected for initial review according to the aforementioned search strategies and provided data regarding anterior cervical discectomy and corpectomy in patients with multilevel CSM. Of these, 496 were initially excluded after reading the abstracts and/or whole articles (). Finally, the systematic literature search generated a total of 15 datasets and 1,368 patients for meta-analysis. The demographic data from studies included in the meta-analysis are shown in .
Figure 1 Flow chart of study selection.
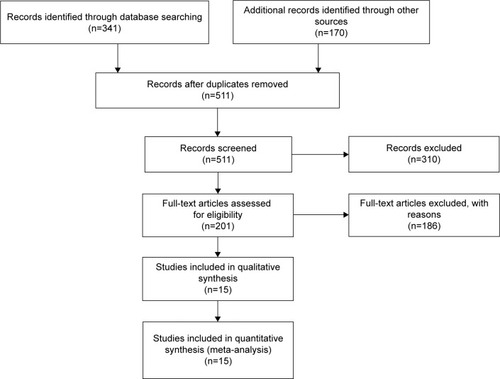
Table 1 Demographic data from studies included in meta-analysis
Methodological quality of the studies
Fifteen selected studies were evaluated to have high levels of methodological quality (more than six stars) according to the Newcastle–Ottawa quality assessment scale.Citation56
Comparison of operation time between ACDF and ACCF for CSM
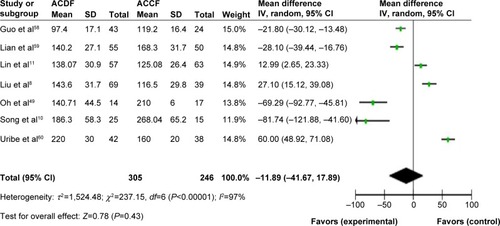
Seven studies with a total of 551 CSM patients who underwent either ACDF or ACCF surgery were meta-analyzed. Heterogeneity analysis shows that I2 was 97%. The test for overall effect (Z=0.78, P=0.43) indicated that the operation time between ACDF and ACCF for CSM was not significantly different ().
Figure 2 Comparison of operation time between ACDF and ACCF for the treatment of CSM.
Comparison of blood loss between ACDF and ACCF for CSM
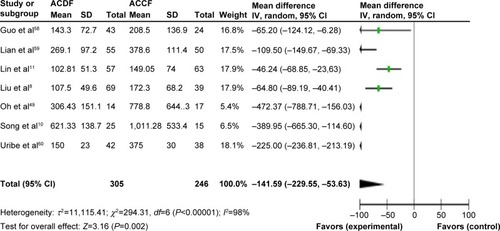
Seven studies reporting blood loss in a total of 551 CSM patients who underwent ACDF or ACCF surgery were also meta-analyzed. Heterogeneity analysis showed that I2 was 98%. The test for overall effect (Z=3.16, P=0.002) indicated that blood loss between ACDF and ACCF for CSM was significantly different ().
Figure 3 Comparison of blood loss between ACDF and ACCF for the treatment of CSM.
Comparison of bone fusion failure between ACDF and ACCF for CSM
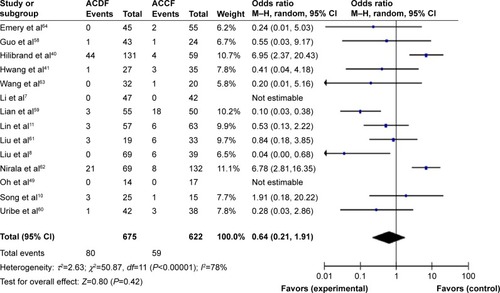
Fourteen studies including bone fusion failure records in a total of 1,297 CSM patients with ACDF or ACCF surgery were meta-analyzed. Heterogeneity analysis shows that I2 was 78%. The test for overall effect (Z=0.8, P=0.42) indicated that bone fusion failure between the two types of surgery was not significantly different ().
Figure 4 Comparison of bone fusion failure between ACDF and ACCF for the treatment of CSM.
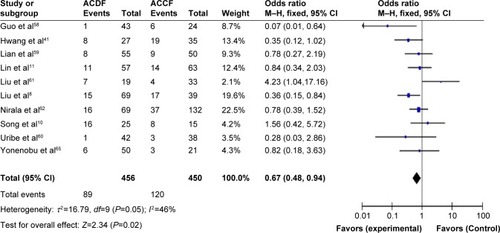
Comparison of numbers of complications between ACDF and ACCF for CSM
Ten studies with a record of numbers of complications during or after ACDF or ACCF surgery in a total of 906 CSM patients were meta-analyzed. Heterogeneity analysis shows that I2 was 46%. The test for overall effect (Z=2.34, P=0.02) indicated that numbers of complications between ACDF and ACCF for CSM was significantly different ().
Figure 5 Comparison of numbers of complications between ACDF and ACCF for the treatment of CSM.
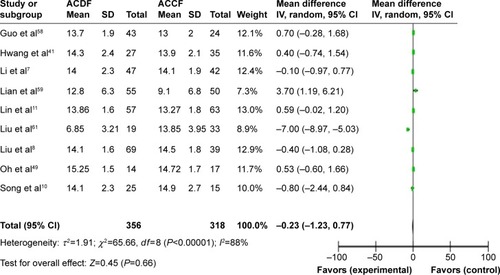
Comparison of post JOA scores between ACDF and ACCF for CSM
Nine studies with post JOA scores in a total of 674 CSM patients with ACDF or ACCF surgery were meta-analyzed. Heterogeneity analysis shows that I2 was 88%. The test for overall effect (Z=0.45, P=0.66) indicated that post JOA scores between ACDF and ACCF for CSM were not significantly different ().
Figure 6 Comparison of post Japanese Orthopedic Association scores between ACDF and ACCF for the treatment of CSM.
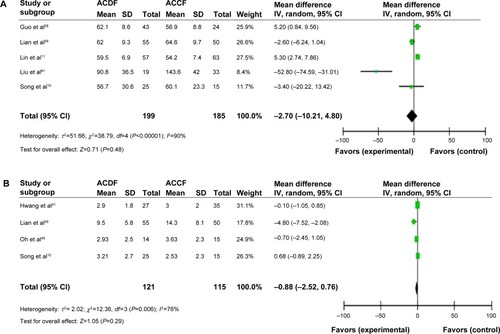
Comparison of clinical outcomes between ACDF and ACCF for CSM
We determined the recovery rates for five studies in a total of 384 CSM patients with ACDF or ACCF surgery. Heterogeneity analysis shows that I2 was 90%. The test for overall effect (Z=0.71, P=0.48) indicated that the recovery rates between ACDF and ACCF for CSM were not significantly different (). In addition, we also determined the VAS scores in four studies in a total of 236 CSM patients with ACDF or ACCF surgery. Heterogeneity analysis shows that I2 was 76%. The test for overall effect (Z=1.05, P=0.29) indicated that the VAS scores between ACDF and ACCF for CSM was not significantly different ().
Figure 7 (A) Comparison of recovery rates between ACDF and ACCF for the treatment of CSM. (B) Comparison of visual analog scale scores between ACDF and ACCF for the treatment of CSM.
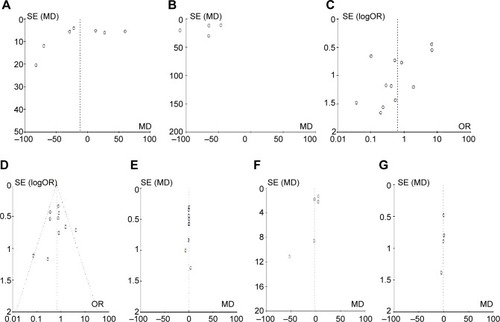
Sensitivity analysis and publication bias
A sensitivity analysis was conducted to assess the stability of our results. The pooled odds ratios or mean differences were not significantly changed, indicating the stability of our analyses. The funnel plots were largely symmetrical () suggesting that there was no publication bias in the meta-analysis of CSM patients with ACDF or ACCF surgery.
Figure 8 The funnel plots are largely symmetrical, suggesting there is no publication bias in the meta-analysis of anterior cervical discectomy and fusion and anterior cervical corpectomy and fusion in the treatment of cervical spondylotic myelopathy.
Abbreviations: SE, standard error; MD, mean difference.
Discussion
Previous studies have shown that surgical treatments of two-level CSM using ACDF or ACCF are similar in terms of clinical outcome. However, with regard to the amount of bleeding and radiological results, two-level ACDF was found to be superior to one-level ACCF in terms of operation times.Citation49
Cunningham et al reviewed retrospective cohort studies comparing ACDF, corpectomy, laminoplasty, and laminectomy and fusion as surgical options for CSM from 1980 to January 2008, and concluded that all approaches yield similar neurorecovery rates.Citation57 Recently, Shamji et al reviewed studies comparing multiple discectomies with single or multiple corpectomy, multiple discectomies with a hybrid discectomy–corpectomy procedure, and multiple corpectomies with a hybrid discectomy–corpectomy procedure, and concluded that all three operative approaches are effective strategies for the anterior surgical management of CSM.Citation1 However, which surgery is a better option in the treatment of multilevel CSM remains unclear.
Based on 15 studies and a total of 1,368 cases of multilevel CSM using ACDF or ACCF, this pooled analysis comprehensively assessed the clinical outcomes after surgery. Using pooled analysis from the included studies, we found that although blood loss and numbers of complications in ACDF was significantly less than in ACCF, other clinical outcomes, such as operation time, bone fusion failure, and post JOA scores between ACDF and ACCF for multilevel CSM were not significantly different.
We did find evidence of publication bias, and consistent results are shown in sensitivity analyses. We should mention several potential limitations of this study. First, the searching strategy was restricted to articles published in the English or Chinese languages. Articles with potentially high-quality data that were published in other languages were not included because of anticipated difficulties in obtaining accurate medical translations. Second, the possibility of information and selection biases and unidentified confounders cannot be completely excluded because all of the included studies were observational. Hence, caution is advised when interpreting our findings and how they may relate to the general population.
Based on this meta-analysis of ACDF and ACCF for the treatment of CSM, we conclude that although blood loss and numbers of complications during surgery in ACDF were significantly less that with ACCF, in terms of other clinical outcomes, such as operation time, bone fusion failure, post JOA scores, recovery rates, and VAS scores, there is no statistically significant difference between ACDF and ACCF for multilevel CSM were not significantly different.
Disclosure
The authors report no conflicts of interest in this work.
References
- ShamjiMFMassicotteEMTraynelisVCNorvellDCHermsmeyerJTFehlingsMGComparison of anterior surgical options for the treatment of multilevel cervical spondylotic myelopathy: a systematic reviewSpine (Phila Pa 1976)201338S195S20923962998
- KimHJTetreaultLAMassicotteEMDifferential diagnosis for cervical spondylotic myelopathy: literature reviewSpine (Phila Pa 1976)201338S78S8823962997
- ToledanoMBartlesonJDCervical spondylotic myelopathyNeurol Clin20133128730523186905
- EubanksJDBeldingJSchnaserECongenital stenosis and adjacent segment disease in the cervical spineOrthopedics201336e1251e125524093699
- DingCHongYLiuHShiRSongYLiTComparison of cervical disc arthroplasty with anterior cervical discectomy and fusion for the treatment of cervical spondylotic myelopathyActa Orthop Belg20137933834623926739
- BurkhardtJKMannionAFMarbacherSA comparative effectiveness study of patient-rated and radiographic outcome after 2 types of decompression with fusion for spondylotic myelopathy: anterior cervical discectomy versus corpectomyNeurosurg Focus201335E423815249
- LiJZhengQGuoXAnterior surgical options for the treatment of cervical spondylotic myelopathy in a long-term follow-up studyArch Orthop Trauma Surg201313374575123503888
- LiuYHouYYangLComparison of 3 reconstructive techniques in the surgical management of multilevel cervical spondylotic myelopathySpine (Phila Pa 1976)201237E1450E145822869063
- BasuSSreeramalingamRAdjacent level spondylodiscitis after anterior cervical decompression and fusionIndian J Orthop20124636036322719127
- SongKJLeeKBSongJHEfficacy of multilevel anterior cervical discectomy and fusion versus corpectomy and fusion for multilevel cervical spondylotic myelopathy: a minimum 5-year follow-up studyEur Spine J2012211551155722526699
- LinQZhouXWangXCaoPTsaiNYuanWA comparison of anterior cervical discectomy and corpectomy in patients with multilevel cervical spondylotic myelopathyEur Spine J20122147448121826497
- FengbinYJinhaoMXinyuanLXinweiWYuCDeyuCEvaluation of a new type of titanium mesh cage versus the traditional titanium mesh cage for single-level, anterior cervical corpectomy and fusionEur Spine J201333
- GaoRYangLChenHLiuYLiangLYuanWLong term results of anterior corpectomy and fusion for cervical spondylotic myelopathyPLoS One20127e3481122514669
- MiyamotoHMaenoKUnoKKakutaniKNishidaKSumiMOutcomes of surgical intervention for cervical spondylotic myelopathy accompanying local kyphosis (comparison between laminoplasty alone and posterior reconstruction surgery using the screw-rod system)Eur Spine J201322
- SahSWangLDahalMAcharyaPDwivediRSurgical management of cervical spondylotic myelopathyJNMA J Nepal Med Assoc20125217217723591248
- UmedaMSasaiKKushidaTA less-invasive cervical laminoplasty for spondylotic myelopathy that preserves the semispinalis cervicis muscles and nuchal ligamentJ Neurosurg Spine20131854555223540735
- UeharaMTakahashiJOgiharaNCervical pedicle screw fixation combined with laminoplasty for cervical spondylotic myelopathy with instabilityAsian Spine J2012624124823275807
- YangHLChenGDZhangHTWangLLuoZPOpen-door laminoplasty with plate fixation at alternating levels for treatment of multilevel degenerative cervical diseaseJ Spinal Disord Tech201326E13E1823075860
- KodeSGandhiAAFredericksDCGroslandNMSmuckerJDEffect of multilevel open-door laminoplasty and laminectomy on flexibility of the cervical spine: an experimental investigationSpine (Phila Pa 1976)201237E1165E117022614794
- MitsunagaLKKlinebergEOGuptaMCLaminoplasty techniques for the treatment of multilevel cervical stenosisAdv Orthop2012201230791622496982
- HardmanJGrafOKouloumberisPEGaoWHChanMRoitbergBZClinical and functional outcomes of laminoplasty and laminectomyNeurol Res20103241642019589202
- RadcliffKELimthongkulWKeplerCKCervical laminectomy width and spinal cord drift are risk factors for postoperative C5 palsyJ Spinal Disord Tech20122020
- RykenTCHearyRFMatzPGCervical laminectomy for the treatment of cervical degenerative myelopathyJ Neurosurg Spine20091114214919769493
- KristofRAKieferTThudiumMComparison of ventral corpectomy and plate-screw-instrumented fusion with dorsal laminectomy and rod-screw-instrumented fusion for treatment of at least two vertebral-level spondylotic cervical myelopathyEur Spine J2009181951195619662441
- OtaniKSatoKYabukiSIwabuchiMKikuchiSA segmental partial laminectomy for cervical spondylotic myelopathy: anatomical basis and clinical outcome in comparison with expansive open-door laminoplastySpine (Phila Pa 1976)20093426827319179921
- ShunzhiYZhonghaiLFengningLZhiCTieshengHSurgical management of 4-level cervical spondylotic myelopathyOrthopedics201336e613e62023672914
- ZhangHSunTLuSLiQYadavSKComparison of effectiveness between laminoplasty and laminectomy decompression and fusion with internal fixation for cervical spondylotic myelopathyZhongguo Xiu Fu Chong Jian Wai Ke Za Zhi20122611911196 Chinese23167101
- WoodsBIHohlJLeeJDonaldsonW3rdKangJLaminoplasty versus laminectomy and fusion for multilevel cervical spondylotic myelopathyClin Orthop Relat Res201146968869521089002
- AndersonPAMatzPGGroffMWLaminectomy and fusion for the treatment of cervical degenerative myelopathyJ Neurosurg Spine20091115015619769494
- GokBMcLoughlinGSSciubbaDMSurgical management of cervical spondylotic myelopathy with laminectomy and instrumented fusionNeurol Res2009311097110119215639
- LeblDRHughesACammisaFPJrO’LearyPFCervical spondylotic myelopathy: pathophysiology, clinical presentation, and treatmentHSS J2011717017822754419
- LawrenceBDShamjiMFTraynelisVCSurgical management of degenerative cervical myelopathy: a consensus statementSpine (Phila Pa 1976)201338S171S17223963012
- LawrenceBDJacobsWBNorvellDCHermsmeyerJTChapmanJRBrodkeDSAnterior versus posterior approach for treatment of cervical spondylotic myelopathy: a systematic reviewSpine (Phila Pa 1976)201338S173S18223962995
- MuthukumarNSurgical management of cervical spondylotic myelopathyNeurol India20126020120922626705
- LawrenceBDBrodkeDSPosterior surgery for cervical myelopathy: indications, techniques, and outcomesOrthop Clin North Am2012432940viiviii22082627
- RaoRDGourabKDavidKSOperative treatment of cervical spondylotic myelopathyJ Bone Joint Surg Am2006881619164016818991
- HillardVHApfelbaumRISurgical management of cervical myelopathy: indications and techniques for multilevel cervical discectomySpine J20066242S251S17097544
- TraynelisVCArnoldPMFourneyDRBransfordRJFischerDJSkellyACAlternative procedures for the treatment of cervical spondylotic myelopathy: arthroplasty, oblique corpectomy, skip laminectomy: evaluation of comparative effectiveness and safetySpine (Phila Pa 1976)9102013 Epub ahead of print
- GoreDRThe arthrodesis rate in multilevel anterior cervical fusions using autogenous fibulaSpine (Phila Pa 1976)2001261259126311389393
- HilibrandASFyeMAEmerySEPalumboMABohlmanHHIncreased rate of arthrodesis with strut grafting after multilevel anterior cervical decompressionSpine (Phila Pa 1976)20022714615111805659
- HwangSLLeeKSSuYFAnterior corpectomy with iliac bone fusion or discectomy with interbody titanium cage fusion for multilevel cervical degenerated disc diseaseJ Spinal Disord Tech20072056557018046168
- SwankMLLoweryGLBhatALMcDonoughRFAnterior cervical allograft arthrodesis and instrumentation: multilevel interbody grafting or strut graft reconstructionEur Spine J199761381439209883
- BolestaMJRechtineGR2ndChrinAMThree- and four-level anterior cervical discectomy and fusion with plate fixation: a prospective studySpine (Phila Pa 1976)2000252040204410954634
- WangJCMcDonoughPWKanimLEEndowKKDelamarterRBIncreased fusion rates with cervical plating for three-level anterior cervical discectomy and fusionSpine (Phila Pa 1976)20012664364611246376
- FraserJFHartlRAnterior approaches to fusion of the cervical spine: a meta-analysis of fusion ratesJ Neurosurg Spine2007629830317436916
- IwasakiMKawaguchiYKimuraTYonenobuKLong-term results of expansive laminoplasty for ossification of the posterior longitudinal ligament of the cervical spine: more than 10 years follow upJ Neurosurg20029618018912450281
- ClowardRBThe anterior approach for removal of ruptured cervical disks. 1958J Neurosurg Spine2007649651117542522
- ChangSWKakarlaUKMaughanPHFour-level anterior cervical discectomy and fusion with plate fixation: radiographic and clinical resultsNeurosurgery20106663964620305488
- OhMCZhangHYParkJYKimKSTwo-level anterior cervical discectomy versus one-level corpectomy in cervical spondylotic myelopathySpine (Phila Pa 1976)20093469269619333101
- HanYCLiuZQWangSJLiLJTanJIs anterior cervical discectomy and fusion superior to corpectomy and fusion for treatment of multilevel cervical spondylotic myelopathy? A systemic review and meta-analysisPLoS One20149e8719124489868
- MoherDLiberatiATetzlaffJAltmanDGReprint – preferred reporting items for systematic reviews and meta-analyses: the PRISMA statementPhys Ther20098987388019723669
- BeroLRennieDThe Cochrane Collaboration. Preparing, maintaining, and disseminating systematic reviews of the effects of health careJAMA1995274193519388568988
- HigginsJPTGreenSCochrane handbook for systematic reviews of interventions version 5.0.2 (updated September 2009)The Cochrane Collaboration2009–2010Accessed March 1
- BeggCBMazumdarMOperating characteristics of a rank correlation test for publication biasBiometrics199450108811017786990
- EggerMDavey SmithGSchneiderMMinderCBias in meta-analysis detected by a simple, graphical testBMJ19973156296349310563
- StangACritical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analysesEur J Epidemiol20102560360520652370
- CunninghamMRHershmanSBendoJSystematic review of cohort studies comparing surgical treatments for cervical spondylotic myelopathySpine (Phila Pa 1976)20103553754320190625
- GuoQBiXNiBOutcomes of three anterior decompression and fusion techniques in the treatment of three-level cervical spondylosisEur Spine J2011201539154421448583
- LianXFXuJGZengBFZhouWKongWQHouTSNoncontiguous anterior decompression and fusion for multilevel cervical spondylotic myelopathy: a prospective randomized control clinical studyEur Spine J20101971371920174838
- UribeJSSangalaJRDuckworthEAValeFLComparison between anterior cervical discectomy fusion and cervical corpectomy fusion using titanium cages for reconstruction: analysis of outcome and long-term follow-upEur Spine J20091865466219214597
- LiuPZhaoJLiQA comparative research of multilevel cervical spondylotic myelopathy treated by two different anterior operative methodsZhongguo Xiu Fu Chong Jian Wai Ke Za Zhi200620362366 Chinese16683431
- NiralaAPHusainMVatsalDKA retrospective study of multiple interbody grafting and long segment strut grafting following multilevel anterior cervical decompressionBr J Neurosurg20041822723215327222
- WangJCMcDonoughPWEndowKKDelamarterRBA comparison of fusion rates between single-level cervical corpectomy and two-level discectomy and fusionJ Spinal Disord20011422222511389372
- EmerySEBohlmanHHBolestaMJJonesPKAnterior cervical decompression and arthrodesis for the treatment of cervical spondylotic myelopathy. Two to seventeen-year follow-upJ Bone Joint Surg Am1998809419519697998
- YonenobuKFujiTOnoKOkadaKYamamotoTHaradaNChoice of surgical treatment for multisegmental cervical spondylotic myelopathySpine (Phila Pa 1976)1985107107164081877