Abstract
Glucocorticoids are commonly used in various fields within medicine. One of their most common and clinically significant side effects is glucocorticoid-induced osteoporosis (GIOP). GIOP is a disease leading to progressive decreases in bone mineral density, decreased bone strength, and increased risk of skeletal fractures. GIOP has a significant impact on the morbidity and health-related quality of life of the patients it affects. Glucocorticoids have deleterious effects on bone through promoting osteoblast apoptosis and inhibiting osteoblastogenesis. Teriparatide exerts anabolic effects on bone, so it is understandable why teriparatide is thought to be a rational treatment option. Clinical studies have indicated teriparatide is efficacious in the treatment of GIOP to improve bone mineral density values at the lumbar spine and femoral neck. Some evidence also suggests teriparatide may reduce rates of vertebral fractures in GIOP patients. Overall, this review of the current clinical evidence suggests teriparatide may be an efficacious and promising agent in the treatment of GIOP.
Introduction
Glucocorticoids are widely used in various specialties in medicine. It is estimated that 2.5% of the elderly population (aged 70–79 years) are prescribed oral glucocorticoid therapy.Citation1 These agents play an important role in the treatment of a variety of diseases, with significant impact on both morbidity and mortality in patients with these diseases. However, glucocorticoids are not benign therapies and are associated with a number of side effects. One of the most common and clinically significant side effects is glucocorticoid-induced osteoporosis (GIOP). GIOP is a disease leading to progressive decreases in bone mineral density, decreased bone strength, and increased risk of skeletal fractures. Citation2 It is estimated that 30%–50% of patients on long-term glucocorticoid therapy will sustain a fracture.Citation3 The risk of fracture is also related to the dosage of glucocorticoids. The estimated rates of vertebral and hip fractures are estimated to be 20% for daily prednisone doses ≤5 mg, and up to 60% for daily doses ≥20 mg, for more than three months.Citation4,Citation5 Even at low doses (<2.5 mg per day), there is an increased risk of vertebral fractures. As the dose was increased from 2.5 mg to 7.5 mg, and >7.5 mg, the risk of vertebral fracture increased accordingly.Citation1 Patients on higher doses of glucocorticoids are also more likely to require these agents for a longer duration.Citation4
Decreases in bone mineral density were evident by 3–6 months after initiating glucocorticoid therapy.Citation5 This is followed by a rapid decline in bone mineral density (BMD) after 6–12 months on glucocorticoid therapy.Citation6 After the one-year mark, there is a drop in the rate of BMD decline. Fracture rates were similar between males and females. However, with advancing age, rates of fractures in females rose exponentially, although this was seen in both control and glucocorticoid groups.Citation5
Inhaled glucocorticoids have also been evaluated regarding their effect on bone metabolism. High doses of inhaled glucocorticoids have been associated with a decline in BMD.Citation7,Citation8 It is still unclear if inhaled glucocorticoids increase fracture rates. There have been reports of increased fractures in both adults and children on inhaled glucocorticoids, but a similar fracture rate was also seen in inhaled nonsteroidal bronchodilator groups as well.Citation9,Citation10
Pathophysiology of glucocorticoid effects on bone
Bone loss resulting from glucocorticoid use occurs through a number of mechanisms. As described earlier, there is an early and rapid phase of bone resorption during the first year of glucocorticoid use. This phase is characterized by a state of increased bone resorption.Citation11
The mechanisms by which glucocorticoids promote bone resorption are not fully understood. Receptor activation of nuclear factor-κB ligand (RANK-L) likely plays a key role, and the expression of RANK-L is significantly increased in osteoblasts and stromal cells when stimulated by glucocorticoids.Citation11 Macrophage colony-stimulating factor levels are also increased with exposure to glucocorticoids through increased nuclear transcription of the macrophage colony-stimulating factor gene.Citation11 RANK-L and macrophage colony-stimulating factor both play pivotal roles in inducing osteoclastogenesis and decreasing osteoclast apoptosis, thereby leading to increased bone resorption (). In addition, osteoprotegerin expression is also decreased in osteoblasts and stromal cells in the presence of glucocorticoids.Citation12 Osteoprotegerin plays a counterregulatory role in the effects of RANK-L, and down-regulation of osteoprotegerin also enhances osteoclastogenesis and decreases rates of osteoclast apoptosis.Citation12
Figure 1 Downstream effect of glucocorticoids on bone metabolism.
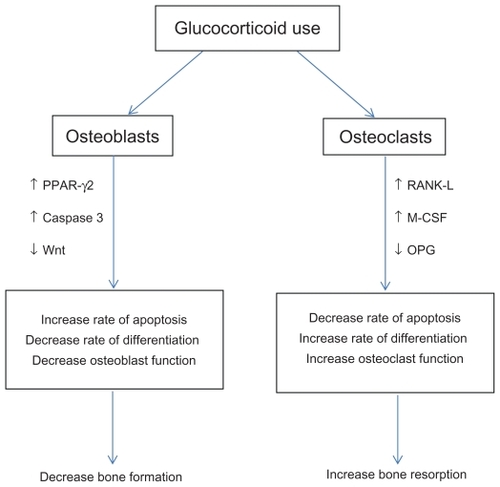
In addition, glucocorticoids also have important effects on osteoblasts. Long-term glucocorticoid use has effects on both osteoblast numbers and their functionCitation13 (). Glucocorticoids lead to a subsequent decrease in osteoblastogenesis through downregulation of the Wnt signalling pathway. There is also an upregulation of peroxisome proliferator-activated receptor-γ2 (PPAR-γ2) which leads to a decrease in osteoblastogenesis.Citation14 PPAR-γ2 activation favors differentiation of bone marrow stromal cells into the adipocyte lineage rather than the osteoblast lineage, thus decreasing osteoblastogenesis. Citation14 Glucocorticoids also activate caspase 3, which is an effector molecule playing a role in several apoptotic pathways. The activation of caspase 3 leads to increased apoptosis of both osteoblasts and osteocytes.Citation15 Loss of osteocytes also has a major impact on bone microarchitecture as a result of disruption of the osteocyte-canalicular network, which subsequently impairs repair of damaged bone.Citation16,Citation17
Mechanism of parathyroid hormone action
Parathyroid hormone plays an essential role in the regulation of calcium metabolism. When parathyroid hormone levels are continuously elevated, as seen in patients with primary or secondary hyperparathyroidism, there is a deleterious effect on bone, leading to a high turnover state and subsequent loss of cortical bone. However, intermittent pulsatile administration of parathyroid hormone has a contrary effect, leading to anabolic effects on bone. This accounts for the anabolic effects of teriparatide, ie, recombinant human parathyroid hormone-(1–34), shown in .
Figure 2 Role of pulsatile parathyroid hormone on osteoblast differentiation and function.
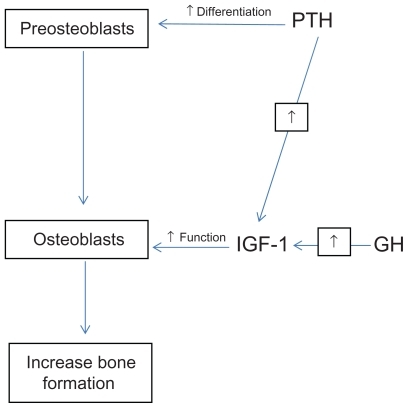
Osteoblasts and stromal cells in the bone marrow have surface receptors for parathyroid hormone. Intermittent pulses of parathyroid hormone activate different mechanisms to those activated by continuous administration of parathyroid hormone, and thus accounts for the different effects on bone metabolism.Citation18
The intermittent pulses of parathyroid hormone bind to the parathyroid hormone-1 receptor, a G-protein-coupled protein, which leads to subsequent activation of cyclic AMP-dependent protein kinase A and protein kinase C signalling pathways, both of which play key roles in regulating osteoblastogenesis and osteoblast function.Citation19
Insulin-like growth factor I (IGF-1) is another regulator of osteoblast function. IGF-1 acts directly on bone tissue as both a growth hormone-dependent hormone and as a local skeletal growth factor.Citation20 Overall, IGF-1 acts to promote bone formation and increases cancellous bone volumeCitation21 (). IGF-1 is primarily produced by the liver, but also by bone cells. Parathyroid hormone plays an important role in IGF-1 action, because parathyroid hormone increases the production of IGF-1 by bone cells. Subsequently, IGF-1 acts primarily on differentiated osteoblasts by increasing osteoblast function and subsequent new bone formation.Citation21 IGF-1 also prevents apoptosis of differentiated osteoblasts, which also contributes to the anabolic effect of pulsatile parathyroid hormone, ie, teriparatide.
The Wnt-β-catenin pathway plays an important role in osteoblastogenesis.Citation22,Citation23 This pathway may also be upregulated with pulsatile parathyroid hormone because sclerostin, a Wnt- β-catenin antagonist, is downregulated after activation of parathyroid hormone.Citation24 Sclerostin is expressed by osteoblasts and osteocytes, and acts through binding to Wnt coreceptors, which in turn prevents Wnt signalling. This upregulation of Wnt-β-catenin may also contribute to the anabolic action of teriparatide.Citation24
Beneficial effects of parathyroid hormone treatment
Conventional treatments for osteoporosis, including bisphosphonates, selective estrogen receptor modulators, calcitonin, and estrogen, have been shown to reduce the rate of bone resorption and preserve bone mass.Citation25 However, none of these have been shown to stimulate new bone formation. Citation25 Teriparatide [recombinant hPTH-(1–34)] is an agent shown to increase both bone mass and bone strength.Citation26 The Fracture Prevention Trial compared the effect of teriparatide 20 μg/day versus placebo in postmenopausal women.Citation26 In this trial, teriparatide was shown to increase lumbar spine and femoral neck BMD and decreased the incidence of both vertebral and nonvertebral fractures in postmenopausal women with osteoporosis.Citation26 This trial showed a reduction in the number of new vertebral fractures (relative risk [RR] 0.35) and in new nonvertebral fractures (RR 0.54).Citation26 The fracture prevention benefits of teriparatide were also shown to be independent of age and initial BMD.Citation27
Aside from its effect on BMD values, teriparatide also had a positive effect on non-BMD determinants of bone strength.Citation28,Citation29 Finally, teriparatide has also been shown to improve certain aspects of health-related quality of life. In particular, there are improvements in pain symptoms, certain aspects of emotional functioning, activities of daily living, and leisure activities also appear to improve with therapy.Citation30
Use of teriparatide in GIOP
GIOP has a significant impact on morbidity and health-related quality of life in the patients that it affects. General prevention strategies include eliminating the dosage of exogenous glucocorticoids, and supplementation with calcium and vitamin D. Certain patients will also require pharmacologic therapy to prevent further bone loss and reduce risk of future fractures.
Current guidelines for GIOP management recommend treatment with bisphosphonates, and in particular, treatment with alendronate or risedronate. In high-risk patients, the addition of a bisphosphonate is recommended early in the course of glucocorticoid therapy.Citation31,Citation32
After reviewing the pathophysiology of GIOP, and the mechanisms by which teriparatide exerts its anabolic effects on bone, it is understandable why teriparatide is thought to be a rational treatment option. Teriparatide directly stimulates osteoblastogenesis and inhibits osteoblast apoptosis, thus enhancing new bone formation with a subsequent increase in BMD. As mentioned earlier, glucocorticoids have deleterious effects on bone through promoting osteoblast apoptosis and inhibiting osteoblastogenesis, and thus teriparatide seems to be a physiologically rational treatment.
Parathyroid hormone was first used in the treatment of GIOP by Lane et al in 1998. They conducted a randomized controlled trial of teriparatide in postmenopausal women with osteoporosis who were also taking corticosteroids and hormone replacement. After treatment for 12 months, lumbar spine BMD increased by 11% as measured by dual-energy X-ray absorptiometry (DXA) and by 35% as measured by quantitative computed tomography (QCT).Citation33 This compared with a 0% increase measured by DXA (p < 0.001) and a 1.7% increase measured by QCT (p < 0.001) in the group treated with estrogen therapy only.Citation33
Lane et al also followed this group of patients treated with teriparatide for an additional 12 months after the initial treatment duration of 12 months was completed. BMD of the lumbar spine were quantified using QCT.Citation34 BMD measurements were also assessed at the lumbar spine, hip, and forearm using DXA. At 24-month follow-up, there was a 45.9% increase in BMD at the lumbar spine when assessed by QCT (p < 0.001) and a 12.6% increase when assessed by DXA (p < 0.001). The change in total hip and femoral neck BMD were not significant compared with the estrogen therapy alone group at 12 months, but there was a 4.7% increase (p < 0.01) for the total hip, and a 5.2% increase (p < 0.01) at the femoral neck at 24 months. The mean percent differences in BMD of the lumbar spine by QCT and DXA between the groups at 24 months were 43.1% and 11.9%, respectively, favoring the teriparatide group (p < 0.001). These results suggest that parathyroid hormone treatment in conjunction with estrogen therapy results in a significant BMD increase in the lumbar spine and hip in postmenopausal women with GIOP when compared with treatment with estrogen alone.Citation34 However, what is more interesting is that bone mass continued to increase after parathyroid hormone treatment (of 12 months’ duration) was discontinued, and this is particularly true for BMD values at the total hip and femoral neck.Citation34
Furthermore, treatment with teriparatide in postmenopausal women with GIOP was shown to increase not only BMD, but also to increase vertebral cross-section area, which was obtained by QCT of the L1 and L2 vertebrae.Citation35 After a 12-month course of teriparatide treatment, the vertebral cross-section area increased by 4.8% (p < 0.001 compared with baseline), and on the follow-up assessment at 24 months (12 months after therapy was discontinued), the vertebral cross-section area was still 2.6% higher than the baseline value (p < 0.05). No change in vertebral cross-section area was seen in the control group.Citation35
To assess the efficacy of teriparatide compared with that of alendronate in patients with GIOP further, Saag et al conducted a double-blind, controlled trial comparing the two treatments.Citation36 The study included both men and women (aged 22–89 years, mean 57.3 years in the alendronate group, mean 56.1 years in the teriparatide group) who had received glucocorticoids for at least three months (prednisone equivalent ≥5 mg daily). A total of 214 patients were randomized to receive teriparatide 20 μg daily, and 214 patients were randomized to receive alendronate 10 mg daily. The primary outcome was change in BMD at the lumbar spine, and secondary outcomes included changes in BMD at the total hip, time to change in BMD, incidence of new fractures, and also measures of bone turnover markers. After 36 months of follow-up, there was a significantly greater increase in BMD of the lumbar spine in the teriparatide group, with an 11.0% increase in the teriparatide group, compared with a 5.3% increase in the alendronate group (p < 0.001). There was also a greater increase in BMD at the total hip (5.2% in the teriparatide group versus 2.7% in the alendronate group, p < 0.001) and femoral neck (6.3% in the teriparatide group versus 3.4% in the alendronate group, p < 0.001).Citation36
Regarding its ability to reduce fractures, three of 173 patients in the teriparatide group were found to have a new vertebral radiographic fracture (1.7%). This compared with 13 of 169 patients (7.7%) with vertebral radiographic fractures in the alendronate group.Citation36 This was statistically significant between the two groups, with a p value of 0.007. There was also a statistically significant difference in clinical vertebral fractures, with four of 160 patients (2.4%) in the alendronate group, compared with 0 of 173 patients in the teriparatide group, with a p value of 0.037. There was no statistically significant difference between the groups regarding incidence rates of nonvertebral fractures (7.0% in alendronate group versus 7.5% in the teriparatide group, p = 0.843) or rates of nonvertebral fragility fractures (2.3% in the alendronate group versus 4.2% in the teriparatide group, p = 0.256). Also of interest is that the duration of teriparatide treatment in this trial was 36 months, which is longer than the usual duration of 24 months.
Post hoc analysis was performed to assess the effect of baseline glucocorticoid dose on BMD values at the lumbar spine, femoral neck, and total hip in patients treated with teriparatide or alendronate.Citation37 For the analysis, patients were divided into a low-dose glucocorticoid group (≤5 mg prednisone/day), a medium-dose group (5–15 mg/day), and a high-dose group (>15 mg per day). In patients treated with teriparatide, lumbar spine BMD increased by 8.1% in the low-dose group, 6.6% in the medium-dose group, and 4.6% in the high-dose group. This is compared with patients treated with alendronate, whereby the lumbar spine BMD increased by 3.6% in the low-dose group, 2.8% in the medium-dose group, and 2.3% in the high-dose group.Citation37 There was no significant difference in BMD at the femoral neck and total hip in either treatment group for the various glucocorticoid doses.
Teriparatide has also been shown to have effects on bone formation markers in patients with GIOP.Citation38 In a study including 159 females and 38 males with GIOP, serum osteocalcin and procollagen type I N-terminal propeptide (PINP) were measured in patients randomized to alendronate or teriparatide. At baseline, bone formation markers were below the reference interval in 33% of patients for osteocalcin and 4% of patients for PINP. After six months of therapy, patients in the teriparatide group had a median increase in osteocalcin levels by 92% and in PINP levels by 108%. In the same time interval, the alendronate group had a decrease in median osteocalcin levels by 40% and a decrease in PINP level by 53%.Citation38 It is unclear which bone turnover marker is best to measure in patients with GIOP treated with teriparatide. Serum levels of PINP, procollagen type I C-terminal peptide, and bone alkaline phosphatase show significant rises after one month of treatment with teriparatide. The changes in PINP levels at one and six months after teriparatide treatment did correlate with changes in femoral neck and lumbar spine BMD at 18 months post-treatment. The other parameters did not correlate with BMD changes after 18 months of teriparatide treatment.
There are a number of side effects which are seen more frequently in the teriparatide group compared with those taking placebo. They have higher frequencies of developing nausea (RR = 2.34), abdominal cramps (RR = 3.22), and hypercalcemia (RR = 9.73).Citation26 In the Fracture Prevention Trial, hypercalcemia (>10.6 mg/dL) was seen in 11% of patients in the teriparatide group, and 3% of patients had successive measurements in the hypercalcemia range,Citation26 although this was not sustained. Currently there are no recommendations regarding monitoring of serum calcium in patients taking teriparatide. Calcium and vitamin D intake through dietary and supplementary sources should be carefully considered based on serum calcium levels. If hypercalcemia persists on teriparatide therapy, then it should be discontinued, and serum calcium levels should be reassessed in 7–10 days.Citation39
Recently, there has been great interest in the association between atypical fractures of the femur and bisphosphonate therapy. There are a number of clinical risk factors which increase the risk of developing an atypical femoral fracture. Glucocorticoid use may be an important risk factor in this process, although the exact mechanism involved is unknown. In a recent systematic review of case reports and case series, nearly 40% of Caucasian women with atypical femur fractures were using glucocorticoids.Citation40 Teriparatide therapy should theoretically be free of this risk due to a completely different mechanism of action. Thus, teriparatide may be a useful option in GIOP patients who develop an atypical fracture of the femur.
Conclusion
In conclusion, GIOP is a common and potentially debilitating consequence of glucocorticoid therapy. Teriparatide has been shown to be efficacious in patients with postmenopausal osteoporosis. This review of the current clinical evidence suggests that teriparatide may be an efficacious and promising agent in the treatment of GIOP.
Disclosure
Dr Adachi has received consulting fees from Amgen, Astra Zeneca, Eli Lilly, GlaxoSmithKline, Merck, Novartis, Pfizer, Procter & Gamble, Roche, Sanofi Aventis, and Servier. Dr Lau has no financial disclosures.
References
- van StaaTPLeufkensHGAbenhaimLBegaudBZhangBCooperCUse of oral corticosteroids in the United KingdomQJM200093210511110700481
- RogerLSerious adverse events with low-dose, long-term corticosteroid therapy in rheumatoid arthritisAm J Med19959966926947503098
- LukertBPRaiszLGGlucocorticoid-induced osteoporosis: Pathogenesis and managementAnn Intern Med199011253523642407167
- van StaaTPLeufkensHGAbenhaimLZhangBCooperCUse of oral corticosteroids and risk of fracturesJ Bone Miner Res2000156993100010841167
- van StaaTPLeufkensHGCooperCThe epidemiology of corticosteroid-induced osteoporosis: A meta-analysisOsteoporos Int2002131077778712378366
- AdachiJDBensenWGBianchiFCividinoAPillersdorfSSebaldtRJVitamin D and calcium in the prevention of corticosteroid induced osteoporosis: A 3 year followupJ Rheumatol199623699510008782129
- IpMLamKYamLKungANgMDecreased bone mineral density in premenopausal asthma patients receiving long-term inhaled steroidsChest19941056172217278205866
- ToogoodJHBaskervilleJCMarkovAEBone mineral density and the risk of fracture in patients receiving long-term inhaled steroid therapy for asthmaJ Allergy Clin Immunol19959621571667636052
- van StaaTPLeufkensHGCooperCUse of inhaled corticosteroids and risk of fracturesJ Bone Miner Res200116358158811277277
- van StaaTPBishopNLeufkensHGCooperCAre inhaled corticosteroids associated with an increased risk of fracture in children?Osteoporos Int2004151078579114985948
- CanalisEBilezikianJPAngeliAGiustinaAPerspectives on glucocorticoid-induced osteoporosisBone200434459359815050888
- CanalisEMechanisms of glucocorticoid action in boneCurr Osteoporos Rep2005339810216131429
- O’BrienCAJiaDPlotkinLIGlucocorticoids act directly on osteoblasts and osteocytes to induce their apoptosis and reduce bone formation and strengthEndocrinology200414541835184114691012
- WuZBucherNLFarmerSRInduction of peroxisome proliferator-activated receptor gamma during the conversion of 3T3 fibroblasts into adipocytes is mediated by C/EBPbeta, C/EBPdelta, and glucocorticoidsMol Cell Biol1996168412841368754811
- WeinsteinRSJilkaRLParfittAMManolagasSCInhibition of osteoblastogenesis and promotion of apoptosis of osteoblasts and osteocytes by glucocorticoids. Potential mechanisms of their deleterious effects on boneJ Clin Invest199810222742829664068
- WeinsteinRSGlucocorticoids, osteocytes, and skeletal fragility: The role of bone vascularityBone201046356457019591965
- LaneNEYaoWBaloochMGlucocorticoid-treated mice have localized changes in trabecular bone material properties and osteocyte lacunar size that are not observed in placebo-treated or estrogen-deficient miceJ Bone Miner Res200621346647616491295
- MurrayTMRaoLGDivietiPParathyroid hormone secretion and action: Evidence for discrete receptors for the carboxyl-terminal region and related biological actions of carboxyl-terminal ligandsEndocr Rev20052617811315689574
- DempsterDWCosmanFParisienMShenVLindsayRAnabolic actions of parathyroid hormone on boneEndocr Rev19931466907098119233
- GiustinaAVeldhuisJDPathophysiology of the neuroregulation of growth hormone secretion in experimental animals and the humanEndocr Rev19981967177979861545
- ZhaoGMonier-FaugereMCLangubMCTargeted overexpression of insulin-like growth factor I to osteoblasts of transgenic mice: Increased trabecular bone volume without increased osteoblast proliferationEndocrinology200014172674268210875273
- CanalisEEconomidesANGazzerroEBone morphogenetic proteins, their antagonists, and the skeletonEndocr Rev200324221823512700180
- KrishnanVBryantHUMacdougaldOARegulation of bone mass by Wnt signalingJ Clin Invest200611651202120916670761
- BellidoTAliAAGubrijIChronic elevation of parathyroid hormone in mice reduces expression of sclerostin by osteocytes: A novel mechanism for hormonal control of osteoblastogenesisEndocrinology2005146114577458316081646
- BenhamouCLEffects of osteoporosis medications on bone qualityJoint Bone Spine200774394717196423
- NeerRMArnaudCDZanchettaJREffect of parathyroid hormone 1–34 on fractures and bone mineral density in postmenopausal women with osteoporosisN Engl J Med2001344191434144111346808
- MarcusRWangOSatterwhiteJMitlakBThe skeletal response to teriparatide is largely independent of age, initial bone mineral density, and prevalent vertebral fractures in postmenopausal women with osteoporosisJ Bone Miner Res2003181182312510801
- NevittMChenPKielDPReduced risk of back pain following teriparatide treatment: A meta-analysisOsteoporos Int200617227328016142502
- ChenPMillerPDDelmasPMisurskiDAKregeJHChanges in lumbar spine BMD and vertebral fracture risk reduction in teriparatide-treated postmenopausal women in osteoporosisJ Bone Miner Res200621111785179017002571
- LauANAliSHSawkaAMImprovement in health-related quality of life in osteoporosis patients treated with teriparatideBMC Musculoskelet Disord2008915118990249
- CompstonJUS and UK guidelines for glucocorticoid-induced osteoporosis: Similarities and differencesCurr Rheumatol Rep200461666914713404
- AbadieECDevogealerJPRingeJDRecommendations for the registration of agents to be used in the prevention and treatment of glucocorticoid-induced osteoporosis: Updated recommendations from the Group for the Respect of Ethics and Excellence in ScienceSemin Arthritis Rheum20053511416084217
- LaneNESanchezSModinGWGenantHKPieriniEArnaudCDParathyroid hormone treatment can reverse corticosteroid-induced osteoporosis. Results of a randomized controlled clinical trialJ Clin Invest19981028162716339788977
- LaneNESanchezSModinGWGenantHKPieriniEArnaudCDBone mass continues to increase at the hip after parathyroid hormone treatment is discontinued in glucocorticoid-induced osteoporosis: Results of a randomized controlled clinical trialJ Bone Miner Res200015594495110804025
- RehmanQLangTFArnaudCDModinGWLaneNEDaily treatment with parathyroid hormone is associated with an increase in vertebral cross-sectional area in postmenopausal women with glucocortico-idinduced osteoporosisOsteoporos Int2003141778112577188
- SaagKGZanchettaJRDevogelaerJPEffects of teriparatide versus alendronate for treating glucocorticoid-induced osteoporosis: Thirty-six-month results of a randomized, double-blind, controlled trialArthritis Rheum200960113346335519877063
- DevogelaerJPAdlerRARecknorCBaseline glucocorticoid dose and bone mineral density response with teriparatide or alendronate therapy in patients with glucocorticoid-induced osteoporosisJ Rheumatol201037114114819918047
- EastellRChenPSaagKGBone formation markers in patients with glucocorticoid-induced osteoporosis treated with teriparatide or alendronateBone201046492993420060078
- MillerPDSafety of parathyroid hormone for treatment of osteoporosisCurr Osteoporos Rep20086121618430395
- GiustiAHamdyNAPapapoulosSEAtypical fractures of the femur and bisphosphonate therapy: A systematic review of case/case series studiesBone201047216918020493982