
Abstract
Nonsteroidal anti-inflammatory drugs (NSAIDs) such as ibuprofen have a long history of safe and effective use as both prescription and over-the-counter (OTC) analgesics/antipyretics. The mechanism of action of all NSAIDs is through reversible inhibition of cyclooxygenase enzymes. Adverse drug reactions (ADRs) including gastrointestinal bleeding as well as cardiovascular and renal effects have been reported with NSAID use. In many cases, ADRs may occur because of drug–drug interactions (DDIs) between the NSAID and a concomitant medication. For example, DDIs have been reported when NSAIDs are coadministered with aspirin, alcohol, some antihypertensives, antidepressants, and other commonly used medications. Because of the pharmacologic nature of these interactions, there is a continuum of risk in that the potential for an ADR is dependent on total drug exposure. Therefore, consideration of dose and duration of NSAID use, as well as the type or class of comedication administered, is important when assessing potential risk for ADRs. Safety findings from clinical studies evaluating prescription-strength NSAIDs may not be directly applicable to OTC dosing. Health care providers can be instrumental in educating patients that using OTC NSAIDs at the lowest effective dose for the shortest required duration is vital to balancing efficacy and safety. This review discusses some of the most clinically relevant DDIs reported with NSAIDs based on major sites of ADRs and classes of medication, with a focus on OTC ibuprofen, for which the most data are available.
Introduction
Cyclooxygenase (COX) inhibitors, commonly called nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, diclofenac, and naproxen, have anti-inflammatory and analgesic/antipyretic properties across a wide range of dosing regimens. Prescription-strength NSAIDs are effective for relief of chronic musculoskeletal pain and inflammation in conditions such as rheumatoid arthritis (RA) or osteoarthritis (OA).Citation1,Citation2 Lower, over-the-counter (OTC) doses of NSAIDs are effective for short-term (eg, ≤10 days) relief of minor aches and pains due to headache, toothache, backache, menstrual cramps, common cold, muscular aches, and arthritis.Citation3 NSAIDs taken at OTC doses can also be effective at relieving painful episodes in patients with chronic diseases such as OA.Citation4 Ibuprofen is an NSAID with a long history of safe and effective use at both prescription (maximum 2,400–3,200 mg/d) and OTC (<1,200 mg/d) doses.Citation3,Citation5 Single-dose studies using OTC doses have confirmed that ibuprofen (400 mg) provides superior analgesic efficacy to acetaminophen (1,000 mg).Citation6,Citation7
All NSAIDs inhibit COX, an enzyme that converts arachidonic acid to prostaglandins, thereby mediating pain, inflammation, and fever. In the process, prostaglandin H2 is converted to five primary prostaglandins, including thromboxane A2 (which stimulates platelet aggregation and blood clot formation) in platelets and prostacyclin (a vasodilator that inhibits platelet aggregation) in the endothelium.Citation8 Two COX isoenzymes (COX-1 and COX-2) are commonly recognized. In general, COX-1 is constitutively expressed and is involved in gastroprotection from stomach acid and in thromboxane formation by platelets. COX-2 is inducible by inflammatory mediators in a wide range of tissues and has been associated with inflammation; however, it may also be constitutively expressed, where it contributes to renal physiology, reproductive function, bone resorption, and neurotransmission.Citation8
Drug–drug interactions (DDIs) have been reported when NSAIDs are coadministered with some common medications, and these DDIs can be classified in several ways. DDIs may result from pharmacokinetic interactions (ie, alterations in drug absorption, volume of distribution, metabolism, or excretion), pharmacodynamic interactions (ie, additive, synergistic, or antagonistic effects that occur despite unaltered plasma levels of the drugs), pharmaceutical incompatibility (eg, combinations of acids and bases), a combination of these mechanisms, or other unknown mechanisms.Citation9 One type of pharmacokinetic DDI of relevance to NSAIDs occurs when one highly protein-bound drug (eg, NSAID) competes for binding sites with other protein-bound drugs in the plasma.Citation9,Citation10
When assessing the safety profile of NSAIDs, it is important to distinguish between prescription and OTC use, especially since many adverse drug reactions (ADRs) are dose related.Citation11 Prescription users typically use high-dose NSAIDs for prolonged periods and are monitored for ADRs on a regular basis by health care providers. In contrast, although risks are generally lower with occasional use of OTC NSAIDs, users of these products are not routinely monitored by a health care provider and may be at risk for unrecognized ADRs. In addition, although a majority of consumers use OTC NSAIDs as per labeled instructions, a small proportion may exceed recommended doses,Citation12 likely resulting in the intake of prescription-level doses, the safety profile of which has also been well characterized.
This review discusses some of the most clinically relevant DDIs reported with NSAIDs based on major sites of ADRs and classes of medication, with a focus on OTC ibuprofen, the most commonly used OTC NSAID.Citation11 Fewer studies are available regarding ADRs and DDIs with other OTC NSAIDs (eg, naproxen, ketoprofen, diclofenac); these data have been included where available. It is likely that the interactions described for ibuprofen apply to these other NSAIDs as well, since they share the same mechanism of action and many of the same pharmacologic properties (with the exception of their degree of affinity for COX-1 vs COX-2). Given the low doses and short-term use of all OTC NSAIDs, risks of DDIs are generally much lower than for the corresponding full prescription dosages of these agents.
Major sites of ADRs
ADRs associated with NSAIDs primarily manifest in gastrointestinal (GI), cardiovascular (CV), and renal sites.
GI effects
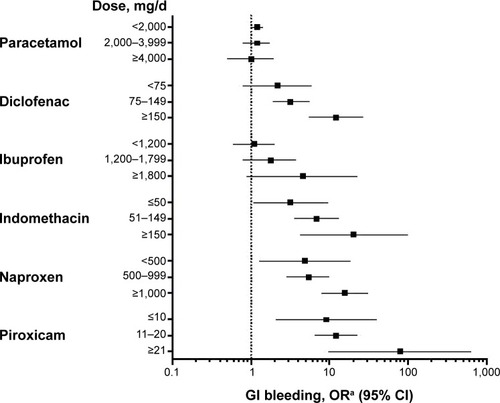
GI complications are well-recognized risks of NSAIDs as a class and vary by the respective NSAID used as well as by dose (ie, higher doses = more GI risk).Citation13–Citation16 Aspirin increases bleeding risk, even at low cardioprotective doses (eg, 75–300 mg).Citation17,Citation18 In terms of nonselective NSAIDs, a meta-analysis of data from three retrospective case-control studies found that ibuprofen had the lowest odds ratio (OR) for development of GI bleeding versus diclofenac, naproxen, piroxicam, and indomethacin, but that the OR increases with dose level for each agent ().Citation19
Figure 1 Effect of dose (in week before index day) on ORs of upper GI bleeding: meta-analysis of three case-control studies.
Abbreviations: CI, confidence interval; GI, gastrointestinal; OR, odds ratio.
The Paracetamol, Aspirin, and Ibuprofen New Tolerability (PAIN) study (N=8,677) assessed the frequency of significant adverse events (AEs) associated with OTC analgesic dosing in patients with acute pain.Citation20 In this study, a significant AE was defined as any event that was serious, severe, or moderate; necessitated a second physician consultation; led to treatment discontinuation; or was of missing intensity. The PAIN study demonstrated that OTC ibuprofen (≤1,200 mg/d) was similar to acetaminophen (≤3,000 mg/d) in terms of the incidence of significant AEs (13.7% vs 14.5%, respectively), but that statistically significantly fewer such events occurred with ibuprofen in comparison with aspirin (≤3,000 mg/d, 18.7%; P<0.001) during 1–7 days of treatment.Citation20 As expected, rates of GI AEs were significantly lower in patients receiving OTC doses of ibuprofen versus aspirin (4.0% vs 7.1%; P<0.001), and interestingly, ibuprofen was noted to produce significantly fewer overall GI AEs vs acetaminophen (5.3%; P=0.025).Citation20 The PAIN study also identified numerous factors associated with increased risk of AEs, including female sex, older age, height ≤160 cm, use of the analgesic for musculoskeletal pain (vs menstrual cramps, sore throat, toothache, or fever), concomitant use of prohibited medications, and increasing number of concomitant medications.Citation21
The prospective, observational Arthritis, Rheumatism, and Aging Medical Information System database study evaluated the GI toxicity of ibuprofen, aspirin, and acetaminophen at various doses in patients with RA (n=5,692) or OA (n=3,124) and found no GI toxicity rates of >1% when each respective agent was taken alone, especially when used occasionally or intermittently at lower doses.Citation22 Interestingly, the investigators found that rates of GI events were significantly higher (P<0.05) in the acetaminophen group taking concurrent therapy plus corticosteroids compared with those taking either ibuprofen or aspirin with concurrent therapy plus corticosteroids.Citation22
In comparisons of GI AEs among NSAID users, results from several meta-analyses further support a lower risk of GI AEs with ibuprofen compared with other NSAIDs.Citation15,Citation16,Citation19,Citation23 For example, Richy et al reported a lower relative risk (RR) for GI complications with ibuprofen (1,200 mg/d median dose; RR: 1.19; 95% confidence interval [CI]: 0.93–1.54 vs no NSAID use) than with other NSAIDs, including naproxen (875 mg/d median dose; RR: 1.83; 95% CI: 1.25–2.68 vs no NSAID use).Citation23 A case-control study (N=1,217; 627 cases with GI bleeding and 590 controls) found that GI bleeding risk increased dose dependently by current ibuprofen use (OR: 1.8; 95% CI: 0.8–4.1 for ≤600 mg/d; OR: 3.5; 95% CI: 1.2–10.7 for 601–1,200 mg/d; and OR: 3.9; 95% CI: 1.2–12.9 for >1,200 mg/d).Citation24
In addition to strength of dose, length of treatment also contributes to GI risk. Lewis et al interviewed 359 persons admitted to hospitals in the Philadelphia, PA, USA, area, and 1,889 randomly telephoned controls for serious GI toxicity to evaluate the potential contribution of OTC NSAIDs to GI toxicity. They found no association of infrequent use (1–3 days in the index week) of OTC NSAIDs with serious upper GI toxicity (OR: 0.67; 95% CI: 0.43–1.06), but the association was significant when OTC NSAIDs were used 4–7 days in the index week (OR: 1.83; 95% CI: 1.14–2.95).Citation25
Concomitant medications also influence the risk of GI events among NSAID users. The risk of upper GI events is increased when non-aspirin NSAIDs are combined with aspirin, but this increase in risk may be ameliorated when NSAIDs are used concurrently with ulcer-healing drugs (ie, proton pump inhibitors).Citation26
CV risk
All non-aspirin NSAIDs may be associated with a potential increase in CV thrombotic risk.Citation27 A US Food and Drug Administration (FDA) Advisory Committee (February 10–11, 2014) concluded that there is insufficient evidence to support claims of difference among NSAIDs with regard to CV risk.Citation28 Labeling for OTC NSAIDs currently states, “the risk of heart attack or stroke may increase if you use more than directed or for longer than directed.”Citation29,Citation30 However, the FDA Advisory Committee concluded that there is no period of latency for CV thrombotic risk, and therefore, patients should take the lowest dose of NSAIDs for the shortest period of time possible.Citation28
A majority of the data on CV risk among NSAID users is from epidemiological studies of prescription NSAIDs. COX-2 inhibitors were developed as prescription NSAIDs with lower GI risks, but some have been posited to have increased CV risk.Citation31,Citation32 In studies evaluating potential risk for CV events (myocardial infarction [MI] or death), ibuprofen at prescription doses has been associated with a range from no risk (adjusted rate ratio: 0.96; 95% CI: 0.81–1.14)Citation33 to a significantly increased risk (hazard ratio [HR]: 1.84; 95% CI: 1.62–2.08; P<0.01).Citation34 Prescription doses of naproxen have been associated with a significantly decreased risk (adjusted rate ratio: 0.75; 95% CI: 0.62–0.92)Citation33 to significantly increased risk (adjusted OR: 1.27; 95% CI: 1.01–1.60; P=0.04) for CV events when taken within the previous 3 months.Citation35
There are few data on actual CV risk with NSAID use at OTC doses, but risk is likely to be small, especially in younger patients who have few CV risk factors.Citation27 It has been hypothesized that the increase in CV risk among NSAID users stems from increased blood pressure (BP) due to COX-2 inhibition in the kidneys – an effect that has not been observed with OTC doses.Citation27 The PAIN study (n=2,886 for OTC ibuprofen), although not specifically designed and/or powered to assess CV risk, reported a low rate of CV events (0.4%) with OTC ibuprofen (up to 1,200 mg/d) that was not significantly different from that of either aspirin (up to 3,000 mg/d; 0.7%; P=0.13) or acetaminophen (up to 3,000 mg/d; 0.6%; P=0.28).Citation20 Although prescription NSAIDs (especially COX-2 inhibitors) are associated with increased risk of death in patients with chronic heart failure, risk does not appear to be increased with OTC ibuprofen (HR: 0.99 for doses ≤1,200 mg/d) or naproxen (HR: 0.88 for doses ≤500 mg/d) in these patients.Citation36
As noted above, the labeling for OTC NSAIDs indicates a potential increase in stroke risk if taken at higher doses or for longer than recommended durations.Citation29,Citation30 A longitudinal cohort study in Denmark reported that risk of stroke is slightly increased (standardized mortality ratio of 1.10 [95% CI: 1.0–1.3] for hemorrhagic stroke and 1.18 [95% CI: 1.1–1.3] for other stroke) among users of prescription ibuprofen.Citation37 However, a second longitudinal cohort study comparing new users of NSAIDs or COX-2 inhibitors with nonusers in a Pennsylvania Medicare drug benefit program found no increased risk of stroke with ibuprofen (rate ratio: 0.95; 95% CI: 0.78–1.16) or naproxen (rate ratio: 0.83; 95% CI: 0.67–1.04).Citation33
Renal toxicity
All NSAIDs can alter renal function by inhibiting COX-1 (which regulates renal hemodynamics and glomerular filtration) and/or COX-2 (which mediates salt and water excretion) expressed in the kidneys.Citation38 Uncommon, but concerning, renal syndromes caused by nonselective NSAIDs include sodium retention, peripheral edema, increased BP and weight, congestive heart failure (rare), hyperkalemia, and acute renal failure.Citation38 Risk factors include preexisting severe hepatic or renal dysfunction, nephrotic syndrome with high-level proteinuria, older age, diabetes, hypertension, and congestive heart failure.Citation38 Furthermore, individuals experiencing renal stress (eg, dehydration) from exercise in hot environments may be at a small increased risk for acute renal failure with ibuprofen.Citation39 A nested case-control analysis of new prescription NSAID users over 65 years of age in Quebec, Canada, (n=4,228 cases hospitalized for acute renal failure; n=84,540 matched controls) found that risk of renal failure was increased with current new use of NSAIDs (rate ratio: 2.05; 95% CI: 1.61–2.60), including naproxen (rate ratio: 2.42; 95% CI: 1.52–3.85), conventional NSAIDs (rate ratio: 2.30; 95% CI: 1.60–3.32), and celecoxib (rate ratio: 1.54; 95% CI: 1.14–2.09).Citation40
NSAIDs may lessen response to diuretics and worsen renal insufficiency associated with use of angiotensin-converting enzyme inhibitors (ACEIs) and angiotensin II receptor blockers (ARBs);Citation38 however, a study of OTC analgesics in elderly patients with diuretic-treated hypertension and mild renal insufficiency found no significant impact of ibuprofen on creatinine clearance nor on blood urea nitrogen, serum creatinine, sodium, or potassium levels.Citation41
Indeed, OTC ibuprofen in general has been shown to have a low risk of renal AEs. In a case-control study of Tennessee Medicaid recipients (N=11,698), OTC ibuprofen doses were not associated with increased risk for acute renal failure; however, the risk increased dose dependently (adjusted ORs: 0.94, 1.89, and 2.32 at ≤1,200, >1,200–<2,400, and ≥2,400 mg/d, respectively).Citation42
Randomized controlled trials (RCTs) have found no increased risk for renal failure in children taking ibuprofen for fever.Citation43,Citation44 Despite evidence from large clinical trials, case studies have reported renal failure in children taking OTC ibuprofen; dehydration may have been a contributing factor.Citation45,Citation46 There have also been cases reported of transient renal failure among children with cystic fibrosis who were concurrently treated with ibuprofen and intravenous aminoglycosides.Citation47
In summary, risk of GI bleeding varies by NSAID and is related to both dose and duration of treatment. Short-term, infrequent use of ibuprofen at OTC doses has a low risk similar to that of acetaminophen and less than that of aspirin. Bleeding risk is increased if NSAIDs are used concomitantly with aspirin and decreased if used with ulcer-healing drugs. All non-aspirin NSAIDs may increase CV thrombotic risk, based largely on epidemiological studies of prescription NSAID use. Limited data are available to allow for assessment of the magnitude of this risk in users of OTC NSAIDs, but risk is likely to be low, especially in young patients with few CV risk factors. Long-term use of high-dose NSAIDs may increase stroke risk, but the corollary among short-term users of low-dose NSAIDs is not well defined. Renal toxicity is an uncommon AE of all NSAIDs, and risk is elevated in those who have preexisting severe hepatic or renal dysfunction, nephrotic syndrome with high-level proteinuria, older age, diabetes, hypertension, congestive heart failure, or dehydration. NSAIDs may lessen response to diuretics and worsen renal insufficiency associated with use of ACEIs and ARBs. Risk of these interactions and renal AEs is low among users of OTC ibuprofen.
Overdose
Unlike acetaminophen and aspirin, the margin of safety (ie, difference between minimal effective dose and minimal toxic dose) with ibuprofen is high, and ibuprofen is not associated with a substantial incidence of serious ADRs in cases of overdose.Citation48 A comparative study found that among 10,134 reported cases of overdose with acetaminophen (48.0%), aspirin (36.6%), and ibuprofen (15.4%) reported to US poison control centers, life-threatening or fatal events were reported in 5.6%, 5.9%, and 1.6% of adults and in 0.3%, 0.4%, and 0.4% of children, respectively.Citation49
Potential drug interactions
Antihypertensives
Hypertension and chronic pain can be frequent comorbidities in the elderly and those with chronic disease; therefore, concomitant use of NSAIDs and antihypertensives is common.Citation50 Efficacy of medications that act on renal prostaglandins (eg, furosemide) or modify their effects (eg, other diuretics or ACEIs) may be reduced, resulting in increases in BP with NSAID coadministration because of inhibition of renal prostaglandins and increased fluid retention.Citation38
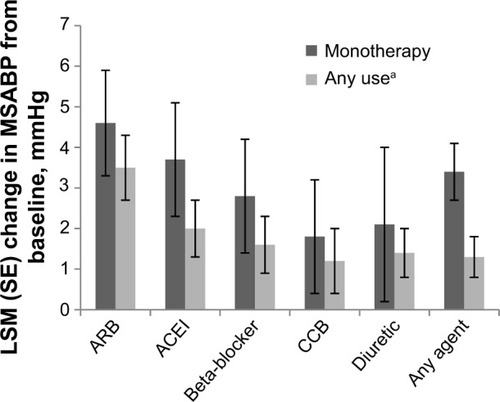
Some trials found increased risk of DDIs when prescription-strength NSAIDs and antihypertensives were coadministered over a period of multiple weeks.Citation50,Citation51 Other trials found no significant effect on BP when OTC doses of ibuprofen or naproxenCitation52 or prescription-dose ibuprofenCitation53,Citation54 were combined with antihypertensives. A recent post hoc analysis of an RCT comparing the effects of lumiracoxib (a prescription COX-2 inhibitor; 100 mg/d) with prescription ibuprofen (1,800 mg/d) in OA patients with hypertension controlled on stable doses of antihypertensive medication(s) observed small but consistent increases of 2.2 mmHg overall versus baseline in 24-hour mean systolic BP (SBP) in the ibuprofen-treated group. The greatest increases occurred when ibuprofen was combined with ARBs or ACEIs ().Citation55
Figure 2 Summary of changes in systolic ambulatory blood pressure when prescription ibuprofen (1,800 mg/d) and antihypertensives are coadministered.
Abbreviations: ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin II receptor blocker; CCB, calcium channel blocker; LSM, least squares mean; MSABP, mean systolic ambulatory blood pressure; SE, standard error.
In addition to effects on BP, there is concern that an interaction between NSAIDs and antihypertensive agents may increase the risk of acute kidney injury, since each of these classes of drugs affects kidney function via differing mechanisms.Citation56 A large case-control analysis consisting of 2,215 cases of acute kidney injury and 21,993 controls without kidney injury, all of whom were taking antihypertensive agents, found that risk of acute kidney injury was not significantly increased when NSAIDs were combined with diuretics, ACEIs, or ARBs; however, a significant increase was observed in those taking triple therapy consisting of an NSAID, a diuretic, and either an ACEI or an ARB (adjusted rate ratio: 1.31; 95% CI: 1.12–1.53).Citation56 In another study, four of 17 African American women who received fosinopril 10–40 mg/d and hydrochlorothiazide (HCTZ) 25 mg/d for hypertension and ibuprofen 2,400 mg/d over 1 month for OA developed acute renal failure (ie, glomerular filtration rate decrease ≥25%).Citation54
Renin–angiotensin–aldosterone system inhibitors
Inhibitors of the renin–angiotensin–aldosterone system include antihypertensives such as ACEIs, ARBs, and direct renin inhibitors. A 4-week RCT of prescription ibuprofen (2,400 mg/d), nabumetone (2,000 mg/d), celecoxib (400 mg/d), or placebo in hypertensive patients (N=385) receiving an ACEI found that ibuprofen coadministration, but not nabumetone or celecoxib coadministration, significantly increased SBP by a mean ± standard error of 6.5±1.4 mmHg (P=0.0001) and diastolic BP by 3.5±0.9 mmHg (P=0.0069) from baseline.Citation50 Prescription-strength ibuprofen was also associated with the greatest percentage of patients who experienced SBP changes of clinical concern, defined as a 20 mmHg increase from baseline and measuring >140 mmHg: 16.7% versus 5.5% in the nabumetone group, 4.6% in the celecoxib group, and 1.1% in the placebo group (P<0.001 for ibuprofen vs placebo).Citation50 A Croatian prospective trial (N=110) evaluated the effects of prescription NSAIDs (piroxicam or ibuprofen; n=60) taken for OA on antihypertensive activity of a calcium channel blocker (amlodipine) or an ACEI/thiazide diuretic (lisinopril/HCTZ) combination. Compared with baseline, mean arterial pressure increased by 9.5 mmHg (8.9%) with ibuprofen and by 10.2 mmHg (9.5%) with piroxicam (both P<0.001) in patients taking lisinopril/HCTZ; there was a nonsignificant 0.5 mmHg (0.5%) increase in mean arterial BP with either NSAID among patients taking amlodipine.Citation57
Few data on potential DDIs between direct renin inhibitors and NSAIDs have been reported; however, a single report from three open-label studies of aliskiren found that concurrent administration with celecoxib (n=22) resulted in minor changes to the pharmacokinetic profile of aliskiren but not that of celecoxib.Citation58
It should also be noted that aldosterone antagonists (eg, spironolactone) are associated with an increased risk of GI bleeding and possibly impaired healing of gastric or duodenal erosions.Citation59 Thus, risk of GI bleeding in patients taking these agents may be further increased when NSAIDs are used concomitantly.Citation60 Patients treated long term with aldosterone antagonists should be informed of the risk of upper GI bleeding and perhaps warned of the risk of using OTC NSAIDs long term.
Diuretics
Thiazide diuretics (eg, HCTZ) are also associated with potential DDIs when combined with NSAIDs.Citation61 A randomized, double-blind, two-period crossover trial evaluating the effects of 4 weeks of prescription ibuprofen (1,800 mg/d) or placebo (4 weeks’ treatment; 2-week washout period between treatments) in combination with HCTZ in hypertensive patients (N=25) found that ibuprofen significantly increased SBP by 4.2 mmHg (supine) and 4.7 mmHg (standing) compared with placebo (P≤0.004).Citation51 An RCT examining the effect of prescription ibuprofen (2,400 mg/d) and naproxen (750 mg/d) on BP in patients (N=97) with mild essential hypertension treated with HCTZ 50 mg/d found a <3 mmHg mean increase in diastolic BP from baseline during the 4-week study for either treatment group, the clinical effects of which were likely minor.Citation62 A single-blind, factorial, parallel-group study (N=88) found that patients taking lisinopril/HCTZ (n=29) who were randomly assigned to concurrent prescription ibuprofen (1,200–1,800 mg/d) or piroxicam (10–20 mg/d) experienced SBP elevations of up to 7.7% (P=0.004) and 9.5% (P=0.001), respectively, compared with baseline.Citation63 An open-label, randomized, five-way crossover study comparing placebo, furosemide alone, furosemide with oral diclofenac, furosemide with diclofenac epolamine patch, or furosemide with ibuprofen 2,400 mg/d (N=40) found that although prescription ibuprofen administration decreased clearance of furosemide and increased urine sodium excretion, no clinically relevant effect on BP was observed in healthy volunteers.Citation64 Topical diclofenac had no effect on furosemide pharmacokinetics or pharmacodynamics, and oral diclofenac compared with furosemide alone decreased urine output, but neither formulation was associated with alterations in BP.Citation64
β-adrenergic and calcium channel blockers
Some NSAIDs, including indomethacin and flurbiprofen (but not naproxen or aspirin), have been found to interact with β-blockers (eg, propranolol, oxprenolol, atenolol), attenuating their antihypertensive effects.Citation65 In an RCT of prescription-strength ibuprofen (1,600 mg/d) plus propranolol, no significant increase in BP was found.Citation66 As noted earlier, a post hoc analysis of an RCT demonstrated that prescription ibuprofen (1,800 mg/d) produced a small increase in SBP when combined with β-blocker (2.8 mmHg) or calcium channel blocker (1.8 mmHg).Citation55 Calcium channel blockers such as verapamil and amlodipine do not appear to be associated with clinically significant interactions with NSAIDs.Citation52,Citation57 These results are expected from the mechanisms of action of both drug families.Citation52
In summary, these data suggest that prescription-strength NSAIDs, including ibuprofen, may be associated with small but statistically significant increases in BP that are greatest when coadministered with ARBs and ACEIs and lowest with calcium channel blockers and loop diuretics. The clinical relevance of these findings remains unclear, although one analysis that modeled the effects of hypertension in patients taking COX-2 inhibitors predicted that NSAID-driven hypertension may contribute to CV events and deaths.Citation67 Given the clear dose- and duration-response relationship between ibuprofen use and ADRs in generalCitation43 and the very small increase in BP observed with prescription-strength NSAIDs, any DDI occurring with short-term OTC ibuprofen and antihypertensives would most likely have only a minor effect on BP. However, of most concern is potential inhibition of antihypertensive efficacy with chronic use of higher doses. Thus, hypertensive patients who require ARBs, ACEIs, or thiazide diuretics such as HCTZ should avoid chronic prescription NSAID use.
Antithrombotics
Interactions between NSAIDs and several classes of anti-thrombotic drugs, including aspirin and warfarin, have been reported. This section will discuss DDIs resulting in CV changes as well as DDIs with aspirin and other NSAIDs that may contribute to asthma exacerbations (by a nonallergic mechanism).
Aspirin
Coadministration of aspirin and most NSAIDs (other than diclofenac and ketorolac) can lead to pharmacodynamic DDIs resulting from competition for access to the acetylation site of platelet-expressed COX-1.Citation68–Citation70 NSAID-driven reversible, transient inhibition of platelet aggregation blocks aspirin’s irreversible inhibition, thereby potentially allowing clot formation.Citation68 This NSAID-driven effect on aspirin is of particular concern in individuals at high CV risk who take low-dose aspirin daily to reduce the risk of a thrombotic event.Citation68,Citation69 A case-control study (N=5,208, including 1,055 cases of first nonfatal MI and 4,153 community controls) found that patients taking daily prophylactic aspirin plus ibuprofen four or more times/week (doses not reported) had double the risk of an MI compared with aspirin-only users, although the difference was not statistically significant (OR: 2.03; 95% CI: 0.60–6.84), whereas the OR for MI with infrequent use (less than four times/week) of ibuprofen plus daily aspirin was 0.60 (95% CI: 0.21–1.66).Citation71 Other studies also indicate that concomitant aspirin and ibuprofen could increase the possibility of experiencing a CV event,Citation72,Citation73 but one of these found no increase in risk of MI associated with intermittent use of NSAIDs (<60 days/year) in healthy persons without CV disease.Citation72
These data and interpretation of risk are somewhat confounded by other studies suggesting that risk for a CV event may actually be reduced with concomitant aspirin and ibuprofen. In a single-center, retrospective analysis, patients prescribed aspirin (typically 325 mg/d) and ibuprofen (mean 1,947 mg/d) (n=3,859) experienced ~40% fewer MIs than those prescribed aspirin alone (n=10,239; rate ratio: 0.61; 95% CI: 0.50–0.73; P<0.001).Citation74 A retrospective study (N=42,611, including 8,688 cases with MI and 33,923 controls) found that patients prescribed aspirin and any NSAID (doses not assessed for either treatment) had a lower risk for MI than those who did not take aspirin and/or NSAIDs (OR: 0.74; 95% CI: 0.57–0.97). In addition, individuals taking ibuprofen plus aspirin in this study had a lower OR for MI (OR: 0.69; 95% CI: 0.42–1.15) than did those taking aspirin with an NSAID other than ibuprofen (OR: 0.76; 95% CI: 0.56–1.04).Citation75
There have been case reports in which ibuprofen may have precipitated an asthma exacerbation in adults and children with aspirin-sensitive asthma,Citation76–Citation79 possibly as a result of increased leukotriene synthesis in response to COX inhibition and related depletion of protective prostaglandins.Citation78,Citation80 The risk of ibuprofen-sensitive asthma was low (~2%) in a small RCT (N=100) of children with asthma and no known aspirin or ibuprofen sensitivity, suggesting that the prevalence of ibuprofen-sensitive asthma in the general population of asthmatics is also low.Citation81 In a large RCT in asthmatic children with febrile illness and no known sensitivity or bronchospastic reactivity to aspirin or other NSAIDs (N=1,879), Lesko et al found no more hospital admissions (RR: 0.63; 95% CI: 0.25–1.6) and actually fewer outpatient consultations for asthma symptoms or exacerbation.Citation43
Warfarin
As a class, NSAIDs are not prone to a direct pharmacodynamic interaction with anticoagulants such as warfarin; however, concurrent use of NSAIDs and antithrombotics may further increase the likelihood of GI bleeding.Citation82 A Danish cohort study (N=4,204) found that anticoagulants alone increased the risk of GI bleeding (standardized incidence ratio [SIR]: 4.0; 95% CI: 2.8–5.6), and risk was further increased by concomitant use of acetaminophen (SIR: 4.4; 95% CI: 1.2–11.4) or non-aspirin NSAIDs (SIR: 8.0; 95% CI: 2.1–20.4; no specific NSAIDs or doses reported).Citation83 Metabolism of S-warfarin, the most clinically relevant warfarin isomer,Citation84 occurs via CYP2C9.Citation85 Ibuprofen and other NSAIDs are also substrates of CYP2C9Citation85 and may thus increase anticoagulant activity by delaying S-warfarin metabolism.Citation86 Therefore, it may be prudent to avoid prescription-strength NSAIDs in patients receiving warfarin. In contrast, one of the metabolites of acetaminophen (N-acetyl-para-benzoquinone-imine) interferes with enzymes involved in the vitamin K cycle, which ultimately can lead to reduction in synthesis of clotting factors and excessive anticoagulation.Citation87 Even with short-term use, acetaminophen given concurrently with anticoagulants may increase international normalized ratio (INR), implying an increase in bleeding risk and necessitating close INR monitoring and possible warfarin dosage adjustments.Citation88–Citation91
In conclusion, although the clinical effect of DDIs between NSAIDs and aspirin is unclear, clinicians may wish to counsel patients taking a daily aspirin to avoid chronic use of ibuprofen, which may reduce aspirin’s ability to prevent CV events.Citation92 The FDA recommends taking ibuprofen ≥8 hours before or ≥30 minutes after immediate-release (not enteric-coated) of aspirin to reduce the likelihood of a potential interaction on platelet function.Citation93 In addition, ibuprofen should be avoided in patients with known or suspected aspirin-sensitive asthma. Patients should be counseled to limit their use of OTC NSAIDs and to avoid acetaminophen while on anticoagulant therapy, the former because of the increased risk of GI bleeding with NSAIDs, however small, and the latter because of the direct interaction that would increase the risk of all-site bleeding.
Antidepressants/mood stabilizers
Antidepressants are psychiatric medications used to alleviate mood and anxiety disorders. Some antidepressants may be associated with an increased risk for bleeding, which may be additively enhanced by coadministration of NSAIDs.
Selective serotonin reuptake inhibitors and tricyclic antidepressants
Selective serotonin reuptake inhibitors (SSRIs) increase bleeding risk by inhibiting platelet adhesion and function.Citation94–Citation96 Coadministration of NSAIDs in patients taking SSRIs can substantially increase the risk of bleeding.Citation97,Citation98 A Dutch population-based cohort study (N=1,961) found that patients prescribed SSRIs plus NSAIDs were prescribed ten times more peptic ulcer drugs (proxy for GI events) than patients receiving an SSRI alone (incidence rate ratios: 12.4; 95% CI: 3.2–48.0 vs 1.2; 95% CI: 0.5–2.8, respectively).Citation98 In a case-control study utilizing a UK general practice research database to identify cases of upper GI bleeding (n=1,651) or ulcer perforation (n=248) and age/sex/time-matched controls (n=10,000), concurrent use of NSAIDs and SSRIs had a more than multiplicative effect on risk of bleeding. Compared with nonuse of both drug classes, RR (95% CI) for bleeding was 2.6 (1.7–3.8) with SSRIs, 3.7 (3.2–4.4) with NSAIDs, and 15.6 (6.6–36.6) with concurrent use of both.Citation97 NSAID dosages and durations were not evaluated individually in these studies.
Several mechanisms may account for the interaction between SSRIs and NSAIDs: 1) both classes inhibit platelet aggregation and function but via different mechanisms;Citation94,Citation99 2) a pharmacokinetic interaction in which some SSRIs inhibit CYP2C9, an enzyme responsible for the metabolism of some NSAIDs (eg, ibuprofen and diclofenac);Citation100 or 3) independent effects in which SSRIs increase symptoms and bleeding via an independent mechanism without any direct pharmacokinetic interaction (eg, by increasing gastric acid secretion).Citation101 Tricyclic antidepressants (TCAs) do not substantially inhibit CYP2C9.Citation100 In the Dutch cohort study, in contrast to the tenfold increase in risk when NSAIDs are added to SSRIs, patients receiving TCAs plus an NSAID experienced a more modest increase in GI events (incidence rate ratio: 2.5; 95% CI: 0.3–20.3) compared with those receiving TCAs alone.Citation98
Lithium
Several prescription-strength NSAIDs have been associated with substantial DDIs resulting in ADRs when coadministered with lithium. One study assessed reports of DDIs between lithium and selective COX-2 inhibitors as reported in the FDA’s Adverse Event Reporting System database as of January 2003.Citation102 Thirteen cases of increased lithium concentration were reported with rofecoxib (plasma concentration increased by 58%–448%), and five were reported with celecoxib (plasma concentration increased by 56%–99%). Increased lithium concentrations were associated with clinical AEs including tremor, nausea/vomiting, upset stomach, renal insufficiency, weakness, ataxia, increased muscle tone, dysarthria, slurred speech, lethargy, sedation, disorientation, nystagmus, and flu-like symptoms.Citation102 The DDI mechanism is unclear; however, NSAID-mediated inhibition of renal prostaglandins may decrease renal lithium excretion.Citation103 In two small studies, prescription ibuprofen (1,800 mg/d in nine patients) and naproxen (750 mg/d in six patients) increased lithium levels.Citation104,Citation105
In summary, although it is clear that prescription-strength NSAIDs should not be routinely taken with SSRIs, it is unclear whether there is sufficient increase in risk with OTC NSAIDs to warrant avoiding their occasional use with SSRIs. Evidence is currently lacking to determine whether ibuprofen or other nonselective NSAIDs administered at OTC doses and durations increase the likelihood of a DDI with lithium. Caution may be advised for older patients and those with altered renal function for whom individual dose adjustments may be necessary.
Alcohol
Alcohol intake is an independent risk factor for GI bleeding that is exacerbated in a dose-dependent manner in individuals taking NSAIDs. These additive effects may be related to a direct toxicity on the gastric mucosa, the development of esophageal varices, and decreased synthesis of coagulation factors in chronic alcoholic liver disease and cirrhosis. Kaufman et al conducted an interview-based case-control survey (N=4,169) of 1,224 inpatients in the US and Sweden with GI bleeding and 2,945 matched neighborhood controls. They found a 2.7-fold higher risk for GI bleeding in individuals who regularly took ibuprofen (at least every other day) at any dose in the week prior to the onset of hematemesis/melena and who drank any amount of alcohol (95% CI: 1.6–4.4). Occasional ibuprofen use was not associated with an increased risk of acute GI bleeding (multivariate RR estimate: 1.2; 95% CI: 0.8–1.7).Citation106 Risk for ADRs in individuals who consume three or more alcoholic drinks every day is also high with non-NSAID analgesics such as aspirin (GI bleeding) and acetaminophen (hepatic dysfunction or failure).Citation107
Herbal/nutraceutical ingredients
Herbal/nutraceutical ingredients are a potential concern primarily because patients do not routinely discuss their use with health care providers, while, in some instances, they may carry a risk of DDIs similar to pharmaceutical products.
St John’s wort
St John’s wort, Hypericum perforatum, is an herbal supplement commonly used for treatment of depression. Its active ingredient, hyperforin, inhibits uptake of serotonin, norepinephrine, and dopamine.Citation108 St John’s wort is a known inducer of multiple CYP enzymes, including CYP3A4, CYP2E1, and CYP2C19, and, as such, it has considerable potential for DDIs;Citation109 however, it does not affect CYP2C9,Citation109 an enzyme that metabolizes some NSAIDs.Citation100 A small study in healthy male volunteers (N=8) found no effect of coadministration of St John’s wort and ibuprofen on either maximum concentration or area under the plasma concentration–time curve of ibuprofen but did identify a significant 31% decrease in S-ibuprofen residence time (P=0.02).Citation110 No other reports describe a clinically relevant effect of St John’s wort on ibuprofen kinetics; therefore, occasional coadministration of OTC ibuprofen with St John’s wort should not be problematic apart from a possible interaction with platelet activity similar to that observed with SSRIs.
Ginkgo biloba
Ginkgo is an herbal therapy taken to improve memory and concentration, reduce tinnitus, and potentially treat peripheral vascular disease. The putative effects of NSAID–Ginkgo interaction are primarily anecdotal;Citation111,Citation112 for example, one case was reported of fatal intracerebral mass bleeding in a 71-year-old man taking Ginkgo and ibuprofen.Citation112 A systematic review of eight RCTs concluded that ginkgo, in and of itself, does not appear to cause clinically important changes in blood coagulation.Citation113 Although some researchers warn against coadministration of ibuprofen with Ginkgo,Citation114 others find there is insufficient evidence to support a serious health risk from combining Ginkgo and NSAIDs.Citation111
Antirheumatics/chemotherapy
Methotrexate and probenecid
Methotrexate is an antimetabolite used at high doses as a chemotherapeutic and at low doses for treatment of psoriasis and RA.Citation115 Several NSAIDs, including prescription ibuprofen and naproxen, have been found to reduce renal clearance of methotrexate,Citation10,Citation116,Citation117 which could lead to toxicity (eg, renal failure or pancytopenia), at least when methotrexate is used at high doses.Citation10 A single-case report speculated that daily use of an OTC ibuprofen product for 4 weeks reduced methotrexate excretion. Resulting methotrexate accumulation caused bone marrow depletion, which may have contributed to Pneumocystis carinii pneumonia in a patient with Crohn’s disease.Citation118 Given that renal effects have also been reported with prescription ibuprofen monotherapy,Citation119 patients taking high-dose methotrexate should avoid NSAID use, even at OTC doses. Additionally, caution should be exercised when NSAIDs are used in patients receiving low-dose methotrexate.Citation115 No other reports of clinically relevant DDIs resulting in ADRs in individuals receiving concomitant NSAIDs and chemotherapeutics or rheumatologic therapies were identified.
In a study of eight healthy volunteers, aspirin antagonized the uricosuric effect of probenecid, a treatment for gout; however, ibuprofen administration had no effect on probenecid activity.Citation120
Female health effects
Reports in the literature have suggested that NSAIDs may reduce the (now-contested) cardioprotective effect of hormone replacement therapy (HRT) and may be associated with increased risk for miscarriage.
HRT
The hypothetical interaction of NSAIDs and HRT was proposed based on results from a case-control study of women aged 50–84 years (N=8,678) who had (n=1,673) or had not (n=7,005) experienced an MI.Citation121 Women currently taking HRT (but no NSAIDs) had a reduced risk of MI (OR: 0.64; 95% CI: 0.48–0.85), whereas there was a trend toward increased risk of MI among women who took both HRT and NSAIDs (any dose; OR: 1.71; 95% CI: 1.05–2.78). The authors concluded that there was a putative cardioprotective effect of HRT alone that may be undermined by NSAIDs.Citation121 However, the benefit of HRT on long-term CV health in postmenopausal women has largely been disproven by the Women’s Health Initiative study.Citation122–Citation124 Interestingly, a recent randomized study (N=1,006) reexamining the effect of HRT on perimenopausal or recently postmenopausal women aged 45–58 years found that HRT significantly reduced CV events;Citation125 however, no association with NSAIDs was examined.
Fertility effects
The hypothesis that NSAIDs may interfere with conception was proposed to explain why some women with RA treated with long-term diclofenac were unable to conceive until after stopping diclofenac.Citation126 A Danish case-control study that included 4,268 women who had miscarried and 29,750 controls who had had live births reported an increased risk for miscarriage associated with prescription NSAID use, especially soon after NSAIDs were taken.Citation127 When study data were reassessed with a consideration for gestational age, this association was diminished in strength, but still positive.Citation128 The authors acknowledged that they could not rule out the possibility that NSAIDs may have been taken to relieve pain caused by the impending miscarriageCitation127,Citation128 (ie, a protopathic biasCitation129). A population-based cohort study of pregnant women in the Kaiser Permanente Medical Care Program in San Francisco, CA, USA (N=1,055), found that NSAIDs (doses not reported) were associated with an 80% increased risk for miscarriage (HR: 1.8; 95% CI: 1.0–3.2), with even higher risks when NSAIDs were taken close to the time of conception or for longer than 1 week.Citation130 There was a trend toward increased risk with aspirin use (HR: 1.6; 95% CI: 0.6–4.1) but no increase in risk associated with acetaminophen (HR: 1.2; 95% CI: 0.8–1.8).
While data are limited, it has been hypothesized that NSAID use may reduce fertility and increase the risk of miscarriage. It may be prudent for women who are trying to become pregnant to avoid NSAID use around the time of conception.Citation130 Additionally, prostaglandins play an important role in maintaining the patency of the fetal ductus arteriosus during the third trimester of pregnancy.Citation131 As a result, OTC ibuprofen product labeling advises consumers that:
It is especially important not to use ibuprofen during the last 3 months of pregnancy unless definitely directed to do so by a doctor because it may cause problems in the unborn child or complications during delivery.Citation29
Corticosteroids
Combined use of oral corticosteroids and NSAIDs may increase the potential for serious GI toxicity. A study of Tennessee Medicaid beneficiaries, including 1,415 patients ≥65 years of age hospitalized for peptic ulcer or upper GI bleeding and 7,063 matched controls, found that current use of oral corticosteroids was associated with a twofold higher RR of peptic ulcer disease compared with nonuse.Citation132 On further analysis, this increased risk was attributed to a 4.4-fold increased risk for peptic ulcer disease in individuals who had also taken NSAIDs (any type or dosage) compared with no elevated risk when NSAID users were excluded (RR: 1.1).Citation132 As discussed above, the Arthritis, Rheumatism, and Aging Medical Information System study found that for patients who received corticosteroids plus other concurrent therapy, the risk of serious GI events was significantly greater with acetaminophen versus ibuprofen (any dose) in patients with RA (15.0 vs 6.1 events/1,000 patient-years, respectively) or OA (12.0 vs 5.4 events/1,000 patient-years, respectively) across all comparable doses.Citation22
A limited nonclinical study suggests that an ulcerogenic potential of NSAIDs in combination with corticosteroids was seen only with a COX-1, but not a COX-2, inhibitor.Citation133 This effect may occur as a result of corticosteroid-induced reductions in arachidonic acid, reducing the substrate for COX enzymes and thus potentially increasing the gastrotoxic effect of NSAIDs.
In summary, although no specific studies have identified a clear risk for increased GI bleeding when OTC NSAIDs are coadministered with oral corticosteroids, it may be prudent for health care providers to prescribe COX-2-specific NSAIDs or counsel patients to avoid OTC NSAIDs to reduce the potential risk for GI bleeding.
Discussion
Prescription-strength ibuprofen and other NSAIDs are associated with an increased risk for GI bleeding that can be exacerbated when combined with alcohol, SSRIs, corticosteroids, and of course anticoagulants. Increased CV risk seen with some COX-2-specific inhibitors has not been observed to the same degree with prescription ibuprofen; therefore, any potential CV risk from OTC doses is likely very low. Likewise, the potential risk for renal effects with OTC ibuprofen or other NSAIDs is low. Unlike acetaminophen and aspirin, ibuprofen has a high margin of safety and is not associated with a substantial incidence of serious ADRs in cases of overdose.Citation48
Reports of ADRs resulting from DDIs between NSAIDs and various drug classes should be assessed based on a continuum of risk and consideration given to both dose and duration. DDIs reported with ibuprofen are pharmacologically driven and related to inhibition of COX enzymes. Because pharmacologic reactions are dose and duration dependent, safety data from clinical studies of prescription-strength ibuprofen or other NSAIDs used long term (as in the treatment of OA or RA) may not be directly applicable to ibuprofen for OTC dosing and duration of use.
Consideration of the continuum of risk based on dose and duration of NSAID use is especially important for patients taking several concomitant medications. Risk of ADRs correlates with number of concurrent prescriptions.Citation134 A study of Utah Medicaid recipients (N=391,890) revealed that 62% received one or more medications and 4.3% received more than seven medications in 1 month. The study authors found an 80% rate of drug-related problems among those prescribed more than seven medications; treatments for pain or inflammation were implicated in 29.1% of these problems.Citation135 Another study found that elderly, largely mobility-restricted German patients receiving home general practitioner visits (N=779) took, on average, 6.8 medications on a regular basis and that ~80% experienced a DDI, of which ~44% were considered moderately or seriously relevant. The combination of NSAIDs with thiazide or loop diuretics was the most frequently implicated in moderately relevant DDIs, accounting for 8.5% of such reactions.Citation61
This review was written to educate clinicians on potential DDI risks when OTC NSAIDs are coadministered with common medications. In many instances, studies in the medical literature report only on DDIs occurring with prescription NSAIDs and do not assess risk at OTC doses and durations. Likewise, many of the studies summarized herein are retrospective case-control studies that do not report on specific dosages or durations of use for the NSAIDs discussed. In those cases, the authors have attempted to evaluate whether these risks are clinically relevant at OTC doses and durations. In these DDIs, the concern is not so much that there might be an increase in the very low risk of ADRs associated with the OTC-dose NSAIDs, but that there could be an increase in the risk associated with very active or potentially dangerous drugs, such as oral anticoagulants or cytostatics. In most or all cases, the drugs potentially involved in a DDI are prescription drugs that are known to have a wide range of ADRs and potentially narrow therapeutic ranges. Because all of these drugs are prescribed, patients will see a health care provider upon the occasion of the prescription. It is the health care provider’s responsibility to inform the patient about the potential risks associated with the concurrent use of OTC NSAIDs for pain or pyrexia and to warn them against prolonged use or use at higher than recommended OTC doses.
Conclusion
NSAIDs such as ibuprofen are generally safe and effective for individuals seeking an OTC analgesic/antipyretic. Reports of ADRs arising from DDIs with NSAIDs and common medications occurred primarily in studies of prescription-strength NSAIDs. The pharmacologic basis of these interactions strongly suggests that low-dose, short-term use of OTC NSAIDs such as ibuprofen should be safe for relief of occasional pain and fever, especially in young, healthy individuals. More caution is warranted in elderly patients with OA or RA, especially those already treated with prescription doses of NSAIDs and those taking an ACEI or diuretic (including spironolactone for heart failure) or low-dose aspirin for prevention of CV events; it may be prudent to advise such patients to avoid use of even short-term OTC NSAIDs unless they are under close medical supervision. Health care providers can be instrumental in educating all patients that using the lowest effective dose of OTC NSAIDs for the shortest required duration is vital to balancing efficacy and safety.
Acknowledgments
Editorial/medical writing support was provided by John O’Flaherty, PhD, of ProEd Communications, Inc., and Lauren Cerruto and John H Simmons, MD, of Peloton Advantage, LLC, and was funded by Pfizer Inc.
Disclosure
Nicholas Moore is an employee of Bordeaux University and Bordeaux University Hospital. The department he heads has worked or is working with, or has received funds from, Abbott Laboratories, ADDS, AFRETH, Aptalis, Arkopharma, Asahi, AstraZeneca, Aventis, Axcan, Baxter, Bayer, Berkem, Bial, Bioalliance, Biopharma, BMS, BNIA, Boehringer Ingelheim, Boots, Caviar de France, Chaine Thermale du Soleil, Celgene, Cephalon, Daiichi Sankyo, Eli Lilly and Company, Ethicon, Eugénie-les-Bains, Expanscience, Génévrier, Genopharm, GlaxoSmith-Kline, Grunenthal, Guerbet, Helsinn, Horus Pharma, I3, Innothera, Ipsen, Janssen-Cilag, Johnson & Johnson, Leo Pharma, Lundbeck, Meda Pharmaceuticals, Medtronic, Merck & Co, Merck Serono, Norgine, Novartis, Novartis Family Health, Novo Nordisk, Nycomed, Orion Corporation, Pfizer, Pfizer FHC, Pierre Fabre, Procter and Gamble, Reckitt Benckiser, Roche, Sanofi, Schering-Plough, Servier, Stallergènes, Takeda, Teva, UCB, Vivalis, Vivatec, Warner Chilcott, Wyeth, and Xanodyne Pharmaceuticals. In addition, public funding for specific projects has been received from the Seventh Framework Program (FP7 [EU]), European Medicines Agency, French Agency for the Safety of Health Products (AFSSAPS), National Agency for the Safety of Medicines and Health Products (MSNA), Directorate General of the Supply of Care (DGOS), French National Authority for Health (HAS), Clinical Research Hospital Program (PHRC), Interregional Delegation of Clinical Research (DIRC), Delegation of Clinical Research and Innovation (DRCi), and University Hospital Center (CHU). Dr Moore has acted as a consultant for AstraZeneca, Aventis, Baxter, Boots, GlaxoSmithKline, Helsinn, Novartis, Pfizer, Reckitt Benckiser, Roche, and other pharmaceutical companies. He holds no stock or other financial interest in any pharmaceutical company. Charles Pollack and Paul Butkerait are employees of Pfizer Consumer Healthcare. The authors report no other conflicts of interest in this work.
References
- Naprelan® (naproxen sodium) [package insert]San Diego, CAVictory Pharma, Inc2009
- Orudis® (ketoprofen) [package insert]Philadelphia, PAWyeth Pharmaceuticals Inc2007
- HershEVMoorePARossGLOver-the-counter analgesics and antipyretics: a critical assessmentClin Ther200022550054810868553
- SchiffMMinicMComparison of the analgesic efficacy and safety of nonprescription doses of naproxen sodium and Ibuprofen in the treatment of osteoarthritis of the kneeJ Rheumatol20043171373138315229960
- RainsfordKDFifty years of ibuprofen: advancing pain and fever managementInt J Clin Pract Suppl20131781223163541
- CooperSASchachtelBPGoldmanEGelbSCohnPIbuprofen and acetaminophen in the relief of acute pain: a randomized, double-blind, placebo-controlled studyJ Clin Pharmacol19892911102610302689471
- SchachtelBPFillingimJMThodenWRLaneACBaybuttRISore throat pain in the evaluation of mild analgesicsClin Pharmacol Ther19884467047113197368
- RaoPKnausEEEvolution of nonsteroidal anti-inflammatory drugs (NSAIDs): cyclooxygenase (COX) inhibition and beyondJ Pharm Pharm Sci200811281s110s19203472
- FreedmanMDDrug interactions: classification and systematic approachAm J Ther19952643344311850688
- HaasDAAdverse drug interactions in dental practice: interactions associated with analgesics, Part III in a seriesJ Am Dent Assoc1999130339740710085663
- DuongMSalvoFParienteAUsage patterns of ‘over-the-counter’ vs prescription-strength nonsteroidal anti-inflammatory drugs in FranceBr J Clin Pharmacol201477588789524102791
- KoffemanARValkhoffVECelikSHigh-risk use of over-the-counter non-steroidal anti-inflammatory drugs: a population-based cross-sectional studyBr J Gen Pract201464621e191e19824686883
- GutthannSPGarcía RodríguezLARaifordDSIndividual nonsteroidal antiinflammatory drugs and other risk factors for upper gastrointestinal bleeding and perforationEpidemiology19978118249116088
- SchoenfeldPKimmeyMBScheimanJBjorkmanDLaineLReview article: nonsteroidal anti-inflammatory drug-associated gastrointestinal complications – guidelines for prevention and treatmentAliment Pharmacol Ther199913101273128510540041
- HenryDLimLLGarcia RodriguezLAVariability in risk of gastrointestinal complications with individual non-steroidal anti-inflammatory drugs: results of a collaborative meta-analysisBMJ19963127046156315668664664
- HenryDMcGettiganPEpidemiology overview of gastrointestinal and renal toxicity of NSAIDsInt J Clin Pract Suppl2003135434912723747
- DerrySLokeYKRisk of gastrointestinal haemorrhage with long term use of aspirin: meta-analysisBMJ200032172701183118711073508
- WeilJColin-JonesDLangmanMProphylactic aspirin and risk of peptic ulcer bleedingBMJ199531069838278307711618
- LewisSCLangmanMJLaporteJRMatthewsJNRawlinsMDWiholmBEDose-response relationships between individual nonaspirin nonsteroidal anti-inflammatory drugs (NANSAIDs) and serious upper gastrointestinal bleeding: a meta-analysis based on individual patient dataBr J Clin Pharmacol200254332032612236853
- MooreNVanganseELeparcJ-MThe PAIN study: Paracetamol, Aspirin and Ibuprofen New tolerability study: a large-scale, randomised clinical trial comparing the tolerability of aspirin, ibuprofen and paracetamol for short-term analgesiaClin Drug Investig19991828998
- MooreNCharlesworthAVan GanseERisk factors for adverse events in analgesic drug users: results from the PAIN studyPharmacoepidemiol Drug Saf200312760161014558184
- FriesJFBruceBRates of serious gastrointestinal events from low dose use of acetylsalicylic acid, acetaminophen, and ibuprofen in patients with osteoarthritis and rheumatoid arthritisJ Rheumatol200330102226223314528521
- RichyFBruyereOEthgenOTime dependent risk of gastrointestinal complications induced by non-steroidal anti-inflammatory drug use: a consensus statement using a meta-analytic approachAnn Rheum Dis200463775976615194568
- BlotWJMcLaughlinJKOver the counter non-steroidal anti- inflammatory drugs and risk of gastrointestinal bleedingJ Epidemiol Biostat20005213714210890286
- LewisJDKimmelSELocalioARRisk of serious upper gastrointestinal toxicity with over-the-counter nonaspirin nonsteroidal anti-inflammatory drugsGastroenterology200512961865187416344055
- Hippisley-CoxJCouplandCLoganRRisk of adverse gastrointestinal outcomes in patients taking cyclo-oxygenase-2 inhibitors or conventional non-steroidal anti-inflammatory drugs: population based nested case-control analysisBMJ200533175281310131616322018
- MooreNSalvoFDuongMBlinPParienteACardiovascular risks associated with low-dose ibuprofen and diclofenac as used OTCExpert Opin Drug Saf201413216717924256349
- Summary Minutes of the Joint Arthritis Advisory Committee and Drug Safety and Risk Management Advisory Committee Meeting February 10–11, 2014Silver Spring, MDFood and Drug Administration; Center for Drug Evaluation and Research2014 Available from: http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/ArthritisAdvisoryCommittee/UCM395527.pdfAccessed September 10, 2014
- Advil® (ibuprofen) [package insert]Madison, NJPfizer Consumer Healthcare2012
- Aleve® (naproxen sodium) [package insert]Whippany, NJBayer HealthCare Consumer Care2014
- Safety Alerts for Human Medical Products: Vioxx (rofecoxib) Sep 2004 [webpage on the Internet]Silver Spring, MDU.S. Food and Drug Administration [updated August 21, 2013]. Available from: http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHu-manMedicalProducts/ucm166532.htmAccessed October 11, 2013
- CaldwellBAldingtonSWeatherallMShirtcliffePBeasleyRRisk of cardiovascular events and celecoxib: a systematic review and meta-analysisJ R Soc Med200699313214016508052
- SolomonDHAvornJStürmerTGlynnRJMogunHSchneeweissSCardiovascular outcomes in new users of coxibs and nonsteroidal antiinflammatory drugs: high-risk subgroups and time course of riskArthritis Rheum20065451378138916645966
- FosbølELGislasonGHJacobsenSRisk of myocardial infarction and death associated with the use of nonsteroidal anti-inflammatory drugs (NSAIDs) among healthy individuals: a nationwide cohort studyClin Pharmacol Ther200985219019718987620
- Hippisley-CoxJCouplandCRisk of myocardial infarction in patients taking cyclo-oxygenase-2 inhibitors or conventional non-steroidal anti-inflammatory drugs: population based nested case-control analysisBMJ20053307504136615947398
- GislasonGHRasmussenJNAbildstromSZIncreased mortality and cardiovascular morbidity associated with use of nonsteroidal anti-inflammatory drugs in chronic heart failureArch Intern Med2009169214114919171810
- LipworthLFriisSBlotWJA population-based cohort study of mortality among users of ibuprofen in DenmarkAm J Ther200411315616315133529
- WeirMRRenal effects of nonselective NSAIDs and coxibsCleve Clin J Med200269Suppl 1SI53SI5812086295
- FarquharWBMorganALZambraskiEJKenneyWLEffects of acetaminophen and ibuprofen on renal function in the stressed kidneyJ Appl Physiol (1985)19998625986049931196
- SchneiderVLévesqueLEZhangBHutchinsonTBrophyJMAssociation of selective and conventional nonsteroidal antiinflammatory drugs with acute renal failure: a population-based, nested case-control analysisAm J Epidemiol2006164988188917005625
- FureySAVargasRMcMahonFGRenovascular effects of nonprescription ibuprofen in elderly hypertensive patients with mild renal impairmentPharmacotherapy19931321431488469621
- GriffinMRYaredARayWANonsteroidal antiinflammatory drugs and acute renal failure in elderly personsAm J Epidemiol2000151548849610707917
- LeskoSMMitchellAAAn assessment of the safety of pediatric ibuprofen. A practitioner-based randomized clinical trialJAMA1995273129299337884951
- LeskoSMMitchellAARenal function after short-term ibuprofen use in infants and childrenPediatrics199710069549579374563
- UlinskiTGuigonisVDunanOBensmanAAcute renal failure after treatment with non-steroidal anti-inflammatory drugsEur J Pediatr2004163314815014745553
- WongWCowardRJMorrisMCIbuprofen induced acute renal failure in an infantN Z Med J2001114114043111700753
- KovesiTASwartzRMacDonaldNTransient renal failure due to simultaneous ibuprofen and aminoglycoside therapy in children with cystic fibrosisN Engl J Med1998338165669424574
- VolansGMonaghanJColbridgeMIbuprofen overdoseInt J Clin Pract Suppl2003135546012723749
- VeltriJCRollinsDEA comparison of the frequency and severity of poisoning cases for ingestion of acetaminophen, aspirin, and ibuprofenAm J Emerg Med1988621041073355621
- PalmerRWeissRZusmanRMHaigAFlavinSMacDonaldBEffects of nabumetone, celecoxib, and ibuprofen on blood pressure control in hypertensive patients on angiotensin converting enzyme inhibitorsAm J Hypertens200316213513912559680
- GurwitzJHEverittDEMonaneMThe impact of ibuprofen on the efficacy of antihypertensive treatment with hydrochlorothiazide in elderly personsJ Gerontol A Biol Sci Med Sci1996512M74M798612107
- HoustonMCWeirMGrayJThe effects of nonsteroidal anti-inflammatory drugs on blood pressures of patients with hypertension controlled by verapamilArch Intern Med199515510104910547748048
- BhagatKEffects of non-steroidal anti-inflammatory drugs on hypertension control using angiotensin converting enzyme inhibitors and thiazide diureticsEast Afr Med J2001781050750911921591
- ThakurVCookMEWallinJDAntihypertensive effect of the combination of fosinopril and HCTZ is resistant to interference by nonsteroidal antiinflammatory drugsAm J Hypertens1999129 Pt 192592810509552
- MacDonaldTMRichardDLheritierKKrammerGThe effects of lumiracoxib 100 mg once daily vs ibuprofen 600 mg three times daily on the blood pressure profiles of hypertensive osteoarthritis patients taking different classes of antihypertensive agentsInt J Clin Pract201064674675520518950
- LapiFAzoulayLYinHNessimSJSuissaSConcurrent use of diuretics, angiotensin converting enzyme inhibitors, and angiotensin receptor blockers with non-steroidal anti-inflammatory drugs and risk of acute kidney injury: nested case-control studyBMJ2013346e852523299844
- PavlicevićIGlavaskiMRumboldtMRumboldtZProhypertensive effects of non-steroidal anti-inflammatory drugs are mostly due to vasoconstrictionColl Antropol201135381782222053561
- AyalasomayajulaSTchaloyanSYehCMA study of the pharmacokinetic interactions of the direct renin inhibitor aliskiren with allopurinol, celecoxib and cimetidine in healthy subjectsCurr Med Res Opin200824371772618234150
- VerhammeKMosisGDielemanJStrickerBSturkenboomMSpironolactone and risk of upper gastrointestinal events: population based case-control studyBMJ2006333756333016840442
- MascleeGMValkhoffVEColomaPMRisk of upper gastrointestinal bleeding from different drug combinationsGastroenterology2014147478479224937265
- HoffmannWvan den BergNThyrianJRFissTFrequency and determinants of potential drug–drug interactions in an elderly population receiving regular home visits by GPs – results of the home medication review in the AGnES-studiesPharmacoepidemiol Drug Saf201120121311131821919114
- KlassenDGoodfriendTLSchunaAAYoungDYPetersonCAAssessment of blood pressure during treatment with naproxen or ibuprofen in hypertensive patients treated with hydrochlorothiazideJ Clin Pharmacol199333109719788227469
- PavlicevićIKuzmanićMRumboldtMRumboldtZInteraction between antihypertensives and NSAIDs in primary care: a controlled trialCan J Clin Pharmacol2008153e372e38218953082
- PatersonCAJacobsDRasmussenSYoungbergSPMcGuinnessNRandomized, open-label, 5-way crossover study to evaluate the pharmacokinetic/pharmacodynamic interaction between furosemide and the non-steroidal anti-inflammatory drugs diclofenac and ibuprofen in healthy volunteersInt J Clin Pharmacol Ther201149847749021781648
- WebsterJInteractions of NSAIDs with diuretics and beta-blockers mechanisms and clinical implicationsDrugs198530132412863124
- DaviesJGRawlinsDCBussonMEffect of ibuprofen on blood pressure control by propranolol and bendrofluazideJ Int Med Res19881631731813044869
- GroverSACoupalLZowallHTreating osteoarthritis with cyclooxygenase-2-specific inhibitors: what are the benefits of avoiding blood pressure destabilization?Hypertension2005451929715545508
- Catella-LawsonFReillyMPKapoorSCCyclooxygenase inhibitors and the antiplatelet effects of aspirinN Engl J Med2001345251809181711752357
- MackenzieISCoughtrieMWMacDonaldTMWeiLAntiplatelet drug interactionsJ Intern Med2010268651652921073556
- SaxenaABalaramnavarVMHohlfeldTSaxenaAKDrug/drug interaction of common NSAIDs with antiplatelet effect of aspirin in human plateletsEur J Pharmacol20137211–321522424075938
- KimmelSEBerlinJAReillyMThe effects of nonselective non-aspirin non-steroidal anti-inflammatory medications on the risk of nonfatal myocardial infarction and their interaction with aspirinJ Am Coll Cardiol200443698599015028354
- KurthTGlynnRJWalkerAMInhibition of clinical benefits of aspirin on first myocardial infarction by nonsteroidal antiinflammatory drugsCirculation2003108101191119512939216
- MacDonaldTMWeiLEffect of ibuprofen on cardioprotective effect of aspirinLancet2003361935757357412598144
- PatelTNGoldbergKCUse of aspirin and ibuprofen compared with aspirin alone and the risk of myocardial infarctionArch Intern Med2004164885285615111370
- FischerLMSchliengerRGMatterCMJickHMeierCRCurrent use of nonsteroidal antiinflammatory drugs and the risk of acute myocardial infarctionPharmacotherapy200525450351015977911
- AntonicelliLTagliabracciAAsthma death induced by ibuprofenMonaldi Arch Chest Dis19955042762787550206
- GorayaJSVirdiVSTo the editor: Exacerbation of asthma by ibuprofen in a very young childPediatr Pulmonol200132326211536457
- MerrittGJSelleRIJrCross-reactivity between aspirin and ibuprofen in an asthmatic – a case reportAm J Hosp Pharm1978351012451248696734
- SzczeklikANizankowskaEMastalerzLSzaboZAnalgesics and asthmaAm J Ther20029323324311941383
- PalmerGMA teenager with severe asthma exacerbation following ibuprofenAnaesth Intensive Care200533226126515960412
- DebleyJSCarterERGibsonRLRosenfeldMReddingGJThe prevalence of ibuprofen-sensitive asthma in children: a randomized controlled bronchoprovocation challenge studyJ Pediatr2005147223323816126056
- MellemkjaerLBlotWJSørensenHTUpper gastrointestinal bleeding among users of NSAIDs: a population-based cohort study in DenmarkBr J Clin Pharmacol200253217318111851641
- JohnsenSPSørensenHTMellemkjoerLHospitalisation for upper gastrointestinal bleeding associated with use of oral anticoagulantsThromb Haemost200186256356811522004
- HirshJDalenJEDeykinDPollerLOral anticoagulants. Mechanism of action, clinical effectiveness, and optimal therapeutic rangeChest19921024 Suppl312S326S1345417
- P450 Drug Interaction Table [webpage on the Internet]Indianapolis, INIndiana University [updated July 12, 2013; cited April 12, 2013]. Available from: http://medicine.iupui.edu/clinpharm/ddis/table.aspxAccessed March 21, 2015
- GreenblattDJvon MoltkeLLInteraction of warfarin with drugs, natural substances, and foodsJ Clin Pharmacol200545212713215647404
- ThijssenHHSouteBAVervoortLMClaessensJGParacetamol (acetaminophen) warfarin interaction: NAPQI, the toxic metabolite of paracetamol, is an inhibitor of enzymes in the vitamin K cycleThromb Haemost200492479780215467911
- MahéICaulinCBergmannJFDoes paracetamol potentiate the effects of oral anticoagulants?: a literature reviewDrug Saf200427532533315061686
- MahéIBertrandNDrouetLParacetamol: a haemorrhagic risk factor in patients on warfarinBr J Clin Pharmacol200559337137415752384
- MahéIBertrandNDrouetLInteraction between paracetamol and warfarin in patients: a double-blind, placebo-controlled, randomized studyHaematologica200691121621162717145598
- ZhangQBal-dit-SollierCDrouetLInteraction between acetaminophen and warfarin in adults receiving long-term oral anticoagulants: a randomized controlled trialEur J Clin Pharmacol201167330931421191575
- MacDonaldTMWeiLIs there an interaction between the cardiovascular protective effects of low-dose aspirin and ibuprofen?Basic Clin Pharmacol Toxicol200698327528016611202
- Information for Healthcare Professionals: Concomitant use of Ibuprofen and Aspirin [webpage on the Internet]Silver Spring, MDU.S. Food and Drug Administration2006 [updated August 14, 2013; cited April 12, 2013]. Available from: http://www.fda.gov/Drugs/Drug-Safety/PostmarketDrugSafetyInformationforPatientsandProviders/ucm125222.htmAccessed March 21, 2015
- SerebruanyVLSelective serotonin reuptake inhibitors and increased bleeding risk: are we missing something?Am J Med2006119211311616443409
- HallbäckIHäggSErikssonACWhissPAIn vitro effects of serotonin and noradrenaline reuptake inhibitors on human platelet adhesion and coagulationPharmacol Rep201264497998323087151
- Bismuth-EvenzalYGonopolskyYGurwitzDIancuIWeizmanARehaviMDecreased serotonin content and reduced agonist-induced aggregation in platelets of patients chronically medicated with SSRI drugsJ Affect Disord20121361–29910321893349
- de AbajoFJRodríguezLAMonteroDAssociation between selective serotonin reuptake inhibitors and upper gastrointestinal bleeding: population based case-control studyBMJ199931972171106110910531103
- de JongJCvan den BergPBTobiHde Jong-van den BergLTCombined use of SSRIs and NSAIDs increases the risk of gastrointestinal adverse effectsBr J Clin Pharmacol200355659159512814454
- SchaferAIEffects of nonsteroidal antiinflammatory drugs on platelet function and systemic hemostasisJ Clin Pharmacol19953532092197608308
- ZullinoDFKhazaalYIncreased risk of gastrointestinal adverse effects under SSRI/NSAID combination may be due to pharmacokinetic interactionsBr J Clin Pharmacol200559111811915606451
- AndradeCSandarshSChethanKBNageshKSSerotonin reuptake inhibitor antidepressants and abnormal bleeding: a review for clinicians and a reconsideration of mechanismsJ Clin Psychiatry201071121565157521190637
- PhelanKMMosholderADLuSLithium interaction with the cyclooxygenase 2 inhibitors rofecoxib and celecoxib and other non-steroidal anti-inflammatory drugsJ Clin Psychiatry200364111328133414658947
- FinleyPRWarnerMDPeabodyCAClinical relevance of drug interactions with lithiumClin Pharmacokinet19952931721918521679
- RaghebMPowellALLithium interaction with sulindac and naproxenJ Clin Psychopharmacol1986631501543711365
- RaghebMIbuprofen can increase serum lithium level in lithium-treated patientsJ Clin Psychiatry19874841611633558329
- KaufmanDWKellyJPWiholmBEThe risk of acute major upper gastrointestinal bleeding among users of aspirin and ibuprofen at various levels of alcohol consumptionAm J Gastroenterol199994113189319610566713
- Food and Drug Administration, HHSOrgan-specific warnings; internal analgesic, antipyretic, and antirheumatic drug products for over-the-counter human use; final monograph. Final ruleFed Regist20097481193851940919507324
- MüllerWESingerAWonnemannMHafnerURolliMSchäferCHyperforin represents the neurotransmitter reuptake inhibiting constituent of hypericum extractPharmacopsychiatry199831Suppl 116219684943
- BorrelliFIzzoAAHerb-drug interactions with St John’s wort (Hypericum perforatum): an update on clinical observationsAAPS J200911471072719859815
- BellECRavisWRLloydKBStokesTJEffects of St John’s wort supplementation on ibuprofen pharmacokineticsAnn Pharmacother200741222923417284505
- IzzoAAErnstEInteractions between herbal medicines and prescribed drugs: an updated systematic reviewDrugs200969131777179819719333
- MeiselCJohneARootsIFatal intracerebral mass bleeding associated with Ginkgo biloba and ibuprofenAtherosclerosis2003167236712818420
- SavovicJWiderBErnstEEffects of Ginkgo biloba on blood coagulation parameters: a systematic review of randomised clinical trialsEvidence-Based Integrative Medicine200523167176
- ChavezMLJordanMAChavezPIEvidence-based drug – herbal interactionsLife Sci200678182146215716427091
- Methotrexate sodium [package insert]Lake Zurich, ILFresenlus Kabi USA, LLC2013
- TracyTSKrohnKJonesDRBradleyJDHallSDBraterDCThe effects of a salicylate, ibuprofen, and naproxen on the disposition of methotrexate in patients with rheumatoid arthritisEur J Clin Pharmacol19924221211251618240
- KremerJMHamiltonRAThe effects of nonsteroidal antiinflammatory drugs on methotrexate (MTX) pharmacokinetics: impairment of renal clearance of MTX at weekly maintenance doses but not at 7.5 mgJ Rheumatol19952211207220778596147
- EganLJDrug interactions in gastroenterology: mechanisms, consequences, and how to avoidClin Gastroenterol Hepatol20042972573015354272
- MurrayMDBlackPKKuzmikDDAcute and chronic effects of nonsteroidal antiinflammatory drugs on glomerular filtration rate in elderly patientsAm J Med Sci199531051881977485222
- BrooksCDUlrichJEEffect of ibuprofen or aspirin on probenecid-induced uricosuriaJ Int Med Res1980842832857409302
- García RodríguezLAEganKFitzGeraldGATraditional nonsteroidal anti-inflammatory drugs and postmenopausal hormone therapy: a drug–drug interaction?PLoS Med200745e15717518513
- HeissGWallaceRAndersonGLWHI InvestigatorsHealth risks and benefits 3 years after stopping randomized treatment with estrogen and progestinJAMA200829991036104518319414
- RossouwJEAndersonGLPrenticeRLWriting Group for the Women’s Health Initiative InvestigatorsRisks and benefits of estrogen plus progestin in healthy postmenopausal women: principal results from the Women’s Health Initiative randomized controlled trialJAMA2002288332133312117397
- MansonJEChlebowskiRTStefanickMLMenopausal hormone therapy and health outcomes during the intervention and extended poststopping phases of the Women’s Health Initiative randomized trialsJAMA2013310131353136824084921
- SchierbeckLLRejnmarkLToftengCLEffect of hormone replacement therapy on cardiovascular events in recently postmenopausal women: randomised trialBMJ2012345e640923048011
- MendonçaLLKhamashtaMANelson-PiercyCHuntBJHughesGRNon-steroidal anti-inflammatory drugs as a possible cause for reversible infertilityRheumatology (Oxford)200039888088210952743
- NielsenGLSørensenHTLarsenHPedersenLRisk of adverse birth outcome and miscarriage in pregnant users of non-steroidal anti-inflammatory drugs: population based observational study and case-control studyBMJ2001322728126627011157526
- NielsenGLSkriverMVPedersenLSørensenHTDanish group reanalyses miscarriage in NSAID usersBMJ2004328743110914715618
- HorwitzRIFeinsteinARThe problem of “protopathic bias” in case-control studiesAm J Med19806822552587355896
- LiDKLiuLOdouliRExposure to non-steroidal anti-inflammatory drugs during pregnancy and risk of miscarriage: population based cohort studyBMJ2003327741136812919986
- MajedBHKhalilRAMolecular mechanisms regulating the vascular prostacyclin pathways and their adaptation during pregnancy and in the newbornPharmacol Rev201264354058222679221
- PiperJMRayWADaughertyJRGriffinMRCorticosteroid use and peptic ulcer disease: role of nonsteroidal anti-inflammatory drugsAnn Intern Med199111497357402012355
- KataokaHHorieYKoyamaRNakatsugiSFurukawaMInteraction between NSAIDs and steroid in rat stomach: safety of nimesulide as a preferential COX-2 inhibitor in the stomachDig Dis Sci20004571366137510961716
- JacubeitTDrischDWeberERisk factors as reflected by an intensive drug monitoring systemAgents Actions Suppl1990291171252316432
- LaFleurJMcBethCGunningKOderdaLSteinvoortCOderdaGMPrevalence of drug-related problems and cost-savings opportunities in medicaid high utilizers identified by a pharmacist-run drug regimen review centerJ Manag Care Pharm200612867768517269846