
Abstract
This study examined the associations of diabetes-related distress (DRD), depressive symptoms, health-related quality of life (HRQoL), and medication adherence with glycemia, blood pressure (BP), and lipid biomarkers in adults with type 2 diabetes mellitus (T2D). This cross-sectional study was conducted in three Malaysian public health clinics in 2012–2013, recruited adult patients (aged ≥30 years) with T2D who had been diagnosed for more than one year, were on active follow-up, and had recent blood test results. Univariable and multivariable analyses were performed to identify significant associated factors for glycated hemoglobin (HbA1c) BP, and lipids. The response rate was 93.1% (700/752). The majority were females (52.8%), Malay (52.4%), and married (78.7%). DRD correlated with systolic BP (r= −0.16); depressive symptoms correlated with low-density lipoprotein cholesterol (r=0.12) and total cholesterol (r=0.13); medication adherence correlated with HbA1c (r= −0.14) and low-density lipoprotein cholesterol (r= −0.11); and HRQoL correlated with casual blood glucose (r= −0.11), high-density lipoprotein cholesterol (r= −0.13), and total cholesterol (r= −0.08). Multivariable analyses showed that HRQoL was significantly associated with casual blood glucose (adjusted B= −0.06, P=0.024); DRD was associated with systolic BP (adjusted B= −0.08, P=0.066); depressive symptoms were associated with low-density lipoprotein cholesterol (adjusted B=0.02, P=0.061), and medication adherence was associated with HbA1c (adjusted B= −0.11, P=0.082) and total cholesterol (adjusted B= −0.06, P=0.086). There were significant and distinctive associations of DRD, depressive symptoms, HRQoL, and medication adherence with glycemia, BP, and lipid biomarkers. Unexpected beneficial therapeutic effects of DRD on BP require further study. A multidisciplinary approach may be needed for risk management in adults with T2D at the primary care level.
Video abstract
Point your SmartPhone at the code above. If you have a QR code reader the video abstract will appear. Or use:
Introduction
It is widely known that patients living with type 2 diabetes (T2D) carry a high burden of psychosocial problemsCitation1 and psychological disorders.Citation2–Citation4 Worrying about the future, the possibility of complications, and feelings of guilt or anxiety when “off-track” with diabetes management are reported to be sources of significant distress.Citation5,Citation6
Emotional distress in people with diabetes mellitus mainly comprises diabetes-related distress (DRD) and depression.Citation7 Among adults with T2D, DRD and depression were reported to be more prevalent and persistent than other affective disorders (anxiety, panic disorders, and dysthymia) over a period of 18 months.Citation3 DRD is defined as patient concerns about disease management, support, emotional burden, and access to care, and is distinctively different from depression, which is not disease-specific or context-specific to diabetes care.Citation8–Citation10 It was suggested from previous studies that DRD could progress to depression,Citation11 a more severe form of emotional distress, which in turn causes poor self-care activity, disease control, morbidity, and mortality.Citation7,Citation12 Fisher (β=0.026)Citation10 and Aikens (adjusted β=0.34)Citation13 reported a cross-sectional relationship between DRD and control of glycated hemoglobin (HbA1c).
Since the introduction of DRD-specific scales such the Diabetes Distress Scale (DDS-17) in 2005Citation8 and the Problem Areas In Diabetes in 1995,Citation14 there have been increasing numbers of studies looking into the relationship between DRD and disease control in adults with T2D.Citation15 Nevertheless, reports of patient self-reported outcome measures, such as DRD, depression, health-related quality of life (HRQoL), and medication adherence (MA) have been few in non-Western countries. As these aspects of patient are important in self-management and disease control,Citation15–Citation17 it is paramount that their associations are studied in patients of other cultural backgrounds. The Asia-Pacific region including Malaysia has reported an increasing prevalence of T2D.Citation18 Abundant local data have shown that poor disease control and suboptimal clinical management are hard to overcome.Citation19–Citation21 This would inevitably lead to increased patient suffering and health care costs from diabetes-related complications.Citation22,Citation23
This study examined the associations of DRD, depression, MA, and HRQoL with the three main biomarkers of risk, namely glycemia, blood pressure (BP), and lipids in adults with T2D. As part of a larger study of emotional burden and its effect on disease control, MA, and quality of life in patients with T2D (EDDMQoL), it is hoped that this study would be informative regarding the associations between these variables to improve existing therapeutic strategies or provide grounds for a potential risk management intervention in these patients.
Materials and methods
This cross-sectional study was conducted from 2012 to 2013. In addition to a questionnaire on demography (age, gender, ethnicity, types of religion, degrees of religiosity, marital status, educational level, employment status, monthly income), exercise, and smoking status, we used a structured case record form to capture comorbidity (hypertension and hyperlipidemia/dyslipidemia), diabetes-related complications, duration of diabetes, glycemic status, and BP and lipid control, along with number and types of medication used. We also used another four questionnaires to evaluate DRD, depressive symptoms (DS), MA, and HRQoL. These questionnaires were prepared in three languages, ie, English, Malay, and Mandarin.
Setting
Participants were recruited from three public health clinics (Klinik Kesihatan Seri Kembangan, Klinik Kesihatan Dengkil, and Klinik Kesihatan Salak) in Malaysia. These health clinics were chosen because they are different in terms of patient sociodemographic characteristics and the geographical regions that they are situated in. The variability of the sites provided a broad range of patients in which to assess the relationships between the study variables.
Participants
We consecutively sampled all patients with T2D who came to the clinics. They were at least 30 years old and had to have been diagnosed more than one year earlier. Patients were on regular follow-up, had made at least three visits in the past year, and had recent blood results within the previous 3 months. We excluded patients who were pregnant or lactating, patients who had a psychiatric/psychological disorder that could impair judgment and memory, and patients who could not read or understand English, Malay, or Mandarin. Patients who fulfilled the criteria were approached and informed of the study, and written consent was secured before answering the questionnaires in the language they preferred. This cross-sectional study was approved by the Medical Research Ethics Committee, Ministry of Health, Malaysia.
Definitions of disease
The definition of T2D in this study was based on the following: either a documented diagnosis of T2D according to 1999 World Health Organization criteriaCitation24 or current treatment recorded in the patient’s card as consisting of lifestyle modification, oral hypoglycemic agents, or insulin. This information was obtained from patient case records.
Glycemic status comprised HbA1c and casual blood glucose (CBG). Hypertension was diagnosed if systolic BP was ≥130 mmHg or diastolic BP was ≥80 mmHg on each of two successive readings obtained by the clinic physicians.Citation25 Lipid profile consisted of low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), triglycerides, and total cholesterol. Dyslipidemia refers to either an increase or decrease in concentration of one or more plasma or serum lipids (LDL-C >2.6 mmol/L, triglycerides >1.7 mmol/L, and HDL-C <1.1 mmol/L).Citation25,Citation26 These clinical data were retrieved from the patient’s medical record using a case record form on the same day as the patient completed the questionnaires.
Definitions of diabetes-related complications
There were five diabetes-related complications in this study; three were classified as microvascular complications, ie, retinopathy, nephropathy, and diabetic foot problems; another two were classified as macrovascular complications, ie, ischemic heart disease and cerebrovascular disease or stroke. These complications were retrieved from patients’ records. Diabetic foot problems comprised foot deformity, current ulcer, amputation, peripheral neuropathy, or peripheral vascular disease.
Diabetes-related distress
DRD was measured using the validated DDS-17.Citation8 This instrument assesses problems and difficulties concerning diabetes during the previous month on a Likert scale from 1 (not a problem) to 6 (a very serious problem).Citation8,Citation27 The DDS-17 yields a total diabetes distress scale score plus four subscale scores that address different types of distress, ie, emotional burden, physician-related distress (PD), regimen-related distress, and diabetes-related interpersonal distress.Citation8 A local translation and validation study of the Malay version of the DDS-17 showed high internal consistency (Cronbach’s α=0.94), and the test-retest reliability value was 0.33 (P=0.009). There was a significant association between mean DDS-17 item score categories (<3 versus ≥3) and HbA1c categories (<7% versus ≥7%, χ2=4.20; P=0.048). [under a journal’s review].
Depressive symptoms
Symptoms of depression were measured using the 9-item Patient Health Questionnaire (PHQ-9), which has been shown to have good construct and criterion validity in diagnosing and assessing the severity of depression.Citation28 The PHQ-9 refers to symptoms experienced by patients during the 2 weeks prior to answering the questionnaire. As a severity measure, the PHQ-9 scores range from 0 to 27. A PHQ-9 score of 0–4 suggests none to minimal depression, 5–9 indicates mild depression, 10–14 indicates moderate depression, 15–19 indicates moderately severe depression, and 20–27 indicates severe depression. The Malay version of the PHQ-9 had been locally validated, with acceptable psychometric properties.Citation29 The reported sensitivity was 87% (95% confidence interval [CI] 71–95), the specificity was 82% (CI 74–88), the positive likelihood ratio was 4.8 (CI 3.2–7.2), and the negative likelihood ratio was 0.16 (CI 0.06–0.40).Citation29
Medication adherence
The 8-item Morisky Medication Adherence Scale (MMAS-8) was used to measure MA. The MMAS-8 is reliable (Cron-bach’s α=0.83), with a sensitivity of 93% and a specificity of 53%,Citation30 and the Malay version of the MMAS-8 has been locally validated, showing a significant relationship between MMAS-8 categories and HbA1c categories (χ2=20.261; P≤0.001).Citation31 The MMAS-8 enquires about patient’s experiences with medications during the 2 weeks prior to answering the questionnaire. The total scale has a range of 0–8, including low adherence (<6), medium adherence (6–7), and high adherence (8).
Health-related quality of life
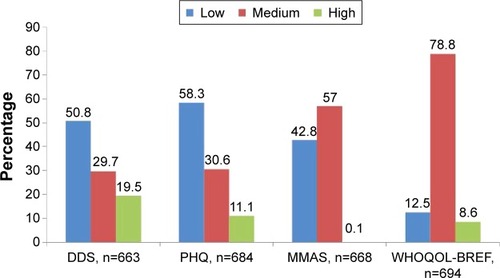
The World Health Organization Quality of Life-Brief (WHOQOL-BREF) produces four HRQoL domains and scores,Citation32 ie, a physical domain, a psychological domain, a social relationships domain, and an environment domain.Citation32 There are two items that examine overall HRQoL separately: question 1 asks about an individual’s overall perception of quality of life and question 2 asks about an individual’s overall perception of his or her health. Higher scores denote higher quality of life. We arbitrarily categorized this variable into three using a 0–100 score, ie, 0–49.99 (low), 50.01–74.99 (medium), or 75–100 (high, ).
Figure 1 Proportion of patients according to the categories of diabetes-related distress, depressive symptoms, medication adherence, and health-related quality of life.
Statistical analysis
The sample size was calculated using G*Power 3.1.2 software.Citation33 Using an estimated relationship effect of r=0.16 between DRD and HbA1c,Citation10,Citation34 a power of 0.95, and significance at 0.05, the estimated sample size was 500. Taking into consideration 30% of incomplete/missing data in the patient medical record and incomplete questionnaires returned from patients, the sample size needed to be increased to 650.
The data analyses were done using PASW version 21.0 (SPSS, Chicago, IL, USA). Descriptive analyses were conducted to characterize the sample, and distributions were visually and quantitatively examined for normality of distribution. Since all the independent variables included were based on past studies, we further selected potential demographic and medical confounders from the univariable analyses. The dependent variables were HbA1c, CBG, systolic BP, diastolic BP, LDL-C, HDL-C, triglycerides, and total cholesterol. The associations of these disease control variables were analyzed using multivariable regression analyses, with potential confounders included in the model and using the criterion of two-tailed P<0.05. Missing data were not imputed because the available data and sample size were deemed adequately powered as evidence by the normal distributions of all the dependent variables as well as the main independent variables (DRD, DS, MA, and HRQoL). As the DDS-17 and PHQ-9 scores were moderately correlated (r=0.51, P<0.0001), they were evaluated both alone and when the other was adjusted for, because their multicol-linearity could distort their individual regression coefficients. Outliers were checked with std (standardized) residual, making sure that the minimum and maximum values did not exceed ±3. There were fewer than five outliers identified in the analyses, and as all the outliers were validated, we included all of them in the analyses. All statistical assumptions were checked and confirmed within acceptable limits.
Results
The participants’ response rate was 93.1% (700/752). The majority were females (52.8%), Malay (52.9%), married or living with partners (79.2%), had non-tertiary education (89.1%), and were earning <RM 3,000 per month (94.5%); most of the patients had some exercise and were non-smokers (). About 80% were reported to have hypertension, but use of antihypertensives was almost 90%. A similar observation was noted for dyslipidemia, with almost doubled percentage use of lipid-lowering agents compared to the prevalence of dyslipidemia (). Use of antiplatelet agents corresponded to the prevalence of complications. shows the sociodemographic characteristics of the patients according to biomarkers of disease. shows the differences in clinical parameters and mean scores for the DDS-17, PHQ-9, WHOQOL-BREF, and MMAS-8 in the three health clinics. shows the proportion of patients according to the categories of DDS-17, PHQ-9, MMAS-8, and WHOQOL-BREF. DRD and DS showed a descending pattern of distribution, with most patients reported to have mild symptoms. With regard to MA, almost all patients reported low to medium adherence with their medication. In terms of HRQoL, the majority of patients experienced a medium level of quality of life ().
Table 1 Sociodemographic characteristic according to the health clinics
Table 2 Clinical variables according to the health clinics
In Pearson correlation analysis, the DDS-17 score correlated with systolic BP (r= −0.157, P<0.001), diastolic BP (r= −0.083, P<0.05), and HDL-C (r=0.105, P<0.05). The PD subscale score showed a significant correlation with triglycerides (r= −0.095, P<0.05) whereas the total DDS-17 score did not show any correlation. The PHQ-9 score correlated with CBG (r=0.087, P<0.05), LDL-C (r=0.115, P<0.001), HDL-C (r=0.118, P<0.001), and total cholesterol (r=0.134, P<0.001). The MMAS-8 score correlated with HbA1c (r= −0.136, P<0.001), CBG (r= −0.088, P<0.05), diastolic BP (r= −0.130, P<0.001), LDL-C (r= −0.105, P<0.05), and total cholesterol (r= −0.136, P<0.001). Total WHOQOL-BREF score correlated with CBG (r= −0.111, P<0.001), HDL-C (r= −0.125, P<0.001), and total cholesterol (r= −0.084, P<0.05). Patient age showed a significant correlation with all disease control biomarkers except for CBG (Pearson r values ranged from −0.279 to 0.133). Diabetes duration (in years) correlated with HbA1c (r=0.212, P<0.001), CBG (r=0.109, P<0.001), diastolic BP (r= −0.196, P<0.001), LDL-C (r= −0.106, P<0.05), and HDL-C (r=0.138, P<0.001).
shows the adjusted effects of DDS-17 (and PD), PHQ-9, WHOQOL-BREF, and MMAS-8 on disease bio-markers. WHOQOL-BREF had significant effect on CBG (adjusted B= −0.06, P=0.024). Other associations that had near significant effects included MMAS-8 on HbA1c, DDS-17 on systolic BP, PHQ-9 on LDL-C, PD on triglycerides, and WHOQOL-BREF and MMAS-8 on total cholesterol.
Table 3 Determinants of disease biomarkers
Discussion
This study examined the associations of DRD, DS, HRQoL, and MA with glycemia, BP, and lipid biomarkers in adults with T2D. There have been very few studies that have investigated these four patient self-reported outcomes in adults with T2D and a multicultural Asian background or their associations with the three important disease status variables (HbA1c, BP, and lipids) in a single setting.
Sociodemographic characteristics, including age, gender, and ethnicity and their associations with disease control were similar to those in previous reports.Citation35–Citation37 In contrast with other cross-sectional data from India,Citation38 Japan,Citation39 and the USA,Citation10,Citation13 we did not observe any association between DRD or DS and HbA1c. Similarly, the associations of age, gender, ethnicity, diabetes duration, and medication use with glycemia, BP, and lipid control were not in parallel with earlier registry-based studies.Citation21,Citation35–Citation37,Citation40 This could be due to small differences in subgroups of these variables in this study or expanded power in the registry-based studies due to their very large sample size. The lack of an association between DRD and glucose biomarkers might indicate the relatively small effects of DRD, which were further diluted after adjusting for other sociodemographic variables. It is possible that DRD was a psychological state of coping (similar to the effects of DDS-17 on systolic BP, and the PD subscale on triglycerides, see below) and not related to failure of self-management that could affect HbA1c. Further studies are needed to look into the role of DRD in self-management of diabetes in patients with different sociocultural backgrounds, relationship to illness perception, coping, MA, and HRQoL.Citation41
The most intriguing results in this study were the higher DRD and the lower systolic BP, higher PD, and lower triglycerides. This consistent trend of DRD with disease biomarkers was marked, with the PD subscale showing the highest (among the DDS-17, PHQ-9, and MMAS-8) and most consistent negative correlation with HbA1c, systolic and diastolic BP, and triglycerides. A plausible explanation for these observations is that DRD might indicate a state of psychological reaction or active coping by patients, resulting in heightened self-management. It is not uncommon for doctors in health clinics to become impatient with patients who do not adhere to advice, talk less even when patients ask for more explanation, and display indifference to patients during busy clinic days.Citation42,Citation43 In these situations, health conscious and capable patients might become distressed, which in turn motivates themselves towards self-care. This indirect and apparent effect of DRD on systolic BP, which is a form of psychological distress related to diabetes management, needs further investigation. Earlier studies reported that DRD was associated with poor diabetes self-care,Citation44–Citation46 and to our best knowledge, none of these studies had made a similar association between DRD and systolic BP. Further research is needed to confirm this hypothesis, and should include measures that assess self-care activity, self-efficacy, coping, and physician behaviors at the same time.
Compared with the DDS-17, which assesses diabetes-specific emotional distress, the PHQ-9 which measures DS and thus implies higher severity of an emotional distress,Citation7 had shown more associations with the disease biomarkers. The presence of stronger associations between the PHQ-9, LDL-C, and total cholesterol suggests that DS affects lipid control more than DRD. A similar finding was reported in the USA, ie, after multivariable analysis, DRD was associated only with HbA1c and not with BP or LDL-C.Citation47 However, in a study from Lithuania, significant correlations were found between scores for emotional state (tension-anxiety, depression-dejection, and confusion-bewilderment) and lipid levels (total cholesterol, triglycerides, and low-density lipoprotein cholesterol) in patients with T2D, especially women.Citation48 It is less clear whether there is any physiological link between DRD or DS and lipid metabolism compared to that is known between these emotional distress with glucose and BP.Citation12,Citation49 Hence, DRD or DS might influence disease control through changed self-care activityCitation50 and health behavior, such as dietary choices, physical exercise, and adherence with therapy.Citation51 It was possible that factors related to the local health clinics themselves, such as accessibility, comfort, health care system, attitudes of health care providers, and availability of drugsCitation52 could affect disease control, as shown by a further reduction in effect size (>10%) after controlling for the health clinic variable.
The results for MA and disease control was consistent with those of previous studies showing a prevalent association and positive effects of MA on disease control biomarkers.Citation53,Citation54 Higher MA was consistently shown to be associated with HbA1c, CBG, LDL-C, and total cholesterol. The direct and potent effects of medications on these biomarkers would be expected. However, loss of MA’s effects after controlling for covariates would suggest that disease control is multifactorial.Citation54 Indirectly, the results of this study show that other outcome measures or confounders should also be considered for DRD and DS in achieving disease control, such as diabetes self-care activity, HRQoL, and diabetes-specific quality of life.Citation55,Citation56 In other words, holistic diabetes care that considers both appropriate use of medications and supporting the psychological states/behaviors of patients would constitute effective diabetes care.
HRQoL as measured by WHOQOL-BREF was the only variable that had a significant effect on CBG after controlling for the other covariates. The other near significant effect of HRQoL was on total cholesterol. It is not unexpected that better HRQoL contributes to better glycemic and lipid control. Previous studies have reported a prevalent association of poor HRQoL with high HbA1c, BP, and lipids.Citation57–Citation59 In addition to the probable mechanisms mentioned above, it is possible that HRQoL itself could have salutogenic effects on disease control.Citation60 This means that patients with better HRQoL would be more capable in terms of self-management, emotional well-being, and social engagement. These attributes would further translate into better health literacy and adherence to therapy, and lead to better disease control. However, the selective effect of HRQoL on CBG is hard to explain in this study. We hypothesize that patients with higher HRQoL adopt selective self-management measures depending on their perceived needs. They might implement glucose control measures more strongly in days leading up to a medical visit at the health clinic but be less stringent at other times. This possibility is suggested by the negative correlation between WHOQOL-BREF score and other disease control biomarkers. However, the small effect sizes of these observations in spite of the relatively large sample size in this study casts doubt regarding the presence of any real or clinically significant relationship between HRQoL and disease control in relatively healthy adult patients with T2D attending these public health clinics.
Limitations and strengths
There are some limitations to this study. The strict inclusion criteria might have led to selection of a study population that was healthier, more adherent, and had better disease control, given that patients who do not turn up regularly for their appointments or have recent blood investigations might consist of those with poorer psychological well being and disease control. In addition, missing data could have been occurred in differential ways across the different category of outcomes, and as such, complete case analyses strategy as adopted in this study might affect the results and conclusions. However, we believe these biases are minimal, given that the distributions (distributions) of DRD, DS, HRQoL, and MA were all normal, and the distributions of disease control biomarkers were also normally distributed, indicating inclusion of a spectrum of disease biomarkers in the study population. The DDS-17, used in this study to measure DRD, may have inadequacies similar to those found with many standardized measures of diabetes distress,Citation14 including lack of comprehensiveness with regard to assessment of sources of diabetes distress; for example, distress attributable to starting insulin, emergence of a new complication, or the accumulated demands and burdens of self-care. This problem might have constrained the scope of T2D’s impacts on the patients.
The strength of this study includes its real-world setting, high response rate, and good sample size. A further strength is that the study population is representative of the wider T2D patient population in this country, which enables generalization of the current findings.Citation61
Conclusion
This study has shown associations of DRD, DS, HRQoL, and MA with glycemia, BP, and lipid biomarkers in adults with T2D at the primary care level. DS, MA, and HRQoL showed the expected associations with many disease biomarkers, except between DRD and BP. Efforts to increase MA may improve disease control more effectively than psychological interventions for DRD and DS. Therefore, the effects of DRD, DS, and HRQoL on MA are worthy of further study. DRD and DS had different effects on disease control, and might need different professional support. Lastly, the possible beneficial and therapeutic effects of DRD on BP require further study to determine the possible mechanisms underpinning this relationship.
Acknowledgments
This study was funded by the Research University Grants Scheme 2 (RUGS/04-02-2105RU). The authors acknowledge the Sepang and Petaling district health offices and officers for their support of this study and the Director-General of Health for giving permission to publish this research. They also acknowledge the World Health Organization and Harith Khalid Al-Qazaz for use of WHOQOL-BREF and the MMAS-8 Malay version, respectively. We thank Rimke Vos of the Julius Center for Health Sciences and Primary Care, University Medical Center Utrecht, the Netherlands, for her input into the initial draft of this manuscript. They would like to record their appreciation of Firdaus Mukhtar, Nor-Kasmawati Jamaludin, and Fuziah Paimin for their input during the planning of the study and assistance with data collection. Finally, they thank the staff at all the clinics for facilitating the data collection.
Disclosure
The authors report no competing interests in this work. The study sponsor had no role in the design or conduct of the study, the writing of this report, or the decision to submit it for publication.
References
- StuckeyHLMullan-JensenCBReachGPersonal accounts of the negative and adaptive psychosocial experiences of people with diabetes in the second Diabetes Attitudes, Wishes and Needs (DAWN2) StudyDiabetes Care2014372466247424973437
- Das-MunshiJStewartRIsmailKBebbingtonPEJenkinsRPrinceMJDiabetes, common mental disorders, and disability: findings from the UK National Psychiatric Morbidity SurveyPsychosom Med20076954355017636148
- FisherLSkaffMMMullanJTAreanPGlasgowRMasharaniUA longitudinal study of affective and anxiety disorders, depressive affect and diabetes distress in adults with type 2 diabetesDiabet Med2008251096110119183314
- LeeSChiuATsangAChowCCChanWBTreatment-related stresses and anxiety-depressive symptoms among Chinese outpatients with type 2 diabetes mellitus in Hong KongDiabetes Res Clin Pract20067428228816701917
- WestCMcDowellJThe distress experienced by people with type 2 diabetesBr J Community Nurs2002760661312514489
- LiCFordESZhaoGBalluzLSBerryJTMokdadAHUndertreatment of mental health problems in adults with diagnosed diabetes and serious psychological distress: the behavioral risk factor surveillance system, 2007Diabetes Care2010331061106420185747
- FisherLGonzalezJSPolonskyWHThe confusing tale of depression and distress in patients with diabetes: a call for greater clarity and precisionDiabet Med20143176477224606397
- PolonskyWHFisherLEarlesJAssessing psychosocial distress in diabetes: development of the Diabetes Distress ScaleDiabetes Care20052862663115735199
- FisherLSkaffMMMullanJTClinical depression versus distress among patients with type 2 diabetes: not just a question of semanticsDiabetes Care20073054254817327318
- FisherLMullanJTAreanPGlasgowREHesslerDMasharaniUDiabetes distress but not clinical depression or depressive symptoms is associated with glycemic control in both cross-sectional and longitudinal analysesDiabetes Care201033232819837786
- SkinnerTCCareyMECradockSDepressive symptoms in the first year from diagnosis of type 2 diabetes: results from the DESMOND trialDiabet Med20102796596720653757
- HoltRIde GrootMLuckiIHunterCMSartoriusNGoldenSHNIDDK International Conference Report on Diabetes and Depression: current understanding and future directionsDiabetes Care2014372067207725061135
- AikensJEProspective associations between emotional distress and poor outcomes in type 2 diabetesDiabetes Care20123524712478
- PolonskyWHAndersonBJLohrerPAAssessment of diabetes-related distressDiabetes Care1995187547607555499
- BerryELockhartSDaviesMLindsayJRDempsterMDiabetes distress: understanding the hidden struggles of living with diabetes and exploring intervention strategiesPostgrad Med J Epub2015331
- NozakiTMoritaCMatsubayashiSRelation between psychosocial variables and the glycemic control of patients with type 2 diabetes: a cross-sectional and prospective studyBiopsychosoc Med20093419298645
- GalloJJBognerHRMoralesKHPostEPTen HaveTBruceMLDepression, cardiovascular disease, diabetes, and two-year mortality among older, primary-care patientsAm J Geriatr Psychiatry20051374875516166403
- WhitingDRGuariguataLWeilCShawJIDF Diabetes Atlas: global estimates of the prevalence of diabetes for 2011 and 2030Diabetes Res Clin Pract20119431132122079683
- MasturaIChewBHLeePYControl and treatment profiles of 70,889 adult type 2 diabetes mellitus patients in MalaysiaInt J Collab Res Intern Med Public Health2011398113
- ChewBHCheongATMasturaIRahmanSASADiabetic hypertensive control and treatment: a descriptive report from the Audit Diabetes Control And Management (ADCM) registryMalays Fam Physician2010513413825606205
- ChewBHMasturaILeePYDeterminants of uncontrolled dyslipidaemia among adult type 2 diabetes in Malaysia: the Malaysian Diabetes Registry 2009Diabetes Res Clin Pract20129633934722305940
- IbrahimWNAljunidSIsmailACost of type 2 diabetes mellitus in selected developing countriesMalaysian Journal of Public Health Medicine2010106871
- CurrieCJMorganCLDixonSThe financial costs of hospital care for people with diabetes who have single and multiple macrovascular complicationsDiabetes Res Clin Pract20056714415115649574
- World Health OrganizationDefinition, diagnosis and classification of diabetes mellitus and its complications. Part 1: diagnosis and classification of diabetes mellitusReport no. 99.2.2013-08-22 17:19:23Geneva, SwitzerlandWorld Health Organization1999 Available from: http://apps.who.int/iris/handle/10665/66040Accessed April 6, 2015
- Ministry of Health MalaysiaManagement of type 2 diabetes mellitusPutrajaya, MalaysiaTechnology, Health Section, Assessment Division, Medical Development2009 Available from: http://www.moh.gov.my/attachments/3878.pdfAccessed April 7, 2015
- American Diabetes AssociationStandards of medical care in diabetes – 2015Diabetes Care201538S1S9325537700
- FisherLHesslerDMPolonskyWHMullanJWhen is diabetes distress clinically meaningful? Establishing cut points for the Diabetes Distress ScaleDiabetes Care20123525926422228744
- KroenkeKSpitzerRLWilliamsJBThe PHQ-9: validity of a brief depression severity measureJ Gen Intern Med20011660661311556941
- SherinaMSArrollBGoodyear-SmithFCriterion validity of the PHQ-9 (Malay version) in a primary care clinic in MalaysiaMed J Malaysia20126730931523082424
- MoriskyDEAngAKrousel-WoodMWardHJPredictive validity of a medication adherence measure in an outpatient settingJ Clin Hypertens200810348354
- Al-QazazHKHassaliMAShafieAASulaimanSASundramSMoriskyDEThe eight-item Morisky Medication Adherence Scale MMAS: translation and validation of the Malaysian versionDiabetes Res Clin Pract20109021622120832888
- SkevingtonSMLotfyMO’ConnellKAThe World Health Organi-zation’s WHOQOL-BREF quality of life assessment: psychometric properties and results of the international field trial. A report from the WHOQOL groupQual Life Res20041329931015085902
- FaulFErdfelderELangAGBuchnerAG*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciencesBehav Res Methods20073917519117695343
- van BastelaarKMPouwerFGeelhoed-DuijvestijnPHDiabetes-specific emotional distress mediates the association between depressive symptoms and glycaemic control in type 1 and type 2 diabetesDiabet Med20102779880320636961
- ChewBHShariff-GhazaliSMasturaIHaniffJBujangMAAge ≥60 years was an independent risk factor for diabetes-related complications despite good control of cardiovascular risk factors in patients with type 2 diabetes mellitusExp Gerontol20134848549123454736
- LeePYCheongATZaitonADoes ethnicity contribute to the control of cardiovascular risk factors among patients with type 2 diabetes?Asia Pac J Public Health20132531632522186400
- ChewBHCheongATAhmadZMasturaIMen suffer more complications from diabetes than women despite similar glycaemic control and a better cardiovascular risk profile: the ADCM study 2008J Mens Health20129190197
- MathewCSDominicMIsaacRJacobJJPrevalence of depression in consecutive patients with type 2 diabetes mellitus of 5-year duration and its impact on glycemic controlIndian J Endocrinol Metab20121676476823087861
- TsujiiSHayashinoYIshiiHDiabetes distress, but not depressive symptoms, is associated with glycaemic control among Japanese patients with type 2 diabetes: Diabetes Distress and Care Registry at Tenri (DDCRT 1)Diabet Med2012291451145522416679
- ChewBHMasturaIShariff-GhazaliSDeterminants of uncontrolled hypertension in adult type 2 diabetes mellitus: an analysis of the Malaysian Diabetes Registry 2009Cardiovasc Diabetol2012115422607105
- McSharryJMoss-MorrisRKendrickTIllness perceptions and glycaemic control in diabetes: a systematic review with meta-analysisDiabet Med2011281300131021418098
- TsigaEPanagopoulouESevdalisNMontgomeryABenosAThe influence of time pressure on adherence to guidelines in primary care: an experimental studyBMJ Open20133pii e002700
- HajosTRPolonskyWHTwiskJWDainMPSnoekFJDo physicians understand type 2 diabetes patients’ perceptions of seriousness; the emotional impact and needs for care improvement? A cross-national surveyPatient Educ Couns20118525826320932702
- OgberaAAdeyemi-DoroAEmotional distress is associated with poor self care in type 2 diabetes mellitusJ Diabetes2011334835221883978
- ZulmanDMRoslandAMChoiHLangaKMHeislerMThe influence of diabetes psychosocial attributes and self-management practices on change in diabetes statusPatient Educ Couns201287748021840149
- ThoolenBJde RidderDTBensingJMGorterKJRuttenGEPsychological outcomes of patients with screen-detected type 2 diabetes: the influence of time since diagnosis and treatment intensityDiabetes Care2006292257226217003303
- PanditAUBaileySCCurtisLMDisease-related distress, self-care and clinical outcomes among low-income patients with diabetesJ Epidemiol Community Health20146855756424489044
- LasaiteLLasieneJKazanaviciusGGostautasAAssociations of emotional state and quality of life with lipid concentration, duration of the disease, and the way of treating the disease in persons with type 2 diabetes mellitusMedicina (Kaunas)2009458594 Lithuanian19289898
- LloydCSmithJWeingerKStress and diabetes: a review of the linksDiabetes Spectrum200518121127
- BeverlyEAGandaOPRitholzMDLook who’s (not) talking: diabetic patients’ willingness to discuss self-care with physiciansDiabetes Care2012351466147222619085
- GoldenSHLazoMCarnethonMExamining a bidirectional association between depressive symptoms and diabetesJAMA20082992751275918560002
- AholaAJGroopPHBarriers to self-management of diabetesDiabet Med20133041342023278342
- BaileyCJKodackMPatient adherence to medication requirements for therapy of type 2 diabetesInt J Clin Pract20116531432221314869
- AscheCLaFleurJConnerCA review of diabetes treatment adherence and the association with clinical and economic outcomesClin Ther2011337410921397776
- TanMYMagareyJSelf-care practices of Malaysian adults with diabetes and sub-optimal glycaemic controlPatient Educ Couns20087225226718467068
- CarperMMTraegerLGonzalezJSWexlerDJPsarosCSafrenSAThe differential associations of depression and diabetes distress with quality of life domains in type 2 diabetesJ Behav Med20143750151023515932
- KiadaliriAANajafiBMirmalek-SaniMQuality of life in people with diabetes: a systematic review of studies in IranJ Diabetes Metab Disord2013125424354933
- WandellPEQuality of life of patients with diabetes mellitus. An overview of research in primary health care in the Nordic countriesScand J Prim Health Care200523687416036544
- PapadopoulosAAKontodimopoulosNFrydasAIkonomakisENiakasDPredictors of health-related quality of life in type II diabetic patients in GreeceBMC Public Health2007718617663782
- VentegodtSOmarHAMerrickJQuality of life as medicine: interventions that induce salutogenesis. A review of the literatureSoc Indic Res2011100415433
- Non-Communicable Disease Section, Disease Control Division, Department of Public HealthNational Diabetes Registry Report, Volume 1:1: 2009-20122013 Available from: file:///C:/Users/susan/Downloads/National_Diabetes_Registry_Report_Vol_1_2009_2012.pdfAccessed April 7, 2015