
Abstract
Objective
The aim of this study was to investigate QT dispersion (QTd), which is the noninvasive marker of ventricular arrhythmia and sudden cardiac death, and P-wave dispersion, which is the noninvasive marker of atrial arrhythmia, in patients with conversion disorder (CD).
Patients and methods
A total of 60 patients with no known organic disease who were admitted to outpatient emergency clinic and were diagnosed with CD after psychiatric consultation were included in this study along with 60 healthy control subjects. Beck Anxiety Inventory and Beck Depression Scale were administered to patients and 12-lead electrocardiogram measurements were obtained. Pd and QTd were calculated by a single blinded cardiologist.
Results
There was no statistically significant difference in terms of age, sex, education level, socioeconomic status, weight, height, and body mass index between CD patients and controls. Beck Anxiety Inventory scores (25.2±10.8 and 3.8±3.2, respectively, P<0.001) and Beck Depression Scale scores (11.24±6.15 and 6.58±5.69, respectively, P<0.01) were significantly higher in CD patients. P-wave dispersion measurements did not show any significant differences between conversion patients and control group (46±5.7 vs 44±5.5, respectively, P=0.156). Regarding QTc and QTd, there was a statistically significant increase in all intervals in conversion patients (416±10 vs 398±12, P<0.001, and 47±4.8 vs 20±6.1, P<0.001, respectively).
Conclusion
A similar relation to that in literature between QTd and anxiety and somatoform disorders was also observed in CD patients. QTc and QTd were significantly increased compared to the control group in patients with CD. These results suggest a possibility of increased risk of ventricular arrhythmia resulting from QTd in CD patients. Larger samples are needed to evaluate the clinical course and prognosis in terms of arrhythmia risk in CD patients.
Keywords:
Introduction
Some psychiatric disorders are known to be correlated with cardiological disorders. There are a number of studies in literature examining the relationship between anxiety disorders and P-wave dispersion (Pd),Citation1 which is considered as an indirect indicator of atrial fibrillation (AF), and QT dispersion (QTd),Citation2 which is considered as an indirect indicator of ventricular arrhythmia.Citation3–Citation5 As well as anxiety disorders, heart rhythm disturbances have been observed in patients with somatoform disorders and a correlation between heart rate and psychiatric conditions is thought to exist.Citation6,Citation7 Conversion disorder (CD) is a type of somatoform disorder according to Diagnostic and Statistical Manual of Mental Disorders (DSM-IV-TR). CD is defined as loss of function or decreased or increased function in motor, sensory, and neurovegetative system organs without an organic cause.Citation8 According to DSM-IV-TR, diagnosis of CD can be made only when functional impairment cannot be explained by neurological and other medical conditions or drug effects and is associated with psychological factors, is not malingering or merely pain or sexual dysfunction, and causes significant distress and impairment of psychological and occupational functioning.Citation9
In our country, 12%–47% of those admitted to psychiatric emergency clinics have CD.Citation10,Citation11 Although a common disease, it is often overlooked or incorrectly treated. Because CD can mimic many other disorders, medical errors may occur during diagnosis.Citation12,Citation13 It is difficult to diagnose CD because its symptoms may get confused with other psychiatric and somatic disorders.Citation11 Here we aimed to investigate the risk of ventricular arrhythmia and AF in patients with CD who often visit emergency rooms with intense anxiety and somatization symptoms.
Methods
A total of 60 patients admitted to general emergency outpatient clinic whose blood count, routine biochemistry, and thyroid hormone profile were at normal range were included and cardiology consultations were made with a preliminary diagnosis of CD. All examination findings were normal, no organic pathology was found, none of the patients were on medication, and the patients were diagnosed with CD by a psychiatrist using structured interview for DSM-IV psychiatric disorders (Structured Clinical Interview for DSM-IV Axis I Disorders – Clinical Version). Also 60 healthy control subjects were included, and written informed consent was taken from all subjects.
The selected population, according to inclusion criteria, included patients who were between 18 and 45 years of age, were literate, and had a diagnosis of CD according to DSM-IV-TR and agreed to participate in the study.
Exclusion criteria were having mental retardation; alcohol and substance use-related disorders; anxiety disorders; mood disorders; schizophrenia and other psychotic disorder diagnosis according to DSM-IV-TR or dementia and other cognitive disorders; neurological disorders leading to unique personality traits such as epilepsy, migraine, multiple sclerosis, and Parkinson’s disease; systemic disorders leading to cognitive impairment; or general chronic medical conditions that may disrupt cardiac conduction system (especially thyroid disease, hypertension, heart valve disorders, myocardial infarction, known atherosclerotic heart disease history, congestive heart failure, cardiomyopathy, pheochromocytoma or diabetes mellitus history, etc). Also patients on continuous drugs for a chronic disease or smoking were excluded.
The control group included volunteers who agreed to participate and were physically and mentally healthy, were not using any drugs, alcohol, or psychoactive substances, and were not smoking.
Materials
A semistructured sociodemographic and clinical data form designed by us according to clinical experience and information obtained from resources considering the purpose of the study (Structured Clinical Interview for DSM-IV Axis I Disorders, Beck Anxiety Inventory, and Beck Depression Inventory) was administered. Also, 12 standard electrocardiogram (ECG) was obtained using a standardized recording device at 50 mm/s paper speed and 1 mV/cm.
Measures
Patient follow-up form (sociodemographic and clinical data collection form)
This form was completed by the researcher doctor and questions regarded patient’s age, sex, weight, height, marital status, education level, employment status, income level, health insurance type, smoking, alcohol, drug use, and psychiatric and cardiac disease history of self and family were included.
Structured Clinical Interview for DSM-IV Axis I Disorders – Clinical Version
It is a structured interview made by First et alCitation14 for DSM-IV Axis I Disorders. Validity and reliability for Turkish population were made.Citation15
Beck Anxiety Inventory
It was developed by Beck et al in 1988 because of the need for a scale to distinguish anxiety from depression.Citation16
It measures the severity of anxiety symptoms and questions subjective anxiety and somatic symptoms. It is a Likert-type (scored 0–3), self-rating scale consisting of 21 items, rating between 0 and 63. Higher total scores indicate the severity of the anxiety symptoms. Validity and reliability studies for Turkey were conducted by Ulusoy et al.Citation17
Beck Depression Inventory
It is a 21-item self-report scale developed by Beck in 1961 in order to measure emotional, cognitive, somatic, and motivational components.Citation18 The scale is composed of 21 items of which 2 of them belong to emotions, 11 of them belong to cognition, 2 of them belong to behaviors, 5 of them belong to somatic symptoms, and 1 of them belongs to interpersonal symptoms. It has a total of 21 questions. Each question scores between 0 and 3 points, and a total score ranging between 0 and 63 points is obtained. Scores between 0 and 9 indicate no/minimal, 10–18 mild, 19–29 moderate, and 30–63 severe depression. Turkish validity and reliability study of Beck Depression Inventory which was used to determine the intensity of depression was conducted by Hisli.Citation19
Electrocardiographic evaluation
Standard ECGs were taken from all patients with a sweeping rate of 50 mm/s and amplitude of 1 mV/cm. P-wave durations and the QT intervals were measured manually in all simultaneously recorded 12 leads of the surface ECG. The mean P-wave duration for at least three complexes was calculated in each lead. The onset of the P-wave is defined as the point of first visible upward slope from baseline for positive waveforms, and as the point of first downward slope from baseline for negative waveforms. The return to the baseline was considered as the end of the P-wave. The Pmax measured in any of the 12 leads of the surface ECG was used as the longest atrial conduction time. The maximum and minimum durations of P-waves (Pmax and Pmin, respectively) were detected, and the difference between Pmax and Pmin was defined as P-wave dispersion (Pd = Pmax – Pmin).
The QT interval was measured from the beginning of the QRS complex to the end of the T-wave at the level of the TP isoelectric baseline. Biphasic T-waves were measured to the time of their final return to the TP isoelectric baseline. When U-waves were present, the QT interval was measured from the beginning of the QRS complex to the nadir of the curve between the T- and U-waves. Heart rate-corrected QT (QTc) was calculated using Bazett’s formula (QTc-d, JTc-d).Citation1 The ventricular repolarization dispersions were determined by calculating the difference between maximum and minimum QT intervals on each ECG, which were termed QTd and heart rate-corrected QTd (QTcd). Extrasystolic and post-extrasystolic cycles were excluded from the measurement.
Statistical analyses
Statistical analysis was performed using the Statistical Package for Social Sciences version 15.0 software for Windows (IBM, Armonk, NY). Categorical data were expressed as frequencies. Continuous variables were presented as the mean ± standard deviation. The variances between the groups were compared with paired-samples t-test. The correlation between QTd and P-wave dispersion was analyzed using Pearson correlation analysis. P-values <0.05 were regarded as significant.
Results
A total of 60 patients diagnosed with CD according to DSM-IV-TR diagnostic criteria and 60 age- and sex-matched healthy control subjects were enrolled. In the patients group, 68.3% (n=41) were male, and in the control group, 31.7% (n=19) were female. The mean ages in the patient and the control group were 35.70±12.1 and 32.00±9.3, respectively. There was no statistically significant difference in terms of sociodemographic characteristics between patient and control groups (P>0.05) ().
Table 1 Sociodemographic characteristics of the CD patients and healthy controls
Sixty participants with conversion in sinus rhythm and 60 individuals as a control group were enrolled. The mean heart rate of the patients was 86±13 per minute. P-wave dispersion measurements did not show any significant differences between the patient and the control group (46±5.7 vs 44±5.5, P=0.156). As seen in , regarding QTc and QTd there were statistically significant increases in all intervals in patients with CD (416±10 vs 398±12, P<0.001 and 47±4.8 vs 20±6.1, P<0.001, respectively). P-wave measurements and QT parameters are set out in . The dispersion of P-wave did not show a significant correlation with QTd (r=−0.059; P=0.655).
Figure 1 QTc and QTd measurements of conversion patients and controls as figure.
Abbreviations: BAI, Beck Anxiety Inventory; BDI, Beck Depression Inventory; QTc, corrected QT; QTd, dispersion QT.
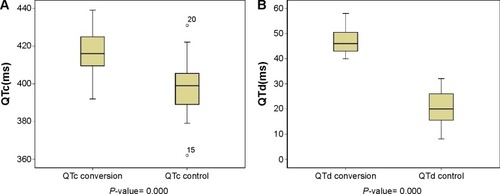
Table 2 P-wave dispersion (ms) and QT dispersion (ms) in CD patients and healthy controls
Discussion
CD is defined as a loss of function in sensory and motor organs without an organic cause.Citation20 CD may occur as part of a chronic pattern known as somatization disorder in the form of physical expression of psychological distress. As a reflection of all these developments, CD took place under the heading “somatoform disorders” in DSM-IV.Citation21 This disease has different clinical manifestations, and a study regarding the frequency of these manifestations with 86 patients revealed that 52.3% of the cases had fainting symptoms, 22.1% of the cases had short-of-breath symptoms, and 18.6% had paralysis symptoms.Citation22 CD may be seen at any age, although it is known that it is most common between 15 and 35 years of age.Citation23 Usually, it is seen by 10% of the population in developing and 13% in underdeveloped countries.Citation20 In our country, 12%–47% of psychiatric emergency admissions and 25.1% of psychiatric consultations are CD.Citation24,Citation25 Studies showed that there are no sex differences during preadolescent period; however, after puberty it is 2–19 times more frequent in women.Citation26–Citation28 In our study, female and male rates in the patient group were 68.3% and 31.7%, respectively. Before somatoform disorder diagnosis is made, the physician should carefully exclude undiagnosed general medical conditions, drug-related conditions, and other psychiatric disorders that may cause similar symptoms or simulated disorders and factitious disorders in which the patient behaves as if existing symptoms were not present. However, medical disorders other than neurological or psychiatric disorders may occur later in 25%–50% of CD patients. Therefore, it is of utmost importance to make full medical and neurological evaluation of CD patients.Citation29 One of these that may occur in anxiety and somatoform disorders is heart conduction abnormalities.
Studies investigating the relationship between anxiety disorders, somatoform disorders, and P-wave and QTd which are considered as indicators of cardiac arrhythmia are very few. Some studies suggested QTd and Pd as indicators of atrial and ventricular arrhythmias in patients with social phobia and panic disorder.Citation4,Citation30 However, similar studies with CD patients were not found. Here we aimed to evaluate P-wave and QTd and identify possible cardiac conduction abnormalities in CD in which significant somatization and anxiety symptoms were seen.
We tried to measure heart rate, rhythm, and time required for electrical activity to reach to the other side of the heart by using our ECG device.Citation31 P-waves indicate atrial depolarizationCitation32 and P-wave dispersion (Pd) indicates the difference between maximum and minimum P-wave duration.Citation33 P-wave dispersion is considered as a sensitive and specific precursor of AF in various clinical situations,Citation34 and it is reported to be used as a predictor for paroxysmal AF.Citation1 Significant variations in cardiac atrial conduction were associated with systemic autonomic symptoms seen during anxiety episodes.Citation30 In a study examining the relationship between the presence of arrhythmia in anxiety disorders and P-wave dispersion, state anxiety was found to effect Pd more than trait anxiety.Citation35 In a study with 30 patients with hypochondriasis (a type of somatoform disorder) and 30 healthy control subjects, Pd durations which were considered to be associated with anxiety were significantly higher in the patient group.Citation36 In another study with patients with panic disorder (a type of anxiety disorder) who experience intense somatic symptoms, 40 patients and controls were examined, and similarly, P-wave dispersion was found to be prolonged in panic disorder patients.Citation30 In our study, anxiety levels were similarly higher; however, there was no statistically significant difference in Pd durations between patients and controls.
Table 3 BAI and BDI scores in CD patients group and healthy group
QTd, defined as the maximal interlead difference in QT intervals on 12 leads of the surface ECG, reflects the regional heterogeneity of ventricular repolarization and has been suggested as an important marker for risk of arrhythmia in addition to the QT interval. Some investigators proposed that it might be a predisposing factor for arrhythmic events and sudden death. Studies showed that in anxiety disorders like panic disorder and social phobia, QTd was significantly higher than controls. This correlation was considered as a result of prolonged anxiety.Citation4,Citation5 In a study conducted with patients with anxiety, when autonomic innervation and QTd were examined, sympathetic activity was found to be increased, QTd was found to be prolonged, and like hypertension, these were thought to increase the occupation or sitting in the left ventricle.Citation37 In hypertension patients with higher levels of anxiety, QTd and left ventricular hypertrophy were seen to increase, and it was considered to be associated with increased sympathetic and decreased parasympathetic modulation.Citation38 In another study, anxiety levels measured by Trait and State Anxiety Inventory were considered to be a possible marker of prolonged QTd.Citation39 A relationship was found between some psychiatric disorders such as somatoform disorders and circadian heart rate.Citation6 Also, in a similar study with psychiatric patients with eating disorder, it was seen that the group with high depression and anxiety scores had a more prolonged QTd.Citation40 In a meta-analysis of five studies, it was found that individuals with higher anxiety levels had higher QTd.Citation41 QTd was found to be significantly increased in patients with Major Depressive Disorder.Citation42 Similarly, in our study, depression, anxiety, and QTd levels were significantly higher in patients than in controls.
Our study has several limitations: the number of participants studied was quite small, there is a possibility of presence of higher than normal anxiety levels in patients with CD who were admitted to emergency clinic, and QTd and Pd levels were measured manually.
In conclusion, in psychiatric disorders like generalized anxiety disorder, social phobia, panic disorder, hypochondriasis, and somatoform disorders with heart conduction abnormalities were observed in literature. Similarly, in our study CD patients were also found to have increased QTd. As prolonged QTd may predict an increased risk of ventricular arrhythmias, we believe that CD patients may benefit from being evaluated in terms of cardiological risk of arrhythmia. However, larger samples are needed to clarify the relationship between CD and cardiac conduction disorders.
Disclosure
The authors report no conflicts of interest in this work.
References
- AytemirKOzerNAtalarEDispersion on 12 lead electrocardiography in patients with paroxysmal atrial fibrillationPACE200023109112
- PerkiomakiJSKoistinenMJYli MayrySHuikuryHVDispersion of QT interval in patients with and without susceptibility to ventricular tachyarrhythmias after previous myocardial infarctionJ Am Coll Cardiol1995261741797797747
- UnsalCKaplanOKSonerSMZUzunlarBUyarelHCalıskanMPWave and QT dispersion in patients with generalized anxiety disorderKosuyolu Kalp Derg2013163214219
- NahshoniEGurSMaromSLevinJBWeizmanAHermeshHQT dispersion in patients with social phobiaJ Affect Disord2004781212614672793
- AtmacaMYavuzkirMIzciFGurokMGAdiyamanSQT wave dispersion in patients with panic disorderNeurosci Bull201228324725222622824
- StampferHGThe relationship between psychiatric illness and the circadian pattern of heart rateAust N Z J Psychiatry19983221871989588297
- BarskyAJClearyPDCoeytauxRRRuskinJNPsychiatric disorders in medical outpatients complaining of palpitationsJ Gen Intern Med1994963063138077994
- OzturkORuh sağlığı ve bozuklukları [Mental health and disorders]8th edAnkaraHekimler Yayin Birligi Press2001389425
- American Psychiatric AssociationDiagnostic and Statistical Manual of Mental DisordersFourth edWashington DC, USAAmerican Psychiatric Association2000 Text Revision
- SalgırtayAAnkara üniversitesi psikiyatri kliniğine bir yıl içinde başvuran acil hastalar üzerinde bir araştırma. Yayınlanmamış Uzmanlık Tezi [A research on emergency patients admitted within one year of the university psychiatric clinic. Unpublished Master Thesis]Ankara Üniversitesi Tıp Fakültesi [Ankara University Medical School]Ankara1979
- BedizUAydemirCBaşterziADKısaCCebeciSGökaEHekimlerin Konversiyon Bozukluğuna Yaklaşımını Etkileyen Faktörler [Affecting factors in approach to conversion disorder of physicians]Klinik Psikiyatri200477379
- AlkımTTuncaZKöroğluEKonversiyon bozukluğu. Psikiyatri Temel Kitabı [Conversion disorder. The Basic Book of Psychiatry]1st edAnkaraHekimler Yayın Birliği1997537544
- GuggenheimFGSadockBJSomatoform Disorders Kaplan and Sadock’s Synopsis of Psychiatry 7 ed, (2)PhiladelphiaLippincott Williams and Wilkins200015041514
- FirstMBSpitzerRLGibbonMStructured Clinical Interview for DSM-IV Clinical Version (SCID-I/CV)Washington D.CAmerican Psychiatric Press1997
- ÇorapçıoğluAAydemirÖYildizMDSM-IV Eksen I Bozukluklari İçin Yapilandirilmiş. Klinik Görüşme Kullanim Kilavuzu (SCID-I) Ankara, Turkey. [Structured Clinical Interview for DSM-IV, Clinical Version]TurkeyHekimler Yayın Birliği1999
- BeckATEpsteinNBrownGSteerRAAn inventory for measuring clinical anxiety: psychometric propertiesJ Consult Clin Psychol1988568938973204199
- UlusoyMŞahinNErkmenHTurkish version of Beck anxiety inventory: psychometric propertiesJ Cogni Psychother1998122163172
- BeckATAn inventory for measuring depressionArch Gen Psychiatry19617151169
- HisliNBeck Depresyon Envanterinin üniversite öğrencileri için geçerliği, güvenirliği [Validity reliability of the Beck Depression Inventory for college students]Psikoloji Derg19897313
- KaplanHISadockBJGrebbJASomatoform Disorders Synopsis of Psychiatry7th edBaltimoreWilliams and Wilkins1994617632
- SaxeGNChinmanGBerkowitzRSomatization in patients with dissociative disordersAm J Psychiatry1994151132913348067489
- ÖzenSÖzbulutÖAltındağZArıcıoğullarıZAcil serviste konver-siyon bozukluğu tanısı konan hastaların sosyodemografik özellikleri, stres faktörleri, I. ve II. Eksen eş tanıları [In the emergency department, diagnosis of conversion disorder socio-demographic characteristics of the patients, stress factors, I. and II. Axis comorbidity]Türkiye’de Psikiyatri200028796
- ChandrasekaranRGoswamiUSivakumarVChitralekhaJHysterical neurosis – a follow-up studyActa Psychiatr Scand19948978808140911
- BedizAUAydemirÇBaşterziADAttitudes of physician towards patients with conversion disorder37th National Congress of Psychiatry Congress HandbookIstanbul20017879
- CanpolatBIGökaEÖrselSSociocultural aspects of emergency psychiatry in today’s Turkey5th World Congress International Association For Emergency Psychiatry Congress Handbook1998
- ConnorKMDavidsonJRGeneralized anxiety disorder: neurobiological and pharmacotherapeutic perspectivesBiol Psychiatry199844128612949861471
- StanleyMABeckJGAnxiety disordersClin Psychol Rev2000201473175410983266
- UzbayİTAnksiyetenin nörobiyolojisi [Neurobiology of anxiety]Klinik Psikiyatri Dergisi20025suppl1513
- RoelofsKNaringGWMoeneFCHoogduinCAThe question of symptom lateralization in conversion disorderJ Psychosom Res200049212511053600
- YavuzkirMAtmacaMDagliNP wave dispersion in panic disorderPsychosom Med20076934434717510287
- WagnerGSDursunANMarrıott’un Pratik Elektrokardiyografisi [Marriott’s Pratic Electrocardiography]10th ed2001264
- CastellanosAKesslerMKMyerburgRJThe resting electrocardiogramSclantCRAlexanderRWHurst’s The HeartNew YorkMcGraw-Hill1994321
- DilaverisPEGialafosEJClinical and electrocardiographic predictors of recurrent atrial fibrillationPacing Clin Electrophysiol200023335235810750136
- DilaverisPEGialafosEJP wave dispersion: a novel predictor of paroxysmal AFAnn Noninvasive Electrocardiol2001615916511333174
- UyarelHKasikciogluHDayiSUAnxiety and P wave dispersion in a healthy young populationCardiology200510416216816131805
- AtmacaMKorkmazHKorkmazSP wave dispersion in patients with hypochondriasisNeurosci Lett2010485314815020813155
- PiccirilloGViolaEBuccaCQT interval dispersion and autonomic modulation in subjects with anxietyJ Lab Clin Med1999133546146810235129
- PiccirilloGElviraSViolaEAutonomic modulation of heart rate and blood pressure in hypertensive subjects with symptoms of anxietyClin Sci19989543529662484
- UyarelHOkmenECobanoğluNKarabulutACamNEffects of anxiety on QT dispersion in healthy young menActa Cardiol2006611838716485737
- TakimotoYYoshiuchiKAkabayashiAEffect of mood states on QT interval and QT dispersion in eating disorder patientsPsychiatry Clin Neurosci200862218518918412841
- KelmansonIAHigh anxiety in clinically healthy patients and increased QT dispersion: a meta-analysisEur J Prev Cardiol201421121568157423945038
- NahshoniEAizenbergDStrasbergBQT dispersion in the surface electrocardiogram in elderly patients with major depressionJ Affect Disorder200060197200