
Abstract
Background
The aim of the present study was to investigate the association between tumor necrosis factor-alpha (TNF-α) gene G-238A polymorphism and risk of coronary artery disease (CAD) using a meta-analytical approach.
Methods
The PubMed and Embase databases were searched for relevant publications up to January 13, 2015. Four authors (XPH, XDZ, XTZ, and ZJZ) independently selected the studies, extracted, and analyzed the data using the Comprehensive Meta-Analysis software. The sensitivity and subgroups analyses were also performed. Either a fixed effects or a random effects model was used to estimate pooled odds ratios (ORs) and their 95% confidence intervals (CIs).
Results
Finally, ten articles including eleven case-control studies involving 4,222 patients and 4,832 controls were yielded. The results indicated no significant association between G-238A polymorphism and CAD risk (A vs G: OR =1.08, 95% CI =0.89–1.30; AA vs GG: OR =1.15, 95% CI =0.59–2.25; GA vs GG: OR =1.14, 95% CI =0.88–1.48; AA vs [GG + GA]: OR =1.09, 95% CI =0.56–2.14; (GA + AA) vs GG: OR =1.11, 95% CI =0.90–1.38). In the subgroup analyses, similar results were obtained with overall populations. The sensitivity analyses showed that the overall results were robust. No publication bias was detected.
Conclusion
Based on current evidence, we can conclude that TNF-α G-238A polymorphism might not be associated with CAD risk.
Introduction
Tumor necrosis factor-alpha (TNF-α) is an inflammatory mediator that plays important roles in inflammatory and immune responses.Citation1 Several single-nucleotide polymorphisms (SNPs) have been identified in the TNF-α promoter.Citation2 Of these SNPs, conversion from guanine (G) to adenine (A) in the promoter at position-308 (rs1800629) and -238 (rs361525) has been intensively studied for these allelic variations showing functional significance.Citation3,Citation4 Many studies have identified that the TNF-α G-308A and/or G-238A are associated with many human diseases,Citation5–Citation8 including coronary artery disease (CAD).Citation9,Citation10 Of these diseases, the association between these two polymorphisms and some diseases were identified via a meta-analytical approach, from which inconsistent results can be pooled from original studies and a more precise results can be provided.Citation11
CAD is also named as ischemic heart disease or coronary heart disease, mainly including stable angina pectoris, unstable angina pectoris, and myocardial infarction.Citation12,Citation13 Serum levels of TNF-α are elevated in patients with CAD and might modify the risk for developing CAD events since it affects endothelial cell hemostatic function.Citation14 Hence, we can hypothesize that TNF-α gene polymorphisms might be involved in the CAD susceptibility. In 1998, Herrmann et al performed a case-control study in France and Northern Ireland population, and the results showed that the TNF-α gene G-308A and G-238A polymorphisms were unlikely to contribute to CAD risk in an important way.Citation15 Since then, many epidemiological studies have been published and inconsistent results have been revealed. The association between TNF-α G-308A polymorphism and CAD risk has been investigated by three published meta-analyses.Citation9,Citation10,Citation16 In contrast, there is no meta-analysis on the association between TNF-α gene G-238A polymorphism and CAD risk until now. Therefore, we conducted this meta-analysis to study the overall correlation between the G-238A polymorphism and CAD susceptibility.
Materials and methods
This meta-analysis was reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement.Citation17 As meta-analysis is a secondary analysis, ethical approval is not necessary.
Eligibility criteria
According to the PICOSCitation18 approach, the publication was considered eligible if it met all the following criteria: 1) the patient was clearly diagnosed with CAD, coronary heart disease, ischemic heart disease, stable angina pectoris, unstable angina pectoris, myocardial infarction, or other CAD variants; 2) the exposure was the presence of G-238A polymorphism in the TNF-α gene; 3) the control group was healthy population or volunteers without coronary heart disease manifestations, either from hospital or community; 4) the outcome was the incidence of CAD, either fatal or nonfatal; and 5) the study was used a case-control design. Moreover, the information essential for calculating odds ratios (ORs) and relevant 95% confidence intervals (CIs) should be provided. We chose the most comprehensive report if duplicate publication or overlapped information was identified.
Information sources
The PubMed and Embase databases were searched for relevant publications up to January 13, 2015. Keywords were coronary heart disease, coronary artery disease, ischemic heart disease, angina pectoris, angina, acute coronary syndrome, myocardial infarction, myocardial infarct, polymorphism, and tumor necrosis factor or TNF. References of recent reviews, previous meta-analyses, and eligibility studies were also manually scanned. Table S1 shows the search strategy used for the PubMed.
Data collection
Two authors (XPH and ZJZ) independently retrieved and selected studies for inclusion according to the aforementioned eligibility criteria. Then these two authors extracted the following data from the included studies: the last name of first author and publication year, country of origin and ethnicity, endpoints of CAD, polymorphism, sample size of cases and controls, source of controls, genotype distribution of cases and controls, genotyping method, and Hardy–Weinberg equilibrium (HWE) for control. HWE was tested by χ2 test at the 50% significance level. Disagreements were resolved by discussion.
Data analysis
The ORs and corresponding 95% CIs were calculated to summarize the pooled effect sizes for G-238A polymorphism. All possible genetic models, the allelic model (A vs G), dominant model ([AG + AA] vs GG), codominant model (AA vs GG, AG vs GG), and recessive model (AA vs [AG +GG]) were used to estimate the overall relationship.
First, the heterogeneity was quantitatively evaluated using the I2 statistic.Citation19 An I2 value no larger than 25% indicates the absence of heterogeneity, so the fixed effects model was suggested; otherwise, the random effects model was used. The subgroup analysis was performed to investigate the source of heterogeneity and the difference between different ethnicities and HWE. The sensitivity analysis was conducted by sequential omission of individual studies to assess the influence of overall results.Citation20 The funnel plot and Egger’s test were used to detect the publication bias.Citation21 All the analyses were conducted using the Comprehensive Meta-Analysis software (version 2.2; Biostat, Englewood, NJ, USA).Citation22,Citation23
Results
Study selection
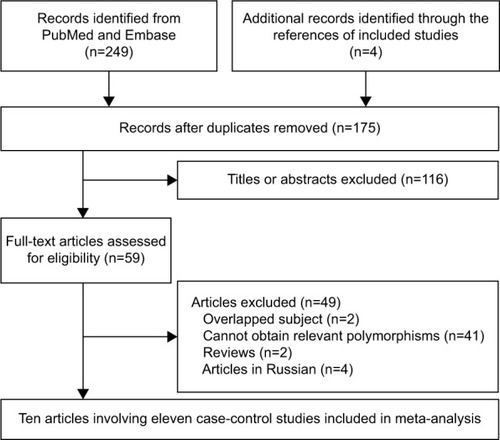
The flowchart of study selection process is shown in . A total of 253 publications were identified initially, and 175 publications were selected for further screening after removing duplicate records. After titles or abstracts were screened, a total of 59 articles preliminarily met the inclusion criteria. Four potential eligible articles were excluded because they were published in Russian and full texts could not be accessed.Citation24–Citation27 Two case-control studies identified in one articleCitation15 were considered as independent studies. From four articlesCitation28–Citation31 with overlapped population, two articlesCitation28,Citation30 presenting more comprehensive information were included. Finally, ten articles with eleven case-control studies were included in this meta-analysis.Citation15,Citation32–Citation40
Figure 1 Flowchart of study section in the meta-analysis.
Study characteristics
Eleven case-control studies involving 4,222 cases and 4,832 controls investigated G-238A polymorphism.Citation15,Citation32–Citation40 There were five studies based on Caucasian populationCitation15,Citation32,Citation33,Citation35 and six studies concerning Asian population.Citation34,Citation36–Citation40 Three of these studies were out of HWE.Citation37–Citation39 All controls were healthy population, eg, healthy visitors of patients, healthy volunteers, healthy blood donors, or outpatients confirmed negative by cardiac assessment. shows the main characteristics of all the included studies.
Table 1 Characteristics of the included studies
Meta-analysis
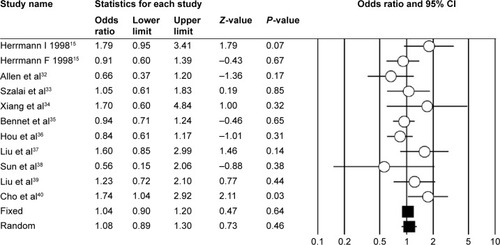
Of the eligible eleven case-control studies, one studyCitation40 reported significant association; in contrast, the other ten studies demonstrated that the association was nonsignificant (). The overall results of five genetic models all identified nonsignificant association between G-238A polymorphism and CAD risk (A vs G: OR =1.08, 95% CI =0.89–1.30, I2=34.33%, ; AA vs GG: OR =1.15, 95% CI =0.59–2.25, I2=0%; GA vs GG: OR =1.14, 95% CI =0.88–1.48, I2=54.34%; AA vs [GG + GA]: OR =1.09, 95% CI =0.56–2.14, I2=0%; [GA + AA] vs GG: OR =1.11, 95% CI =0.90–1.38, I2=41.92%).
Figure 2 Forest plot of overall population of TNF-α G-238A polymorphism and CAD risk (A vs G model).
Abbreviations: TNF-α, tumor necrosis factor-alpha; CAD, coronary artery disease; CI, confidence interval.
After being stratified by ethnicity, the results of Asian and Caucasian populations were similar to that of the overall population. The studies in HWE also revealed nonsignificant association. shows the overall and subgroup analyses results of G-238A polymorphism and CAD risk. The sensitivity analysis showed that none of the included eleven studies dramatically influenced the pooled results under all the five genetic models ().
Figure 3 Forest plot of sensitivity analysis by omitting a single study each time of overall population of TNF-α G-238A polymorphism and CAD risk (A vs G model).
Abbreviations: TNF-α, tumor necrosis factor-alpha; CAD, coronary artery disease; CI, confidence interval.
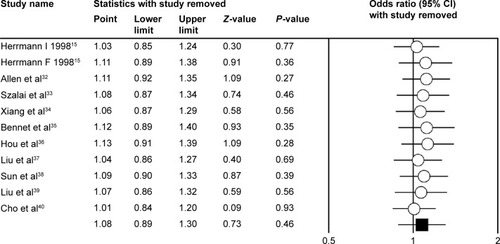
Table 2 Results of overall estimates and subgroup analysis
Publication bias
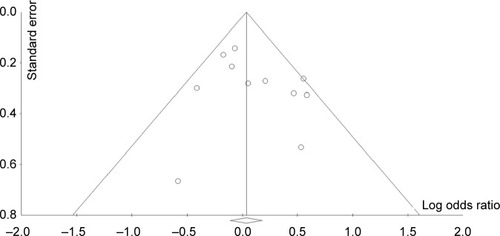
The funnel plots () and Egger’s test demonstrated that there was no publication bias in our meta-analysis (P=0.28 for A vs G; P=0.14 for AA vs GG; P=0.06 for GA vs GG; P=0.17 for AA vs [GG + GA]; P=0.12 [GA + AA] vs GG).
Figure 4 Funnel plot of standard error by log odds ratio for detection publication bias of G-238A polymorphism (A vs G model).
Discussion
CAD remains the major cause of mortality and morbidity worldwide. Smoking, diabetes, hypertension, obesity, family history, stress, hyperlipidemia, and alcohol abuse were considered the conventional risk factors of CAD; however, these conventional factors can only explain 50% of the total risk factors of CAD cases.Citation41–Citation47 Genetic factors might contribute to the other half of the total risk factors, and many polymorphisms are considered to be associated with the onset and development of CAD.Citation12,Citation46,Citation48–Citation51 Our meta-analysis focused on the TNF-α gene promoter G-238A polymorphism and revealed that this polymorphism was not associated with CAD risk. In the subgroup analyses, similar results with overall population were obtained, and the sensitivity analyses showed that the overall results were robust.
There were ten publications with eleven case-control studies focusing on the G-238A polymorphism and CAD risk in our meta-analysis. According to the result of literature search, our meta-analysis is the first meta-analysis on the G-238A polymorphism. Similar to G-308A polymorphism,Citation9,Citation10,Citation16 our result also revealed a nonsignificant association between G-238A polymorphism and risk of CAD. We also performed subgroup analysis to investigate the effects of ethnicity and HWE. Only Asian and Caucasian populations were adopted. The subgroup analysis revealed no association for Asian population, Caucasian population, and the studies in HWE. Considering the interesting phenomenon of G-308A polymorphism,Citation9,Citation10,Citation16 the G-238A polymorphism included small number of studies and needs further research. In other words, the current result is not the final result.
For this polymorphism, how many new studies should be conducted in the future remains a question. Based on current evidence, we could not judge whether the sample size was sufficient for decisive conclusion. Moreover, whether significant correlation between G-238A polymorphism and risk of CAS exists in other ethnicity, such as Africans or Turks, remains unclear. Also, the polymorphism associated with patients with CAD and concomitant diseases, such as periodontal disease,Citation52 also needs to be examined in further researches. Moreover, our meta-analysis also provides some clinical implications. We knew that, the personalized drug treatment is involved in the genetic background. Hence, development of a special drug for patients with CAD with G-238A polymorphism is not needed. However, the clinicians should advise their patients with this polymorphism to have peace of mind and not to take this polymorphism as a risk factor in the clinical work. TNF-α G-238A polymorphism might not be considered for the genetic diagnosis of CAD.
Obviously, heterogeneity was large in three genetic models. Mild heterogeneity detected in certain genetic models and subgroup analyses was only partially explained by ethnicity and HWE (). The heterogeneity is common in meta-analysis of genetic association studies,Citation23,Citation53–Citation55 and we should not ignore it since pooled results may be influenced by heterogeneity. Therefore, the substantial heterogeneity was one limitation of our meta-analysis. Second, as all the included studies were limited within Asians or Caucasians, our conclusion may not be reasonably extrapolated for other ethnic groups. Third, the sample size from eligible studies was not enough. The small sample size might influence the result. Although we tried our best to collect all the relevant studies, certain publications published in languages other than English or Chinese were excluded because of inaccessibility to the full text and/or impenetrability due to language barriers. Hence, although the test for publication bias revealed no publication bias in our meta-analysis, the bias that originated from publication bias should not be ignored. Fourth, for lacking original data of gene–gene and gene–environmental interactions and adjusted conventional risk factors, we could not further evaluate potential gene–gene and gene–environmental interactions based on adjusted ORs. Finally, for lacking appropriate methodological quality tool,Citation11 we did not assess the risk of bias of included studies. Hence, current results based on unadjusted data may be confounded to the pooled effect.
Conclusion
In conclusion, there was no evidence suggesting that TNF-α G-238A polymorphism was associated with the risk of CAD. The nonsignificant results were without ethnic difference. Due to the limitations and implications of current meta-analysis, we suggest that further well-designed studies with large sample size should be conducted to clarify the association between the polymorphisms and CAD risk, among which meta-analysis of genome-wide association studiesCitation56 is the best.
Acknowledgments
This study was supported by the National Natural Science Foundation of the People’s Republic of China (No 81273971). The funders had no roles in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Supplementary material
Table S1 The search strategy of PubMed
Disclosure
The authors report no conflicts of interest in this work.
References
- GowersIRWaltersKKiss-TothEReadRCDuffGWWilsonAGAge-related loss of CpG methylation in the tumour necrosis factor promoterCytokine201156379279722004920
- AllenRDPolymorphism of the human TNF-alpha promoter – random variation or functional diversity?Mol Immunol19993615–161017102710698305
- FalvoJVTsytsykovaAVGoldfeldAETranscriptional control of the TNF geneCurr Dir Autoimmun201011276020173386
- D’AlfonsoSRichiardiPMA polymorphic variation in a putative regulation box of the TNFA promoter regionImmunogenetics19943921501547903959
- SongGGChoiSJJiJDLeeYHAssociation between tumor necrosis factor-alpha promoter-308 A/G, -238 A/G, interleukin-6-174 G/C and -572 G/C polymorphisms and periodontal disease: a meta-analysisMol Biol Rep20134085191520323657600
- ChengKZhaoYJLiuLWanJJTumor necrosis factor-alpha 238 G/A polymorphism and risk of hepatocellular carcinoma: evidence from a meta-analysisAsian Pac J Cancer Prev20131453275327923803115
- ZhuangLMaWCaiDZhongHSunQAssociations between tumor necrosis factor-alpha polymorphisms and risk of psoriasis: a meta-analysisPLoS One2013812e6882724324571
- LiYYTumor necrosis factor-alpha g308alpha gene polymorphism and essential hypertension: a meta-analysis involving 2244 participantsPLoS One201274e3540822536381
- ZhangHFXieSLWangJFChenYXWangYHuangTCTumor necrosis factor-alpha G-308A gene polymorphism and coronary heart disease susceptibility: an updated meta-analysisThromb Res2011127540040521296384
- PereiraTVRudnickiMFrancoRFPereiraACKriegerJEEffect of the G-308A polymorphism of the tumor necrosis factor alpha gene on the risk of ischemic heart disease and ischemic stroke: a meta-analysisAm Heart J2007153582183017452160
- ZengXZhangYKwongJSThe methodological quality assessment tools for preclinical and clinical studies, systematic review and meta-analysis, and clinical practice guideline: a systematic reviewJ Evid Based Med20158121025594108
- LiebWVasanRSGenetics of coronary artery diseaseCirculation2013128101131113824002717
- GlozierNToflerGHColquhounDMPsychosocial risk factors for coronary heart diseaseMed J Aust2013199317918023909539
- PlutzkyJInflammatory pathways in atherosclerosis and acute coronary syndromesAm J Cardiol2001888101511423051
- HerrmannSMRicardSNicaudVPolymorphisms of the tumour necrosis factor-alpha gene, coronary heart disease and obesityEur J Clin Invest199828159669502188
- ChuHYangJMiSTumor necrosis factor-alpha G-308 A polymorphism and risk of coronary heart disease and myocardial infarction: a case-control study and meta-analysisJ Cardiovasc Dis Res201232849022629023
- MoherDLiberatiATetzlaffJAltmanDGGroupPPreferred reporting items for systematic reviews and meta-analyses: the PRISMA statementPLoS Med200967e100009719621072
- LiberatiAAltmanDGTetzlaffJThe PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaborationBMJ200967
- HigginsJPThompsonSGDeeksJJAltmanDGMeasuring inconsistency in meta-analysesBMJ2003327741455756012958120
- PatsopoulosNAEvangelouEIoannidisJPSensitivity of between-study heterogeneity in meta-analysis: proposed metrics and empirical evaluationInt J Epidemiol20083751148115718424475
- EggerMDavey SmithGSchneiderMMinderCBias in meta-analysis detected by a simple, graphical testBMJ199731571096296349310563
- BorensteinMHedgesLHigginsJComprehensive Meta-Analysis: A Computer Program for Meta-Analysis [Computer Program]Englewood, NJBiostat Inc2007
- YanYWengHShenZHWuLZengXTAssociation between interleukin-4 gene -590 c/t, -33 c/t, and 70-base-pair polymorphisms and periodontitis susceptibility: a meta-analysisJ Periodontol20148511e354e36225029213
- SukhininaTSShakhnovichRMBarsovaRMValue of allele gene polymorphism of the inflammation system for prognosis of patients with myocardial infarctionKardiologiia20125231521 Russian [with English abstract]22839439
- KonenkovVIShevchenkoAVProkof’evVFMaksimovVNComplex of genotypes of cytokines as a genetic factor of risk of development of myocardial infarction of in European population of Russia menKardiologiia20125272229 Russian [with English abstract]22839710
- ShevchenkoAVGolovanovaOVKonenkovVIAnalysis of polymorphism of three positions of promoter region of TNF-gene in patients with ischemic heart disease, unstable angina and myocardial infarctionKardiologiia2010502914 Russian [with English abstract]20146672
- SudomoinaMASukhininaTSBarsovaRMComplex analysis of association of inflammation genes with myocardial infarctionMol Biol (Mosk)2010443463471 Russian [with English abstract]20608170
- SzaboGVThe role and importance of gene polymorphisms in the development of atherosclerosisInterv Med Appl Sci201351465124265890
- SzaboGVAcsadyGTumornecrosis-factor-alpha 308 GA polymorphism in atherosclerotic patientsPathol Oncol Res201117485385721455632
- GhazouaniLKhalifaSBAbboudN-308G>A and -1031T>C tumor necrosis factor gene polymorphisms in Tunisian patients with coronary artery diseaseClin Chem Lab Med200947101247125119803813
- GhazouaniLBen Hadj KhalifaSAbboudNTNF-alpha -308G>A and IL-6 -174G>C polymorphisms in Tunisian patients with coronary artery diseaseClin Biochem20104313–141085108920493832
- AllenRALeeEMRobertsDHParkBKPirmohamedMPolymorphisms in the TNF-alpha and TNF-receptor genes in patients with coronary artery diseaseEur J Clin Invest2001311084385111737221
- SzalaiCFustGDubaJAssociation of polymorphisms and allelic combinations in the tumour necrosis factor-alpha-complement MHC region with coronary artery diseaseJ Med Genet2002391465111826025
- XiangPXLiYZhangPAHuangCXStudy on plasma TNFa level and TNFa polymorphisms in patients with coronary heart diseaseJian Yan Yi Xue2004195434437 Chinese [with English abstract]
- BennetAMvan MaarleMCHallqvistJAssociation of TNF-alpha serum levels and TNFA promoter polymorphisms with risk of myocardial infarctionAtherosclerosis2006187240841416243340
- HouLHuangJLuXWangLFanZGuDPolymorphisms of tumor necrosis factor alpha gene and coronary heart disease in a Chinese Han population: interaction with cigarette smokingThromb Res2009123682282618814905
- LiuYJinWLuLChenQJShenWFAssociation between single nucleotide polymorphism in tumor necrosis factor-α gene promoter and coronary heart diseaseZhen Duan Xue Li Lun Yu Shi Jian200985506509 Chinese [with English abstract]
- SunSYZengXQJinAMFanWHZhangJCAssociation of tumor necrosis factor alpha gene polymorphisms in the promoter region with chronic periodontitis and coronary heart diseaseLin Chuang Kou Qiang Yi Xue Za Zhi200955279282 Chinese [with English abstract]
- LiuYLuLWuZJChenQJShenWFJinWRelationship between tumor necrosis factor-a gene and risk of coronary artery disease in Shanghai Han populationShaghai Jiao Tong Da Xue Xue Bao (Yi Xue Ban)2011315592597 Chinese [with English abstract]
- ChoHCYuGLeeMYKimHSShinDHKimYNTNF-alpha polymorphisms and coronary artery disease: association study in the Korean populationCytokine201362110410923507260
- MuhlesteinJBSecondary prevention of coronary artery disease with antimicrobials: current status and future directionsAm J Cardiovasc Drugs20022210711814727986
- GibsonCMCannonCPGreeneRMRescue angioplasty in the thrombolysis in myocardial infarction (TIMI) 4 trialAm J Cardiol199780121269205014
- YusufSHawkenSOunpuuSINTERHEART Study InvestigatorsEffect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case-control studyLancet2004364943893795215364185
- NilssonPMNilssonJABerglundGPopulation-attributable risk of coronary heart disease risk factors during long-term follow-up: the Malmo preventive projectJ Intern Med2006260213414116882277
- EdmondsonDNewmanJDWhangWDavidsonKWEmotional triggers in myocardial infarction: do they matter?Eur Heart J201334430030623178642
- SimonASVijayakumarTMolecular studies on coronary artery disease-a reviewIndian J Clin Biochem201328321522624426215
- OhiraTIsoHCardiovascular disease epidemiology in Asia: an overviewCirc J20137771646165223803294
- XuQYuanFShenXPolymorphisms of C242T and A640G in CYBA gene and the risk of coronary artery disease: a meta-analysisPLoS One201491e8425124392120
- LinBHuangYZhangMWangJWuYAssociation between apolipoprotein C3 Sst I, T-455C, C-482T and C1100T polymorphisms and risk of coronary heart diseaseBMJ Open201441e004156
- WuZLouYLuLHeterogeneous effect of two selectin gene polymorphisms on coronary artery disease risk: a meta-analysisPLoS One201492e8815224498435
- WangXZhangJDuXSongMJiaCLiuHAssociation of A561C and G98T polymorphisms in E-selectin gene with coronary artery disease: a meta-analysisPLoS One2013811e7930124260191
- LengWDZengXTKwongJSHuaXPPeriodontal disease and risk of coronary heart disease: An updated meta-analysis of prospective cohort studiesInt J Cardiol20146947226313869
- ZengXTLiuDYKwongJSLengWDXiaLYMaoMMeta-analysis of association between interleukin-1beta C-511T polymorphism and chronic periodontitis susceptibilityJ Periodontol201586681281925741583
- ZhangLChenLMWangMNThe G894t, T-786c and 4b/a polymorphisms in Enos gene and cancer risk: a meta-analysisJ Evid Based Med20147426326925586457
- ZengXTLuoWGengPLGuoYNiuYMLengWDAssociation between the TP53 codon 72 polymorphism and risk of oral squamous cell carcinoma in Asians: a meta-analysisBMC Cancer20141446924969046
- HouLZhaoHA review of post-GWAS prioritization approachesFront Genet2013428024367376