
Abstract
Aim
The pathophysiology of slow coronary flow (SCF) involves atherosclerosis, small vessel dysfunction, platelet function disorders, and inflammation. It has been known that eosinophils also play a significant role in inflammation, vasoconstriction, thrombosis, and endothelial dysfunction. We propose to evaluate the relationship between eosinophilia and SCF.
Methods
All patients who underwent coronary angiography between January 2011 and December 2013 were screened retrospectively. Of 6,832 patients, 102 patients with SCF (66 males, mean age 52.2±11.7 years) and 77 control subjects with normal coronary angiography (50 males, mean age 50.7±8.1 years) were detected. Baseline characteristics, hematological test results, and biochemical test results were obtained from the hospital database.
Results
Baseline characteristics of the study groups were comparable between groups. There was no significant difference between groups regarding leukocyte count, paletelet count, and mean platelet volume. However, patients with SCF had a higher eosinophil count than the controls (0.24±0.17×103/μL vs 0.16±0.15×103/μL, P=0.002). In addition, eosinophil count was found to be correlated with thrombolysis in myocardial infarction (TIMI) frame count in the SCF group (r=0.3, P<0.01). There was no significant correlation between eosinophil count and the number of coronary arteries showing slow flow.
Conclusion
Patients with SCF have higher blood eosinophil count, and this may play an important role in the pathogenesis of SCF. Elevated baseline eosinophil count may indicate the presence of SCF.
Introduction
The pathophysiological mechanisms of slow coronary flow (SCF) remain undetermined. However, several hypotheses have been offered for SCF, comprising a form of early phase of atherosclerosis, small vessel dysfunction, platelet function disorders, and instability between vasoconstrictor and vasodilatory factors. Recently, inflammation has been reported to have an important role in the development of SCF phenomenon.Citation1,Citation2
Previous studies have found the incidence of SCF changing between 1% and 7% in patients undergoing angiography.Citation3 On the other hand, increased cardiovascular mortality associated with SCF has been reported.Citation4 It has also been known that eosinophils play an important role in endothelial dysfunction, thrombosis, vasoconstriction, and inflammation.Citation5,Citation6 Eosinophils stimulate the aggregation and activation of platelets. Furthermore, they relieve the formation of thrombosis through inhibition of thrombomodulin.Citation7–Citation9 Therefore, we aimed to evaluate the relationship between blood eosinophil count and SCF as well as its correlation with thrombolysis in myocardial infarction (TIMI) frame count and the number of coronary arteries showing slow flow.
Methods
Patient selection
In the present study, angiography records of 6,832 patients who underwent coronary angiography because of chest pain or objective signs of ischemia (treadmill exercise or myocardial perfusion SPECT [single photon emission computed tomography]) between January 2011 and December 2013 were retrospectively evaluated for the presence of SCF. Patients with SCF and who were proved to have normal coronary arteries (NCAs) were included as SCF group. Exclusion criteria were 1) troponin positivity; 2) coronary ectasia on coronary angiogram; 3) moderate-to-severe valvular heart disease; 4) congestive heart failure; 5) chronic renal disease (glomerular filtration rate [GFR] <60 mL/min/1.73 m2); 6) thyroid dysfunction; 7) anemia; 8) inflammatory disease; 9) active infection; 10) hypertension; 11) hyperlipidemia (low density lipoprotein [LDL] ≥160 mg/dL); 12) diabetes mellitus; 13) bronchial asthma and chronic obstructive pulmonary disease; 14) drug intake such as steroids and immunosuppressive treatment; 15) current use of cardiovascular medical therapy; 16) under the age of 40; and 17) chronic liver disease.
After applying inclusion and exclusion criteria, a total of 102 patients with SCF were included in the study. Control group comprised 77 patients with angiographically NCAs without SCF.
In addition, patients were further divided into three subgroups: one-vessel, two-vessel, and three-vessel SCF. Routinely measured clinical and laboratory parameters such as complete blood count and biochemical test results were obtained from the medical records of the patients. Venous peripheral blood samples were routinely taken on admission from all patients at hospitalization before coronary angiography. Blood samples were routinely drawn into standardized tubes containing dipotassium ethylenediaminetetraacetic acid (EDTA) and were studied within 2 hours upon arrival in the laboratory. All hematological measurements were performed using an XT-2000i analyzer (Sysmex Corporation of America, Long Grove, IL, USA). Transthoracic echocardiography was performed before coronary angiography with a Philips HD11 XE device using 2.5 MHz phased-array transducer. The left ventricular ejection fraction (LVEF) was assessed by modified Simpson’s method.Citation10
The present study was approved by the Dicle University ethics committee (Diyarbakir, Turkey) and complies with the requirements of the Declaration of Helsinki.
Coronary angiography
At our hospital, we perform coronary angiography with Judkin’s method. We give a total of 6–8 mL low osmolar contrast agent for each demonstration of right and left coronary arteries. The coronary flow rates were assessed according to the TIMI frame count (TFC) method that was previously standardized. The normal frame counts for the left-anterior descending (LAD) artery (36±2.3 frames) are 1.7 times greater than the mean for the circumflex (Cx) artery (22.2±3.8 frames) and the right coronary artery (21.7±2.8 frames). Therefore, the longer LAD frame counts were corrected by dividing by 1.7 to derive the corrected TFC as described earlier.Citation11 The mean TFC for each subject was calculated by summation of the TFCs for the LAD, Cx, and right coronary artery and then dividing the sum by 3. SCF was defined as corrected TFC >2 standard deviations (SDs) from the normal reference values.Citation11 Coronary angiograms were independently assessed by two or three cardiologists who were blinded to the clinical findings of the subjects.
Statistical analysis
SPSS statistical software, version 22.0 (IBM Corporation, Armonk, NY, USA), was used for the statistical analyses. Continuous variables are expressed as mean ± SD. Categorical variables are expressed as percentages. The normality of distribution of continuous variables was evaluated by the Kolmogorov–Smirnov test. For continuous variables, the Student t-test or Mann–Whitney U-test was used to test differences between the main groups, and the one-way analysis of variance test or Mann–Whitney U-test was used to test differences between the subgroups. Categorical data were analyzed with the χ2 test. Two-tailed P-values <0.05 were considered as statistically significant. Pearson’s or Spear-man’s correlation was used to determine the strength of the relationship between the parameters when appropriate. Linear regression analysis was used to detect independent factors affecting the presence of SCF.
Results
All records of 6,832 patients who underwent coronary angiography were retrospectively screened, of which 102 patients with SCF (mean age 52±11 years, 34 females) and 77 patients with NCAs (mean age 50±8 years, 41 females) were detected. There was no statistically significant difference between the two groups with regard to age, sex, body mass index, blood pressures, New York Heart Association classes, LVEF, glucose, tryglicerides, WBC count, platelet count, and neutrophil (). However, hemoglobin level, and eosinophil count were found to be elevated in patients with SCF when compared to those with NCA (14.8±3.4 g/L vs 13.8±1.7 g/L, P=0.03; 0.24±0.17×103/μL vs 0.16±0.15×103/μL, P=0.002, respectively) (). Eosinophil count was not significantly different among patients with one-vessel, two-vessel, and three-vessel SCF (). Eosinophil count was mildly correlated with TFC in patients with SCF (r=0.3, P=0.002; ). Regression analysis showed that eosinophil count was an independent factor for the presence of SCF ().
Figure 1 The correlation between eosinophil count and TIMI frame count.
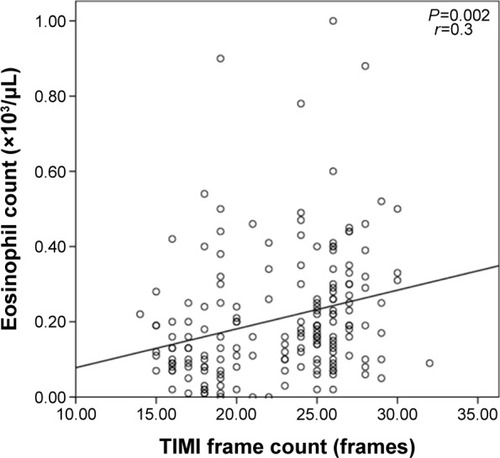
Table 1 Baseline and laboratory characteristics of the study groups
Table 2 Eosinophil counts in SCF subgroups
Table 3 Regression analysis with SCF as the dependent variable
Discussion
In our study, we have found significant differences in eosinophil count between patients with SCF and those with NCAs. The higher eosinophil count may indicate the presence of SCF.
The pathophysiology of SCF is not fully understood. However, it has a close relationship with accompanying atherosclerosis, oxidative stress, endothelial dysfunction, increased inflammatory parameters, vasculitis, and platelet function disorder.Citation1,Citation2,Citation5,Citation6 Especially, the association between SCF and inflammatory parameters is intriguing. Recent studies showed that SCF was associated with various inflammatory markers such as serum YKL 40, hs-CRP, plasma factors IX and XII, myeloperoxidase levels, soluble serum CD 40 ligand, interlukein 6 (IL-6), intercellular adhesion molecule 1 (ICAM-1), WCAM-1, and E-selectin.Citation12–Citation17 Eosinophils are laden with a variety of granule-associated molecules that play a role in the formation of thrombosis and vascular damage. Two of the four principal cationic proteins of the eosinophil granule, major basic protein and eosinophil peroxidase, were shown to be platelet agonists.Citation7
Eosinophils create an increased disposition to thrombosis by way of leukocyte, platelet stimulation, and release of tissue factor.Citation7,Citation18 Eosinophils store and release tissue factors and proteins like major basic protein and eosinophil peroxidase. These proteins have important role in activating platelets and thrombus formation by inhibiting trombomodulin. Activated eosinophils and eosinophil granule proteins were detected within the necrotic and thrombotic lesions and, furthermore, were found mainly in acute tissue damage in the endocardium and in the walls of small blood vessels. These findings indicated the potential role of eosinophils in vascular injury and inflammation.Citation19–Citation21 There is some evidence that eosinophil granule proteins can activate factor XII, platelets, and mononuclear cells in patients with hypereosinophilic syndrome, which may also underlie the procoagulant activity of eosinophils.Citation7 Recent studies have shown that eosinophils are related to arterial tortuosity, dilatation, thrombosis, cardiac syndrome X, and nondipper hypertension.Citation22,Citation23 Additionally, eosinophils have been shown to be associated with stent thrombosis, stent restenosis, coronary artery calcification, and acute coronary syndromes as described earlier. Furthermore, it was reported that elevated serum eosinophil concentration might be responsible for cardiac mural thrombus and embolic events.Citation24–Citation27
In our study, we demonstrated an increased eosinophil count in SCF patients when compared to the control subjects with NCAs. However, we did not observe a significant association between eosinophil count and the number of affected vessels, which have SCF. In addition, compatible with previous studies, we found a significantly higher level of hemoglobin in the SCF group. But it has not reached a statistical power in regression analysis. It has been well known that hematocrit value has been shown to be a significant determinant of blood viscosity in many studies.Citation28–Citation30 Mares et al evaluated the role of the blood viscosity in patients with ischemic heart disease and found that high viscosity is an independent predictor of both in-hospital and long-term adverse outcomes.Citation31 Blood viscosity is also a risk factor in cardiovascular events.Citation32
Our study has some limitations. First, due to the retrospective design of our study, risk factor modification could not be completely made. Second, since NCA definition was based on the angiographic appearance, all atherosclerotic plaques could not be excluded. Third, retrospective studies may inherently carry a selection bias.
Conclusion
In conclusion, our findings may contribute to the etiopathogenesis of SCF. Further randomized studies are needed to confirm our results.
Disclosure
The authors report no conflicts of interest in this work.
References
- LiJJXuBLiZCQianJWeiBQIs slow coronary flow associated with inflammation?Med Hypotheses20066650450816288834
- GokceMKaplanSTekeliogluYErdoganTKucukosmanogluMPlatelet function disorder in patients with coronary slow flowClin Cardiol20052814514815813623
- GoelPKGuptaSKAgarwalAKapoorASlow coronary flow: a distinct angiographic subgroup in syndrome XAngiology20015250751411512688
- AmasyaliBTurhanHKoseSAborted sudden cardiac death in a 20-year-old man with slow coronary flowInt J Cardiol2006109427429
- SasanoHVirmaniRPattersonRHRobinowitzMGuccionJGEosinophilic products lead to myocardial damageHum Pathol19892098508572777241
- WangJMahmudSAThompsonJAGengJGKeyNSSlungaardAThe principal eosinophil peroxidase product. HOSCN is a uniquely potent phagocyte oxidant inducer of endothelial cell tissue factor activity: a potential mechanism for thrombosis in eosinophilic inflammatory statesBlood2006107255856516166591
- RohrbachMSWheatleyCLSlifmanNRGleichGJActivation of platelets by eosinophil granule proteinsJ Exp Med19901724127112742212954
- OlsenEGSpryCJRelation between eosinophils and endomyocardial diseaseProg Cardiovasc Dis19852742412543880918
- BlétryOSolalPHerremanGCardiac manifestations of the hypereosinophilia syndrome: a report on fifteen casesAnn Med Interne (Paris)1981132116257224466
- LangRMBierigMDevereuxRBChamber Quantification Writing GroupAmerican Society of Echocardiography’s Guidelines and Standards CommitteeEuropean Association of EchocardiographyRecommendations for chamber quantification: a report from the American Society of Echocardiography’s Guidelines and Standards Committee and the Chamber Quantification Writing Group, developed in conjunction with the European Association of Echocardiography, a branch of the European Society of CardiologyJ Am Soc Echocardiogr2005181440146316376782
- GibsonCMCannonCPDaleyWLTIMI frame count: a quantitative method of assessing coronary artery flowCirculation1996938798888598078
- XuYMengHLSuYMSerum YKL-40 is increased in patients with slow coronary flowCoron Artery Dis201526212112525356814
- YurtdaşMYaylaliYTKayaYOzdemirMIncreased plasma high-sensitivity C-reactive protein and myeloperoxidase levels may predict ischemia during myocardial perfusion imaging in slow coronary flowArch Med Res2014451636924316393
- TürkmenMToprakCAçarGPlasma factor XI and XII activity in patients with slow coronary flowBlood Coagul Fibrinolysis2014
- DurakoğlugilMEKocamanSAÇetinMIncreased circulating soluble CD40 levels in patients with slow coronary flow phenomenon: an observational studyAnadolu Kardiyol Derg2013131394423070634
- LiJJQinXWLiZCIncreased plasma C-reactive protein and interleukin-6 concentrations in patients with slow coronary flowClin Chim Acta2007385434717706955
- TurhanHSaydamGSErbayARIncreased plasma soluble adhesion molecules; ICAM-1, VCAM-1, and E-selectin levels in patients with slow coronary flowInt J Cardiol2006108222423016002164
- MoosbauerCMorgensternECuvelierSLEosinophils area major intravascular location for tissue factor storage and exposureBlood20071093995100217003379
- SlungaardAVercellottiGMTranTGleichGJKeyNSEosinophil cationic granule proteins impair thrombomodulin function. A potential mechanism for thromboembolism in hypereosinophilic heart diseaseJ Clin Invest1993914172117308386194
- YoshikawaSKayesSGParkerJCEosinophils increase lung microvascular permeability via the peroxidasehydrogen peroxide-halide system. Bronchoconstriction and vasoconstriction unaffected by eosinophil peroxidase inhibitionAm Rev Respir Dis199314749149208385432
- RodeghieroFCastamanGRuggeriMCazzavillanMFerracinGDiniEFibrinolytic studies in 13 unrelated families with factor XII deficiencyHaematologica199176128322055558
- KuzeytemizMDemirMSenturkMThe relationship between eosinophil and nondipper hypertensionCor Vasa2013556487491
- DemirMSentürkMKuzeytemizMThe relationship between eosinophil and cardiac syndrome XClin Appl Thromb Hemost201321432532824057398
- NiccoliGSchiavinoDBelloniFPreintervention eosinophil cationic protein serum levels predict clinical outcomes following implantation of drug-eluting stentsEur Heart J200930111340134719383735
- JonerMFinnAVFarbAPathology of drug-eluting stents in humans: delayed healing and late thrombotic riskJ Am Coll Cardiol200648119320216814667
- YutaniCIshibashi-UedaHSuzukiTKojimaAHistologic evidence of foreign body granulation tissue and de novo lesions in patients with coronary stent restenosisCardiology199992317117710754347
- TanakaMFukuiMTomiyasuKEosinophil count is positively correlated with coronary artery calcificationHypertens Res201235332532822072111
- ChienSShear dependence of effective cell volume as a determinant of blood viscosityScience19701689779785441028
- BaskurtOKMeiselmanHJBlood rheology and hemodynamicsSemin Thromb Hemost20032943545014631543
- CokeletGRGoldsmithHLDecreased hydrodynamic resistance in the two-phase flow of blood through small vertical tubes at low flow ratesCirc Res1991681171984854
- MaresMBertoloCTerribileVGirolamiAHemorheological study in patients with coronary artery diseaseCardiology1991781111162070368
- FornalMKorbutRAKrolczykJGrodzickiTLeft ventricular geometry and rheological properties of erythrocytes in patients at cardiovascular disease riskClin Hemorheol Microcirc20094320320819847054