
Abstract
Background
Hepatocellular carcinoma (HCC) is a severe health condition associated with high hospitalizations and mortality rates, which also imposes a relevant economic burden.
Purpose
The aim of the present survey is to investigate treatment strategies and related costs for HCC in the intermediate and advanced stages of the disease.
Patients and methods
The survey was conducted in four Italian centers through structured interviews with physicians. Information regarding the stage of disease, treatments performed, and related health care resource consumption was included in the questionnaire. Direct health care cost per patient associated with the most relevant treatments such as sorafenib, transarterial chemoembolization (TACE), and transarterial radioembolization (TARE) was evaluated.
Results
Between 2013 and 2014, 285 patients with HCC were treated in the four participating centers; of these, 80 were in intermediate stage HCC (Barcelona Clinic Liver Cancer Classification [BCLC] B), and 57 were in the advanced stage of the disease (BCLC C). In intermediate stage HCC, the most frequent first-line treatment was TACE (63%) followed by sorafenib (15%), radiofrequency ablation (14%), and TARE (1.3%). In the advanced stage of HCC, the most frequently used first-line therapy was sorafenib (56%), followed by best supportive care (21%), TACE (18%), and TARE (3.5%). The total costs of treatment per patient amounted to €12,214.54 with sorafenib, €13,418.49 with TACE, and €26,106.08 with TARE. Both in the intermediate and in the advanced stage of the disease, variability in treatment patterns among centers was observed.
Conclusion
The present analysis raises for the first time the awareness of the overall costs incurred by the Italian National Healthcare System for different treatments used in intermediate and advanced HCC. Further investigations would be important to better understand the effective health care resource usage.
Introduction
Hepatocellular carcinoma (HCC) is the fifth most common malignancy worldwide, which causes approximately 500,000 deaths every year,Citation1 and it is characterized by biological and clinical heterogeneity and different prognoses.Citation2,Citation3 It is also the second most common cause of death from cancer worldwide and the second most rapidly increasing type of cancer in the United States.Citation4–Citation6 The incidence of HCC increases progressively with advancing age in all populations, reaching its peak at the age of 70.Citation7 Moreover, HCC contributes substantially to health care spending.
In Italy, liver cancer is one of the first five causes of death in males (7%);Citation8 12,500 new cases of liver tumors were expected in 2014, accounting for 3% of the overall incidence of all tumors, with a male:female ratio of 2:1. The incidence of HCC has decreased in both sexes, since the mid 90s.Citation8 Approximately 21,000 patients with a previous diagnosis of HCC (1% of all patients with a cancer) lived in Italy in 2011.Citation8
The most important risk factors for HCC are cirrhosis due to chronic hepatitis B and chronic hepatitis C, alcoholic cirrhosis, or nonalcoholic steatohepatitis, high body mass index, and diabetes mellitus.Citation9–Citation11
Worldwide, the most important risk factor for liver cancer is chronic hepatitis B or hepatitis C virus. People infected with both viruses have a high risk of developing chronic hepatitis, cirrhosis, and liver cancer. The risk of developing liver cancer is higher if patients are also heavy drinkers.Citation12 The vast majority of patients developing liver cancer already have some evidence of cirrhosis. Obesity increases the risk of developing liver cancer, probably because it can result in fatty liver disease and cirrhosis. Type 2 diabetes is associated with an increased risk of liver cancer, usually in patients who also have other risk factors (eg, heavy alcohol use, chronic viral hepatitis).Citation12 This risk may be increased as type 2 diabetes patients tend to be over-weight or obese, which can cause liver problems.Citation12 Although HCC patients can benefit from radical resection, transplantation, or radiofrequency ablation thanks to preliminary screening and diagnosis, tumors in some patients (those with background cirrhosis in particular) still progress rapidly because of local spreading or metastases.
The Barcelona Clinic Liver Cancer Classification (BCLC) correlates stages of the disease with treatment modalities, and identifies five stages of HCC (0, A, B, C, and D) according to preestablished prognostic variables and treatment modalities for each stage of the disease, thus providing both prognostic prediction and treatment allocation recommendations.Citation13 The American Association for the Study of Liver Disease (AASLD) guidelines 2010,Citation14 the European Association for the Study of the Liver (EASL) guidelines 2012,Citation15 and the Italian Association for the Study of the Liver (AISF 2012)Citation16 are the most updated guidelines for the treatment of HCC and include staging and prognostic–therapeutic stratification (EASL–BCLC guidelines) ().
Figure 1 Updated staging system and treatment strategy.
Abbreviations: HCC, hepatocellular carcinoma; PST, performance status test; CLT, cadaveric liver transplantation; LDLT, liver donor liver transplantation; RF, radio frequency ablation; PEI, percutaneous ethanol injection; TACE, transarterial chemoembolization; OS, overall survival.
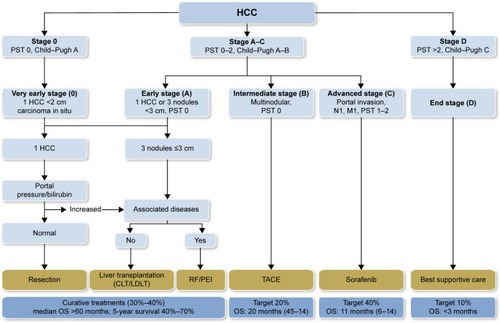
In the intermediate stage (BCLC B), patients with asymptomatic tumors (without an invasive pattern) survive 16 months on average;Citation2,Citation17,Citation18 chemoembolization prolongs the survival of these patients up to 19–20 months, according to randomized controlled trial and meta-analysis of pooled data.Citation17
HCC exhibits intense neoangiogenic activity during its progression. The rationale for transarterial chemoembolization (TACE) is that the intra-arterial infusion of a cytotoxic agent followed by embolization of the tumor-feeding blood vessels will result in a strong cytotoxic and ischemic effect. This procedure combines transcatheter delivery of chemotherapy emulsioned with lipiodol, followed by vascular stagnation achieved with embolic agents. Chemoembolization achieves partial responses in 15%–55% of patients and significantly delays tumor progression and macrovascular invasion. Overall, the median survival for intermediate HCC cases is expected to be approximately 16 months, whereas after chemoembolization, the median survival is ~20 months.Citation15,Citation19,Citation20
Patients in the advanced stage of the disease (BCLC stage C) (cancer-related symptoms and/or macrovascular invasion and/or extrahepatic spread) have poorer prognosis, and the expected median survival without treatment is ~6 months,Citation18,Citation21 or 25% at first year,Citation19 which is extended to 11 months by treatment with sorafenib.Citation20
Sorafenib, a multikinase inhibitor, is the standard systemic therapy suggested by guidelines for HCC BCLC stage C or for intermediate stage after failure of or ineligibility for locoregional therapies (treatment-stage migration strategy).Citation13
Efficacy and safety of sorafenib were evaluated in several clinical studies;Citation22 the Phase III SHARP studyCitation23 demonstrated that sorafenib significantly increased overall survival by 44% vs placebo (10.7 vs 7.9 months, respectively; P<0.001) and almost doubled median time to progression (5.5 vs 2.8 months, respectively; hazard ratio [HR]: 0.58, P<0.001).
These results were confirmed by a Phase III study conducted in the Asia–Pacific region;Citation24 in this trial, sorafenib significantly increased the overall survival by 47% vs placebo (6.5 vs 4.2 months, respectively; HR: 0.68; P=0.014) and doubled the median time to progression vs placebo (2.8 vs 1.4 months, respectively; HR: 0.57, P=0.0005).
In both Phase III studies, the safety profiles of sorafenib were predictable and manageable, and the benefits of sorafenib were consistent across subgroups by etiology, tumor burden, tumor stage, and prior therapy. Based on these results, international and national guidelines recommended sorafenib as the treatment of choice for advanced HCC (level of evidence IACitation15,Citation25/positively strong). A few studiesCitation26–Citation31 reported the economic burden of HCC worldwide, and while sorafenib cost-effectiveness analyses have been published,Citation32,Citation33 to our knowledge no data exist on the cost-effectiveness of TACE for HCC. The objective of the present analysis is to investigate treatment pathways and related health care costs for HCC BCLC stage B and stage C patients.
Material and methods
The aim of the present survey is to investigate the current patterns of treatment, health care resource consumption, and costs related to the treatment of HCC in the intermediate and advanced stages of the disease, through an analysis of the therapeutic pathways followed in four Italian centers. The survey was conducted through structured interviews involving gastroenterology and interventional radiology units. Ethical approval for this study was obtained from Policlinico Umberto I Roma, AOU Seconda Università di Napoli, Policlinico Paolo Giaccone Palermo, and AO Brotzù Cagliari. Informed consent was obtained from all patients.
The data collected in the project remained the property of each facility provider and were managed in aggregate and anonymous form, without access to individual patient data.
The following information was collected:
Number of patients with HCC by stage
Distribution of patients by treatment options (TACE, transarterial radioembolization [TARE] systemic treatment) and line of treatment (first- and secon-line treatment)
Treatments administered (frequency, average number of locoregional therapies, and duration of treatment for systemic therapies)
Diagnostic procedures and laboratory tests associated with each treatment
Specialist visits and follow-up associated with each treatment (percentage of patients undergoing examinations/visits and frequency)
Consumption of medical and nonmedical supplies associated with treatments (type of consumables, quantity, and unitary costs)
Cost of medical, nursing, and technical staff involved in patient management during the treatment.
Unit costs considered in this analysis and related sources are reported in .
Table 1 Resources consumption and costs
As for drugs, the cost per milligram was estimated as the average cost of different packs at the maximum price reimbursed by the Italian National Health Service.
In order to estimate the average cost per month of therapy, an 80% adherence to treatment was considered for sorafenib, along with published data on oral antineoplastic treatments.Citation34 The reference year of the present survey was 2013.
Results
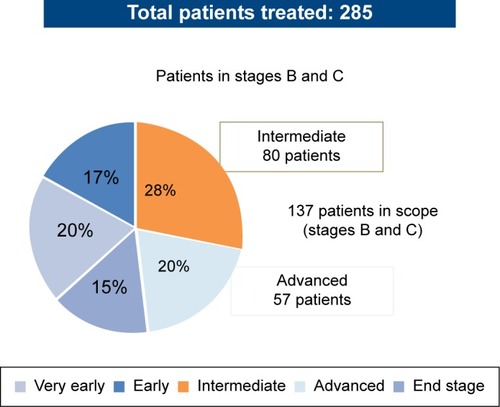
The present survey involved 137 patients with intermediate and advanced stage HCC, BCLC stage B, and BCLC stage C among a cohort of 285 patients (mean age: 66 years, 74% males) treated in four Italian centers specialized in the treatment of patients with HCC (Policlinico Umberto I Roma, AOU Seconda Università di Napoli, Policlinico Paolo Giaccone Palermo, AO Brotzù Cagliari). In the overall population, 20% of patients were in the very early stage of the disease (HCC BCLC stage 0), 17% in the early stage (HCC BCLC stage A), 28% in the intermediate stage (HCC BCLC stage B), 20% in the advanced stage (HCC BCLC stage C), and the remaining 15% in the terminal stage (HCC BCLC stage D) ().
Figure 2 Distribution of total patients treated.
First- and second-line treatments for patients in the intermediate and advanced stages of the disease are reported in and .
Figure 3 First-line treatments of patients with intermediate and advanced HCC.
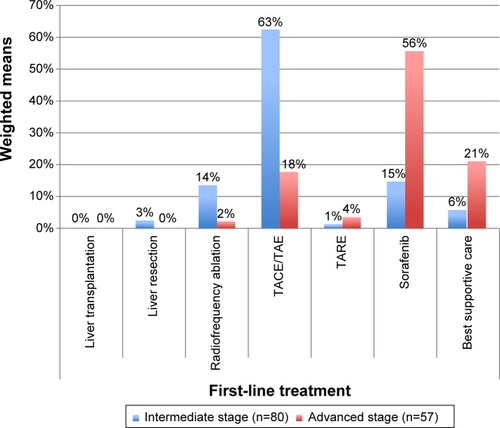
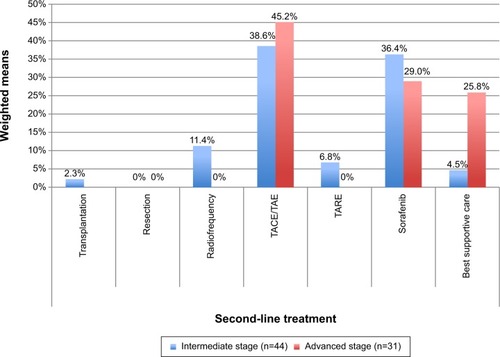
Figure 4 Second-line and subsequent treatments for patients with intermediate and advanced HCC.
Among the 80 patients in the intermediate stage of the disease treated with first-line therapies, 63% (minimum 50% to maximum 80%) were treated with TACE, 15% with sorafenib (range, 10%–17%), 14% (range, 5%–30%) with radiofrequency ablation, and the remaining 10% with other therapies (best supportive care, TARE, and liver resection).
Of these, 55% (n=44) were treated with second-line or subsequent therapies. The most frequent second-line or subsequent therapies were TACE – 39% (range, 5%-60%) and sorafenib – 36% (range, 9%–40%).
Among the 57 patients in the advanced stage of the disease treated with first-line therapies, sorafenib was the most frequently used first-line treatment: 56% (range, 12%–79%). Best supportive care was used in 21% of patients (range, 15%–24%) as the first-line option.
Of these, 54.4% (n=31) were then treated with second-line or subsequent therapies. TACE was the most frequent second-line option in the advanced stage – 45% (range, 0%–80%), followed by sorafenib – 29% (range, 0%–60%), and best supportive care – 26% (range, 0%–30%).
The mean duration of treatment with sorafenib in 137 patients with intermediate and advanced stage HCC was 6.1 months in all treatment lines combined.
The average number of TACE was 2.5 procedures/patient, and patients treated with TARE received an average of 1.5 procedures/patient.
The health care resources used in association with each type of therapy are reported in .
Table 2 Resources according to type of treatment
Mean resource consumption related to the different treatments, and related costs of consumables and professional resources are reported in and .
Table 3 Per-patient resource consumption and costs of consumables by procedure
Table 4 Per-patient resource consumption and costs of professional resources by treatment
Regarding the systemic treatment, the average cost per tablet (200 mg) of sorafenib to public health care structures (including the two 5% transient price reductions, as per Italian law at the time of the analysis)Citation35,Citation36 accounted for €28.70.
Considering the overall mean daily dosage (612 mg) and an estimated 80% of adherence to therapy,Citation34 the average per-month cost of treatment with sorafenib amounted to €1,986.36.
On the basis of the unitary cost per procedure/month of treatment and the duration of each therapy, the calculated average total costs of the different treatments are reported in .
Table 5 Overall cost per patient by type of treatment
Discussion
The results of the present analysis, aimed at evaluating the patterns of treatment and the costs related to HCC treatments, show a high variability among centers concerning procedures used in both the intermediate and advanced stages, first-line and subsequent lines. TACE was the treatment of choice in intermediate HCC, as suggested by the guidelines, but ~38% of patients were treated with alternative therapies. Sorafenib was the most frequently used first-line therapy in advanced HCC as recommended by international and Italian guidelines, although ~45% of these patients received other first-line treatments. A potential role of the combined approach of these therapies in intermediate HCC patients, as suggested by recent publications,Citation37 is still experimental and needs further confirmatory trials. The cost of HCC treatment amounted to ~€12,200/patient for sorafenib, €13,400/patient for TACE, and €26,100/patient for TARE.
The unitary costs of the treatments that were used in the calculations originate from tariffs and average acquisition costs at the national level (determined on a benchmark of 23 tenders). This methodology allows a comparison among treatment strategies based on the same evaluation criteria. From the perspective of health care cost of treatment, some facts should be taken into consideration. Treatment guidelines recommend TACE for intermediate HCC. The costs sustained by the centers for this procedure are, however, only partially covered by their diagnosis-related group’s (DRG)Citation38 tariff (€5,304 vs a reimbursement tariff of €4,085; DRG 203: malignancy of hepatobiliary system or pancreas).Citation32 Regarding TARE, which is not recommended by treatment guidelines either in intermediate stage or in advanced stage HCC, the costs sustained by the centers are relevant (~€17,400/patient/procedure), while at the national level, the DRG’s reimbursement tariff for TARE is DRG 409 (radiotherapy),Citation38 reimbursed at €1,471. Among the centers involved in the present study, only one performs this kind of procedure.
Sorafenib, recommended by national and international guidelines as the treatment of choice for advanced HCC, is dispensed in Italy by hospital pharmacies and registered in the “file F” that is used for specific categories of drugs distributed by NHS health care structures not covered by DRGs or tariffs (sorafenib cost is directly reimbursed to hospitals by local health care units or regions). We note, however, that this evaluation is only a cost analysis and does not take into account unplanned hospitalization, cost of side effects, and their treatment. The inclusion of these “shadow costs” could change the final cost of HCC treatment. Furthermore, we did not find any cases of HCC surgical treatments. Recent literature,Citation39 for example, showed that surgical therapies could also give the best results in patients with intermediate or advanced HCC. A limitation of the present study is that the centers that participated in this analysis may not accurately mirror the situation of the entire Italian territory, although they are centers experienced in the treatment of HCC, selected among hospitals with a wide volume of activity in this field. To our knowledge, this is the first study that evaluates the costs of treatment patterns for intermediate/advanced HCC patients in a real-life setting in Italy.
Conclusion
Sorafenib is recommended by international and Italian guidelines (level of evidence IA/strong positive) as the treatment of choice for advanced HCC. It was the most frequently used treatment in this setting; the associated cost of treatment was €12,200/patient. TACE was the most widely used treatment in intermediate HCC, and its associated costs of €13,400/patient are only partially covered by the DRG’s reimbursement tariffs. TARE, which is not indicated as a treatment choice in HCC management guidelines, was performed in one of the participating centers with an associated average cost of €26,100/patient that is not covered by the national reference DRG. The present study highlights the need for additional analyses of the national health care system resources that are being used routinely for the treatment of HCC and the associated outcomes, and can be the basis for future research and analysis of the cost-effectiveness of TACE, alone or combined with sorafenib, for the treatment of HCC.
Acknowledgments
The survey was supported by an unrestricted grant of Bayer Healthcare S.p.A.
Disclosure
The authors report no conflicts of interest in this work.
References
- El-SeragHBHepatocellular carcinoma: an epidemiologic viewJ Clin Gastroenterol2002355 Suppl 2S72S7812394209
- CabibboGEneaMAttanasioMBruixJCraxìACammàCA meta-analysis of survival rates of untreated patients in randomized clinical trials of hepatocellular carcinomaHepatology2010511274128320112254
- VillaECritelliRLeiBMarzocchiGNeoangiogenesis-related genes are hallmarks of fast-growing hepatocellular carcinomas and worst survival. Results from a prospective studyGut Epub29201510.1136/gutjnl-2014-308483.
- International Agency for Research on CancerWorld Health OrganizationGLOBOCAN 2012: estimated cancer incidence, mortality and prevalence worldwide Available from: http://globocan.iarc.fr/Pages/fact_sheets_cancer.aspxAccessed January 29, 2015
- EverhartJERuhlCEBurden of digestive diseases in the United States part II: lower gastrointestinal diseasesGastroenterology2009136374175419166855
- FerlayJShinHRBrayFFormanDMathersCParkinDMEstimates of worldwide burden of cancer in 2008: GLOBOCAN 2008Int J Cancer2010127122893291721351269
- El-SeragHBMasonACRising incidence of hepatocellular carcinoma in the United StatesN Engl J Med199934074575010072408
- I numeri del cancro in Italia 2014. AIOM AIRTUM. [Cancer numbers in Italy in 2014. AIOM AIRTUM] Available from: http://www.registri-tumori.it/PDF/AIOM2014/I_numeri_del_cancro_2014.pdfAccessed January 21, 2015 Italian
- SchwartzMRoayaieSKonstadoulakisMStrategies for the management of hepatocellular carcinomaNat Clin Pract Oncol20074742443217597707
- YangJDRobertsLRHepatocellular carcinoma: a global viewNat Rev Gastroenterol Hepatol20107844845820628345
- KudoMIzumiNKokudoNManagement of hepatocellular carcinoma in Japan: consensus-based clinical practice guidelines proposed by the Japan Society of Hepatology (JSH) 2010 updated versionDig Dis20112933936421829027
- American Cancer SocietyLiver Cancer Available from: http://www.cancer.org/cancer/livercancer/detailedguide/liver-cancer-risk-factorsAccessed February 3, 2015
- LlovetJMBrúCBruixJPrognosis of hepatocellular carcinoma: the BCLC staging classificationSemin Liver Dis19991932933810518312
- BruixJShermanMAASLD Practice Guideline 2010. Management of hepatocellular carcinoma: an updateHepatology2011531020102221374666
- European Association for the Study of the LiverEuropean Organisation for Research and Treatment of CancerEASL–EORTC clinical practice guidelines: management of hepatocellular carcinomaJ Hepatol20125690894322424438
- Italian Association for the Study of the Liver (AISF)AISF Expert PanelAISF Coordinating CommitteeBolondiLCilloUColomboMPosition paper of the Italian Association for the Study of the Liver (AISF): the multidisciplinary clinical approach to hepatocellular carcinomaDig Liver Dis201345971272310.1016/j.dld.2013.01.01223769756
- LlovetJMBruixJSystematic review of randomized trials for unresectable hepatocellular carcinoma: chemoembolization improves survivalHepatology20033742944212540794
- LlovetJMBruixJMolecular targeted therapies in hepatocellular carcinomaHepatology2008481312132718821591
- CammàCSchepisFOrlandoATransarterial chemoembolization for unresectable hepatocellular carcinoma: meta-analysis of randomized controlled trialsRadiology2002224475412091661
- CabibboGGencoCDi MarcoVPredicting survival in patients with hepatocellular carcinoma treated by transarterial chemoembolisationAliment Pharmacol Ther20113419620421564144
- LlovetJMBustamanteJCastellsANatural history of untreated nonsurgical hepatocellular carcinoma: rationale for the design and evaluation of therapeutic trialsHepatology19992962679862851
- BolondiLCraxiATrevisaniFRefining sorafenib therapy: lessons from clinical practiceFuture Oncol201511344946525360997
- LlovetJMRicciSMazzaferroVSorafenib in advanced hepatocellular carcinomaN Engl J Med2008359437839010.1056/NEJMoa070885718650514
- ChengALKangYKChenZEfficacy and safety of sorafenib in patients in the Asia-Pacific region with advanced hepatocellular carcinoma: a phase III randomised, double-blind, placebo-controlled trialLancet Oncol2009101253410.1016/S1470-2045(08)70285-719095497
- AIOM Guidelines2014 Available from: http://www.aiom.itAccessed February 24, 2015
- TheinHHIsaranuwatchaiWCampitelliMAHealth care costs associated with hepatocellular carcinoma: a population-based studyHepatology20135841375138410.1002/hep.2623123300063
- MishraAOtgonsurenMVenkatesanCThe inpatient economic and mortality impact of hepatocellular carcinoma from 2005 to 2009: analysis of the US nationwide inpatient sampleLiver Int20133381281128610.1111/liv.1220123710596
- ZhuLLiJDongXHospital costs and length of hospital stay for hepatectomy in patients with hepatocellular carcinoma: results of a prospective case seriesHepatogastroenterology2011581122052205710.5754/hge1014922234077
- GondekKLangKDanchenkoNEconomic costs of hepatocellular carcinoma in the United StatesJ Clin Oncol200826Suppl 156555 ASCO Annual Meeting Proceedings (Post-Meeting Edition)
- LangHCWuJCYenSHThe lifetime cost of hepatocellular carcinomaAppl Health Econ Health Policy200861556518774870
- MarinhoRTGiriaJMouraMGRising costs and hospital admissions for hepatocellular carcinoma in Portugal (1993–2005)World J Gastroenterol200713101522152717461443
- IavaroneMCabibboGPiscagliaFon behalf of the SOFIA (SOraFenib Italian Assessment) study groupField-practice study of sorafenib therapy for hepatocellular carcinoma: a prospective multi-center study in ItalyHepatology2011542055206321898496
- CammáCCabibboGPettaSon behalf of the WEF and the SOFIA study groupsCost-effectiveness of sorafenib treatment in field practice for patients with hepatocellular carcinomaHepatology2013571046105423299720
- SpoelstraSLGivenCWAssessment and measurement of adherence to oral antineoplastic agentsSemin Oncol Nurs201127211613221514481
- Determinazione AIFA del 3 luglio 2006, Gazzetta Ufficiale n. 156 del 7 luglio 2006. [AIFA Determination of 3 July 2006. Official Gazette no 156 of 7 July 2006] Available from: http://www.medicoeleggi.com/argomenti00/italia2006/19145.htmAccessed January 28, 2015 Italian
- Determinazione AIFA del 27 settembre 2006, Gazzetta n. 227 del 29 settembre 2006. [AIFA Determination 26 September 2006. Official Gazette no 156 of 29 September 2006] Available from: http://www.medicoeleggi.com/argomenti00/italia2006/19186.htmAccessed January 28, 2015 Italian
- CabibboGMaidaMCammàCCraxìAIs the efficacy of sorafenib treatment in patients with hepatocellular carcinoma affected by age?Expert Rev Anticancer Ther201313121355136124224926
- DECRETO 18 ottobre 2012. Remunerazione prestazioni di assistenza ospedaliera per acuti, assistenza ospedaliera di riabilitazione e di lungodegenza post acuzie e di assistenza specialistica ambulatoriale. (13A00528) (GU Serie Generale n. 23 del 28-1-2013 – Suppl Ordinario n.8. [Decree 18 October 2012. Remuneration performance of hospital assistance for acutes, hospital assistance to rehabilitation and long-term assistance after acute and specialist outpatient assistance] Available from: http://www.gazzettaufficiale.it/eli/id/2013/01/28/13A00528/sgAccessed January 29, 2015 Italian
- ZhangZMGuoJXZhangZCTherapeutic options for intermediate-advanced hepatocellular carcinomaWorld J Gastroenterol201117131685168921483627
- Conferenza Stato-Regioni 21/11/2014 – Rapporto STEM: “Prima analisi dei costi per il personale del Servizio Sanitario Nazionale Anni 2010/2012” [State-Regions Conference 11/21/14. STEM Report: “First cost analysis for National Health Service personnel in 2010/2012”] Available from: http://www.regioni.it/riforme/2014/11/21/conferenza-stato-regioni-21112014-rapporto-stem-prima-analisi-dei-costi-per-il-personale-del-servizio-sanitario-nazionale-anni-20102012-376317/Accessed January 23, 2015 Italian
- Italian Medicines AgencyReimbursement list. Class H list Available from: http://www.agenziafarmaco.gov.it/sites/default/files/111.84470.1172743348645ce4c.pdfAccessed January 23, 2015
- SetacciFde DonatoGChisciEEconomic impact of endarterectomy vs carotid artery stenting: a one year, single center studyEuroIntervention20073334034419737715