
Abstract
There are more than 12 new antiepileptic drugs approved in the last 2 decades. Even with these newer agents, seizure remission is still unachievable in around 30% of patients with partial-onset seizures (POS). Brivaracetam (BRV) is chemically related to levetiracetam (LEV) and possesses a strong binding affinity for the synaptic vesicle protein 2A tenfold above that of LEV, and other possible modes of antiepileptic actions. BRV is now under Phase III development for POS, but data from one Phase III trial also suggested its potential efficacy for primary generalized seizures. The purpose of this review is to provide updated information on the mechanisms of action of the available antiepileptic drugs, with a focus on BRV to assess its pharmacology, pharmacokinetics, clinical efficacy, safety, and tolerability in patients with uncontrolled POS. To date, six Phase IIb and III clinical trials have been performed to investigate the efficacy, safety, and tolerability of BRV as an adjunctive treatment for patients with POS. Generally, BRV was well tolerated and did not show significant difference in safety profile, compared to placebo. The efficacy outcomes of BRV, although not consistent across trials, did indicate that BRV was a promising add-on therapy for patients with POS. In conclusion, the many favorable attributes of BRV, like its high oral efficacy, good tolerability, dosing regimen, and minimal drug interaction, make it a promising antiepileptic therapy for patients with uncontrolled partial-onset epilepsy.
Introduction
Epilepsy is a chronic neurological disorder characterized by recurrent seizures and is estimated to affect approximately 50 million people worldwide.Citation1 Globally, an estimated 2.4 million people are diagnosed with epilepsy each year.Citation1 Epilepsy is not only associated with detrimental effects on the health and quality of life (QoL) of the individual patient, but also places a huge psychological and economic burden on the family members of the sufferers. When the diagnosis of epilepsy is established, treatment will be initiated accordingly. The primary treatment objectives are to achieve lifelong seizure freedom,Citation2,Citation3 reduce morbidity and mortality, and improve QoL,Citation4 ideally without intolerable adverse events (AEs).Citation5 Nonpharmacological management modalities like surgeryCitation6 and vagus nerve stimulationCitation7 are available for a selected proportion of patients, while the majority of individuals are managed with antiepileptic drugs (AEDs). Although the prognosis for the majority of patients is good, up to 30% of cases do not show complete remission despite appropriate therapy with AEDs. Normally, the AED is selected on the basis of the clinical efficacy, tolerability, drug interaction, and ease of use.Citation8 It is reported that most patients could be successfully managed by monotherapy alone;Citation8 however, up to 50% still need to be treated with combination therapy.Citation9
Monotherapy is the best pharmacotherapeutic option when first starting AED treatment.Citation10 If monotherapy is poorly tolerated or ineffective, the strategy is to switch to another drug; and if the first drug has partial efficacy and is well tolerated, it is worthwhile to try another drug in combination.Citation11 However, add-on therapy has been shown to be more effective when started immediately after first drug failure rather than after a second drug has also failed.Citation12 Nevertheless, when adequate trials of two tolerated, appropriately chosen, and administered AEDs (whether as monotherapy or in combination) fail to achieve sustained seizure freedom, a diagnosis of drug-resistant epilepsy could be subsequently made.Citation3
Among the two major types of epilepsy, partial-onset seizures (POS) occur in more than 60% of patients and are the most commonly encountered type of seizure in the adult population.Citation13 Often affected by comorbid disorders, these patients are difficult to treat, and approximately one-third of cases are resistant to AED management, including combination regimens.Citation14 The introduction of a large number of newer AEDs with more attractive pharmacokinetic, safety, and tolerability profiles over the past 20 years has, indeed, increased the treatment options to clinicians, but has not had a substantial effect on the seizure remission for patients with drug-resistant epilepsy.Citation14 A study assessing seizure freedom rates achieved with the newer AEDs including gabapentin, lamotrigine, topiramate, tiagabine, oxcarbazepine, levetiracetam (LEV), zonisamide, and pregabalin administered as an add-on therapy to patients with drug-resistant partial-onset epilepsy showed rather disappointing results.Citation15 Among the included placebo-controlled randomized controlled trials (RCTs), the seizure-free rates for patients who completed the double-blind phase of the trials (between 12 and 21 weeks) ranged from 0.8% to a maximum of 7.1%.Citation15 Although another study has reported a more promising seizure-free rate over 6 months, as high as 14%, with the use of the newer AEDs in real-life clinical practice,Citation16 it is obvious that a considerable proportion of patients with epilepsy are inadequately controlled with the available AEDs.Citation17
The current review aimed to discuss the emerging and current treatment for POS and then focus on the newly invented AED, brivaracetam (BRV), with a thorough examination of its pharmacology, mode of action, pharmacokinetics, comparative safety, efficacy, and tolerability, as well as its impact on patient-centered outcomes (eg, QoL, patient satisfaction).
Outline of targets for therapy and treatments for POS
POS originate from an area of the brain that is abnormally hyperexcitable and is intrinsically capable of increased abnormal firing of individual neurons.Citation18 This hyperexcitable environment is due to the augmentation of excitatory synaptic currents mediated by the neurotransmitters glutamate and aspartate.Citation18,Citation19 This hyperexcitable state is usually quickly terminated by inhibitory currents related to the neurotransmitter gamma-aminobutyric acid (GABA).Citation17 In order to produce a seizure, three conditions are needed:Citation19 first, the existence of hyperexcitable pacemaker area able to develop intrinsic bursts of action potentials that are usually brief and abolished by inhibitory mechanisms related to the neurotransmitter GABA; second, the absence of inhibition that allows this hyperexcitable state in the pacemaker area to be sustained; and the third condition is the ability of this pacemaker to recruit other brain areas.Citation17 Therefore, the currently marketed AEDs or emerging AEDs are targeted at one or more of the above-described mechanisms that are engaged in initiating and sustaining seizures. It is worth mentioning that LEV appears to have a unique mode of action that, at this time, remains to be clearly characterized. It is believed to bind to a specific, as yet unidentified, site on the synaptic plasma membrane.Citation20 The characteristics of the currently available AEDs are summarized in .
Table 1 Characteristics of current and emerging AEDs as adjunctive treatment for partial-onset epilepsy
AEDs that modulate voltage-gated channels
The most common target among AEDs is the sodium channel, which is responsible for the upstroke of the action potential in neurons and other excitable cells.Citation52 Sodium channel blockade is the best characterized mechanism of currently available AEDs. These AEDs prevent the return of the channels to the active state by stabilizing the inactive form. In doing so, repetitive firing of the axons is prevented. Presynaptic and postsynaptic blockade of sodium channels of the axons causes stabilization of the neuronal membranes, blocks and prevents post-tetanic potentiation, limits the development of maximal seizure activity, and reduces the spread of seizures. Traditional sodium channel blockers include phenytoin, carbamazepine (and its derivatives), lamotrigine, and so on.
Another type of voltage-gated channel that AEDs usually bind is the calcium channel. These AEDs, for example, pregabalin and gabapentin, regulate the opening and closing of the α2δ subunit, thus controlling the entry of calcium ions into presynaptic neurons and decreasing the release of various presynaptic neurotransmitters.Citation53,Citation54
One novel ion channel that is targeted by AEDs is the neuronal potassium channel. It acts via enhancing the activity of Kv7.2/Kv7.3 potassium channels by binding within the pore region.Citation55,Citation56 These channels generate the M current, a non-inactivating potassium conductance that regulates the neuronal firing rate at a subthreshold voltage between −60 and −40 mV.Citation57 Enhancing the M current hyperpolarizes the cell membrane toward the potassium equilibrium potential.Citation58 Retigabine (ezogabine) is the AED that falls into this category.
AEDs that enhance GABA-related inhibitory activity
A seizure reflects an imbalance between excitatory and inhibitory activity in the brain, with an increment of excitation over inhibition. The most important inhibitory neurotransmitter in the brain is GABA. It is the predominant inhibitory neurotransmitter in the central nervous system and is released in up to 40% of all synapses.Citation59 Impairment of GABA function is widely recognized to provoke seizures, while facilitation has an anticonvulsant effect.Citation60 GABA inhibitory activity can be achieved via the activation of GABAA receptor (phenobarbital), GABA reuptake inhibitor (tiagabine),Citation20 and GABA transaminase inhibitor (vigabatrin).Citation20
AEDs that modulate the glutamate-mediated excitation
Glutamate is the principal excitatory neurotransmitter in the mammalian brain. Focal injection of glutamate induces seizures in animals, and overactivation of glutamatergic transmission or abnormal glutamate receptor properties are observed in certain experimental seizure models and human epilepsy syndrome. A new AED (perampanel) has a new well-defined mechanism of action by selectively modulating excitatory glutamatergic transmission via modulation of the α-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid receptor.
AEDs that have multiple mechanisms of action
Some AEDs may invoke multiple mechanisms of action to exert their anticonvulsive effects. Valproate, a broad-spectrum AED, is reported to block voltage-dependent sodium channel,Citation20 T-type calcium channel,Citation61 and may elevate whole brain GABA levels and potentiate GABA response.Citation60 Topiramate may be involved in the inhibition of sodium and calcium currents, blockade of the α-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid/kainite subtype of glutamate receptor, and facilitation of GABA effects at the GABAA receptor.Citation20 Zonisamide could act through blocking the voltage-gated sodium channel, inhibiting T-type calcium channels,Citation62–Citation64 and enhancing GABA release and inhibiting glutamate release.Citation62,Citation64 Felbamate is believed to be the first effective AED with a direct action on the N-methyl-d-aspartate (NMDA) subtype of glutamate receptor,Citation20 and it also inhibits NMDA/glycine-stimulated increases in intracellular calcium,Citation65 reduces inward currents evoked by NMDA application to striatal neurons,Citation66 and blocks NMDA receptor-mediated excitatory postsynaptic potentials.Citation67
Brivaracetam
Pharmacology
Mode of action
Synaptic vesicle protein 2 (SV2) is a membrane glycoprotein common to all synaptic and endocrine vesicles. The synaptic vesicle protein 2A (SV2A), the primary SV2 isoform, is a widely distributed central nervous system protein, and is believed to participate in the coordination of synaptic vesicle exocytosis and neurotransmitter release.Citation68 This is shown by the observation that SV2A knockout mice develop seizures, which leads to their demise within the first few weeks.Citation68 In contrast, while heterozygous SV2A knockout mice do not demonstrate spontaneous seizures, they exhibit enhanced susceptibility to the convulsant effect of pilocarpine and kainite, a reduced 6 Hz seizure threshold, and an enhanced rate of seizure kindling.Citation69
LEV is thought to exert its main action at a specific binding site – the presynaptically located SV2A, which modulates presynaptic transmitter release.Citation70 BRV is a highly selective and reversible SV2A ligand with a 15- to 30-fold higher affinity than LEV in rat and human brain.Citation71,Citation72 The increased binding affinity of BRV, compared to LEV, to the presynaptically located SV2A corresponds to a higher efficacy in the animal models.Citation73 In addition to this, the modulation of SV2A function by BRV is also believed to contribute to its anticonvulsant effect. Besides, BRV also displays inhibitory activity at neuronal voltage-dependent sodium channels.Citation74 At any rate, the sodium channel modulation represents a distinct activity of BRV compared with LEV.Citation75 Furthermore, compared to LEV, BRV is able to inhibit NMDA-gated currents by up to one third.Citation74 All these modes of action may be associated with the wider spectrum of anticonvulsant mechanism of BRV.
The activity of BRV was studied in both focal and generalized seizure models. In the amygdala-kindled rat, BRV produced a more profound suppression of both motor seizure severity and after-discharge duration than LEV.Citation76 In mice genetically susceptible to audiogenic seizures, BRV offered more potent protection from clonic convulsions than LEV, while in the Genetic Absence Epilepsy Rat from Strasbourg, it exerted a more complete suppression of spike–wave discharge than LEV.Citation77 The anticonvulsant properties of BRV were also investigated in a partially drug-resistant self-sustaining status epilepticus rat model. The combination of diazepam and BRV was able to reduce the duration of active seizures to 3% of controls, which indicated potent anticonvulsant activity of the compound in status epilepticus.Citation78
Pharmacokinetics
BRV is rapidly absorbed after oral administration, with a tmax around 1 hour (ranging from 0.5 to 1.75 hours) and Cmax between 10 and 1,400 mg, when applied in a single dose.Citation76 However, a high fat meal is likely to delay tmax to 3 hours and decrease Cmax by about 28%.Citation79 BRV has a linear fashion of pharmacokinetics over a dose range from 10 to 600 mg. It was evenly absorbed throughout the gastrointestinal tract, as evidenced by the relative area under the curve (AUC) (100% = stomach) of 101%, 98%, and 97% following delivery in the proximal jejunum, distal jejunum, and ascending colon, respectively.Citation76 The metabolic clearance of BRV is increased in a time-dependent manner at supratherapeutic doses and a steady state is reached within a week of repeated administration.Citation76 The terminal elimination half-life of BRV is approximately 8 hours and does not vary with the applied doses.Citation80 Its protein binding is low with a volume of distribution of 0.6 L/kg, marginally lower than total body water.Citation79,Citation81 The primary metabolic pathways of BRV include hepatic hydrolysis of the acetamide group, CYP2C8-mediated hydroxylation, and a combination of these pathways,Citation76 mainly by the CYPSC8 isoform of cytochrome P450 (CYP450) and, to a lesser degree, by the isoforms CYP3A4 and CYP2C19,Citation82 but all metabolites in the human urine (2-[2-oxo-4-propylpyrrolidin-1-yl]butyric acid (35%) and 2-[2-oxo-4-propylpyrrolidin-1-yl]-4-hydroxy-butanamide [<10%]) are not pharmacologically active.Citation79 Its elimination is reliant on metabolism, largely via the activity of CYP450 system; thus, the renal clearance of the parent drug is low at 0.06 mL/min/kg (whereas the metabolites have a high renal clearance). It was reported that in patients with chronic liver disease, total body clearance of BRV may be reduced by 25%–35% and plasma half-life is accordingly prolonged to 14–17 hours,Citation76 while no major adjustment in dosage is required in patients with severe renal impairment without dialysis.Citation83
Pharmacodynamics
Studies in healthy volunteers showed that in high-dose range, BRV was associated with dose-related sedation and decreased alertness.Citation79,Citation81 For subjects on 200, 400, 800 mg daily and placebo, the mean (standard deviation) AUC change from baseline (ΔAUC0–12 hours) on day 7 was 6 (13), 12 (42), 17 (21), and 3 (9), respectively, for the Pentobarbital–Chlorpromazine-Alcohol Group subscale of the Addictive Research Centre Inventory-49 questionnaire (it measures sedative drug effects). The mean (standard deviation) ΔAUC0–12 hours of the visual analog scale (VAS), an alertness scale with higher value indicative of reduced alertness, was 5 (22), 46 (109), 57 (95), and −2 (26), respectively, while no trends of changes on the calmness VAS scale, ataxia (International Cooperative Ataxia Rating Scale Examination), or other neurological examinations were observed.Citation79,Citation81
The potential pharmacodynamic interaction between alcohol and BRV was also investigated. Coadministration of BRV and ethanol in healthy subjects was associated with additive effects on most of the pharmacodynamic variables (eg, saccadic peak velocity, smooth pursuit, adaptive tracking performance, and VAS alertness) without relevant pharmacokinetic interaction between BRV and ethanol.Citation84
Comparative safety, efficacy, and tolerability of BRV
Safety and tolerability
Generally, all studies did not report statistically significant difference between BRV and placebo groups in terms of treatment-emergent adverse events (TEAEs).Citation85–Citation89 Furthermore, no evident trend was observed in the incidence of TEAEs across all doses of BRV. The most commonly reported TEAEs were dizziness, headache, nasopharyngitis, nausea, fatigue, and somnolence from mild to moderate intensity. The TEAEs reported by greater than 5% of patients during the treatment period in each trial are shown in . A visual inspection of the incidence of TEAE identified that dizziness, somnolence, and influenza more frequently occurred in the BRV-treated group regardless of the doses administered.Citation88 The meta-analysis of five BRV trials also identified no statistically significant association between the administration of BRV and the majority of safety endpoints, including at least one TEAE, drug-related TEAEs, and serious adverse events.Citation90 However, in terms of individual TEAEs, another pooled analysis reported a significant difference between 20 mg BRV and placebo in the incidences of fatigue and nasopharyngitis (relative risk [RR]: 3.00 [95% confidence interval {CI}: 1.20–7.47] and 5.98 [95% CI: 1.36–26.34], respectively). Moreover, increased incidence of fatigue and irritability was also detected in the 50 mg BRV group compared to placebo (RR: 2.38 [95% CI: 1.16–4.88] and 2.95 [95% CI: 1.03–8.44], respectively). In addition, the risk of somnolence was significantly different between 150 mg BRV and placebo groups (RR: 2.21 [95% CI: 1.02–4.80]), while no significant differences were observed for either dose of 5 or 100 mg with respect to the TEAEs recorded in individual studies.Citation91
Table 2 Incidence of TEAEs in the trials of brivaracetam
Regarding treatment discontinuation, patients withdrew from each trial due to AEs, lack of efficacy, loss to follow-up, and withdrawal of consent due to personal reasons. However, all the RCTs did not show remarkable distinctions in withdrawal rates between BRV and placebo groups (). Nevertheless, the majority of discontinuation was accounted for by AEs caused by either BRV or concomitant AEDs. The results of meta-analysis on the overall withdrawal rate also indicated no statistical difference between BRV and placebo groups (RR: 1.08, 95% CI: 0.73–1.59; P=0.70).Citation90 The reason for withdrawal as assessed by another meta-analysis also showed consistent and similar results.Citation91
Table 3 Patient flow in the clinical trials of brivaracetam
Besides, the effects of BRV on cardiac repolarization and neurocognition were studied in healthy subjects. It was found that the QT interval did not increase with plasma concentration of BRV,Citation92 and BRV did not alter the profile of cognitive, subjective, and electrophysiologic effects, compared to placebo.Citation93
Efficacy
To date, six RCTs have reported the efficacy outcomes of various doses of BRV as adjunctive treatment in a population of patients with partial-onset epilepsies.Citation85–Citation89,Citation94 The percentage reduction in baseline-adjusted POS frequency/weekCitation85–Citation89 (or 28 days)Citation94 over placebo was adopted as the primary efficacy outcome across all RCTs, while the responder rate (defined as the percentage of patients who achieved 50% reduction in seizure frequency compared to baseline) was employed as the secondary efficacy outcome. In general, higher dose of BRV is likely to produce significant efficacy outcome, compared to placebo. Among these studies, a Phase IIb trialCitation86 and a Phase III trialCitation89 failed to detect a significant difference in the primary efficacy outcome, while in the other four RCTs, 50 mg/dayCitation85,Citation87,Citation88 or 100 and 200 mg/dayCitation94 of BRV was found to be more effective than placebo in achieving the primary efficacy outcome. The percentage reduction in baseline-adjusted POS frequency/week ranged from −0.9%Citation88 to 22.1%Citation85 across all the doses. In comparison, a recently published study on two higher doses of BRV (100 and 200 mg/day) reported the most promising outcomes.Citation94 The reduction in baseline-adjusted POS frequency/28 days over placebo was 22.8% (P<0.001) and 23.2% (P<0.001) for BRV 100 and 200 mg/day, respectively. Regarding the rate of responders, more studies reported significant difference for this outcome (). Nevertheless, the lower doses (ie, 5 and 20 mg/day) used in three RCTs did not show any statistical difference between BRV and placebo in the primary efficacy endpoint. and summarize the ≥50% responder and seizure-free rates across all the RCTs of BRV.
Figure 1 Responder rates of ≥50% in the RCTs of BRV.
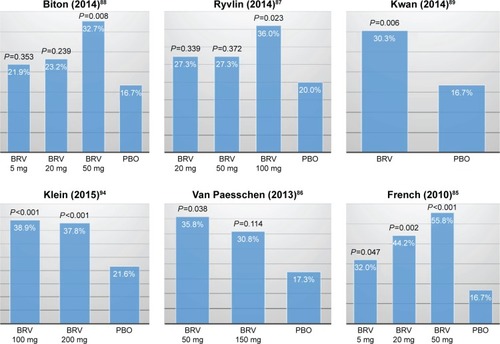
Figure 2 Seizure-free rates in the RCTs of BRV.
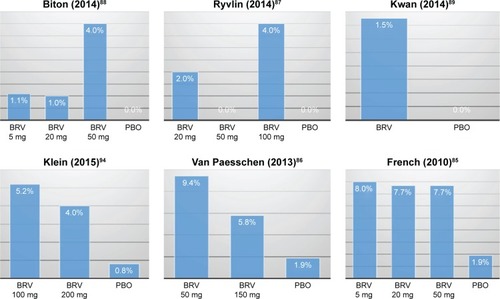
Table 4 Characteristics and primary results of key RCTs for brivaracetam
Two meta-analysesCitation90,Citation91 that synthesized the results of responder rate and seizure-free rate yielded similar results across all doses of BRV from five RCTs.Citation85–Citation89 In a fixed-effects model, the responder rate was significantly higher in BRV group compared with placebo group for doses of 20 mg/day (RR: 1.63, 95% CI: 1.18–2.27; P=0.003), 50 mg/day (RR: 2.00, 95% CI: 1.50–2.66; P<0.001), and 100 mg/day (RR: 1.80, 95% CI: 1.12–2.88; P=0.01).Citation90 Whereas, regarding seizure-free rate reported in three RCTs,Citation85,Citation86,Citation88 significant difference was detected for the dose of 50 mg/day (RR: 5.80, 95% CI: 1.54–21.84; P=0.009) in only one meta-analysis.Citation90 However, it is worth noting that the seizure-free rate was defined as free from POS in two of those three studies.Citation85,Citation86
Patient profiles
Patients with similar epilepsy-specific and demographic characteristics were studied in the six Phase IIb and III RCTs. For recruitment, patients were required to experience at least fourCitation85,Citation86,Citation89 or eight Citation87,Citation88 POS, depending on the length of the baseline period. However, the inclusion criteria across the studies varied slightly: the latest Phase III RCT enrolled subjects with the widest age range (16–80 years old)Citation94 and three other RCTs recruited patients aged between 16 and 70 years, while subjects recruited in the two Phase IIb trials had the narrowest age range (16–65 years old).Citation87–Citation89 It was reported that compared to middle-aged patients with epilepsy, elderly patients were more likely to respond favorably to treatment even at lower doses.Citation95 In fact, other studies have also shown better treatment outcome in elderly patients with epilepsy.Citation96,Citation97 This may give rise to heterogeneity in the study population across RCTs. With regard to the concomitant AEDs, except for the study by Kwan et alCitation89 (with one to three AEDs allowed during the study period), only one or two concomitant AEDs were allowed in all the trials. This may lead to the enrollment of patients with varied levels of uncontrolled POS. Of note, the number of prior AEDs used by patients in the past 5 years in the reported trials varied substantially as well. For instance, in the study by Van Paesschen et al,Citation86 34.6%–45.3% of patients had taken and discontinued ≥5 AEDs during the past 5 years compared to 2.0%–7.0% in the study by Ryvlin et al.Citation87 It has been demonstrated that the rates of seizure freedom and patients with a >50% seizure frequency reduction after administration of new AED decrease as a function of the number of previously failed AEDs.Citation98 So, this would be another source of heterogeneity in patient characteristics among trials. Nonetheless, from two meta-analyses,Citation90,Citation91 the statistical measures (χ2 and I2) did not show considerable heterogeneities across the included RCTs for outcomes such as responder rate and seizure-free rate. This might suggest that the aforementioned differences in the study populations were not significant in producing heterogeneity.
Patient-reported outcomes
Epilepsy, as a chronic disorder, has considerable negative effect on people’s day-to-day functioning. Meanwhile, seizures are still poorly controlled in around 30% of patients, even with multiple antiepileptic therapies. For these patients, traditional clinical outcomes that measure the treatment effect, such as seizure frequency, seizure-free days, and responder rate, might not be sufficient to capture all the benefits generated by treatment and are also incapable of reflecting the total impact of epilepsy on patient’s well-being and their own perception of treatment effect. Consequently, an increasing number of RCTs integrated the measurement of QoL of patients into the design of epilepsy trials to provide a more holistic evaluation of treatment effects and adverse effects of newly invented AEDs. To date, the QoL in patients with POS administered BRV has not been reported. Instead, the only study in patients with genetically ascertained Unverricht–Lundborg disease with action myoclonus reported a significant improvement in QoL as measured by Quality of Life in Epilepsy-30 at BRV 50 and 150 mg/day, despite its statistically significant effect on action myoclonus.Citation99
At the time of this review, three Phase III, open-label, multicenter, flexible-dose (up to a maximum dose of 150 mg/day), long-term follow-up trials (NO1125, NCT00175916; NO1199, NCT00150800; and NO1315, NCT00761774) are still ongoing to evaluate the long-term safety/tolerability and maintenance of efficacy of BRV in patients with POS who had participated in previous trials. Although the proportion of patients from the BRV group who entered into the open phase of the individual trials did not generally show a favorable trend compared to the placebo group, a meta-analysis of trials of adjunctive AEDs in adults with drug-resistant focal epilepsy found the responder rates to placebo virtually double between 1989 and 2009.Citation100 This may partially explain the unnoticeable difference between BRV and placebo groups. Anyway, when the results from those trials are released, a more comprehensive picture of BRV may become available.
Conclusion
Monotherapy is the first step to try for all patients with newly diagnosed epilepsy. Following an ineffective or intolerable initial monotherapy, the next step is to add or switch to another AED. Evidence has indicated that add-on therapy might be more effective when started immediately after the first drug failure rather than after a second drug has also failed.Citation12 After failing to achieve sustained seizure freedom with two tolerated, appropriately chosen and administered AEDs (regardless of monotherapy or multitherapy) in a patient,Citation3 the patient could be classified as having drug-resistant epilepsy. When add-on therapy is warranted (for those who either failed the first monotherapy or have drug-resistant epilepsy), seizure characteristics, drug and patient factors become an important consideration when implementing the management strategies.Citation101 Selection of an AED is usually made based on the seizure type, spectrum of activity, tolerability, drug interaction, and patient’s personal circumstances.Citation101
Similar to all the other newer generations of AEDs, BRV has been investigated as an adjunctive therapy for adult patients with uncontrolled partial-onset epilepsies (and in very limited number of patients with generalized epilepsiesCitation89). So far, BRV appears to be a useful new addition to adjunctive treatment option for partial-onset epilepsy, particularly for patients who had not achieved adequate seizure control with one or more other adjunctive therapies.Citation85,Citation87,Citation88,Citation94 In general, the newer group of AEDs has been associated with better safety and tolerability, fewer AEs, and improved QoL, compared with more traditional agents. However, with no direct head-to-head comparison among these newly invented drugs, it is extremely difficult for clinicians to choose from a dozen of these newer agents. It was even reported that clinicians often choose therapy according to their own comfort level with the particular AEDs, rather than weighing up all disadvantages and advantages of older versus newer, less-familiar drugs.Citation8 Hence, drugs with simpler dosing regimens and uncomplicated titration schedules, undoubtedly, have an advantage. BRV, with a twice-daily dosing regimen and well tolerated by patients even at a dose of 200 mg/day without up-titration, would be an attractive option.Citation94 But when LEV and BRV are compared, given the similarity in chemical structure and possible pharmacology between them, the choice is more complicated. The relationship between primary efficacy outcome in BRV pivotal trials and history of LEV administration (prior LEV, concomitant LEV, and LEV-naïve) was explored.Citation88 Of interest, LEV-naïve patients and those with prior LEV histories achieved numerically (though statistically not significant) greater reduction in seizure frequency compared to placebo,Citation85,Citation86,Citation88 while concomitant LEV might reduce the efficacy of BRV.
As BRV is still under review by different regulatory agencies (including US Food and Drug Administration and European Medicines Agency) for the treatment of POS in patients of age 16 years and above with epilepsy, no data about its use in real-life clinical practice is available at the moment. Meanwhile, it has gained an orphan drug status for development in progressive and symptomatic myoclonic seizures in Europe and US, respectively.Citation102 In summary, the many favorable attributes of BRV, like its high oral efficacy, good tolerability, dosing regimen, and minimal drug interaction, make it a promising antiepileptic choice for patients with uncontrolled partial-onset epilepsy.
Disclosure
The authors report no conflicts of interest in this work.
References
- World Health Organization [homepage on the Internet]Epilepsy2016 [updated February, 2016]. Available from: http://www.who.int/media-centre/factsheets/fs999/en/Accessed August 18, 2015
- SanderJWThe epidemiology of epilepsy revisitedCurr Opin Neurol20031616517012644744
- KwanPArzimanoglouABergATDefinition of drug resistant epilepsy: consensus proposal by the ad hoc Task Force of the ILAE Commission on Therapeutic StrategiesEpilepsia2010511069107719889013
- PeruccaEBeghiEDulacOShorvonSTomsonTAssessing risk to benefit ratio in antiepileptic drug therapyEpilepsy Res20004110713910940614
- KwanPBrodieMJRefractory epilepsy: a progressive, intractable but preventable condition?Seizure200211778411945093
- StefanHHalaszPGil-NagelARecent advances in the diagnosis and treatment of epilepsyEur J Neurol2001851953911784335
- FisherRSEgglestonKSWrightCWVagus nerve stimulation magnet activation for seizures: a critical reviewActa Neurol Scand20151311825145652
- BrodieMJKwanPThe star systems – overview and use in determining antiepileptic drug choiceCNS Drugs20011511211465010
- LeppikIEMonotherapy and polypharmacyNeurology200055S25S2911147565
- BeghiEPeruccaEThe management of epilepsy in the 1990s. Acquisitions, uncertainties and priorities for future researchDrugs1995496806947601010
- BrodieMJFrenchJAManagement of epilepsy in adolescents and adultsLancet200035632332911071202
- KwanPBrodieMJEpilepsy after the first drug fails: substitution or add-on?Seizure2000946446811034869
- SchmitzBMontourisGSchaubleBCaleoSAssessing the unmet treatment need in partial-onset epilepsy: looking beyond seizure controlEpilepsia2010512231224020973782
- KwanPBrodieMJEffectiveness of first antiepileptic drugEpilepsia2001421255126011737159
- GazzolaDMBalcerLJFrenchJASeizure-free outcome in randomized add-on trials of the new antiepileptic drugsEpilepsia2007481303130717521343
- CallaghanBCAnandKHesdorfferDHauserWAFrenchJALikelihood of seizure remission in an adult population with refractory epilepsyAnn Neurol20076238238917880009
- NasreddineWBeydounAAtwehSAbou-KhalilBEmerging drugs for partial onset seizuresExpert Opin Emerg Drugs20101541543120476851
- DichterMABasic mechanisms of epilepsy: targets for therapeutic interventionEpilepsia199738Suppl 9S2S69578539
- NajmIMJanigroDBabbTLMechanisms of epileptogenesis and experimental models of seizuresElaineWAjayGDeepakKLThe Treatment of Epilepsy: Principles and Practice3 edPhiladelphiaLippincott Williams & Wilkins20013334
- KwanPSillsGJBrodieMJThe mechanisms of action of commonly used antiepileptic drugsPharmacol Ther200190213411448723
- RamaratnamSMarsonAGBakerGALamotrigine add-on for drug-resistant partial epilepsyCochrane Database Syst Rev2001CD00190911687001
- Lamotrigine (Lamictal) Available from: https://www.gsksource.com/pharma/content/dam/GlaxoSmithKline/US/en/Prescribing_Information/Lamictal/pdf/LAMICTAL-PI-MG.PDFAccessed August 25, 2015
- CastilloSSchmidtDBWhiteSOxcarbazepine add-on for drug-resistant partial epilepsyCochrane Database Syst Rev2000CD00202810908522
- Oxcarbazepine (Trileptal) Prescribing Information Available from: https://www.pharma.us.novartis.com/product/pi/pdf/trileptal.pdfAccessed August 25, 2015
- ChangXCYuanHWangYXuHQZhengRYEslicarbazepine acetate add-on for drug-resistant partial epilepsyCochrane Database Syst Rev2011CD00890722161441
- Eslicarbazepine acetate (Aptiom) Prescribing Information Available from: http://www.aptiom.com/Aptiom-Prescribing-Information.pdfAccessed August 25, 2015
- UthmanBMBazilCWBeydounALong-term add-on pregabalin treatment in patients with partial-onset epilepsy: pooled analysis of open-label clinical trialsEpilepsia20105196897820345940
- Pregabalin (Lyrica) Prescribing Information Available from: http://labeling.pfizer.com/ShowLabeling.aspx?id=561Accessed August 25, 2015
- MarsonAGKadirZAHuttonJLChadwickDWGabapentin for drug-resistant partial epilepsyCochrane Database Syst Rev2000CD001415
- Gabapentin (Neutontin) Prescribing Information Available from: http://labeling.pfizer.com/ShowLabeling.aspx?id=630Accessed August 25, 2015
- CraigDRiceSPatonFFoxDWoolacottNRetigabine for the adjunctive treatment of adults with partial-onset seizures in epilepsy with and without secondary generalization: a NICE single technology appraisalPharmacoeconomics20133110111023341194
- Retigabine (Trobalt) Prescribing Information Available from: https://www.medicines.org.uk/emc/medicine/24527Accessed August 25, 2015
- SplinterMYEzogabine (retigabine) and its role in the treatment of partial-onset seizures: a reviewClin Ther20123418451856.e184122917854
- PereiraJMarsonAGHuttonJLTiagabine add-on for drug-resistant partial epilepsyCochrane Database Syst Rev2002CD00190812137637
- Tiagabine (Gabitril) Prescribing Information Available from: http://www.gabitril.com/pdf/Gabitril_PI_GAB-012.pdfAccessed August 25, 2015
- Vigabatrin (Sabril) Prescribing Information Available from: http://www.lundbeck.com/upload/us/files/pdf/Products/Sabril_PI_US_EN.pdfAccessed August 25, 2015
- MarsonAGKadirZAHuttonJLChadwickDWThe new antiepileptic drugs: a systematic review of their efficacy and tolerabilityEpilepsia1997388598809579887
- FaulknerMAPerampanel: a new agent for adjunctive treatment of partial seizuresAm J Health Syst Pharm20147119119824429011
- Perampanel (Fycompa) Prescribing Information Available from: http://ca.eisai.com/pdf/new/Fycompa-PM-April%203-13_EN_Eisai.pdfAccessed August 25, 2015
- HsuWWSingCWHeYWorsleyAJWongICChanEWSystematic review and meta-analysis of the efficacy and safety of perampanel in the treatment of partial-onset epilepsyCNS Drugs20132781782723918722
- PulmanJJetteNDykemanJHemmingKHuttonJLMarsonAGTopiramate add-on for drug-resistant partial epilepsyCochrane Database Syst Rev2008CD00141718646072
- Topiramate (Topomax) Prescribing Information Available from: https://www.topamax.com/topamax/assets/topamax.pdfAccessed August 25, 2015
- ChadwickDWMarsonAGZonisamide add-on for drug-resistant partial epilepsyCochrane Database Syst Rev2005CD00141616235282
- Zonisamide (Zonegran) Prescribing Information Available from: http:www,accessdata,fda.gov/drugsatfda_docs/label/2009/020789s022s0251bl.pdfAccessed August 25, 2015
- ShiLLDongJCNiHJGengJSWuTXFelbamate as an add-on therapy for refractory epilepsyCochrane Database Syst Rev20147CD00829525036694
- Felbamate (Felbatol) Prescribing Information Available from: http://www.felbatol.com/Accessed August 25, 2015
- ChaisewikulRPriviteraMDHuttonJLMarsonAGLevetiracetam add-on for drug-resistant localization related (partial) epilepsyCochrane Database Syst Rev2001CD00190111279737
- Levetiracetam (Keppra) Prescribing Information Available from: http://www.accessdata.fda.gov/drugsatfda_docs/label/2009/021035s078s080,021505s021s024lbl.pdfAccessed August 25, 2015
- WestonJShukrallaAMcKayAJMarsonAGLacosamide add-on therapy for partial epilepsyCochrane Database Syst Rev20156CD00884126077821
- Lacosamide (Vimpat) Prescribing Information Available from: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/000863/WC500050338.pdfAccessed August 25, 2015
- BecerraJLOjedaJCorrederaERuiz GiménezJReview of therapeutic options for adjuvant treatment of focal seizures in epilepsy: focus on lacosamideCNS Drugs201125Suppl 131622141347
- MeislerMHKearneyJASodium channel mutations in epilepsy and other neurological disordersJ Clin Invest20051152010201716075041
- RogawskiMABazilCWNew molecular targets for antiepileptic drugs: alpha 2 delta, SV2A, and K(v)7/KCNQ/M potassium channelsCurr Neurol Neurosci Rep2008834535218590620
- BeydounANasreddineWAtwehSEfficacy and tolerability of pregabalin in partial epilepsyExpert Rev Neurother200881013102418590472
- RundfeldtCNetzerRThe novel anticonvulsant retigabine activates M-currents in Chinese hamster ovary-cells transfected with human KCNQ2/3 subunitsNeurosci Lett2000282737610713399
- WuttkeTVSeebohmGBailSMaljevicSLercheHThe new anti-convulsant retigabine favors voltage-dependent opening of the Kv7.2 (KCNQ2) channel by binding to its activation gateMol Pharmacol2005671009101715662042
- DelmasPBrownDAPathways modulating neural KCNQ/M (Kv7) potassium channelsNat Rev Neurosci2005685086216261179
- MainMJCryanJEDupereJRCoxBClareJJBurbidgeSAModulation of KCNQ2/3 potassium channels by the novel anticonvulsant retigabineMol Pharmacol20005825326210908292
- OlsenRWAvoliMGABA and epileptogenesisEpilepsia1997383994079118844
- LoscherWValproate: a reappraisal of its pharmacodynamic properties and mechanisms of actionProg Neurobiol199958315910321796
- KellyKMGrossRAMacdonaldRLValproic acid selectively reduces the low-threshold (T) calcium current in rat nodose neuronsNeurosci Lett19901162332382175404
- HolderJLJrWilfongAAZonisamide in the treatment of epilepsyExpert Opin Pharmacother2011122573258121967409
- Schulze-BonhageAZonisamide in the treatment of epilepsyExpert Opin Pharmacother20101111512620001433
- BitonVClinical pharmacology and mechanism of action of zonisamideClin Neuropharmacol20073023024017762320
- TaylorLAMcQuadeRDTiceMAFelbamate, a novel antiepileptic drug, reverses N-methyl-D-aspartate/glycine-stimulated increases in intracellular Ca2+ concentrationEur J Pharmacol19952892292337621896
- PisaniAStefaniASiniscalchiAMercuriNBBernardiGCalabresiPElectrophysiological actions of felbamate on rat striatal neuronesBr J Pharmacol1995116205320618640345
- PuglieseAMCorradettiREffects of the antiepileptic drug felbamate on long-term potentiation in the CA1 region of rat hippocampal slicesNeurosci Lett199621521248880744
- CrowderKMGuntherJMJonesTAAbnormal neurotransmission in mice lacking synaptic vesicle protein 2A (SV2A)Proc Natl Acad Sci U S A199996152681527310611374
- LeclercqKKaminskiRDassesseDKlitgaardHMatagneASeizure susceptibility of SV2A heterozygous mice in models of temporal lobe epilepsy. Program No. 492.17Neuroscience Meeting PlannerSan Diego, CASociety for Neurosciences2007
- LynchBALambengNNockaKThe synaptic vesicle protein SV2A is the binding site for the antiepileptic drug levetiracetamPNAS20041019861986615210974
- GillardMFuksBLeclercqKMatagneABinding characteristics of brivaracetam, a selective, high affinity SV2A ligand in rat, mouse and human brain: relationship to anti-convulsant propertiesEur J Pharmacol2011664364421575627
- MatagneAMargineanuDGKendaBMichelPKlitgaardHAnti-convulsive and anti-epileptic properties of brivaracetam (ucb 34714), a high-affinity ligand for the synaptic vesicle protein, SV2ABr J Pharmacol20081541662167118500360
- Schulze-BonhageABrivaracetam for the treatment of epilepsyExpert Opin Pharmacother2011121959196621682662
- ZonaCPieriMCarunchioICurcioLKlitgaardHMargineanuDGBrivaracetam (ucb 34714) inhibits Na(+) current in rat cortical neurons in cultureEpilepsy Res201088465419914041
- MargineanuDGKlitgaardHBrivaracetam inhibits spreading depression in rat neocortical slices in vitroSeizure20091845345619211275
- von RosenstielPBrivaracetam (UCB 34714)Neurotherapeutics20074848717199019
- MatagneACKendaBMMichelPKlitgaardHucb 34714, a new pyrrolidone derivative: comparison with levetiracetam in animal models of chronic epilepsy in vivoEpilepsia200344260
- WasterlainUSuchomelovaLMatagneABrivaracetam is a potent anticonvulsant in experimental status epilepticusEpilepsia200546219220
- Sargentini-MaierMLRolanPConnellJThe pharmacokinetics, CNS pharmacodynamics and adverse event profile of brivaracetam after single increasing oral doses in healthy malesBr J Clin Pharmacol20076368068817223857
- RolanPPigeoletEStockisAUCB 34714: Single and multiple rising dose safety, tolerability, and pharmacokinetics in healthy subjectsEpilepsia20044531431515030493
- RolanPSargentini-MaierMLPigeoletEStockisAThe pharmacokinetics, CNS pharmacodynamics and adverse event profile of brivaracetam after multiple increasing oral doses in healthy menBr J Clin Pharmacol200866717518341673
- WhomsleyRBrochotADell’AieraSIdentification of the cytochrome P450 isoforms responsible for the hydroxylation of BrivaracetamAAPS J200793408
- Sargentini-MaierMLSokalskiABoulangerPJacobsTStockisABrivaracetam disposition in renal impairmentJ Clin Pharmacol2012521927193322235139
- StockisAKruithofACVan GervenJMDe KamMLWatanabeSPeetersPAInteraction study between brivaracetam and ethanol in healthy subjectsEpilepsy Curr201515332
- FrenchJACostantiniCBrodskyAvon RosenstielPGroupNSAdjunctive brivaracetam for refractory partial-onset seizures: a randomized, controlled trialNeurology20107551952520592253
- Van PaesschenWHirschEJohnsonMFalterUvon RosenstielPEfficacy and tolerability of adjunctive brivaracetam in adults with uncontrolled partial-onset seizures: a phase IIb, randomized, controlled trialEpilepsia201354899722813235
- RyvlinPWerhahnKJBlaszczykBJohnsonMELuSAdjunctive brivaracetam in adults with uncontrolled focal epilepsy: results from a double-blind, randomized, placebo-controlled trialEpilepsia201455475624256083
- BitonVBerkovicSFAbou-KhalilBSperlingMRJohnsonMELuSBrivaracetam as adjunctive treatment for uncontrolled partial epilepsy in adults: A phase III randomized, double-blind, placebo-controlled trialEpilepsia201455576624446953
- KwanPTrinkaEVan PaesschenWRektorIJohnsonMELuSAdjunctive brivaracetam for uncontrolled focal and generalized epilepsies: results of a phase III, double-blind, randomized, placebo-controlled, flexible-dose trialEpilepsia201455384624116853
- MaJHuangSYouCAdjunctive brivaracetam for patients with refractory partial seizures: a meta-analysis of randomized placebo-controlled trialsEpilepsy Res2015114596526088886
- TianXYuanMZhouQWangXThe efficacy and safety of brivaracetam at different doses for partial-onset epilepsy: a meta-analysis of placebo-controlled studiesExpert Opin Pharmacother2015161755176726165169
- RosillonDAstrucBHulhovenREffect of brivaracetam on cardiac repolarisation – a thorough QT studyCurr Med Res Opin2008242327233718601811
- MeadorKJGevinsALeesePTOtoulCLoringDWNeurocognitive effects of brivaracetam, levetiracetam, and lorazepamEpilepsia20115226427220887370
- KleinPSchiemannISperlingMA randomized double-blind, placebo-controlled, multicenter, parallel-group study to evaluate the efficacy and safety of adjunctive brivaracetam in adults patients with partial-onset seizures67th American Academy of Neurology Annual Meeting, AAN; 2015Washington DCNeurology2015
- RamsayRRowanASlaterJCollinsJNemireROrtizWEffect of age on epilepsy and its treatment: results from the VA Cooperative StudyEpilepsia19943591
- CockerellOCJohnsonALSanderJWASShorvonSDPrognosis of epilepsy: a review and further analysis of the first nine years of the British National General Practice Study of Epilepsy, a prospective population-based studyEpilepsia19973831469024182
- MattsonRHCramerJACollinsJFA comparison of valproate with carbamazepine for the treatment of complex partial seizures and secondarily generalized tonic clonic seizures in adults. The Department of Veterans Affairs Epilepsy Cooperative Study No. 264 GroupN Engl J Med19923277657711298221
- SchillerYNajjarYQuantifying the response to antiepileptic drugs: effect of past treatment historyNeurology200870546518166707
- KalviaiinenRGentonPAndermannEBrivaracetam in patients with Unverricht-Lundborg disease: Results from two randomized, placebo-controlled, double-blind studiesEpilepsia2009504719682051
- RheimsSPeruccaECucheratMRyvlinPFactors determining response to antiepileptic drugs in randomized controlled trials. A systematic review and meta-analysisEpilepsia20115221923321269281
- SanderJWThe use of antiepileptic drugs – Principles and practiceEpilepsia200445283415315513
- Johannessen LandmarkCJohannessenSIPharmacological management of epilepsy: recent advances and future prospectsDrugs2008681925193918778117