
Abstract
Impaired fracture healing, especially when associated with bacterial infection, is a severe complication following long-bone fractures and requires special treatment. Because standard diagnostic techniques might provide falsely negative results, we evaluated the sonication method for detection of bacteria on implants of patients with fracture nonunions. A total of 49 patients with a nonunion (group NU) and, for comparison, 45 patients who had undergone routine removal of osteosynthetic material (group OM), were included in the study. Five different diagnostic methods (culture of tissue samples, culture of intraoperative swabs, histopathology of tissue samples, culture of sonication fluid, and 16S ribosomal DNA polymerase chain reaction of sonication fluid) were compared and related to clinical data. Among the diagnostic tests, culture of sonication fluid demonstrated by far the highest detection rate of bacteria (57%) in group NU, and rather unexpectedly 40% in group OM. Culture of sonication samples also revealed a broad spectrum of bacteria, in particular Propionibacterium spp. In conclusion, our results indicate that more bacteria can be detected on implants of patients with atrophic nonunions of long-bone fractures by means of the sonication procedure, which provides a valuable additional diagnostic tool to decide on a surgical procedure (eg, two-step procedure) and to further specify antimicrobial therapy.
Background
Fracture nonunions caused by bacterial infections still pose one of the most feared complications in the field of orthopedic surgery.Citation1 Therapy frequently consists of repeated and extensive debridement accompanied by prolonged antibiotic treatment, which puts patients at high risk of associated complications, reduces quality of life due to functional disabilities, and results in high socioeconomic costs.Citation2–Citation7
In particular, patients with open fractures are at risk of infection, but also patients with closed fractures and severe soft-tissue damage develop infections following osteosynthetic procedures.Citation8,Citation9 Staphylococcus aureus has been described as the main causative agent in approximately 50%–60% of cases,Citation10–Citation12 but recently other species also, such as Propionibacterium spp., have been linked to implant-associated infections.Citation13,Citation14
Infections of the bone are particularly difficult to treat, since bacteria form so-called biofilms on the implant surface, which make them more resistant to antibiotics and biocides.Citation15–Citation18 The diagnosis of biofilm infections by standard microbiological diagnostics (cultures of tissue samples or swabs) often yields falsely negative results, and it has been argued that up to 40% of cases are falsely deemed aseptic.Citation19–Citation21
Sonication of removed implants has led to an improved detection rate, because the majority of bacteria are attached to the implant surface, and thus can be gently removed.Citation22,Citation23 Aim of this study was to apply sonication to implants from patients with atrophic nonunions and compare the results with standard diagnostic techniques (culture of tissue samples, intraoperative swabs, histopathology of tissue samples). We hypothesized that more nonunions are associated with an infection and that sonication might demonstrate a broader spectrum of bacteria that so far has gone undetected. We also compared the results with implants from patients who had undergone routine removal of osteosynthetic material.
Materials and methods
Patient-derived material
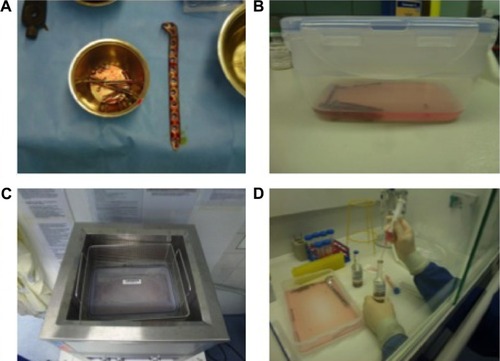
From March 2014 to September 2014, 94 patients were included in this study at the Clinic for Orthopedics and Trauma Surgery, Heidelberg University Hospital. A total of 49 patients were scheduled for surgery due to long-bone nonunion, and underwent implant removal or exchange (an example of a patient treated for fracture nonunion is shown in ). Diagnosis of nonunion was made due to patients’ complaints, clinical examination, and by conventional X-ray and/or computed tomography scan. The diagnosis of an infectious nonunion was based on clinical evaluation (reddening, swelling, hyperthermia, pain, pus intraoperatively, existence of a sinus tract) and laboratory results (elevated C-reactive protein [CRP] concentration and white cell count).
Figure 1 Treatment of an infectious nonunion by means of the Masquelet technique.
Abbreviation: PMMA, polymethyl methacrylate.

The criteria for an infection were a sinus tract, pus intraoperatively, or at least three positive signs just mentioned. During surgery, an intraoperative swab of the wound, as well as one to three tissue samples, were taken directly adjacent to the implant, and if possible each sample was divided and sent to the Microbiology Department and the Pathology Department for examination. In cases of very small tissue specimens, the entire sample was sent to the Microbiology Department.
Additionally, 45 patients who had undergone routine removal of osteosynthetic material were included in this study. There were no clinical or laboratory signs of an infection, and X-rays showed satisfactory fracture healing. Swabs and tissue samples were collected as described earlier, though due to small surgical incisions, only a limited number of tissue samples were available for histopathological analysis.
To test the sonication procedure for possible contamination, ten randomly chosen sterile screws were collected during different surgical procedures and treated according to the sonication protocol. All of these samples tested negative for bacterial contamination. All of the sonication samples were handled by one person only. The study was approved by the ethics committee of the Faculty of Medicine of Heidelberg University, and written informed consent was obtained from the patients.
Patient data
A total of 49 patients with nonunions (group NU) and 45 patients undergoing routine removal of osteosynthetic material (group OM) were included in the study. The patients’ average age was 49.3 (22–81) years for group NU and 45.2 (18–80) years for group OM. There were 15 female and 34 male patients in group NU, and 22 females and 23 males in group OM. None of the patients was under immunosuppressive therapy; 20.4% of group NU and 2.2% of group OM were diagnosed with diabetes (clinical data are summarized in ).
Table 1 Clinical data
Sonication of implants
The removed osteosynthetic materials (nails, screws, plates) were placed into sterile plastic boxes in various sizes depending on implant size (Bandelin Electronic GmbH & Co KG, Berlin, Germany) in the operating room. Enough Ringer’s solution to cover the implant was added (50–200 mL). They were then placed in an ultrasound bath (Ultrasonic TI-H 20; Elma Schmidbauer GmbH, Singen, Germany) and treated with ultrasonic power of 100% (250 W) and ultrasonic frequency of 45 kHz for 1 minute. These settings have been shown to detach bacteria from the implant surface while ensuring bacterial viability.Citation24 Following sonication, 10 mL of the fluid was placed into each aerobic and anaerobic blood-culture bottle (Bactec plus aerobic/anaerobic; BD, Franklin Lakes, NJ, USA) (). The bottles were incubated at 36°C until positive or for a maximum of 14 days in a Bactec FX (BD). Positive bottles were subcultured on Columbia 5% sheep-blood agar (BD), chocolate agar, MacConkey agar, and Streptococcus-selective (SCS) agar (all BioMérieux SA, Marcy-l’Etoile, France) until positive. All positive samples showed growth on the subculture the next day. Bacteria were identified by a matrix-assisted laser desorption/ionization time-of-flight (MALDI-TOF) mass spectrometer (Microflex; Bruker Corporation, Billerica, MA, USA). Susceptibility testing was done using the Vitek® 2 microbial identification system (BioMérieux). Additionally, eubacterial 16S ribosomal DNA (rDNA) polymerase chain reaction (PCR) was performed as previously described.Citation25
Figure 2 Sonication procedure.
Diagnostic procedures
Tissue samples were processed according to the following protocol. After arrival at the lab, the tissue was ground using a porcelain mortar, followed by the addition of 1 mL of 0.9% NaCl. This suspension was inoculated onto Columbia 5% sheep blood agar (BD), chocolate agar, MacConkey agar, SCS agar, Schaedler Neo Vanco +5% sheep blood (SNVS) agar (all BioMérieux), and thioglycolate broth (BD), and then Gram staining was performed. Plates and broth were incubated until positive or for a maximum of 5 days at 36°C in 5% CO2 or under anaerobic conditions. Identification of bacteria was done with the MALDI-TOF mass spectrometer. Susceptibility testing was done using the Vitek 2 microbial identification system.
For intraoperative swabs, the eSwab system was used. After arrival at the lab, 10 µL of liquid Amies was inoculated onto Columbia 5% sheep-blood agar (BD), chocolate agar, MacConkey agar, SCS agar, SNVS agar (all BioMérieux), and thioglycolate broth (BD), and then Gram staining was performed. Plates and broth were incubated for 2 days at 36°C in 5% CO2 or under anaerobic conditions. Identification and susceptibility testing was done as described earlier.
The incubation time was chosen according to microbiological expertise (swabs for 2 days and tissue samples for 5 days). Swabs were transported in liquid Amies transport media with flocked swabs. These swabs released their content completely into the transport medium, which was used for the inoculation of plates. On the other hand, the tissue had to be ground before inoculation, and part of it was put into an enrichment broth. Therefore, with tissue samples, sometimes there were cases that were not culture-positive until day 5.
For histopathological diagnostics, the samples were fixed in formalin and embedded in paraffin, and after the cutting slices of 2 µm thickness, routine hematoxylin–eosin staining was performed. The criterion for an implant-associated infection was at least 23 polymorphonuclear neutrophils per ten high-power fields.Citation26
Statistical tests
The concordance of the results of the five diagnostic methods and of the clinical evaluation was calculated using Cohen’s κ-test, and the interpretation of the test was as in Landis and Koch.Citation27 The correlation between CRP concentration/white blood cell count and culture of either sonication fluid or tissue samples was calculated by the Spearman test. With regard to the clinical data (), differences between groups were calculated using the unpaired t-test (age), Mann–Whitney U-test (number of previous surgeries at the same location), or Fisher’s exact test (all others).
Results
Evaluation of diagnostic methods in implant infections
Implants were removed from various locations (). Conventional microbial diagnostic of tissue samples and swabs was performed, as was histopathological examination of tissue samples. After sonication of the removed implant, the presence of bacteria in the fluid was assessed by conventional culture and eubacterial 16S rDNA PCR. As summarized in , more bacteria were detected following culture of sonication fluid (57.1% group NU, 40% group OM) compared to culture of tissue samples (10.2% group NU, 17.2% group OM), histology of tissue samples (9.3% group NU, 25% group OM), and PCR analysis of sonication fluid (11.9% group NU, 10.5% group OM). Culture of intraoperative swabs provided the least positive results (6.8% group NU, 0% group OM) (data summarized in ).
Table 2 Number of patient samples acquired from group NU and group OM, and number of positive results
Agreement or nonagreement of these five diagnostic methods was determined using Cohen’s κ-test. There was only one moderate agreement between culture of tissue samples and culture of intraoperative swabs; all other diagnostic tests revealed fair, slight, or no agreement (data summarized in ).
Table 3 Agreement of diagnostic methods
Clinical evaluation
Patients with nonunions were evaluated according to the aforementioned clinical criteria for an infection (see Materials and methods section). In this group, 16 of 49 patients (32.7%) showed signs suspicious of an infection. Using the Cohen κ-score, we compared the clinical evaluation of an infection with culture of sonication fluid and with culture of tissue samples. There was no agreement between clinical evaluation and culture of sonication fluid (κ<0) or 16S rDNA PCR of sonication fluid (κ<0); there was slight agreement between clinical evaluation and culture of tissue samples (κ=0.038), as well as culture of intraoperative swab (κ=0.006), and fair agreement between clinical evaluation and histopathology of tissue samples (κ=0.294).
Standard laboratory tests (CRP concentration and white cell count) were correlated with positive results of culture of sonication fluid and of culture of tissue samples by means of the Spearman test. We found no statistically significant correlation between these parameters.
Identification of bacterial species
We compared the bacterial species that were detected following culture of sonication fluid or culture of tissue samples ( and ). Culture of sonication fluid revealed a broader spectrum of bacteria, and in particular Propionibacterium spp. were detected more reliably than by culture of tissue samples. When tissue samples were positive, only one bacterial species was detected by culture of tissue samples. Bacteria detected by culture of tissue sample and culture of sonication fluid in the same case were not always concurrent ( and ).
Table 4 Bacterial species detected following culture of tissue samples and culture of sonication fluid of patients with nonunions (group NU)
Table 5 Bacterial species detected following culture of tissue samples and culture of sonication fluid of patients undergoing routine removal of osteosynthetic material (group OM)
We also tried mapping bacteria found in certain locations, but due to the limited number of patients included in this study and the considerable variety of bacteria, no significant differences in distribution of bacteria could be determined (Table S1).
Discussion
Our results showed that 57.1% of atrophic nonunions of long-bone fractures were associated with bacteria on the implant surface if culture of implant sonication is performed. The strengths of the study were prospective study design, thoroughly documented clinical data, existence of a comparison group, and random testing of the sonication method. Limitations of the study were the number of patients included not being sufficient for mapping of bacterial species (Table S1), varying number of tissue samples retrieved, lack of a generally accepted definition for implant-associated infections, and negative PCR results, possibly due to a dilution effect.
Fracture repair is a complex multistep process, which when disturbed may result in nonunion of the bone.Citation28 Bacterial infections are one possible reason for impaired fracture healing and diagnostics, and treatment of infectious nonunions still pose a challenge in the field of orthopedic surgery.Citation6,Citation8,Citation9,Citation11,Citation19,Citation20 Sonication of implants has led to an increased detection rate of bacteria in prosthetic joint infection.Citation22,Citation23 The aim of this study was to investigate whether more bacteria could be detected on implants of fracture non-unions by means of the sonication method.
In our study, culture of sonication fluid far outreached all other diagnostic methods, showing positive results in 57% of atrophic fracture nonunions. To test the sonication method for contamination, ten sterile screws were randomly chosen during different surgical procedures and processed according to the sonication protocol. Bacteria were not detected in any of these samples, making possible contamination during the sonication procedure unlikely. Culture of intraoperative swabs showed poor results, as previously described in the literature, and should therefore only be used if tissue samples or sonication are not available.Citation29
Using molecular methods to diagnose implant infections is controversial in the literature,Citation30 though a number of conclusive reports exist that advocate the use of such methods.Citation31,Citation32 We therefore speculated that molecular diagnostics might significantly enhance the detection rate of bacteria also in atrophic nonunions. Surprisingly, eubacterial 16S rDNA PCR of sonication fluid showed poor results when compared to culture of sonication fluid. This might have been due to a dilution effect in the sonication fluid, which might have produced falsely negative results. When evaluating the five different diagnostic methods, we found that the agreement between all of them was mostly fair or slight only (), leading us to the conclusion that a discrepancy of diagnostic tests cannot safely rule out an infection.
We also compared the results of group NU with group OM. Interestingly, 40% of group OM were positive by culture of sonication fluid, even though the implants did not cause any clinical problems and fracture healing was not impaired in these patients. This finding has been previously described by Obst et al.Citation32 According to their study, the majority of routinely removed implants were colonized, which raises the question whether bacterial biofilms on implants should be considered pathogenic at all and whether they are actually the cause of nonunions.
There are several possible explanations for this phenomenon. First, even though bacterial biofilms are not considered to be a highly aggressive form of life,Citation33 there might be differences in virulence between various bacterial strains and hence in clinical significance. Furthermore, even though the immune system is capable of recognizing and attacking biofilms,Citation34,Citation35 there are possible reasons as to why the immune system fails to eliminate biofilm infection in some cases.
First, it could be a matter of time: how fast a biofilm develops (how many bacteria are present) and how fast the immune system responds. Once a biofilm has formed and the immune system fails to cope with the infection, a persistent inflammatory response ensues, which leads to osteoclast generation and tissue degradation.Citation36,Citation37
Second, individual differences in the immune response have been described in association with nonunions. According to Szczęsny et al, genetic mutations, such as the TLR4 gene mutation 1/W, have been identified to be associated with ineffective recognition and elimination of bacteria, and thus predispose these patients to impaired fracture healing.Citation38 Our data showing improved detection of bacteria on osteosynthetic materials by means of the sonication method are in line with results by others.Citation39
The question of whether bacteria detected by culture of sonication fluid are truly pathogenic or whether the sonication method should be considered too sensitive for clinical practice is controversial among orthopedic surgeons. It has been suggested that the sonication results be verified by a number – at least 50 colony-forming units per plate – and to discard fewer bacteria as insignificant.Citation23 However, one should keep in mind that bacteria in biofilms adapt to altered environments (such as culture mediums) very slowly or not at all.Citation40,Citation41 There have also been reports of bacteria in a so-called viable but not culturable state, which could easily be misinterpreted as falsely negative if bacterial numbers are the sole criterion for an infection.Citation42,Citation43
Bacteria detected on implants of patients with atrophic nonunions should not be discarded as insignificant, because bacteria were also detected in 40% of patients without impaired fracture healing. As previously discussed, there are individual reasons why bacteria might add to the pathology of impaired fracture healing in some patients while the majority of fractures heal without complications, despite the presence of bacteria.
We were also interested in evaluating the type of bacteria that can be detected in fracture nonunions. Compared to other diagnostic tools, a wide spectrum of bacteria was found following sonication. Among those were Propionibacterium spp., which for a long time have been considered merely associated with skin-related diseases, but have been linked to implant infections as well.Citation13,Citation14 By means of the sonication procedure and by incubation for up to 14 days, we were able to detect propionibacteria that previously have gone unnoticed. In group OM, propionibacteria were even the most frequently detected bacteria (40%).
According to Grice et al,Citation44 a specific combination of bacteria can be found at sebaceous, moist, and dry-skin areas. We wondered whether a mapping of bacteria detected by implant sonication might offer a clue concerning the origin of bacteria (patient’s skin, contamination from surroundings in open fractures, intraoperative contamination), and hence specify antibiotic prophylaxis more precisely. However, due to the large variety of bacteria and the limited number of patients, no significant differences in the distribution of bacteria were able to be detected.
It is widely accepted, that Staphylococcus spp. make up 50%–60% of implant-associated infections, and S. aureus is thought the major causative agent of bone infections.Citation10–Citation12 In our study, 55% of bacteria found in group NU and 30% found in group OM were in fact Staphylococcus spp.; however, S. aureus was not detected in a single case in either group. This highlights once more that new diagnostic methods have enabled us to detect a wider spectrum of bacteria that seem to be associated with implant infections.
Conclusion
Our data show that bacteria detected on implants by culture of sonication fluid might contribute to the pathology of a large number of atrophic fracture nonunions, and that a previously underestimated variety of bacterial species might be associated with impaired fracture healing.
The pathogenicity of detected bacteria should be discussed in an interdisciplinary setting for each individual case, and further studies on clinical outcome following different treatment strategies might support our finding that culture of sonication fluid is a valuable additional tool to determine a surgical course of action (eg, Masquelet two-step procedure) and to improve antibiotic treatment.
Author contributions
All authors contributed toward data analysis, drafting and revising the paper and agree to be accountable for all aspects of the work.
Acknowledgments
This study was funded by the Center for Orthopedics, Trauma Surgery and Spinal Cord Injury, Heidelberg University Hospital. UD was supported by the Olympia-Morata-Scholarship of the Faculty of Medicine of Heidelberg University.
Supplementary material
Table S1 Distribution and number of bacterial species found by culture of sonication fluid: group NU and group OM
Disclosure
The authors report no conflicts of interest in this work.
References
- MoghaddamAZimmermannGHammerKBrucknerTGrütznerPAvon RecumJCigarette smoking influences the clinical and occupational outcome of patients with tibial shaft fracturesInjury201142121435144221665205
- PoultsidesLALiaropoulosLLMalizosKNThe socioeconomic impact of musculoskeletal infectionsJ Bone Joint Surg Am20109211e1320810849
- TsukayamaDTPathophysiology of posttraumatic osteomyelitisClin Orthop Relat Res1999360222910101307
- GaeblerCBergerUSchandelmaierPRates and odds ratios for complications in closed and open tibial fractures treated with unreamed, small diameter tibial nails: a multicenter analysis of 467 casesJ Orthop Trauma200115641542311514768
- StengelDBauwensKSehouliJEkkernkampAPorzsoltFSystematic review and meta-analysis of antibiotic therapy for bone and joint infectionsLancet Infect Dis20011317518811871494
- SchmidmaierGLuckeMWildemannBHaasNPRaschkeMProphylaxis and treatment of implant-related infections by antibiotic-coated implants: a reviewInjury200637Suppl 2S105S11216651063
- MoghaddamAElleserCBiglariBWentzensenAZimmermannGClinical application of BMP 7 in long bone non-unionsArch Orthop Trauma Surg20101301717619885667
- GustiloRBAndersonJTJSBS classics. Prevention of infection in the treatment of one thousand and twenty-five open fractures of long bones. Retrospective and prospective analysesJ Bone Joint Surg Am200284-A468211940635
- NoumiTYokoyamaKOhtsukaHNakamuraKItomanMIntramedullary nailing for open fractures of the femoral shaft: evaluation of contributing factors on deep infection and nonunion using multivariate analysisInjury20053691085109316054148
- ArciolaCRCampocciaDSpezialePMontanaroLCostertonJWBiofilm formation in Staphylococcus implant infections. A review of molecular mechanisms and implications for biofilm-resistant materialsBiomaterials201233265967598222695065
- CampocciaDMontanaroLArciolaCRThe significance of infection related to orthopedic devices and issues of antibiotic resistanceBiomaterials200627112331233916364434
- CorvecSPortilloMEPasticciBMBorensOTrampuzAEpidemiology and new developments in the diagnosis of prosthetic joint infectionInt J Artif Organs2012351092393423138706
- AubinGGPortilloMETrampuzACorvecSPropionibacterium acnes, an emerging pathogen: from acne to implant-infections, from phylotype to resistanceMed Mal Infect201444624125024656842
- PortilloMECorvecSBorensOTrampuzAPropionibacterium acnes: an underestimated pathogen in implant-associated infectionsBiomed Research International2013201380439124308006
- GristinaAGJenningsRANaylorPTMyrvikQNWebbLXComparative in vitro antibiotic resistance of surface-colonizing coagulase-negative staphylococciAntimicrob Agents Chemother19893368138162764528
- DonlanRMRole of biofilms in antimicrobial resistanceASAIO J2000466S47S5211110294
- FuxCACostertonJWStewartPSStoodleyPSurvival strategies of infectious biofilmsTrends Microbiol2005131344015639630
- CampocciaDMontanaroLBaldassarriLAnYHArciolaCRAntibiotic resistance in Staphylococcus aureus and Staphylococcus epidermidis clinical isolates from implant orthopedic infectionsInt J Artif Organs200528111186119116353126
- NelsonCLMcLarenACMcLarenSGJohnsonJWSmeltzerMSIs aseptic loosening truly aseptic?Clin Orthop Relat Res2005437253016056022
- ParviziJGhanemEMenasheSBarrackRLBauerTWPeriprosthetic infection: what are the diagnostic challenges?J Bone Joint Surg Am200688Suppl 413814717142443
- NeutDvan HornJRvan KootenTGvan der MeiHCBusscherHJDetection of biomaterial-associated infections in orthopaedic joint implantsClin Orthop Relat Res200341326126812897618
- TunneyMMPatrickSGormanSPImproved detection of infection in hip replacements. A currently underestimated problemJ Bone Joint Surg Br19988045685729699813
- TrampuzAPiperKEJacobsonMJSonication of removed hip and knee prostheses for diagnosis of infectionN Engl J Med2007357765466317699815
- DapuntULehnerBBurckhardtIZimmermannSHänschGMEwerbeckVEvaluation of implant sonication as a diagnostic tool in implant-associated infectionsJ Appl Biomater Funct Mater201412313514025199070
- SudaAJKommerellMGeissHKProsthetic infection: improvement of diagnostic procedures using 16S ribosomal deoxyribonucleic acid polymerase chain reactionInt Orthop201337122515252123917855
- MorawietzLClassenRASchröderJHProposal for a histopathological consensus classification of the periprosthetic interface membraneJ Clin Pathol200659659159716731601
- LandisJRKochGGThe measurement of observer agreement for categorical dataBiometrics1977331159174843571
- Ai-AqlZSAlaglASGravesDTGerstenfeldLCEinhornTAMolecular mechanisms controlling bone formation during fracture healing and distraction osteogenesisJ Dent Res200887210711818218835
- AggarwalVKHigueraCDeirmengianGParviziJAustinMSSwab cultures are not as effective as tissue cultures for diagnosis of periprosthetic joint infectionClin Orthop Relat Res2013471103196320323568679
- RyuSYGreenwood-QuaintanceKEHanssenADMandrekarJNPatelRLow sensitivity of periprosthetic tissue PCR for prosthetic knee infection diagnosisDiagn Microbiol Infect Dis201479444845324972853
- PortilloMESalvadóMSorliLMultiplex PCR of sonication fluid accurately differentiates between prosthetic joint infection and aseptic failureJ Infect201265654154822960370
- ObstUMartenSMNiessnerCHartwigEBacterial DNA from orthopedic implants after routine removalInt J Artif Organs201134985686222094566
- StewartPSCostertonJWAntibiotic resistance of bacteria in biofilmsLancet2001358927613513811463434
- GuentherFStrohPWagnerCObstUHänschGMPhagocytosis of staphylococci biofilms by polymorphonuclear neutrophils: S. aureus and S. epidermidis differ with regard to their susceptibility towards the host defenseInt J Artif Organs200932956557319856266
- GüntherFWabnitzGHStrohPHost defence against Staphylococcus aureus biofilms infection: phagocytosis of biofilms by polymorphonuclear neutrophils (PMN)Mol Immunol2009468–91805181319261332
- DapuntUMaurerSGieseTGaidaMMHänschGMThe macrophage inflammatory proteins MIP1α (CCL3) and MIP2α (CXCL2) in implant-associated osteomyelitis: linking inflammation to bone degradationMediators Inflamm2014201472861924795505
- DapuntUGieseTLasitschkaFLehnerBEwerbeckVHänschGMOsteoclast generation and cytokine profile at prosthetic interfaces: a study on tissue of patients with aseptic loosening or implant-associated infectionsEur J Inflamm2014121147159
- SzczęsnyGOlszewskiWLZagozdaMGenetic factors responsible for long bone fractures non-unionArch Orthop Trauma Surg2011131227528120730440
- YanoMHKlautauGBda SilvaCBImproved diagnosis of infection associated with osteosynthesis by use of sonication of fracture fixation implantsJ Clin Microbiol201452124176418225232155
- DonlanRMCostertonJWBiofilms: survival mechanisms of clinically relevant microorganismsClin Microbiol Rev200215216719311932229
- Hall-StoodleyLStoodleyPEvolving concepts in biofilm infectionsCell Microbiol20091171034104319374653
- OliverJDRecent findings on the viable but nonculturable state in pathogenic bacteriaFEMS Microbiol Rev201034441542520059548
- KuehlBMartenSMBischoffYBrenner-WeissGObstUMALDI-ToF mass spectrometry-multivariate data analysis as a tool for classification of reactivation and non-culturable states of bacteriaAnal Bioanal Chem201140151593160021769553
- GriceEAKongHHConlanSTopographical and temporal diversity of the human skin microbiomeScience200932459311190119219478181