
Abstract
This review summarizes the epidemiological trend, risk factors, prevention strategies such as vaccination, staging, current novel therapeutics, including the drugs under clinical trials, and future therapeutic trends for hepatocellular carcinoma (HCC). As HCC is the third most common cause of cancer-related death worldwide, its overall incidence remains alarmingly high in the developing world and is steadily rising across most of the developed and developing world. Over the past 15 years, the incidence of HCC has more than doubled and it increases with advancing age. Chronic infection with hepatitis B virus is the leading cause of HCC, closely followed by infection with hepatitis C virus. Other factors contributing to the development of HCC include alcohol abuse, tobacco smoking, and metabolic syndrome (including obesity, diabetes, and fatty liver disease). Treatment options have improved in the past few years, particularly with the approval of several molecular-targeted therapies. The researchers are actively pursuing novel therapeutic targets as well as predictive biomarker for treatment of HCC. Advances are being made in understanding the mechanisms underlying HCC, which in turn could lead to novel therapeutics. Nevertheless, there are many emerging agents still under clinical trials and yet to show promising results. Hence, future therapeutic options may include different combination of novel therapeutic interventions.
Introduction
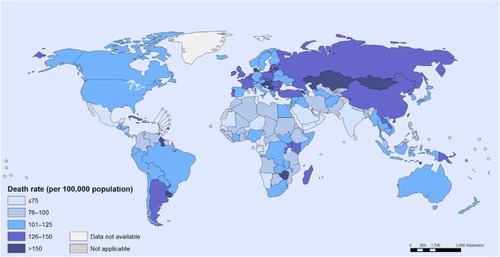
Hepatocellular carcinoma (HCC) is defined as the carcinoma emanating from the liver and also includes various underlying diseases.Citation1,Citation2 Globally, the cancer prevalence was reported to be 10.9 million per annum, and liver cancer came up as the sixth most common cancer with 749,000 casesCitation1,Citation2 and was ranked the third highest cause of cancer-related death with 692,000 mortalities per year.Citation1 However, its geographical distribution is not uniformCitation1–Citation3 as shown in .Citation4 The highest HCC incidence occurs in resource-poor or developing countries such as sub-Saharan African, East Asia, and Melanesia, which covers 85% of reported global cases.Citation2,Citation3,Citation5 Contrarily, incidence in developed countries is much lower, except in Southern Europe.Citation2,Citation3 To date, the mortality rate in the USA increased by 40% between the years of 1990 and 2004 as a result of hepatitis C virus (HCV) events.Citation2
Figure 1 Cancer mortality: age-standardized death rate per 100,000 population, both sexes, 2008.
Furthermore, HCC incidences increase with advancing age.Citation1,Citation3,Citation6 The peak age for HCC incidence is at 70 years.Citation2,Citation3,Citation7 However, peak age of incidence is less than 70 years in Chinese and black Africans.Citation2,Citation5,Citation7 With regard to sex, it strikes males more than females, with a ratio of 2.4.Citation3,Citation6,Citation7 Last decade, HCC mortality rose, particularly for male population in Austria, Denmark, Germany, Greece, Ireland, Portugal, Norway, Spain, Switzerland, and UK.Citation2,Citation3 This paper aims first at describing the current and future therapeutic trends in HCC management, second at identifying the preventative measures in lowering the incidence of HCC, and finally at reviewing the progress in novel therapeutics in developing and developed regions.
Risk factors
These variations of risk factors link to etiology, complexity, and geographical distribution, particularly between developing and developed regions ().Citation1
Table 1 The common risk factors in HCC
Risk of HCC according to HBV genotype
Individuals with chronic hepatitis B virus (HBV) infection are at increased risk of developing end-stage liver disease (including cirrhosis, hepatic failure, and HCC), with a cumulative lifetime incidence of 15%–40%.Citation11–Citation13 Other important risk factors for HCC include the presence of HBV e-antigen – a surrogate marker of active viral replication – and the amount of HBV (ie, viral load) in serum.Citation14,Citation15
Several reportsCitation16–Citation19 have also suggested that the genetic characteristics of HBV, including HBV genotype and specific genetic mutations, are associated with the development of HCC. Most of the recent studies suggest that the genetic characteristics of HBV, including HBV genotype and specific genetic mutations, are associated with the development of HCC.Citation20–Citation22
To date, HBV has been classified in to eight genotypes (A–H), according to intergroup divergence of 8% or more in the complete nucleotide sequence.Citation23 Recent focus is on the clinically important differences in outcomes that are associated with the different HBV genotypes.Citation24 The HBV genotypes have distinct geographical distributionsCitation25 and have been reported to have clinical relevance.Citation26 For example, patients with genotypes C and D have a higher risk of disease progression and a poorer clinical outcome compared to the patients with genotypes A and B. Patients with genotypes A and B have a better response to IFN-based therapy than those with genotypes C and D.Citation27 However, the association of genotypes B and C with HCC development remains controversial; some studies have shown that genotype C HBV infection is a risk factor for HCC,Citation28,Citation29 while others did not obtain the same results.Citation30,Citation31 The reason for these inconsistencies between the results, especially those derived from the same region,Citation28,Citation32 is unclear.
Staging
Introduction of various staging systems by different guide-lines helps select the suitable interventions according to HCC classificationsCitation1,Citation3,Citation5,Citation6,Citation33 ( and ).
Table 2 Child–Pugh classification of severity of liver disease
Table 3 BCLC staging
Management
Treatment
Resection
Resection is the first-line therapy for localized HCC without cirrhosis.Citation3,Citation5,Citation6,Citation34–Citation37 Resection is not recommended in cirrhotic patients due to increased risk of perioperative decompensation.Citation6,Citation37,Citation38 Nevertheless, resection is possible in cirrhotic patients whose liver transplantation (LT) is deemed to be unsuitable, provided that their hepatic function is well preserved.Citation1,Citation34
Portal vein hypertension is regarded as an absolute contraindication to resection in EASL–EORTC Clinical Practice Guidelines.Citation3,Citation35 Studies demonstrated that the 5-year survival rate is only 30% regardless of the Child–Pugh score in the presence of portal vein hypertension and elevated bilirubin level, compared to 70% 5-year survival in patients with normal bilirubin level without portal vein hypertension.Citation34,Citation37 However, in other studies, it was also demonstrated that the presence of significant portal vein hypertension does not influence the outcomes of resection, even in cirrhotic patients.Citation38,Citation39
Larger tumor is associated with higher risk of vascular invasion and dissemination.Citation34 A cutoff of <2 cm was demonstrated as an independent predictor of survival rates in Japan, and the outcomes of each groups were 66% 5-year survival in <2 cm tumor group, 52% in 2–5 cm tumor group, and 37% in >5 cm tumor group after resection procedure.Citation3
Recurrence rate occurs up to 70% after 5 years is the main problem with resection.Citation1,Citation34,Citation37 However, the evidence to demonstrate the effectiveness of initiating adjunct therapy after resection in preventing recurrence is not conclusive.Citation5,Citation34
Liver transplantation
LT is the best curative therapy for candidates unsuitable to undergo liver resection as well as for patients with underlying cirrhosis. However, dismal results as in high recurrence rate and 5-years survival rates below 50% have been recorded due to poor patient selection.Citation6,Citation37
Generally, LT can only be performed in patients in early stage of HCC.Citation34,Citation38 Milan criteria defined patients with single nodule <5 cm, or up to three separate nodules <3 cm, with no evidence of gross vascular invasion and no regional nodal or distant metastases.Citation5,Citation40,Citation41 Using Milan criteria of patient selection, posttransplantation outcome with 5-year survival rates exceeds 70% (as shown in several studies).Citation34,Citation35
Nevertheless, shortage of donor livers has caused an unbearably long transplant waiting time,Citation34,Citation35 resulting in waiting list exclusion when patients’ HCC progression extends beyond the transplantable criteria.Citation42 The rate of waiting list exclusion may be as high as 25% if the waiting list is longer than 12 months.Citation34,Citation35 Model for End-stage Liver Disease score was therefore utilized to allocate the organ fairly according to priority.Citation34,Citation35,Citation41
Neoadjuvant therapy, such as chemoembolization and percutaneous ablation, can be employed to maintain the tumor burden within the ranges of the Milan criteria and prevent dropout from the waiting list, especially if transplant waiting time exceeds 6 months and patient’s condition worsens.Citation6,Citation34,Citation35 However, the long-term benefit of the therapy is still uncertain as there are several studies showing no survival benefit in employing these interventions.Citation37,Citation41
Percutaneous ablation
Percutaneous ablation is the best treatment option for patients with early-stage HCC (BCLC 0-A tumors) who are not suitable for resection or LT.Citation34,Citation35 The most common techniques are percutaneous ethanol injection (PEI) and radiofrequency ablation (RFA).Citation36 Currently, RFA has progressively replaced PEICitation35,Citation37,Citation38 because RFA requires lesser treatment sessions and results in higher complete necrosis rate and long-term survival rates than PEI, as demonstrated in many studies.Citation43–Citation46
When comparing therapeutic outcomes of RFA with surgical resection, resection is more effective than RFA for larger tumors (>3, <5 cm) in terms of disease-free survival and overall survival, while RFA is more cost-effective than surgical resection for smaller early HCCs (<2 cm).Citation47,Citation48
Chemoembolization
Chemoembolization is used as a palliative treatment for patients with inoperable HCC.Citation49 It is the recommended first-line therapy for patients with intermediate-stage (BCLC stage B) disease having well-preserved liver function and asymptomatic multinodular tumors without vascular invasion or extrahepatic spread ().Citation3
Table 4 Types of chemoembolization
Another technique called radioembolization, involving infusion of Iodine-131 or Yttrium-90 into hepatic artery, has been shown to exhibit antitumor results, but it is not recommended as a standard therapy as further research trials are needed to evaluate the efficacy.Citation3
Systemic therapies
Perspectives on drug therapies
HCC is among the most chemoresistant tumors, and until 2007, no systemic chemotherapy was recommended for patients with advanced tumors ( and ).Citation51–Citation53 Systemic chemotherapy with cytotoxic agents, such as doxorubicin, gemcitabine, cisplatin, 5-fluorouracil, or combined regimens for palliative care, was associated with low response rates (<10%) with only marginal improvements in survival. Moreover, these drugs are poorly tolerated in patients with underlying liver cirrhosis. Interferon (IFN) therapy, anti-androgens, or tamoxifen used in the treatment of advanced HCC show contradictory results without obvious benefit. A meta-analysis of seven RCTs, including 898 patients, evaluated tamoxifen versus conservative management and showed neither antitumor effects nor survival benefits for tamoxifen. Subsequent large RCTs reported negative results in terms of survival. Cisplatin, IFN, doxorubicin, and fluorouracil (PIAF) used in combination showed promising activity in a Phase II study. A randomized Phase III study including 188 patients with HCC was conducted to investigate the effect of PIAF combination compared to doxorubicin alone. The median survival rate of the PIAF group did not significantly differ from the doxorubicin group (8.67 versus 6.83 months), and patients treated with the PIAF regimen experienced a significantly higher rate of myelotoxicity.Citation50–Citation53
Table 5 Molecular-targeted therapies
Table 6 HBsAg carriers before and after initiate universal vaccination in high HBV prevalence countries
Prevention
Understanding risk factors of HCC supports the rationale for designing of prevention strategies, which aids in avoiding infection, chronic liver damage, and carcinogenesis process as well as early diagnosis of the disease and reduces the risk of recurrence.Citation54,Citation55
Vaccination
HBV is attributable to more than 50% of the cases of HCC globally, it accounts for 15% of HCC in developed countries and 80%–90% of HCC in developing countries such as Asia and Africa.Citation54,Citation55 World Health Organization (WHO) introduced universal vaccination to all newborns and high-risk groups as routine immunization.Citation54,Citation56 Most of the studies showed that hepatitis B core antibody, hepatitis B surface antigen (HBsAg) carriers, HCC incidence, and HCC-related mortality were decreased following initiation of universal vaccination ().Citation57–Citation61 Therapies stratified according to stage along with the treatment strategies and rational of HCC were summarized ().Citation62–Citation65
Table 7 Therapies stratified according to stage
Antiviral treatment
Studies have shown that antiviral treatment of chronic HBV and HCV infections may reduce the risk of HCC.Citation3,Citation37,Citation66 Chen et alCitation14 demonstrated that incidence of HCC is associated with serum HBV DNA, which further supports the analysis showing that low viremia levels decreases the risk of HCC development. Therefore, antiviral therapy is used for HCC risk reduction, while viral suppression also reverses cirrhosis, another risk factor of HCC development.Citation66,Citation67
Oral nucleoside analogs (NAs) have been used to treat chronic hepatitis B.Citation67 The use of first-generation NA is limited due to the development of resistance and virological relapse after treatment cessation.Citation61 Newer generation NA with high antiviral and low drug-resistant potency, such as entecavir and tenofovir, are available.Citation66,Citation68 At the same time, combination therapy of pegylated IFN with ribavirin works well in preventing HCC development associated with HCV infection.Citation68,Citation69
Surveillance
Surveillance is a diagnostic test applied periodically to patients at risk of developing a disease, aiming to reduce disease-related mortality through early diagnosis ().Citation3,Citation35
Table 8 Categories of patients suitable for surveillance
Serological and imaging tests are used in HCC surveillance, ultrasonography is the most widely used.Citation3 Surveillance is mainly based on ultrasound examination as measuring alpha-fetoprotein levels, which is an example of serological test, has demonstrated inadequate sensitivity and specificity in recent studies.Citation35
Other preventive measures
WHO recommends implementation of an integrated and comprehensive strategy based on five key elements as listed in , aiming at preventing transfusion-transmitted HBV and HCV infection, especially in sub-Saharan African countries where there is relatively high risk of such mode of transmission. On the other hand, risky behaviors such as tattooing, body piercing, and unprotected sexual intercourse should be avoided to prevent transmission of HCV and HBV, along with implementation of related health policies by governmental health agencies ().Citation3,Citation55,Citation70
Table 9 Strategy to prevent transfusion-transmitted HBVand HCVinfection by WHO
Discussion
Current novel therapeutics
Surgical intervention that includes liver resection and LT is the mainstay of treatment of HCC, but the selection criteria for both differ in different published clinical guidelines, resulting in difficulty in selecting the most appropriate therapy in treating HCC.Citation74–Citation79 Certain groups of patients who are defined to have well-preserved liver function and are deemed to be fit to undergo resection (Child–Pugh A score) may be regarded as not suitable for resection due to other circumstances such as the presence of portal vein hypertension.
Meanwhile, the gold standard in selecting patients for LT, Milan criteria, possesses some limitations that may exclude some of the potential patients.Citation18 University of California at San Francisco criteria have been proposed, in which selection is based on having a single tumor nodule up to 6.5 cm or three or fewer tumors, the largest of which is <4.5 cm with the sum of the tumor diameters <8 cm.Citation80 Its outcome is comparable to patients who are selected by using Milan criteria.Citation40 Nevertheless, more studies should be conducted to confirm the validity of this extended criteria. However, it is still preferable to establish a standardized universal classification system in evaluating the liver status in patients with HCC to ensure the most appropriate option is selected for the patients, for both resection and LT procedure.
To date, sorafenib is the first and only available systemic therapy approved by FDA for treatment of HCC.Citation3 Nevertheless, many emerging agents are still under clinical trials and yet to show promising results.Citation51,Citation81
Future therapeutic trends
Living donor liver transplantation (LDLT) is proposed as it provides advantages to reduce the waiting time and increase the number of patients benefit from LT due to severe short-age of deceased donor livers. By comparing LDLT with deceased donor liver transplantation (DDLT), the waiting time is significantly shorter and dropout rate has reduced from 18% to 0%.Citation40 However, it is still uncertain whether the outcome of LDLT is equivalent or more favorable to that of DDLT.Citation82
For tumors with size <2 cm and with the BCLC stage A, both PEI and RFA achieve complete responses in more than 90% of cases with good long-term outcome, which may substitute the roles of surgical intervention in early HCC in the future. In future, technical developments may achieve ablation areas of 5 cm or more in diameter, which will make percutaneous ablation an effective alternative to surgery even for tumors measuring 3 cm or more.Citation38
Future therapeutic options may include different combination of novel therapeutic interventions. Combination of TACE-DEB has lesser complications than TACE due to slow release of chemotherapeutic drug.Citation83 TACE-DEB was also better tolerated and significantly decreased liver toxicity and adverse events and showed improved antitumoral effect.Citation3,Citation84
There are also studies revealing the possibility of combination therapy of sorafenib with either TACE or radioembolization as both these combinations had demonstrated better therapeutic outcomes with improved overall survival and time to progression.Citation3,Citation39,Citation83,Citation84 More studies need to be conducted to examine this possibility as well as to solve the uncertainties regarding dose, frequency, and duration of sorafenib in combination therapy.
Universal vaccination is also one of the therapeutics interventions for HCC, especially in developing countries. A cost-effectiveness analysis by Hung and ChenCitation84 demonstrated that universal vaccination shows high cost-effectiveness in reducing long-term sequelae of acute hepatitis B infection, HCC death, and chronic illnesses,Citation56,Citation85 which is further supported by another cost-effectiveness analysis by Hong et alCitation85 in Vietnam.Citation80
However, an effective prophylaxis vaccine for HCV is not yet available. Thus, preventing HCC is completely dependent on antiviral therapy for patients, until an effective vaccine is developed.Citation68 Antiviral therapy with nucleotide analogs may be preferable than IFN treatment due to less adverse side effects and can be considered as a cost-effective adjuvant therapy for HCC after curative treatment.Citation80 However, the exact role of antiviral treatment in preventing HBV-related HCC has been difficult to establish, due to the slow biological evolution of HBV.Citation66
Future technical aspect or extended indications for liver resection for HCC
Recent improvement in surgical techniques and perioperative care has increased the safety and expanded the indication of hepatic resection for HCC to include large tumors that require extended hepatectomy in cirrhotic patients. Selection of appropriate candidates for hepatectomy depends on careful assessment of the tumor status and liver function reserve. Evaluation of the general fitness of patients is also critical because comorbid illness is an important cause of postoperative mortality, even if the patients have good liver function reserve. With careful patient selection and surgical expertise, the current operative mortality of hepatectomy for HCC is approximately 5% or less in major centers. Improved long-term survival results after resection of HCC have also been reported recently, with an overall 5-year survival rate of approximately 50%. The improved perioperative and long-term survival results have strengthened the role of hepatectomy as the mainstay of treatment for HCC despite the availability of a number of other treatment options for localized HCC.Citation86
The main clinical advantage of laparoscopy for cirrhotic patients is probably the significantly lower rate of post-operative ascitic decompensation, which was reported in four comparative studies and three meta-analysis. This finding could be explained by the preservation of portosystemic venous collateral circulation around the liver and parietal abdominal wall, limited mobilization and manipulation of the liver, restricted fluid requirements, and decreased blood loss. Gaillard et alCitation87 advocated that the positive pressure of the pneumoperitoneum might exert a tamponade effect on bleeding from intra-abdominal varices, which are a low-pressure system, thus decreasing blood loss. Lower blood transfusion requirement is also an advantage of the laparoscopic approach in this very risky group of patients.Citation87
Disclosure
The authors report no conflicts of interests in this work.
References
- RaoulJNatural history of hepatocellular carcinoma and current treatment optionsSemin Nucl Med2008382S13S1818243838
- KewMHepatocellular carcinoma: epidemiology and risk factorsJ Hepatocellular Carcinoma2014115125
- EASL–EORTC Clinical Practice Guidelines: management of hepatocellular carcinomaEur J Cancer201248559964122424278
- World Health Organization [Internet]WHO: cancer mortality and morbidity Available from: http://www.who.int/gho/ncd/mortality_morbidity/cancer/en/Accessed December 23, 2014
- JelicSSotiropoulosGHepatocellular carcinoma: ESMO clinical practice guidelines for diagnosis, treatment and follow-upAnn Oncol201021Suppl 5v59v6420555104
- RyderSGuidelines for the diagnosis and treatment of hepatocellular carcinoma (HCC) in adultsGut200352Suppl 31iii812477745
- HaNHaNAhmedARisk factors for hepatocellular carcinoma in patients with chronic liver disease: a case–control studyCancer Causes Control201223345546222258434
- KityaDBbosaGMulogoEAflatoxin levels in common foods of South Western Uganda: a risk factor to hepatocellular carcinomaEur J Cancer Care2009194516521
- IgbohNMNnamahNKOnwubikoDHepatic dysfunction in patients infected with human immune deficiency virusInt J Pharma Res Rev201324912
- TrichopoulosDBamiaCLagiouPHepatocellular carcinoma risk factors and disease burden in a European cohort: a nested case-control studyJ Natl Cancer Inst2011103221686169522021666
- YangHYehSHChenPJAssociations between hepatitis b virus genotype and mutants and the risk of hepatocellular carcinomaJ Natl Cancer Inst2008100161134114318695135
- BeasleyRPHepatitis B virus. The major etiology of hepatocellular carcinomaCancer19886110194219562834034
- McMahonBJHepatocellular carcinoma and viral hepatitisWilsonRAViral Hepatitis: Diagnosis, Treatment, PreventionNew York, NYMarcel Dekker199731530
- ChenCJYangHISuJRisk of hepatocellular carcinoma across a biological gradient of serum hepatitis B virus DNA levelJAMA200629516573
- YangHILuSNLiawYFHepatitis B e antigen and the risk of hepatocellular carcinomaN Engl J Med2002347316874
- BaptistaMKramvisAKewMCHigh prevalence of 1762(T) 1764(A) mutations in the basic core promoter of hepatitis B virus isolated from black Africans with hepatocellular carcinoma compared with asymptomatic carriersHepatology199929394653
- KaoJHChenPJLaiMYChenDSHepatitis B genotypes correlate with clinical outcomes in patients with chronic hepatitis BGastroenterology200011835549
- KaoJHChenPJLaiMYChenDSBasal core promoter mutations of hepatitis B virus increase the risk of hepatocellular carcinoma in hepatitis B carriersGastroenterology2003124232734
- YuMWYehSHChenPJHepatitis B virus genotype and DNA level and hepatocellular carcinoma: a prospective study in menJ Natl Cancer Inst200597426572
- MishraSKHepatitis B virus genotypes, mutations and the risks for hepatocellular carcinomaGastroenterol Hepatol Open Access2014110000210.15406/ghoa.2014.01.00002
- KaoJHChenPJLaiMYChenDSHepatitis B genotypes correlate with clinical outcomes in patients with chronic hepatitis BGastroenterology2000118355455910702206
- YuMWYehSHChenPJHepatitis B virus genotype and DNA level and hepatocellular carcinoma: a prospective study in menJ Natl Cancer Inst200597426527215713961
- ChanHL-YHuiAYWongMLGenotype C hepatitis B virus infection is associated with an increased risk of hepatocellular carcinomaGut2004531494149810.1136/gut.2003.03332415361502
- OritoEIchidaTSakugawaHGeographic distribution of hepatitis B virus (HBV) genotype in patients with chronic HBV infection in JapanHepatology200134359059411526547
- HuyTTSallAAReynesJMAbeKComplete genomic sequence and phylogenetic relatedness of hepatitis B virus isolates in CambodiaVirus Genes200836229930518264750
- KaoJHHepatitis B viral genotypes: clinical relevance and molecular characteristicsJ Gastroenterol Hepatol200217664365012100608
- LinCLKaoJHThe clinical implications of hepatitis B virus genotype: recent advancesJ Gastroenterol Hepatol201126Suppl 112313021199523
- ChanHLHuiAYWongMLGenotype C hepatitis B virus infection is associated with an increased risk of hepatocellular carcinomaGut200453101494149815361502
- YuMWYehSHChenPJHepatitis B virus genotype and DNA level and hepatocellular carcinoma: a prospective study in menJ Natl Cancer Inst200597426527215713961
- SumiHYokosukaOSekiNInfluence of hepatitis B virus genotypes on the progression of chronic type B liver diseaseHepatology2003371192612500184
- YuenMFTanakaYShinkaiNRisk for hepatocellular carcinoma with respect to hepatitis B virus genotypes B/C, specific mutations of enhancer II/core promoter/precore regions and HBV DNA levelsGut20085719810217483190
- YuenMFSablonEYuanHJSignificance of hepatitis B genotype in acute exacerbation, HBeAg seroconversion, cirrhosis-related complications, and hepatocellular carcinomaHepatology200337356256712601354
- RobertLOkenMCreechRToxicity and response criteria of the Eastern Cooperative Oncology GroupAm J Clin Oncol1982566496557165009
- BruixJShermanMPractice Guidelines Committee, American Association for the Study of Liver DiseasesManagement of hepatocellular carcinomaHepatology20054251208123616250051
- BruixJShermanMPractice Guidelines Committee, American Association for the Study of Liver DiseasesManagement of hepatocellular carcinoma: an updateHepatology20115331020102221374666
- LiovetJMBruixJNovel advancements in the management of hepatocellular carcinoma in 2008J Hepatol200848S20S3718304676
- DhanasekaranRLimayeACabreraRHepatocellular carcinoma: current trends in worldwide epidemiology, risk factors, diagnosis, and therapeuticsHepat Med20124193724367230
- RazaASoodGKHepatocellular carcinoma review: current treatment, and evidence-based medicineWorld J Gastroenterol201420154115412724764650
- SantambrogioRKlugerMDCostaMHepatic resection for hepatocellular carcinoma in patients with Child-Pugh’s A cirrhosis: is clinical evidence of portal hypertension a contraindicationHPB (Oxford)201215788423216782
- TsoulfasGCurleySAAbdallaEKBarnettCCHertlMLiver transplantation for hepatocellular carcinomaUpToDate2013
- EASL-EORTC clinical practice guidelines: management of hepatocellular carcinomaJ Hepatol20125690894322424438
- de VillaVLoCMLiver transplantation for hepatocellular carcinoma in AsiaOncologist201212111321133118055852
- LivraghiTGoldbergSNLazzaroniSMeloniFSolbiatiLGazelleGSSmall hepatocellular carcinoma: treatment with radio-frequency ablation versus ethanol injectionRadiology1999210365566110207464
- LencioniRAAllgaierHPCioniDSmall hepatocellular carcinoma in cirrhosis: randomized comparison of radio frequency thermal ablation versus percutaneous ethanol injectionRadiology200322823524012759473
- AnsariDAnderssonRRadiofrequency ablation or percutaneous ethanol injection for the treatment of liver tumorsWorld J Gastroenterol201218101003100822416173
- ChaDILeeMWRhimHChoiDKimYSLimHKTherapeutic efficacy and safety of percutaneous ethanol injection with or without combined radiofrequency ablation for hepatocellular carcinomas in high risk locationsKorean J Radiol201314224024723483664
- ColecchiaASchiumeriniRCucchettiAPrognostic factors for hepatocellular carcinoma recurrenceWorld J Gastroenterol201420205935595024876717
- (a)CucchettiAPiscagliaFCesconMCost-effectiveness of hepatic resection versus percutaneous radiofrequency ablation for early hepatocellular carcinomaJ Hepatol20135930030723603669 (b)KangBKimH-CChungJWSafety of chemotherapeutic infusion or chemoembolization for hepatocellular carcinoma supplied exclusively by the cystic arteryCardiovasc Intervent Radiol20133651313131923262478
- LloverJMRicciSMazzaferroVHilgardPSorafenib in advanced hepatocellular carcinomaN Engl J Med200835937839018650514
- ChengA-LKangY-KLinD-YSunitinib versus sorafenib in advanced hepatocellular cancer: results of a randomized phase III trialJ Clin Oncol201331324067407524081937
- IllanuevaALlovetJMTargeted therapies for hepatocellular carcinomaGastroenterology20111401410142621406195
- LlovetJMBruixJTesting molecular therapies in hepatocellular carcinoma: the need for randomised phase II trialsJ Clin Oncol200927683383519139428
- PerzJFArmstrongGLFarringtonLAHutinYJBellBPThe contributions of hepatitis B virus and hepatitis C virus infections to cirrhosis and primary liver cancer worldwideJ Hepatol20064552953816879891
- AnnaGNoraCAdrianaSVeronicaVFabioFHepatitis B virus-related hepatocellular carcinoma: primary, secondary, and tertiary preventionEur J Cancer Prev20112038138821540746
- World Health OrganizationHepatitis B vaccine2005 Available from: http://www.who.int/vaccines/en/hepatitisb.shtml/shtml#strategiesAccessed October 23, 2015
- ChanCYLeeSDLoKJLegend of hepatitis B vaccination: the Taiwan experienceJ Gastroenterol Hepatol200419212112614731119
- VivianiSJackAHallAJHepatitis B vaccination in infancy in The Gambia: protection against carriage at 9 years of ageVaccine1999172946295010462228
- NgKPSawTLBakiAImpact of expanded program of immunization against hepatitis B infection in school children in MalaysiaMed Microbiol Immunol200519416316815834754
- SharmaNKandpalJNautiyalSCReal time PCR usage in the quantification of hepatitis B virus DNA – clinical applications in disease managementInt J Pharma Res Rev2013264551
- LiangXBiSYangWEpidemiological Serosurvey of hepatitis B in China – declining HBV prevalence due to hepatitis B vaccinationVaccine2009276550655719729084
- Fernandez-RodriguezCMGutiérrez-GarcíaMLPrevention of hepatocellular carcinoma in patients with chronic hepatitis BWorld J Gastroinstest Pharmacol Ther201453175182
- BruixJHessheimerAJFornerABoixLVilanaRLlovetJMNew aspects of diagnosis and therapy of hepatocellular carcinomaOncogene2006253848385616799626
- DufourJFBargelliniIDe MariaNDe SimonePGoulisIMarinhoRTIntermediate hepatocellular carcinoma: current treatments and future perspectivesAnn Oncol201324Suppl 2ii24ii2923715940
- LinSHoffmannKSchemmerPTreatment of hepatocellular carcinoma: A systematic reviewLiver Cancer201213–414415824159579
- GomaaAIWakedIRecent advances in multidisciplinary management of hepatocellular carcinomaWorld J Hepatol20157467368725866604
- ChanHLWongGLTseCHChanHYWongVWViral determinants of hepatitis B surface antigen seroclearance in hepatitis B antigen negative chronic hepatitis B patientsJ Infect Dis2011204340841421742839
- The 5th Asia-Pasific Primary Liver Cancer Expert Meeting (APPLE 2014)ChengALHsuCHHsuCA Bridge to a Consensus on HCC ManagementTaipei, Taiwan20143285397
- UenoYSollanoJDFarrellGCPrevention of hepatocellular carcinoma complicating chronic hepatitis CJ Gastroenterol Hepatol20092453153619368633
- MarianoAMeleATostiMERole of beauty treatment in the spread of parenterally transmitted hepatitis viruses in ItalyJ Med Virol20047421622015332269
- CDCProgress toward prevention of transfusion-transmitted hepatitis B and hepatitis C infection – Sub-Saharan Africa, 2000–2011MMWR2014632961361925055184
- CDCProgress toward strengthening national blood transfusion services – 14 countries, 2008–2010MMWR20116015781582
- World Health OrganizationBlood safety and availability2013 Available from: http://www.who.int/mediacentre/factsheets/fs279/en/index.htmlAccessed October 23, 2015
- KandaTNakamotoSWuSYokosukaONew treatments for genotype 1 chronic hepatitis C – focus on simeprevirTher Clin Risk Manag20141038739424920913
- GentileIBuonomoARZappuloEMAsunaprevir, a protease inhibitor for the treatment of hepatitis C infectionTher Clin Risk Manag20141049350425061308
- ValadezJAJuárezIGGPedreroRRTorreAManagement of chronic hepatitis C virus infection in patients with end-stage renal disease: a reviewTher Clin Risk Manag20151132933825767389
- KarnsakulWAlfordMKSchwarzKBManaging pediatric hepatitis C: current and emerging treatment optionsTher Clin Risk Manag2009565166019707281
- ChaeHBHannHWTime for an active antiviral therapy for hepatitis B: an update on the management of hepatitis B virus infectionTher Clin Risk Manag20073460561218472982
- DhillonRRossiSHerrineSKPegylated interferon 2a and 2b in combination with ribavirin for the treatment of chronic hepatitis C in HIV infected patientsTher Clin Risk Manag20084478979619209261
- MazzaferroVChunYSPoonRTPLiver transplantation for cellular carcinomaAnn Surg Oncol20081541001100718236119
- ChongCCNWongGLHWongVWSLeeKFLaiPBSChanHLYRole of anti-viral therapy on hepatitis B virus (HBV)-related hepatocellular carcinoma (HCC)Liver Tumors – Epidemiology, Diagnosis, Prevention and Treatment2013 Available from: http://www.intechopen.com/books/liver-tumors-epidemiology-diagnosis-prevention-and-treatment/role-of-anti-viral-therapy-on-hepatitis-b-virus-hbv-related-hepatocellular-carcinoma-hcAccessed October 23, 2015
- LiapiEGeschwindJFHTranscatheter arterial chemoembolization for liver cancer: is it time to distinguish conventional from drug-eluting chemoembolizationCardiovasc Intervent Radiol2010341374921069333
- LlovetJMDecaensTRaoulJ-LBoucherEBrivanib in patients with advanced hepatocellular carcinoma who were intolerant to sorafenib or for whom sorafenib failed: results from the randomized phase III BRISK-PS studyJ Clin Oncol201331283509351623980090
- LewisALDreherMRLocoregional drug delivery using image-guided intra-arterial drug eluting bead therapyJ Control Release2012161233835022285550
- HungHFChenTHProbabilistic cost-effectiveness analysis of the long term effect of universal hepatitis B vaccination: an experience from Taiwan with high hepatitis B virus infection and Hepatitis B e antigen positive prevalenceVaccine2009276770677619735755
- HongARobinDHermanJCost-effectiveness analysis of hepatitis B immunization in Vietnam: application of cost-effectiveness affordability curves in health care decision makingValue Health Regional20121714
- PoonRT-PFanS-THepatectomy for hepatocellular carcinoma: patient selection and postoperative outcomeLiver Transpl2004102 Suppl 1S39S4514762838
- GaillardMTranchartHDagherILaparoscopic liver resections for hepatocellular carcinoma: current role and limitationsWorld J Gastroenterol201420174892489924803800