
Abstract
Aim
To compare the long-term survival outcomes of radiofrequency ablation and liver resection for single very early/early stage hepatocellular carcinoma (HCC).
Methods
The Cochrane Library (Issue 3, 2015), Embase (1974 to March 15, 2015), PubMed (1950 to March 15, 2015), Web of Science (1900 to March 15, 2015), and Chinese Biomedical Literature Database (1978 to March 15, 2015) were searched to identify relevant trials. Only trials that compared radiofrequency ablation and liver resection for single very early stage (≤2 cm) or early stage (≤3 cm) HCC according to the Barcelona clinic liver cancer (BCLC) staging system were considered for inclusion in this review. The primary outcomes that we analyzed were the 3-year and 5-year overall survival (OS) rates, and the secondary outcomes that we analyzed were the 3-year and 5-year disease-free survival (DFS) rates. Review Manager 5.3 was used to perform a cumulative meta-analysis. Possible publication bias was examined using a funnel plot. A random-effects model was applied to summarize the various outcomes.
Results
Six studies involving 947 patients were identified that compared radiofrequency ablation (n=528) to liver resection (n=419) for single BCLC very early HCC. In these six studies, the rates of 3-year OS, 5-year OS, 3-year DFS, and 5-year DFS were significantly lower in the radiofrequency ablation group than in the liver resection group (risk ratio [RR] =0.90, 95% confidence interval [CI]: 0.83–0.98, P=0.01; RR =0.84, 95% CI: 0.75–0.95, P=0.004; RR =0.77, 95% CI: 0.60–0.98, P=0.04; and RR =0.70, 95% CI: 0.52–0.94, P=0.02, respectively). Ten studies involving 2,501 patients were identified that compared radiofrequency ablation (n=1,476) to liver resection (n=1,025) for single BCLC early HCC. In these ten studies, the rates of 3-year OS, 5-year OS, 3-year DFS, and 5-year DFS were also significantly lower in the radiofrequency ablation group than in the liver resection group (RR =0.93, 95% CI: 0.88–0.98, P=0.003; RR =0.84, 95% CI: 0.75–0.94, P=0.002; RR =0.72, 95% CI: 0.58–0.89, P=0.002; and RR =0.47, 95% CI: 0.33–0.67, P<0.0001, respectively).
Conclusion
The long-term survival outcomes for patients with single BCLC very early/early stage HCC appear to be superior after liver resection compared to radiofrequency ablation.
Introduction
Hepatocellular carcinoma (HCC) ranks sixth in terms of the most common neoplasms.Citation1–Citation3 The age-adjusted overall incidence of HCC was ~16 cases per 100,000 individuals in 2008.Citation1–Citation3 HCC is highly prevalent in Asia, and its incidence is increasing in Europe and in the US.Citation4 In recent decades, the development of diagnostic technology and the widespread screening of populations with a high risk of developing HCC have increased the detection of early stage HCC.Citation5–Citation7
Liver transplantation is regarded as the best curative approach for early stage HCC. However, only a small percentage of patients are offered this treatment due to high hospital costs and a shortage of liver donors.Citation5–Citation9 Liver resection is also a good surgical treatment for early stage HCC, and the 5-year survival rate of this procedure is >50%.Citation6–Citation8 However, some patients with HCC cannot undergo a liver resection due to either poor liver function or rejection. Many nonsurgical treatments have been proposed for these patients, such as radiofrequency ablation, microwave coagulation, and high-intensity focused ultrasound.Citation10–Citation14
The management of very early stage (Child-Pugh A, solitary ≤2 cm) and early stage (Child-Pugh A or B, solitary ≤3 cm) HCC, according to the Barcelona clinic liver cancer (BCLC) staging system, is controversial.Citation15 Various systematic reviews and meta-analyses have confirmed the short-term efficacy of radiofrequency ablation for BCLC early stage HCC.Citation16 The role of radiofrequency ablation in the management of BCLC very early stage HCC has not been systematically evaluated. The long-term survival outcome of patients with HCC is an important measure for the evaluation of various treatments.Citation5–Citation7 This systematic review compares the long-term survival outcomes of radiofrequency ablation versus liver resection for patients with single BCLC very early/early stage HCC.
Materials and methods
Study selection
The Cochrane Library (Issue 3, 2015), Embase (1974 to March 15, 2015), PubMed (1950 to March 15, 2015), Web of Science (1900 to March 15, 2015), and Chinese Biomedical Literature Database (1978 to March 15, 2015) were searched to identify trials that compared radiofrequency ablation with liver resection in the management of single BCLC very early/early stage HCC. The following keywords were used in these searches: catheter ablation, radiofrequency ablation, liver resection, hepatectomy, liver cancer, HCC, and liver neoplasm. The references of the relevant publications were also manually searched to identify any additional relevant clinical trials.
Criteria for inclusion and exclusion
The criteria for inclusion of the identified studies were as follows: 1) conformance to the BCLC staging classification: very early stage (Child-Pugh A, solitary ≤2 cm) or early stage (Child-Pugh A or B, solitary ≤3 cm); 2) comparison of the effects of radiofrequency ablation versus liver resection for single BCLC very early/early stage HCC, irrespective of etiology or the presence of liver cirrhosis or viral hepatitis; and 3) at least one outcome of interest reported.
The criteria for exclusion were as follows: 1) investigation of HCC nodules of >3 cm; 2) investigation of recurrent HCC; and 3) investigation of patients with cholangiocarcinomas or liver metastases.
Data extraction
The following data were extracted from each trial by two independent authors: 1) study design; 2) year of publication and authors; 3) number and characteristics of patients; and 4) outcome measures. The discrepancy between the two authors was resolved by discussion.
Outcomes
The primary outcomes measured in this review were the 3-year and 5-year overall survival (OS) rates. The secondary outcomes measured in this review were the 3-year and 5-year disease-free survival (DFS) rates.
Quality and publication bias assessment
The quality of each trial was evaluated using the GRADE system.Citation17 Funnel plots were applied to evaluate publication bias.Citation18 Both visual asymmetry and Egger’s linear regression test were used to examine the existence of publication bias.Citation19
Statistical analysis
Review Manager 5.3 (RevMan; Cochrane Collaboration, Oxford, UK) was used to perform a meta-analysis. Statistical heterogeneity among trials was determined by the chi-square test.Citation20 The risk ratio (RR) and 95% confidence interval (CI) were used to evaluate the treatment efficacy.Citation20 A result was regarded as statistically significant if the P-value was <0.05.Citation20 A random-effects model was used to summarize the various outcomes for conservative estimates. We conducted the meta-analysis and systematic review according to the Cochrane Handbook for Systematic Reviews of Interventions and Preferred Reporting Items for Systematic Reviews and Meta-Analyses.Citation21,Citation22
Results
Search results
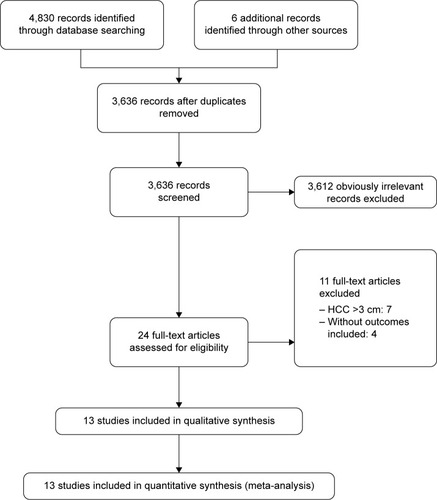
A total of 4,830 records were identified by electronic searches of the Cochrane Library (n=322), Embase (n=1,847), PubMed (n=1,581), Web of Science (n=820), and Chinese Biomedical Literature Database (n=260) and a manual search of the reference lists of the included trials (n=6). We excluded 1,200 duplicated records and 3,612 irrelevant records by screening titles and abstracts. Twenty-four full-text articles were retrieved for further assessment. We excluded eleven articles for the reasons listed in .
Figure 1 Flow diagram showing study selection process.
Description of studies
Thirteen studies published between 2008 and 2015 fulfilled the inclusion criteria, including two randomized controlled trials (RCTs) and eleven nonrandomized studies (NRS).Citation23–Citation35 Three studies compared radiofrequency ablation with liver resection for BCLC very early stage HCC,Citation25,Citation29,Citation30 seven studies compared radiofrequency ablation with liver resection for BCLC early stage HCC,Citation23,Citation24,Citation31–Citation35 and three studies compared radiofrequency ablation with liver resection for both BCLC very early stage and early stage HCC.Citation26–Citation28 A total of six studies including 947 patients (528 radiofrequency ablations and 419 liver resections) compared radiofrequency ablation with liver resection for BCLC very early stage HCC.Citation25–Citation30 Ten studies with a total of 2,501 patients (1,476 radiofrequency ablations and 1,025 liver resections) compared radiofrequency ablation with liver resection for BCLC early stage HCC.Citation23–Citation25,Citation29–Citation35 The characteristics and quality of the included trials are presented in and .
Table 1 Characteristics and quality of included studies for single BCLC very early stage HCC
Table 2 Characteristics and quality of included studies for single BCLC early stage HCC
Effects of interventions
Radiofrequency ablation versus liver resection for single BCLC very early stage HCC
The outcome measures data are presented in .
Table 3 The long-term outcomes of radiofrequency ablation versus liver resection for single BCLC very early stage HCC
Three-year OS rate: Five studiesCitation25–Citation27,Citation29,Citation30 reported this outcome. Patients in the radiofrequency ablation group had significantly lower 3-year OS rate than those in the liver resection group (RR =0.90, 95% CI: 0.83–0.98, P=0.01; heterogeneity: I Citation2=54%, P=0.07; ).
Figure 2 Forest plots of meta-analysis.
Abbreviations: CI, confidence interval; M–H, Mantel–Haenszel test.
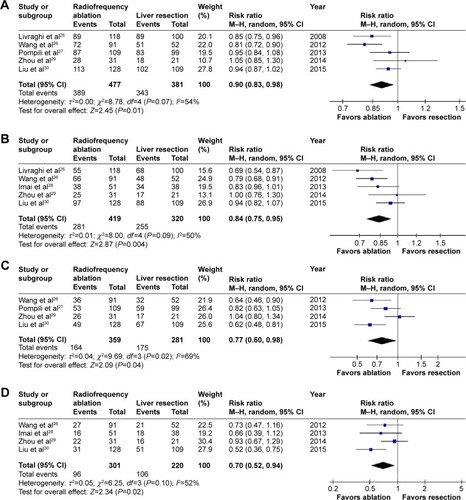
Five-year OS rate: Five studiesCitation25,Citation26,Citation28–Citation30 reported this outcome. Patients in the radiofrequency ablation group had significantly lower 5-year OS rate than those in the liver resection group (RR =0.84, 95% CI: 0.75–0.95, P=0.004; heterogeneity: I2=50%, P=0.09; ).
Three-year DFS rate: Four studiesCitation26,Citation27,Citation29,Citation30 reported this outcome. Patients in the radiofrequency ablation group had significantly lower 3-year DFS rate than those in the liver resection group (RR =0.77, 95% CI: 0.60–0.98, P=0.04; heterogeneity: I2=69%, P=0.02; ).
Five-year DFS rate: Four studiesCitation26,Citation28–Citation30 reported this outcome. Patients in the radiofrequency ablation group had significantly lower 5-year DFS rate than those in the liver resection group (RR =0.70, 95% CI: 0.52–0.94, P=0.02; heterogeneity: I2=52%, P=0.10; ).
Radiofrequency ablation versus liver resection for single BCLC early stage HCC
The outcome measures data are presented in .
Table 4 The long-term outcomes of radiofrequency ablation versus liver resection for single BCLC early stage HCC
Three-year OS rate: Ten studiesCitation23,Citation24,Citation26–Citation28,Citation31–Citation35 reported this outcome. Patients in the radiofrequency ablation group had significantly lower 3-year OS rate than those in the liver resection group (RR =0.93, 95% CI: 0.88–0.98, P=0.003; heterogeneity: I2=59%, P=0.008; ).
Figure 3 Forest plots of meta-analysis.
Abbreviations: CI, confidence interval; M–H, Mantel–Haenszel test; MELD, model for end-stage liver disease; TNM, tumor node metastasis; CLIP, cancer of the liver Italian program; JIS, Japan integrated staging.
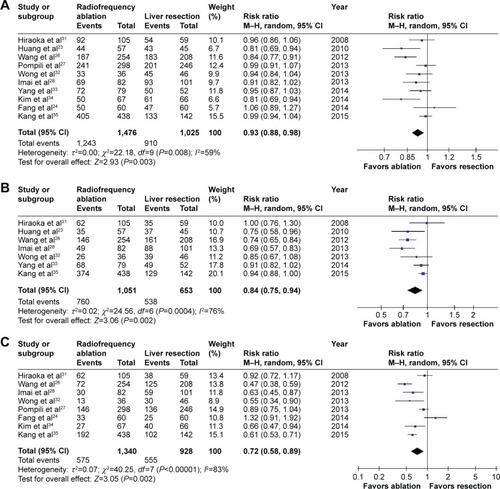
Five-year OS rate: Seven studiesCitation23,Citation26,Citation28,Citation31–Citation33,Citation35 reported this outcome. Patients in the radiofrequency ablation group had significantly lower 5-year OS rate than those in the liver resection group (RR =0.84, 95% CI: 0.75–0.94, P=0.002; heterogeneity: I2=76%, P=0.0004; ).
Three-year DFS rate: Eight studiesCitation24,Citation26–Citation28,Citation31,Citation32,Citation34,Citation35 reported this outcome. Patients in the radiofrequency ablation group had significantly lower 3-year DFS rate than those in the liver resection group (RR =0.72, 95% CI: 0.58–0.89, P=0.002; heterogeneity: I2=83%, P<0.00001; ).
Five-year DFS rate: Six studiesCitation26,Citation28,Citation31–Citation33,Citation35 reported this outcome. Patients in the radiofrequency ablation group had significantly lower 5-year DFS rate than those in the liver resection group (RR =0.47, 95% CI: 0.33–0.67, P<0.0001; heterogeneity: I2=77%, P=0.0005; ).
Quality of evidence and publication bias
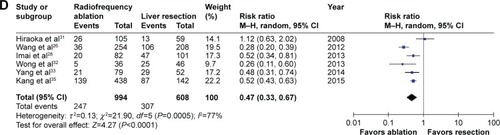
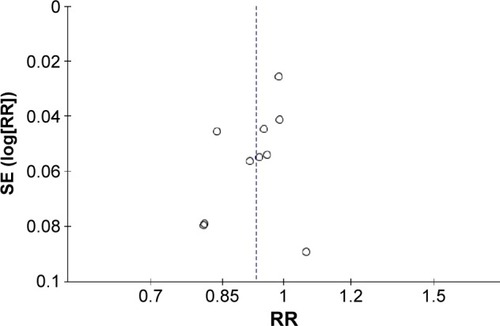
Only one study had a moderate quality,Citation23 and the quality of all other studies varied from low to very low ( and ). Thus, the current quality of evidence is considered very low. A funnel plot of the 3-year OS rate is presented in . Neither visual asymmetry nor Egger’s linear regression test (P=0.15) of the funnel plot indicated publication bias.
Figure 4 Funnel plot of the 3-year disease-free survival rate.
Abbreviations: SE, standard error; RR, risk ratio.
Discussion
This systematic review comprehensively collected the available long-term survival outcomes for radiotherapy versus liver resection for single BCLC very early/early stage HCC. The results indicated that liver resection led to significantly better long-term survival outcomes than radiofrequency ablation in the management of single BCLC very early/early stage HCC.
There are several HCC staging systems (eg, Child-Pugh, MELD, TNM, Okuda, CLIP, JIS, and BCLC),Citation5–Citation9 of which the BCLC staging system is the most commonly used.Citation15 The BCLC staging system is recommended by both the American Association for the Study of Liver Diseases (AASLD) and the European Association for the Study of the Liver (EASL).Citation6,Citation7 According to the current AASLD and EASL guidelines, liver transplantation, liver resection, and radiofrequency ablation are the recommended treatment choices for single BCLC very early/early stage HCC.Citation6,Citation7 There is little evidence available on the optimal management of single BCLC very early/early stage HCC.Citation25–Citation30 The AASLD and EASL guidelines are based on several retrospective cohort studies.Citation6,Citation7 The National Comprehensive Cancer Network and the Asian Pacific Association for the Study of the Liver do not mention the management of single BCLC very early stage HCC.Citation8,Citation9 Due to the shortcomings of liver transplantation, radiofrequency ablation and liver resection are commonly used to treat single BCLC very early/early stage HCC.Citation24–Citation35
Currently, the management of single BCLC very early/early stage HCC is controversial. With a 5-year OS rate of >50%, liver resection is generally considered the preferred first-line treatment.Citation6,Citation7 Liver resection offers the possibility of the curative excision of the entire tumor and microscopic tumor thrombi.Citation36 Alternatively, radiofrequency ablation is a minimally invasive technique that can be performed using a percutaneous or laparoscopic approach.Citation37 Many systematic reviews have demonstrated comparable short-term survival outcomes, lower morbidity, and shorter hospitalization in the radiofrequency ablation group when compared to the liver resection group.Citation16 However, the quality of published systematic reviews on this topic is poor due to the low quality of evidence and high clinical heterogeneity of the included studies.Citation16
Compared to previous systematic reviews, the major advantages of this systematic review are the use of the BCLC staging system and the evaluation of long-term survival outcomes. The findings of this review suggest that liver resection results in significantly better survival outcomes than radiofrequency ablation in the management of single BCLC very early/early stage HCC. The improvement in survival outcomes over time after liver resection may be associated with an improved understanding of liver anatomy, improved perioperative care, and increased surgical experience. Furthermore, radiofrequency ablation has some disadvantages. Radiofrequency ablation causes thermal injury and is therefore not suitable for the treatment of HCC located close to other organs (eg, gallbladder, colon, or kidney). In addition, the heat-sink effect of radiofrequency ablation complicates the complete ablation of HCC adjacent to large vessels.
Our review is subject to the following limitations. First, only two RCTs with sample sizes were included in the meta-analysis; the other studies were all NRS. Second, much of the data in this review were from NRS, and the Jadad scores of those NRS were very low; therefore, the quality of evidence is considered very low. Third, most of the included studies were conducted in Eastern countries, and thus, the results of this review are only applicable to Eastern populations.
Conclusion
In summary, this review encompasses all currently available evidence regarding the comparison of radiofrequency ablation with liver resection for single BCLC very early/early stage HCC. Based on this evidence, liver resection appears to be superior to radiofrequency ablation in terms of long-term survival outcomes. Future high-quality RCTs from Western countries are necessary to confirm our findings.
Author contributions
He Z-X and Zhang W designed the study. Xiang P and Gong J-P performed the literature research and collected the data. Cheng N-S analyzed the data. He Z-X and Zhang W wrote the paper. All authors contributed toward data analysis, drafting and critically revising the paper and agree to be accountable for all aspects of the work.
Acknowledgments
We would like to thank Jian Hu and Yao Cheng, who assisted with the development of the review.
Disclosure
The authors report no conflicts of interest in this work.
References
- FerlayJShinHRBrayFFormanDMathersCParkinDMEstimates of worldwide burden of cancer in 2008: GLOBOCAN 2008Int J Cancer2010127122893291721351269
- FornerALlovetJMBruixJHepatocellular carcinomaLancet201237998221245125522353262
- de LopeCRTremosiniSFornerAReigMBruixJManagement of HCCJ Hepatol201256suppl 1S75S8722300468
- El-SeragHBHepatocellular carcinomaN Engl J Med2011365121118112721992124
- BruixJShermanMPractice Guidelines Committee, American Association for the Study of Liver DiseasesManagement of hepatocellular carcinomaHepatology20054251208123616250051
- BruixJShermanMAmerican Association for the Study of Liver DiseasesManagement of hepatocellular carcinoma: an updateHepatology20115331020102221374666
- European Association for the Study of the LiverEuropean Organisation for Research and Treatment of CancerEASL-EORTC clinical practice guidelines: management of hepatocellular carcinomaJ Hepatol201256490894322424438
- OmataMLesmanaLATateishiRAsian Pacific Association for the Study of the Liver consensus recommendations on hepatocellular carcinomaHepatol Int20104243947420827404
- National Comprehensive Cancer Network [webpage on the Internet]NCCN Clinical Practice Guidelines in Oncology: Hepatobiliary Cancers. Version 2 [updated March 2015]The NCCN Guideline Available from: http://www.nccn.org/professionals/physician_gls/pdf/hepatobiliary.pdfAccessed January 12, 2016
- ChenMSLiJQZhengYA prospective randomized trial comparing percutaneous local ablative therapy and partial hepatectomy for small hepatocellular carcinomaAnn Surg2006243332132816495695
- FengKYanJLiXA randomized controlled trial of radiofrequency ablation and surgical resection in the treatment of small hepatocellular carcinomaJ Hepatol201257479480222634125
- SatoMWatanabeYUedaSMicrowave coagulation therapy for hepatocellular carcinomaGastroenterology19961105150715148613057
- SekiTNonakaTKubotaYMizunoTSameshimaYUltrasonically guided percutaneous ethanol injection therapy for hepatocellular carcinomaAm J Gastroenterol19898411140014072479262
- NgKKPoonRTChanSCHigh-intensity focused ultrasound for hepatocellular carcinoma: a single-center experienceAnn Surg2011253598198721394012
- LlovetJMBrúCBruixJPrognosis of hepatocellular carcinoma: the BCLC staging classificationSemin Liver Dis199919332933810518312
- WangYLuoQLiYDengSLiXWeiSA systematic assessment of the quality of systematic reviews/meta-analyses in radiofrequency ablation versus hepatic resection for small hepatocellular carcinomaJ Evid Based Med20147210312025155767
- GuyattGHOxmanADSchünemannHJTugwellPKnottnerusAGRADE guidelines: a new series of articles in the Journal of Clinical EpidemiologyJ Clin Epidemiol201164438038221185693
- SterneJACEggerMMoherDhomepage on the InternetChapter 10: addressing reporting biasesHigginsJPTGreenSCochrane Handbook for Systematic Reviews of Interventions. Version 5.1.0 [updated March 2011]The Cochrane Collaboration Available from: www.cochrane-handbook.orgAccessed January 12, 2016
- EggerMDavey SmithGSchneiderMMinderCBias in meta-analysis detected by a simple, graphical testBMJ199731571096296349310563
- DeeksJJHigginsJPTAltmanDGhomepage on the InternetChapter 9: analysing data and undertaking meta-analysesHigginsJPTGreenSCochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]The Cochrane Collaboration Available from: www.cochrane-handbook.orgAccessed January 12, 2016
- HigginsJPTGreenShomepage on the InternetCochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]The Cochrane Collaboration Available from: www.cochrane-handbook.orgAccessed January 12, 2016
- ShamseerLMoherDClarkeMPreferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: elaboration and explanationBMJ2015349g764725555855
- HuangJYanLChengZA randomized trial comparing radiofrequency ablation and surgical resection for HCC conforming to the Milan criteriaAnn Surg2010252690391221107100
- FangYChenWLiangXComparison of long-term effectiveness and complications of radiofrequency ablation with hepatectomy for small hepatocellular carcinomaJ Gastroenterol Hepatol201429119320024224779
- LivraghiTMeloniFDi StasiMSustained complete response and complications rates after radiofrequency ablation of very early hepatocellular carcinoma in cirrhosis: is resection still the treatment of choice?Hepatology2008471828918008357
- WangJHWangCCHungCHChenCLLuSNSurvival comparison between surgical resection and radiofrequency ablation for patients in BCLC very early/early stage hepatocellular carcinomaJ Hepatol201256241241821756858
- PompiliMSavianoAde MatthaeisNLong-term effectiveness of resection and radiofrequency ablation for single hepatocellular carcinoma ≤3 cm. Results of a multicenter Italian surveyJ Hepatol2013591899723523578
- ImaiKBeppuTChikamotoAComparison between hepatic resection and radiofrequency ablation as first-line treatment for solitary small-sized hepatocellular carcinoma of 3 cm or lessHepatol Res201343885386423281579
- ZhouZLeiJLiBLiver resection and radiofrequency ablation of very early hepatocellular carcinoma cases (single nodule <2 cm): a single-center studyEur J Gastroenterol Hepatol201426333934424150522
- LiuPHHsuCYHsiaCYSurgical resection versus radiofrequency ablation for single hepatocellular carcinoma ≤2 cm in a propensity score modelAnn Surg Epub2015313
- HiraokaAHoriikeNYamashitaYEfficacy of radiofrequency ablation therapy compared to surgical resection in 164 patients in Japan with single hepatocellular carcinoma smaller than 3 cm, along with report of complicationsHepatogastroenterology200855882171217419260499
- WongKMYehMLChuangSCSurvival comparison between surgical resection and percutaneous radiofrequency ablation for patients in Barcelona Clinic Liver Cancer early stage hepatocellular carcinomaIndian J Gastroenterol201332425325722932964
- YangHJLeeJHLeeDHSmall single-nodule hepatocellular carcinoma: comparison of transarterial chemoembolization, radiofrequency ablation, and hepatic resection by using inverse probability weightingRadiology2014271390991824520944
- KimJMKangTWKwonCHSingle hepatocellular carcinoma ≤3 cm in left lateral segment: liver resection or radiofrequency ablation?World J Gastroenterol201420144059406524744596
- KangTWKimJMRhimHSmall Hepatocellular carcinoma: radiofrequency ablation versus nonanatomic resection-propensity score analyses of long-term outcomesRadiology2015275390891925688888
- VivarelliMGuglielmiARuzzenenteASurgical resection versus percutaneous radiofrequency ablation in the treatment of hepatocellular carcinoma on cirrhotic liverAnn Surg2004240110210715213625
- MachiJUchidaSSumidaKUltrasound-guided radiofrequency thermal ablation of liver tumors: percutaneous, laparoscopic, and open surgical approachesJ Gastrointest Surg20015547748911985998