Abstract
From a retrospective evaluation of data on accidents and deaths during dental procedures, it has been shown that several patients who refused dental treatment died of asphyxia during dental procedures. We speculated that forcible maximum opening of the mouth by using a mouth prop triggers this asphyxia by affecting the upper airway. Therefore, we assessed the morphological changes of the upper airway following maximal opening of the mouth. In 13 healthy adult volunteers, the sagittal diameter of the upper airway on lateral cephalogram was measured between the two conditions; closed mouth and maximally open mouth. The dyspnea in each state was evaluated by a visual analog scale. In one subject, a computed tomograph (CT) was taken to assess the three-dimensional changes in the upper airway. A significant difference was detected in the mean sagittal diameter of the upper airway following use of the prop (closed mouth: 18.5 ± 3.8 mm, maximally open mouth: 10.4 ± 3.0 mm). All subjects indicated upper airway constriction and significant dyspnea when their mouth was maximally open. Although a CT scan indicated upper airway constriction when the mouth was maximally open, muscular compensation was admitted. Our results further indicate that the maximal opening of the mouth narrows the upper airway diameter and leads to dyspnea. The use of a prop for the patient who has communication problems or poor neuromuscular function can lead to asphyxia. When the prop is used for patient refusal in dentistry, the respiratory condition should be monitored strictly, and it should be kept in mind that the “sniffing position” is effective for avoiding upper airway constriction. Practitioners should therefore consider applying not only systematic desensitization, but also general anesthesia to the patient who refuses treatment, because the safety of general anesthesia has advanced, and general anesthesia may be safer than the use of a prop and restraints.
Introduction
The number of cases of accidental death or shock associated with dental procedures was investigated from 1950 to 2004 in Japan.Citation1 The deaths of 126 patients in 200 cases of accidents were reported. The main causes of death were acute cardiac failure (24%) and asphyxia (21%). Asphyxia most frequently occurred in healthy children or mentally-disabled patients undergoing a dental procedure with a mouth prop and body restrainer. It has been reported that percutaneous arterial oxygen saturation (SpO2) decreases significantly when patients are treated while having a mouth prop and body restrainer in place.Citation2 However, the underlying cause is of the increased risk of asphyxia in these situations is not clear. Therefore, it is necessary to clarify the cause of such accidents in order to prevent them from occurring in the future. We speculated that the maximum opening of the mouth by use of a mouth prop results in morphologic changes around the upper airway. To assess this possibility, the influence of maximal opening of the mouth using a mouth prop on airway morphology was investigated statistically using Wilcoxon t-test, Chi-square test, and Spearman rank-correlation analysis from cephalometric evaluations.
Subjects and methods
After approval of the ethical review board of Ohu university, 13 healthy adult volunteers (age: 33.0 ± 9.8 years, height: 170.8 ± 6.5 cm, body weight: 72.0 ± 6.5 kg) () who consented for this study participated as the subjects. Due to ethical concerns about using students or patients as subjects (because this study used X-rays), 13 staff members of our hospital participated voluntarily in this study. All subjects were kept under two conditions (closed mouth and the maximally open mouth as a result of the use of a mouth prop) in supine position for 30 seconds. Lateral cephalograms were taken under each condition. During each condition, the patient’s SpO2 (%) was measured, and their extent of dyspnea was evaluated by using a visual analog scale (VAS) (0 mm = no dyspnea, 100 mm = unbearable dyspnea). KXO-50F (Toshiba, Tokyo, Japan) was used as an X-ray generator, and the conditions of the X-rays used for this study are shown in . The universal mouth prop (Oyama Dental Industrials, Tokyo, Japan) was used to keep the mouth maximally open. The measurement points on the lateral cephalogram in this study are shown in . These measurement points were based on a study that evaluated the upper airway constriction after orthognathic surgery.Citation3 Under each condition, the three intervals in the sagittal diameter of the upper airway at the uvular tip (A), at the midpoint between the 2nd and 3rd cervical vertebra as a tongue base (B), and at the epiglottic vallecula (C), were traced and measured from the measurement points on the lateral cephalogram. Then the average of A, B, and C was assumed as the mean upper airway diameter. In addition, the inter-cusp interval from the upper to lower incisor was traced and measured in each condition. To minimize the technical errors, each dataset was adopted from the average value of tracing made by three different researchers who was calibrated previously.
Figure 1 Measurement points in the upper airway on the lateral cephalogram. Three intervals in the sagittal diameter of upper airway at; A) Uvular tip. B) Midpoint between the 2nd and 3rd cervical vertebra as a tongue base. C) Epiglottic vallecula.
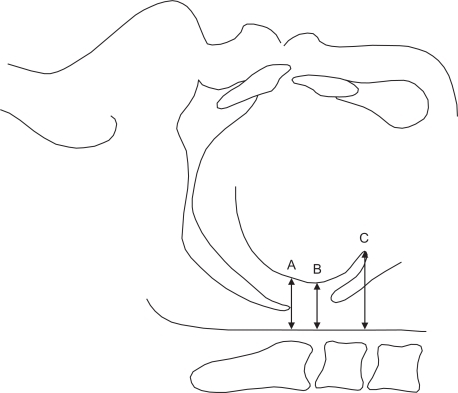
Table 1 Characteristics of the study subjects
Table 2 Conditions of lateral cephalometric radiography
Statistical analysis was performed by Wilcoxon t-test and 2 × 2 Chi-square test, and P < 0.05 was considered as statistically significant. In addition, Spearman rank-correlation analysis was applied to confirm the correlation between the constriction rate (%) in the mean upper airway diameter and the body mass index (BMI) [body weight (kg)/height (m)Citation2] as an obesity index, the inter-cusp interval (mm) from upper to lower incisor in maximum opening, or the VAS (mm) of dyspnea.
In one subject, head-neck X-ray computed tomography (CT) was used to assess the three-dimensional changes around the upper airway space in each condition. Only one subject was used for X-ray CT due to ethical considerations because the radiation exposure dose was larger than cephalogram. However, the morphological findings of the head-neck X-ray CT were interpreted by the department of oral anatomy.
Results
The results of the lateral cephalograms of the 13 subjects are shown in , and all results of measurements are shown in . The inter-cusp interval from the upper to lower incisor when the mouth was maximally open was 57.5 ± 8.5 mm. In the sagittal diameter of the upper airway of the 13 subjects, A was 16.1 ± 3.0 mm, B was 14.6 ± 3.8 mm, and C was 24.7 ± 5.7 mm in the closed mouth condition. However, A decreased to 7.4 ± 3.1 mm, B decreased to 7.7 ± 3.0 mm and C decreased to 16.3 ± 5.2 mm, when the mouth was in the maximally open position. These decreases were observed in all subjects (), and the decreases resulted in significant (P = 0.0016) decreases in the mean upper airway diameter (Closed mouth: 18.5 ± 3.8 mm, Maximally open mouth: 10.4 ± 3.0 mm). Mesurements A, B, and C were constricted by 54.1%, 47.3%, and 47.4%, respectively. There is little difference in the constriction rate between these three points ().
Figure 2 Individual cephalograms for each patient. All subjects indicated upper airway constriction by maximum opening of the mouth.
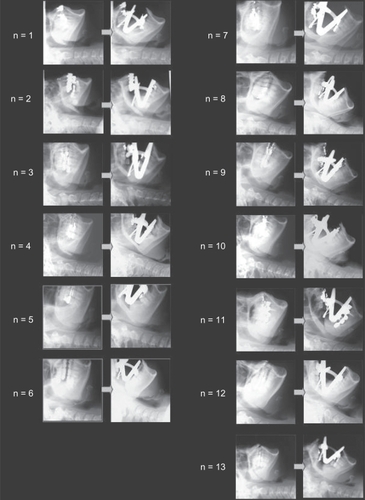
Figure 3 Decreases in the sagittal upper airway diameter induced by maximum opening of the mouth.
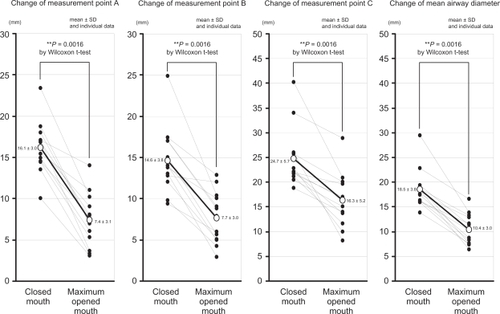
Figure 4 Changes in the upper airway formation induced by maximum opening of the mouth.
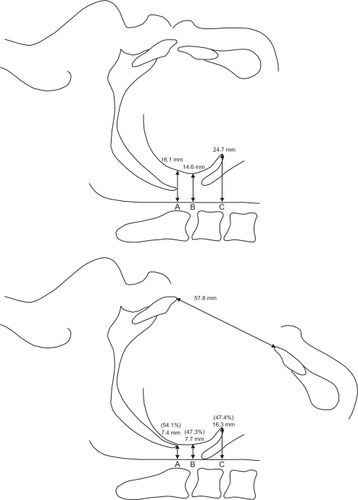
Table 3 A summary of the data generated during the present study
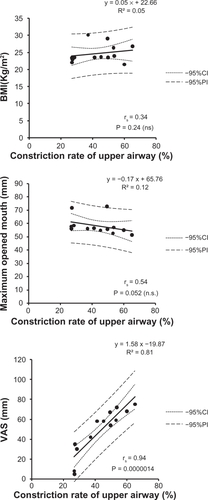
The VAS of the dyspnea was 0 ± 0 mm in the closed mouth position, but increased to 48.5 ± 22.2 mm when the subject had a maximally open mouth. In addition, the subjects’ sensation of dyspnea increased significantly (P = 0.0016). There were no significant differences in oxygenation, with the average SpO2 being 97.6 ± 0.9% in the closed mouth position, and 97.2 ± 0.8% when the subjects were in the maximally open mouth position (). Moreover, there was no significant correlation between the constriction rate in the mean upper airway diameter and the BMI as obesity index, or the inter-cusp interval from the upper to the lower incisors during maximum opening. However, a positive correlation (P = 0.0000014) was detected between the constriction rate in the mean upper airway diameter and the VAS of dyspnea ().
Figure 5 Changes of dyspnea and SpO2 induced by maximum opening of the mouth.
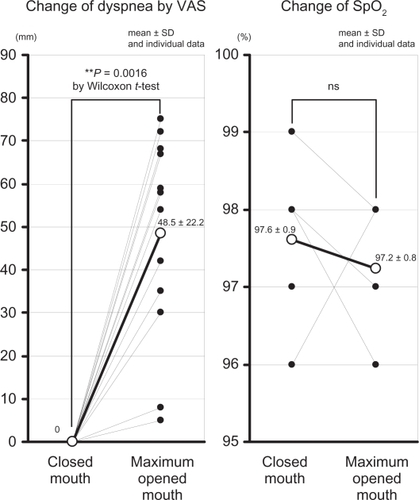
Figure 6 Correlation between the constriction rate (%) in the mean upper airway diameter and BMI (kg/m2), maximum opening of the mouth (mm), or VAS (mm).
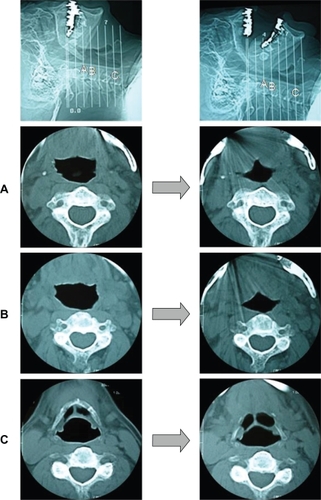
Although the head-neck X-ray CT also indicated that upper airway constriction was induced by maximum opening of the mouth, the finding of superior pharyngeal muscle constriction was observed to keep the upper airway diameter ().
Figure 7 Difference in the airway between the closed mouth and the maximally open mouth. This X-ray computed tomograph (CT) also indicated that the upper airway became narrower when the mouth is maximally open.
Discussion
It has previously been reported that the airway diameter decreases after mandibular setback surgery for mandibular prognathism,Citation3–Citation5 and the airway diameter increases after the use of mandibular traction or after patients wear a mandibular advancement device (MAD) as oral application for the treatment of sleep apnea syndrome.Citation6–Citation8 However, there have not been any previous reports about the influence of mouth position on upper airway shape and function. To investigate whether mouth position during dental procedures affects the upper airway, we used a mouth prop to enforce maximum mouth opening, then investigated the effects on the airway via cephalometric evaluation.
According to an investigation of the causes of death associated with dental procedures, asphyxia had occurred most often when the pediatric patients or mentally-disabled patients with strong treatment refusal were treated using a mouth prop and body restrainer. For such patients, we tend to use the mouth prop under maximum opening, because it is easier to remove the mouth prop. Therefore, to determine whether there was a link between the use of a mouth prop and airway constricture (possibly leading to asphyxia), the changes in the upper airway induced by maximum opening of the mouth by a mouth prop was investigated in this study.
From this result, we concluded that when the mouth is maximally open while the subject is maintained in the supine position, the mean upper airway diameter decreased to approximately half. We speculate that the tongue base, muscle, and soft tissue around the pharynx were physically pushed toward the posterior wall of the pharynx by the opened mandible, thus reducing the airway diameter. This suggests that keeping the mouth maximally open by mouth prop for dental procedures might lead to airway constriction.
Although we did not observe any significant change in the SpO2 in our subjects, we did observe significant dyspnea in all subjects. However, all of our study subjects were healthy adults, and they were kept in the maximally open mouth position for only 30 seconds.
The upper airway, which includes the nasal cavity, pharynx and larynx, has several functions (heating, humidifying and filtering air, as well as regulating swallowing and speech).Citation9 The diameter and compliance of the upper airway are adjusted according to the situation. When negative pressure is provided in the upper airway, the airway patency reflex works to dilate the airway by activating the surrounding muscles. Citation10 It has thus been suggested that the upper airway rarely constricts under the conscious state.Citation11 In fact, our finding of pharyngeal muscle contraction in the head-neck X-ray CT is regarded as occurring to compensate for the effects of the mouth prop and to help resist the upper airway constriction. It would appear that this compensatory response is mediated by the superior pharyngeal constrictor muscle and the pharyngeal plexus, which consists of the glossopharyngeus, vagus, and accessory nerves, which control the superior pharyngeal constrictor muscle. Therefore, it should be examined more whether the compensatory response is dysfunctional in pediatric patients, disabled patients, myopathic patients, and the patients who are taking psychoactive and/or sedative drugs that impair the neuromuscular function.
In this study, no significant correlation was found between the constriction rate in the mean upper airway diameter and the BMI, or the degree of maximum opening of the mouth. Therefore, the probability of upper airway constriction by mouth prop does not depend on the degree of obesity or the maximum opening mouth. It appears that the upper airway constriction depends primarily on the pharyngeal neuromuscular function. On the other hand, a correlation was detected between the constriction rate in the mean upper airway diameter and the VAS of dyspnea. This suggests that the feeling of dyspnea progresses as the constriction rate in the upper airway increases. This indicates that special attention should be paid to patient complaints of dyspnea in order to prevent further hypoxia.Citation12,Citation13
In this study, the data were taken under the supine position, because most of usual dental procedures are administered with patients in the supine position. Compared to the seated position, in the supine position, the diaphragm is displaced toward the head by abdominal pressure. Then, a decrease in thoracic compliance results in a decrease of functional residual capacity.Citation14 Additional use of body restraints further impairs respiratory function, and SpO2 has been demonstrated to decrease significantly when pediatric patients were treated under body restraint.Citation2 In this study, keeping the mouth at its maximum open position using a mouth prop for 30 seconds induced dyspnea even without use of body restraints. Therefore, it should be confirmed whether the combined use of a mouth prop and body restraints amplifies the risk or not.
Pediatric subjects were excluded from this study for ethical considerations. However, anatomically, children have relatively large tongues and short necks in comparison with adults.Citation15 And, the primitive pharyngeal reflex is inhibited by microgenia, sleep apnea syndrome, taking psychoactive or sedative drugs, and hypertrophy of the adenoids, tonsils, and tongue.Citation16 Furthermore, it has been reported that the arterial oxygen saturation decreased significantly by bite block for dental procedure in the handicapped patients.Citation13
Systematic desensitization therapy is often successful, making the use of a mouth prop and/or body restraints unnecessary.Citation17,Citation18 However, when the mouth prop must be used during a dental procedure, the patient’s respiratory condition should be carefully monitored. In particular, a pulse-oxymeter is effective for detecting hypoxia at an early stage.Citation2,Citation19,Citation20 To ensure better dilation of the upper airway in the supine position, the so-called “sniffing position” which keeps elevation in both the forehead and chin using a thick pillow is effective.Citation21 Such a position is recommended when patients must be treated using a mouth prop.
Recently, intubated general anesthesia has become safer than before, as dramatic progress in drugs, monitoring, equipment, and technology has been made. From the 1950s to the 1990s, the mortality caused by general anesthesia plummeted from 1/2,860 to 1/400,000 respectively.Citation22,Citation23 The mortality caused by local anesthesia is approximately 7 times higher than that caused by general anesthesia.Citation24
Conclusions
The influence of maximum opening of the mouth using a mouth prop on the upper airway was investigated from lateral cephalograms of patients in control (closed mouth) and prop-induced open-mouthed positions. We made several observations:
The mean upper airway diameter decreased to approximately half following maximum opening of the mouth using a mouth prop, and subjects reported feeling significant dyspnea.
The maximum opening of the mouth for 30 seconds did not change the SpO2, however, the subjects reported feeling significant dyspnea.
In the head-neck X-ray CT, upper airway muscle contraction was observed to serve as a compensatory mechanisms to maintain the proper upper airway diameter. This muscle contraction is likely controlled by the superior pharyngeal constrictor muscle and pharyngeal plexus.
Disclosures
The authors report no conflicts of interest in this work.
References
- ItoHOgawaSSeinoHAn analysis of 200 cases of severe shock and cardiopulmonary arrest that were related with dental treatment or oral surgeryJapanese Journal of Reanimatology20052428287
- ShimamuraKHaruyamaHAizawaNFluctuations in the pulse rate and SpO2 during dental treatment of the children under restraintJapanese Journal of Pediatric Dentistry2005435613618
- TerakadoKShiinaYNaruseTEffects of surgical orthodontic treatment on oral cavity, tongue, and pharyngeal airway (Part 1: Changes caused by mandibular setback surgery)Shika Gakuh1997972181191
- DegerliyurtKUkeiKHashibaYThe effect of mandibular setback or two-jaws surgery on pharyngeal airway among different gendersInt J Oral Maxillofac Sur2009386647652
- HwangSChungCJChoiYJChanges of hyoid, tongue and pharyngeal airway after mandibular setback surgery by intraoral vertical ramus osteotomyAngle Orthod201080230230819905855
- PradelWLauerGDingerJMandibuler traction – an alternative treatment in infants with Pierre Robin sequence –J Oral Maxillofac Surg200967102232223719761918
- LeeCHKimJWLeeHJAn investigation of upper airway changes associated with mandibular advancement device using sleep videofluoroscopy in patients with obstructive sleep apneaArch Otolaryngol Head Neck Surg2009135991091419770424
- DoffMHHoekemaAPruimGJEffects of a mandibular advancement device on the upper airway morphology: a cephalometric analysisJ Oral Rehabil20093633033719382298
- PierceRJWorsnopCJUpper airway function and dysfunction in respirationClin Exp Pharmacol Physiol200926111010027063
- ThachBTNeuromuscular control of upper airway patencyClin Perinatol19921947737881464190
- IsonoSNishinoTAirway protective reflexes and mechanisms of airway maintenanceKokyu To Junkan1998465469475
- HagbergCGeorgiRKrierCComplications of managing the airwayBest Pract Res Clin Anaesthesiol200519464165916408539
- OgasawaraTWatanabeTHosakaKHypoxemia due to inserting a bite block in severely handicapped patientsSpec Care Dentist199515270738619167
- FroeseABBryanACEffects of anesthesia and paralysis on diaphragmatic mechanics in manAnesthesiology19744132422554604401
- DickisonAEThe normal and abnormal pediatric upper airway. Recognition and management of obstructionClin Chest Med1987845835963322644
- NishinoTTagaitoYIsonoSCough and other reflexs on irritation of airway mucosa in manPulm Pharmacol199695–62852929232665
- GolabekTSystematic desensitization: a treatment for odontophobiaTIC19824111456128804
- CarlssonSGLindeABerggrenUReduction of dental fear: psychophysiological correlatesCommunity Dent Oral Epidemiol19861452532572878764
- FukayamaHYagielaJAMonitoring of vital signs during dental careInt Dent J200656210210816620039
- YamazakiSKawaaiHSasakiSAvailability of a remote online hemodynamic monitoring system during treatment in a private dental office for medically high-risk patientsTher Clin Risk Manage200844721726
- BurwellDRJonesJGThe airway and anesthesia. PathophysiologyAnaesthesia199651109439548984870
- BeecherHKToddDPA study of deaths associated with anesthesia and surgery based on a study of 599, 548 anesthesias in ten institutions, 1948–1952 inclusiveAnn Surg1954140123413159140
- VoelkerRMedical News and Perspectives; Anesthesia-related risk have plummetedJAMA199527364454467837345
- OlssonGLHallěnBCardiac arrest during anesthesia. A computeraided study in 250, 543 anaestheticsActa Anaesthesiol Scand19883286536643213390