Abstract
Cutaneous lupus erythematosus (CLE) encompasses a variety of lesions that may be refractory to systemic or topical agents. Discoid lupus erythematosus (DLE) and subacute cutaneous lupus erythematosus (SCLE) are the most common lesions in clinical practice. The topical calcineurin inhibitors, tacrolimus and pimecrolimus, have been used to treat resistant cutaneous lupus since 2002 and inhibit the proliferation and activation of T-cells and suppress immune-mediated cutaneous inflammation. This article reviews the mechanism of action, efficacy, adverse effects, and the recent concern about their possible carcinogenic effect. Although the total number of patients is small and there is only one relevant randomized controlled study, the data are encouraging. Many patients, previously resistant to systemic agents or topical steroids, improved after four weeks of treatment. DLE and SCLE lesions were less responsive, reflecting the chronicity of the lesions, although more than 50% of patients still showed improvement. Topical calcineurin inhibitors may be a safe and effective alternative to topical steroids for CLE although the only approved indication is for atopic dermatitis.
Introduction
Cutaneous lesions are a common and often disfiguring manifestation of autoimmune connective tissue diseases. Cutaneous lupus erythematosus (CLE) is a broad term which includes a variety of lesions which may appear without the systemic manifestations of systemic lupus erythematosus (SLE). Pure CLE is usually not life-threatening, but frequently contributes to significant clinical and psychological morbidity, especially when lesions develop on the face. By contrast, cutaneous lesions commonly develop in patients with SLE.
The most widely used classifications of CLE are those of GillianCitation1 and Kuhn.Citation2 The clinical manifestations of CLE are divided into acute (ACLE), subacute (SCLE), chronic (CCLE) and intermittent (ICLE) forms. ACLE typically presents in the context of the systemic disease as a photosensitive, maculopapular rash over sun-exposed areas or as a localized malar rash. SCLE appears as annular polycyclic or psoriasiform lesions in sun-exposed areas without scarring. CCLE is further divided into discoid lupus erythematosus (DLE, scarring erythematosus macules or plaques with pigment changes localized to the upper part of the body, arms and face), lupus profundus (LEP, panniculitis) and chilblain lupus (CHLE, pernio-like skin lesions). ICLE presents as lupus tumidus (urticarial lesions in sun-exposed areas).
Administration of systemic agents such as corticosteroids, hydroxychloroquine, mepacrine, methotrexate, mycophenolate mofetil, cyclophosphamide and/or azathioprine for the underlying systemic disease leads in many cases to remission of the cutaneous lesions. The use of topical treatments such as steroids, and barrier sun protection in conjunction with systemic treatment usually provides additional benefit. Nevertheless, many patients suffer from resistant cutaneous lesions despite therapy. On the other hand, cutaneous lesions may be the only manifestation of disease such as SCLE and DLE, making it difficult to justify systemic agents, because of their side effects. A variety of systemic (dapsone, thalidomide, retinoids, IV immunoglobulins) and topical agents (intralesional steroids, retinoids) as well as laser therapy, phototherapy, photopheresis, and cryotherapy have been used for resistant cutaneous lesions.Citation3 There is a need therefore for alternative therapies.
The literature was systematically reviewed for all the articles involving topical calcineurin inhibitors by using the Medline search database. Search terms included tacrolimus, pimecrolimus, cutaneous lupus erythematosus and topical calcineurin inhibitors. All the publications involving clinical trials (prospective, retrospective, or case-controlled studies) in lupus patients were included in this review as well as many publications relevant to the pathophysiology of pimecrolimus and tacrolimus and experience in other diseases.
Topical calcineurin inhibitors
Tacrolimus (FK506) is a macrolide immunomodulator which was isolated in 1984 from the fungus Streptomyces Tsukubaensis, which was found near Tsukuba mountain in Ibraki, Japan. The word tacrolimus is derived from Tsukuba, macrolide and immunosuppression. Pimecrolimus (SDZ ASM 981) is a synthetic product of ascomycin which is a product of Streptomyces hygroscopicus.
These agents bind to the cytoplasmic protein macrophilin-12, forming a complex that blocks the serine-threonine phosphatase calcineurin.Citation4 Calcineurin is a protein that activates, by dephosphorylation, the cytoplasmic subunit of nuclear factor of activated T-cells (NF-AT), which enters the nucleus and forms a complex with the nuclear subunit promoting the production of many cytokines such as interleukin-2 (IL-2), IL-3, IL-4, IL-5, interferon-γ, and tumor necrosis factor-α (TNF-α).Citation5–Citation7
Calcineurin inhibitors inhibit T-cell activation. They also inhibit mast cell degranulation and release of inflammatory mediators such as histamine, tryptase, and cytokines.Citation8 Pimecrolimus, but not tacrolimus, has no effects on dendritic cells and does not affect maturation of Langerhans cells in infants.Citation9 Neither agent affects endothelial cells or fibroblasts, so do not cause skin atrophy or telangiectasis. Their propensity to pass through the skin is lower than that of steroids, avoiding any systemic side effects from their absorption.Citation10 Pimecrolimus is 20 times more lipophilic than tacrolimus, with a higher affinity for skin and lower permeation even in severely inflamed skin.Citation11 On the other hand, tacrolimus has a stronger immunosuppressant capacity than pimecrolimus.Citation12
Treatment indications
In 1989, oral tacrolimus was first used in preventing graft rejection after solid organ transplantation (liver, kidneys, lungs).Citation13 In November 2000, tacrolimus ointment was approved by the US FDA Dermatologic Committee for the treatment of atopic dermatitis in children and adults and this remains the only approved indication.Citation14,Citation15
Since then, topical calcineurin inhibitors have been used off-label in many resistant cutaneous lesions in other diseases such as psoriasis,Citation16 localized scleroderma,Citation17 chronic actinic dermatitis,Citation18 pyoderma gangrenosum,Citation19 Behçet’s disease,Citation20 lichen planus,Citation21 rheumatoid ulcers,Citation22 steroid-induced rosacea,Citation23 vitiligo,Citation24 dermatomyositis,Citation25 hand eczema,Citation26 asteatotic eczema,Citation27 autoimmune bullous dermatosis,Citation28 seborrheic dermatitis,Citation29 allergic contact dermatitis,Citation30 and graft-versus-host disease.Citation31 The commercially available forms are Protopic® or Prograf® 0.03% and 0.1% ointment (tacrolimus) and Elidel® 1% cream (pimecrolimus).
Safety
The topical calcineurin inhibitors appear to be safe for use in chronic inflammatory skin diseases.Citation32 Side effects are usually mild, and include irritation, pruritus, burning sensation, or increased erythema. These adverse reactions are usually transient and subside with continuation oftreatment. Low penetration of the inflamed skin reduces the risks of any systemic side effects.
These agents seem to be a safer alternative to potent topical steroids, which usually are effective, cheap and fast-acting but their chronic use results in skin atrophy, teleangiectasiae, dermatitis, and pustules. Calcineurin inhibitors can be used safely over sensitive areas like the face, mucous membranes, and genitaliaCitation33 where the skin is thin, or during infancy and early childhood. They are not systemically absorbed even when large areas of skin are affected. They are highly effective even as monotherapy and they result in rapid and sustained improvement. There have been no reports of any statistically significant incidence of local infections (bacterial, viral, or fungal) during their use,Citation34 although there may be a slightly increased risk for local Varicella zoster virus, Herpes simplex virus, eczema herpeticum, impetigo, and molluscum contagiosum.Citation35 Clearly however, they should not be used in obviously infected skin lesions.
Although generally safe, in March 2005 the Food and Drug Administration (FDA) informed health care professionals and patients about a potential risk of cancer from the use of tacrolimus which was based on animal studies and case reports.Citation36 The first report was that of a squamous cell cancer of the penis after use of tacrolimus.Citation37 Since then, more than 19 cases of cancer were reported in association with tacrolimus use. Half of them involved lymphomas and the rest were skin tumors at the site of application (squamous cell carcinoma, sarcoma, melanoma).Citation38,Citation39 In animal models it was found that tacrolimus reduces the CD4/CD8 ratio in lymph nodes and that its concentration in the draining lymph nodes was as high as after oral use.Citation40 Tacrolimus was also found to inhibit apoptosis in nonlymphoid cells and to affect proteins that participate in the cancer signaling pathways (Erk activation resulting in cell proliferation and p53 inhibition resulting in reduced apoptosis).Citation41
On the other hand, many reviews and publications failed to connect topical calcineurin inhibitors with an increased risk of cancerCitation42 in adults and children.Citation43,Citation44 There was no evidence of systemic immunosuppression among infants treated intermittently with 1% pimecrolimus for up to two years, and all demonstrated a normal immune response to vaccinations without increased systemic or skin infections.Citation45,Citation46 The analysis of data from clinical studies with more than five million patients treated with pimecrolimus cream since December 2001 failed to show any increased risk of cancer.Citation47
A recent study showed that topical calcineurin inhibitors were associated with a slightly increased risk of lymphoma compared with the general population, but the same risk was also noticed in users of topical steroids, suggesting that all topical treatments may increase lymphoma risk.Citation48 Another study found an association between lymphoma (especially of the skin) and use of topical steroids but not with calcineurin inhibitors and that the risk depended on steroid potency and duration of exposure.Citation49
Topical calcineurin inhibitors and cutaneous lupus erythematosus
Many case reports and a few prospective trials have been published since 2002 when lupus skin lesions were first treated with topical calcineurin inhibitors (see ). The first report was by Yoshimasu et alCitation50 who used tacrolimus ointment 0.1% once a day for four weeks in three SLE and four DLE patients with facial rash, and four further patients with dermatomyositis. Improvement was noticed in all SLE patients but only in one with discoid lesions. Walker et alCitation51 reported two patients with discoid lupus who showed significant improvement with tacrolimus ointment 0.03% in 0.05% clobetasol propionate cream while ZabawskiCitation52 reported one patient with discoid lupus treated successfully with pimecrolimus cream 1%.
Table 1 Topical calcineurin inhibitors in cutaneous lupus erythematosus
Tacrolimus was also effective in the treatment of one patient with lupus tumidus.Citation53 Böhm et alCitation54 successfully treated three patients (one with SLE and two with SCLE) with tacrolimus and Kanekura et alCitation55 had the same results in three patients with SLE and facial skin lesions.
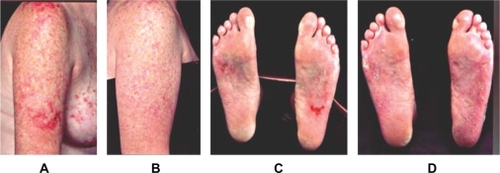
In 2004, Drüke et alCitation56 and de la Rosa Carrillo et alCitation57 treated one patient with SCLE and one patient with discoid lupus with tacrolimus. Lampropoulos et alCitation58 published an open-label study of 11 patients comprising five with discoid lupus, four with SCLE and two with SLE. Tacrolimus ointment was applied twice daily for six weeks with a good response in both patients with SLE, two of four patients with SCLE (see ) and two patients with discoid lupus, while one patient with DLE had a partial response. A couple of months later an open uncontrolled clinical trial was published by Kreuter et alCitation59 who used pimecrolimus 1% cream in 11 patients with different forms of lupus erythematosus comprising four with DLE, three with SLE, two with SCLE, and two with lupus tumidus. Pimecrolimus cream was applied twice daily for three weeks under semi-occlusive conditions (overnight occlusion with hydrocolloid dressings) with significant improvement in all patients (57% improvement on a clinical severity score).
Figure 1 Two patients with SCLE lesions on upper right limb and SCLE lesions on soles, respectively, before (A, C) and after (B, D) treatment with tacrolimus ointment. Copyright © 2004. Reprinted with permission from Lampropoulos CE, Sangle S, Harrison P, Hughes GR, D’Cruz DP. Topical tacrolimus therapy of resistant cutaneous lesions in lupus erythematosus: A possible alternative. Rheumatology (Oxford). 2004;43:1383–1385.
In 2005, Tlacuilo-Parra et alCitation60 reported 10 patients with discoid lupus treated successfully with pimecrolimus for eight weeks. The overall improvement on a clinical severity score was 52%. Three patients showed a reduction of more than 70%, four patients 50%–70%, and three patients 30%–50%. All patients had a skin biopsy before and after treatment which showed a significant reduction in the density of the dermal lymphocytic infiltrate. A quality of life index was also used (Skindex-29),Citation61 with a mean improvement of 46%. In the same year Heffernan et alCitation62 reported five patients with discoid lupus erythematosus who showed improvement of their rash after 12 weeks of tacrolimus ointment. Meller et alCitation63 described one patient with SCLE and Cassis et alCitation64 a further patient with SCLE attributable to monocyclic antidepressant therapy who were treated successfully with tacrolimus.
Three publications concerning the use of calcineurin inhibitors and cutaneous lupus erythematosus were published in 2006. Sugano et alCitation65 successfully treated four patients with discoid lupus using tacrolimus ointment for 4–8 weeks while von Pelchrzim et alCitation66 had 50% success (one of two patients with SLE and one of two patients with DLE). Nagao et alCitation67 reported a patient with cutaneous lupus overlapping with lichen planus who was treated effectively with tacrolimus.
Tzung et alCitation68 published the first randomized, double-blind, controlled study in 2007. Eighteen patients with facial rashes participated, of whom 13 had SLE, four had DLE and one had SCLE. Tacrolimus ointment was applied twice daily on one side of the face and clobetasol propionate 0.05% ointment on the other side. A partial response was noticed in all patients without significant differences between the two creams, but 11 patients developed teleangiectasiae on the clobetasol side during the first three weeks, indicating better tolerability and safety of tacrolimus compared with topical steroids.
A retrospective study was published in 2009 by Madan et al.Citation69 A specially formulated preparation of tacrolimus 0.3% in clobetasol propionate 0.05% ointment was compared with either 0.1% tacrolimus or clobetasol propionate 0.05% as monotherapy in 18 patients with cutaneous lupus erythematosus, which seemed to be more effective. This is in accordance with experimental evidence that combination of corticosteroids with calcineurin inhibitors can achieve superior therapeutic efficacy and stronger inhibition of T-cell proliferation compared with monotherapy.Citation70
Discussion
Cutaneous lesions in lupus erythematosus may prove very resistant to classical systemic and topical agents. These lesions usually appear in visible areas resulting in significant psychological effects. Therapy is often unsatisfactory because of recalcitrant disease or serious side effects from corticosteroids.
Over the last two decades, tacrolimus and the newer calcineurin inhibitor pimecrolimus have emerged as effective immunosuppressive and anti-inflammatory agents. The experience in atopic dermatitis showed that they are very effective and safe, especially in children and for facial lesions where only weak topical steroids can be used. These ointments are expensive, but a cost-effectiveness analysis showed that in the long term the cost is similar for tacrolimus and high-potency corticosteroids.Citation71 They are not systemically absorbed, even when large areas of skin are affected, and their adverse reactions usually subside with continuation of treatment. Their use must be combined with sun protection because most of the cutaneous lesions in lupus are photosensitive.
The usual effective treatment is application of the cream twice daily for at least four weeks, during which time improvement of symptoms is expected. Skin lesions in SLE can improve significantly in most patients, but this is less likely in patients with discoid lupus or SCLE. The response to treatment is partial in these particular types of cutaneous lupus and prolonged therapy may be needed, reflecting the chronicity and unresponsiveness of these lesions.Citation72 Nevertheless, 50%–60% of patients report a partial or good response, an encouraging result if we consider that these cutaneous lesions are usually resistant to systemic or other topical agents. Recent studies have shown that combination of calcineurin inhibitors with steroids is more effective than monotherapy, suggesting that this should be considered for very resistant lesions.
Most of the publications are case reports with small numbers of patients. The only randomized, double-blind study showed calcineurin inhibitors and steroids had similar efficacy but without serious side effects, reflecting the necessity for more prospective trials with larger numbers of patients. The warning issued by the FDA regarding the possible low risk of cancer should be considered by the prescribing physician, especially as these agents remain off-label for use in lupus. A further consideration is the increased risk of lymphoma that is associated with having SLE,Citation73 and so treatment should be limited to short periods of time. In conclusion, the data in the literature taken together suggest that topical calcineurin inhibitors can be considered to be a relatively safe and attractive alternative treatment for resistant cutaneous lesions in lupus erythematosus.
Disclosures
The authors report no conflict of interest in this work.
References
- GillianJNSontheimerRDDistinctive cutaneous subsets in the spectrum of lupus erythematosusJ Am Acad Dermatol198144714757229150
- KuhnARuzickaTClassification of cutaneous lupus erythematosusKuhnALehmannPRuzickaTCutaneous lupus erythematosusHeidelberg, GermanySpringer2005
- TingWWSontheimerRDLocal therapy for cutaneous and systemic lupus erythematosus: Practical and theoretical considerationsLupus20011017118411315348
- SárdyMRuzickaTKuhnATopical calcineurin inhibitors in cutaneous lupus erythematosusArch Dermatol Res2009301939818797893
- HomeyBAssmannTVohrHWTopical FK506 suppresses cytokine and costimulatory molecule expression in epidermal and local draining lymph node cells during primary skin immune responsesJ Immunol1998160533153409605132
- GisondiPEllisCNGirolomoniGPimecrolimus in dermatology: Atopic dermatitis and beyondInt J Clin Pract20055996997416033622
- MarslandAMGriffithsCEThe macrolide immunosuppressants in dermatology: Mechanisms of actionEur J Dermatol20021261862212459545
- GrassbergerMSteinhoffMSchneiderDLugerTAPimecrolimus – an anti-inflammatory drug targeting the skinExp Dermatol20041372173015560755
- MeindlSVaculikCMeingassnerJGDifferential effects of corticosteroids and pimecrolimus on the developing skin immune system in humans and miceJ Invest Dermatol20091292184219219295616
- BillichAAschauerHAszodiAStuetzAPercutaneous absorption of drugs used in atopic eczema: Pimecrolimus permeates less through skin than corticosteroids and tacrolimusInt J Pharm2004269293514698574
- WeissHMFresneauMMoeniusTStuetzABillichABinding of pimecrolimus and tacrolimus to skin and plasma proteins: Implications for systemic exposure after topical applicationDrug Metab Dispos2008361812181818524871
- WolffKStuetzAPimecrolimus for the treatment of inflammatory skin diseaseExpert Opin Pharmacother2004564365515013932
- StarzlTETodoSFungJFK506 for liver, kidney and pancreas transplantationLancet19892100010042478846
- US FDA Advisory Committee recommends approval for Tacrolimus ointmentSkin Ther Lett200065
- NakagawaHEtohTIshibashiYTacrolimus ointment for atopic dermatitisLancet19943448837522297
- YamamotoTNishiokaKTopical tacrolimus: An effective therapy for facial psoriasisEur J Dermatol20031347147314693492
- MancusoGBerdondiniRMTopical tacrolimus in the treatment of localized sclerodermaEur J Dermatol20031359059214721783
- EvansAVPalmerRAHawkJKErythrodermic chronic actinic dermatitis responding only to topical tacrolimusPhotodermatol Photoimmunol Photomed200420596114738535
- PeteringHKiehlPBreuerCKappAWerfelTPyoderma gangrenosum: Successful topical therapy with tacrolimus (FK506)Hautarzt200152475011220239
- SakaneTMochizukiMInubaGMasudaKA phase II study of FK506 (tacrolimus) on refractory uveitis associated with Behçet’s disease and allied conditionsRyumachi1995358028138594659
- VolzTCaroliULüdtkeHPimecrolimus cream 1% in erosive oral lichen planus – a prospective randomized double-blind vehicle-controlled studyBr J Dermatol200815993694118647310
- SchuppeHRichter-HintzDStierleHEHomeyBRuzickaTLehmannPTopical tacrolimus for recalcitrant leg ulcer in rheumatoid arthritisRheumatology20003910510610662882
- GoldmanDTacrolimus ointment for the treatment of steroid-induced rosacea: A preliminary reportJ Am Acad Dermatol20014499599811369912
- GawrodgerDJOrmerodADShawLGuideline for the diagnosis and management of vitiligoBr J Dermatol20081591051107619036036
- LampropoulosCED’CruzDPTopical tacrolimus treatment in a patient with dermatomyositisAnn Rheum Dis2005641376137716100347
- RobertsonLNew and existing therapeutic options for hand eczemaSkin Therapy Lett2009141519585057
- WollinaUThe role of topical calcineurin inhibitors for skin diseases other than atopic dermatitisAm J Clin Dermatol2007815717317492844
- LugerTPaulCPotential new indications of topical calcineurin inhibitorsDermatology2007215Suppl 1S45S54
- CookBAWarshawEMRole of topical calcineurin inhibitors in the treatment of seborrheic dermatitis: A review of pathophysiology, safety and efficacyAm J Clin Dermatol20091010311819222250
- RallisEKorfitisCGregoriouSRigopoulosDAssigning new roles to topical tacrolimusExpert Opin Investig Drugs20071612671276
- WolffDSteinerBHildebrandtGEdingerMHollerEPharmaceutical and cellular strategies in prophylaxis and treatment of graft-versus-host diseaseCurr Pharm Res20091519741997
- WooDKJamesWDTopical tacrolimus: A review of its uses in dermatologyDermatitis20051662115996345
- DraelosZDUse of topical corticosteroids and topical calcineurin inhibitors for the treatment of atopic dermatitis in thin and sensitive skin areasCurr Med Res Opin20082498599418284804
- GuptaAKChowMPimecrolimus: A reviewJ Eur Acad Dermatol Venereol20031749350312941081
- LangleyRGLugerTACorkMJSchneiderDPaulCAn update on the safety and tolerability of pimecrolimus cream 1%: Evidence from clinical trials and post-marketing surveillanceDermatology2007215Suppl 1S27S44
- US Food and Drug AdministrationFDA Public Health Advisory: Elidel (pimecrolimus) cream and Protopic (tacrolimus) ointmentRockville, MDUS Food and Drug Administration2005
- LangelandTEnghVTopical use of tacrolimus and squamous cell carcinoma on the penisBr J Dermatol200515218318515656830
- BeckerJCHoubenRVelterCSBröckerEBThe carcinogenic potential of tacrolimus ointment beyond immune suppression: A hypothesis creating case reportBMC Cancer20066716405733
- WooltortonEEczema drugs tacrolimus (Protopic) and pimecrolimus (Elidel): Cancer concernsCMAJ20051721179118015817641
- NiwaYNasrIAre we starting to induce skin cancer in order to avoid topical steroidsJ Eur Acad Dermatol Venereol20051938738915857478
- Gomez-LechonMJSerraltaADonatoMTThe immunosuppressant drug FK506 prevents Fas-induced apoptosis in human hepatocytesBiochem Pharmacol2004682427243315548389
- RustinMHThe safety of tacrolimus ointment for the treatment of atopic dermatitis: A reviewBr J Dermatol200715786187317854353
- PaulCCorkMRossiABPappKABarbierNde ProstYSafety and tolerability of 1% pimecrolimus cream among infants: Experience with 1133 patients treated up to 2 yearsPediatrics2006117118128
- RingJBarkerJBehrendtHReview of the potential photococarcinogenicity of topical calcineurin inhibitors: Position statement of the European Dermatology ForumJ Eur Acad Dermatol Venereol20051966367116268869
- PappKAWerfelTFölster-HolstRLong-term control of atopic dermatitis with pimecrolimus cream 1% in infants and young children: A two-year studyJ Am Acad Dermatol20055224024615692468
- PappKABreuerKMeurerMLong-term treatment of atopic dermatitis with pimecrolimus cream 1% in infants does not interfere with the development of protective antibodies after vaccinationJ Am Acad Dermatol20055224725315692469
- US Food and Drug AdministrationNovartis Elidel (pimecrolimus) cream 1% briefing documentRockville, MDUS Food and Drug Administration2005
- SchneeweissSDohertyMZhuSTopical treatments with pimecrolimus, tacrolimus and medium-to high-potency corticosteroids and risk of lymphomaDermatology200921972119293564
- ArellanoFMAranaAWentworthCEFernández-VidaurreCSchliengerRGCondeELymphoma among patients with atopic dermatitis and/or treated with topical immunosuppressants in the United KingdomJ Allergy Clin Immunol20091231111111619361841
- YoshimasuTOhtaniTSakamotoTOshimaAFurukawaFTopical FK506 (tacrolimus) therapy for facial erythematous lesions of cutaneous lupus erythematosus and dermatomyositisEur J Dermatol200212505211809595
- WalkerSLKirbyBChalmersRJThe effect of topical tacrolimus on severe recalcitrant chronic discoid lupus erythematosusBr J Dermatol200214740540612174136
- ZabawskiETreatment of cutaneous lupus with ElidelDermatol Online J200282512546779
- BacmanDTanbajewaAMegahedMRuzickaTKuhnATopical treatment with tacrolimus in lupus erythematosus tumidusHautarzt20035497797914513247
- BöhmMGaubitzMLugerTAMetzeDBousmannGTopical tacrolimus as a therapeutic adjunct in patients with cutaneous lupus erythematosus. A report of three casesDermatology200320738138514657631
- KanekuraTYoshiiNTerasakiKMiyoshiHKanzakiTEfficacy of topical tacrolimus for treating the malar rash of systemic lupus erythematosusBr J Dermatol200314835335612588393
- DrükeAGambichlerTAltmeyerPDreitagMKreuterA0.1% Tacrolimus ointment in a patient with subacute cutaneous lupus erythematosusJ Dermatolog Treat200415636414754655
- De la Rosa CarrilloDChristensenOBTreatment of chronic discoid lupus erythematosus with topical tacrolimusActa Derm Venereol20048423323415202845
- LampropoulosCESangleSHarrisonPHughesGRD’CruzDPTopical tacrolimus therapy of resistant cutaneous lesions in lupus erythematosus: A possible alternativeRheumatology (Oxford)2004431383138515266063
- KreuterAGambichlerTBreuckmannFPimecrolimus 1% cream for cutaneous lupus erythematosusJ Am Acad Dermatol20045140741015337984
- Tlacuilo-ParraAGuevara-GutiérrezEGutiérrez-MurilloFPimecrolimus 1% cream for the treatment of discoid lupus erythematosusRheumatology (Oxford)2005441564156816159951
- Jones-CaballeroMPẽnasPFGarcia-DiezABadiaXChrenMMThe Spanish version of skindex-29Int J Dermatol20003990791211168659
- HeffernanMPNelsonMMSmithDIChungJH1% tacrolimus ointment in the treatment of discoid lupus erythematosusArch Dermatol20051411170117116172325
- MellerSBruch-GerharzDRuzickaTHomeyBTopical treatment of subacute-cutaneous lupus erythematosus with tacrolimusHautarzt20055636836915750673
- CassisTBCallenJPBupropion-induced subacute cutaneous lupus erythematosusAustralas J Dermatol20054626626916197429
- SuganoMShintaniYKobayashiKSakakiburaNIsomuraIMoritaASuccessful treatment with topical tacrolimus in four cases of discoid lupus erythematosusJ Dermatol20063388789117169097
- Von PelchrzimRSchmookTFriedrichMWormMEfficacy of topical tacrolimus in the treatment of various cutaneous manifestations of lupus erythematosusInt J Dermatol200645848516426386
- NagaoKChenKRA case of lupus erythematosus/lichen planus overlap syndromeJ Dermatol20063318719016620224
- TzungTYLiuYSChangHWTacrolimus vs clobetasol propionate in the treatment of facial cutaneous lupus erythematosus: A randomized, double-blind, bilateral comparison studyBr J Dermatol200715619119217199600
- MadanVAugustPJChalmersRJEfficacy of topical tacrolimus 0.3% in clobetasol propionate 0.05% ointment in therapy-resistant cutaneous lupus erythematosus: A cohort studyClin Exp Dermatol20093470570819077095
- WiniskiAWangSSchwendingerBStuetzAInhibition of T-cell activation in vitro in human peripheral blood mononuclear cell by pimecrolimus and glucocorticosteroids and combinations thereofExp Dermatol20071669970417620098
- EllisCNDrakeLAPrendergastMMCost-effectiveness analysis of tacrolimus ointment versus high-potency topical corticosteroids in adults with moderate to severe atopic dermatitisJ Am Acad Dermatol20034855356312664019
- WollinaUHanselGThe use of topical calcineurin inhibitors in lupus erythematosus: An overviewJ Eur Acad Dermatol Venereol2008221618005117
- BernatskySRamsey-GoldmanRIsenbergDHodgkin’s lymphoma in systemic lupus erythematosusRheumatology (Oxford)20074683083217255135