Abstract
Dupuytren’s disease (DD) is a common disease of the hand and is characterized by thickening of the palmar fascia and formation of tight collagenous disease cords. At present, the disease is incurable and the molecular pathophysiology of DD is unknown. Surgery remains the most commonly used treatment for DD, but this requires extensive postoperative therapy and is associated with high rates of recurrence. Over the past decades, more indepth exploration of the molecular basis of DD has raised the hopes of developing new treatment modalities. This paper reviews the clinical presentation and molecular pathophysiology of this disease, as well as current and emerging treatment. It also explores the implications of new findings in the laboratory for future treatment.
Introduction
Dupuytren’s disease (DD), also known as Dupuytren’s contracture, is a common pathologic condition of the hand. The hallmark of the disease is the formation of occasionally painful nodules in the palm of the hand and of tendon-like cords that lead to flexion deformities of the affected fingers. This pathology can lead to pain upon gripping, but most patients seek medical attention when contractures result in limitations in dexterity. Patients complain about not being able to put their gloves on or that they cannot grasp objects well. Often there are social concerns, such as embarrassment when shaking hands.Citation1 Treatment is mostly offered to patients who desire correction of flexion deformities or to those who are bothered by the painful nodules. However, in the absence of a full understanding of the molecular pathology, treatment is currently aimed at eliminating the contracted pathologic disease tissue, without correcting the underlying pathophysiology. Because of this, recurrences are common and current work is aimed at a deeper understanding of the disease process. This review summarizes the clinical presentation of the disease, reviews current and emerging treatment, and touches on new data regarding the molecular pathophysiology of DD. It also explores the implications of these advancements for future work.
Clinical presentation and anatomy
DD often occurs bilaterally, but typically affects one hand more severely than the other. The earliest signs of DD involve changes in the skin, such as the presence of pits in the skin of the palm or changes to the skin on the dorsum of the hand with the presence of knuckle pads or Garrod nodes.Citation2,Citation3
The ring and small fingers are most often involved, although the other fingers and thumb may also be affected.Citation3 The disease is thought to progress from a palmar nodule into a longitudinal cord. These cords seem to follow normal palmar fascial structures which in their healthy states are designated as “bands”. As the cord matures, it contracts and becomes more fibrotic, taking on a more distinct tendon-like appearance and resulting in flexion contractures of the digits.Citation4
In the palm, the most common cord is the precentral cord, which arises from the precentral band of the palmar fascia and typically results in a flexion deformity of the metacarpophalangeal (MCP) joint. Other cords in the palm include the vertical and natatory cords (arising respectively from the vertical bands of Legueu and Juvara and the natatory ligaments), although these are less common than the precentral cord.Citation5
In the fingers, the most common cords are the central, lateral, and spiral cord.Citation4 The central cord is an extension of the precentral cord that forms in the midline of the fingers and attaches to the flexor tendon sheath. This cord can cause deformities in the MCP joint and proximal interphalangeal (PIP) joint. The lateral cord is a continuation of the bifurcated precentral cord and is considered the pathologic state of the lateral digital sheath. Unlike the central cord, it attaches to the skin or to the tendon sheath near Grayson’s ligament. This cord usually results in deformities of the PIP joint, but can also affect the DIP joint. The spiral cord is also an extension of the precentral cord that starts off deep to the neurovascular bundle and distal to the MCP joint. In the digit, the cord advances lateral to the neurovascular bundle to involve the lateral digital sheath and then superficial to the neurovascular bundle to involve Grayson’s ligament. In doing so, the cord wraps itself around the neurovascular bundle, which causes the superficial, proximal, and central displacement of the neurovascular bundle when finger contractures are produced. This displacement puts the neurovascular bundle at risk of damage during surgery.Citation3
Prevalence and risk factors
DD is considered an inherited dominant condition with variable penetrance, affecting males more often than females.Citation6 Typically, disease onset is in the fourth or fifth decade of life in males, while the disease tends to develop later in life for females.Citation6,Citation7 Although primary DD is more prevalent in males, the probability of recurrence is approximately equal between the sexes after surgery.Citation6 DD has been traced to a population of Germanic and Celtic tribes who migrated across Northern Europe to Scandinavia and to the British Isles. From there, the disease was brought by emigrants to the New World, including Australia and North America. DD is less common in other parts of the world, such as Southern Europe, South America, and Asia,Citation8 although in certain populations within this area, specifically Japan and Taiwan, higher prevalence rates have been reported.Citation9 In Iceland, the prevalence of DD can be as high as 40% in males over 70 years.Citation10
In 1963, Hueston first described a “Dupuytren’s diathesis”, a term which describes factors that would strongly predict disease severity and disease recurrence after treatment.Citation11 Patients of Northern European descent, those who present at a younger age of onset, and those who have a positive family history of DD have an increased probability of developing the condition, as well as having a more aggressive disease progression. Similarly, patients who have bilateral hand involvement and ectopic lesions (such as knuckle pads, plantar fibromatosis [Lederhosen disease], or penile fibromatosis [Peyronie’s disease]) are more likely to have aggressive disease progression and an increased risk of recurrence. The severity of a patient’s disease presentation continues to be an important factor in the management of this disease, and recently the statistical risk for disease recurrence based on these diathesis factors has been calculated.Citation12
In addition to genetic factors, a number of comorbidities and socioenvironmental factors play a role in this condition. Studies have suggested that DD clusters in patients with certain underlying health conditions, such as diabetes mellitusCitation13,Citation14 and epilepsy.Citation15 Lifestyle risk factors that have been associated with DD include smoking and high alcohol consumption.Citation16–Citation18 Other factors, such as manual labor,Citation19 hand or wrist trauma,Citation20 and a history of repetitive hand vibrationsCitation21 have also been associated with the disease. The contributions of these factors remain controversial, however, and other studies have been unable to identify any correlation.Citation22
Treatment
While the current research focus is on the identification of potential molecular therapies for DD management, the most widely practiced intervention is still surgical resection of the disease cords.Citation23,Citation24 Surgical treatment is based on the simple premise that the disease cords prevent the fingers from extending and that excision of the diseased tissue leads to “freeing-up” of the joints and return of range of motion. Review of the surgical results, however, often shows incomplete return of range of motion and considerable rates of recurrence. Nonetheless, because surgery still forms the mainstay of treatment, we will include surgical treatment of DD in this review.
Surgery for Dupuytren’s disease
Surgical intervention is typically considered when the contracture significantly affects hand function. This is usually where the MCP and/or PIP flexion contracture exceeds 30°, and many surgeons use a simple assessment such as the “table-top test” to determine appropriateness for surgery. This “table-top test” dictates that once a hand can no longer be placed flat on the table, consideration should be given to surgical release.Citation25
There are a number of surgical variations available to address finger contractures in DD. Multiple options to expose the fascia have been described, including longitudinal midline incisions closed with Z-plasties, Bruner-type zigzag incisions, and multiple transverse incisions.Citation26 Most operations for the correction of DD contractures involve some form of palmar fasciectomy, and fasciectomy can be divided into local, regional, and radical fasciectomy. Of the three, local fasciectomy is the least invasive, and involves resection of segments of the disease cord, thereby releasing finger contracture. Because residual disease tissue remains in the hand following the local fasciectomy procedure, the chance of recurrence is high.Citation3 A more extensive approach is regional or partial fasciectomy, a technique involving the removal of as much of the affected fascia as possible.Citation27 Radical or total fasciectomy is a more invasive procedure, involving the excision of the palmar and digital fascia. This technique is associated with an increased risk of surgical complications and does not have lower recurrence rates when compared with partial fasciectomy.Citation28
For less advanced disease involving only palmar cords, the use of fasciotomy has been advocated. Fasciotomy is a technique used to release contractures by dividing the disease cord without the excision of the diseased tissue.Citation29 As the diseased tissue is not removed, the risk of disease recurrence is relatively high.Citation30 The closed procedure, often referred to as needle fasciotomy or needle aponeurotomy, involves the placement of a needle adjacent to the cord, and “slicing” or “piercing” of the disease cord with the sharp beveled edge of the needle to release the contracture.Citation31,Citation32 While this procedure is minimally invasive in nature, most surgeons still believe that it should be used with caution because it puts the flexor tendons and nerves at risk of being severed during surgery.Citation32 It is currently believed to have a role only in the management of mild to moderate MCP contractures. An alternative approach to the closed fasciotomy is the open fasciotomy procedure. This approach involves creating an incision in the palm of the hand, allowing visualization of the disease cord. The cord can then be severed, thereby releasing the contracture. This procedure is less invasive than closed fasciotomy, but has the advantage of reducing the risk of damage to the nerves in the hand because it allows for direct visualization of the disease cord.
For management of aggressive or recurrent disease, dermofasciectomy has been recommended. This extensive technique involves excision of the diseased fascia en bloc with the overlying skin, and subsequent use of skin grafts to close the skin.Citation33,Citation34 Compared with fasciectomy alone, dermofasciectomy offers a lower chance of disease recurrence. Because of this, despite longer postoperative rehabilitation, this technique is sometimes recommended for younger patients or for those with Dupuytren’s diathesis and a history of aggressive disease recurrence.
To improve long-term results, splinting is prescribed as a postoperative physical therapeutic modality.Citation35 While the effectiveness of splinting without surgery is dubious, most surgeons would still advocate it as an adjunct to surgery to maximize finger extension and function.Citation3,Citation36 After the acute wound healing stage has passed, most surgeons would also continue night splinting to maintain extension in the remodeling phase of wound healing.
Recurrence rates following surgery remain high and, recurrence rates increase with longer follow-up periods.Citation3 Complications of surgery include digital nerve injury, skin flap loss, wound healing problems, infection, hematoma, and postoperative stiffness. Occasionally patients develop a regional complex pain syndrome or exhibit prolonged postoperative inflammation requiring prolonged hand therapy.Citation37 In the end, some patients with a history of multiple recurrences or surgery-associated complications opt for amputation of the affected finger(s) rather than undergo further surgery.
Biologic treatment approaches
Because of the high rates of disease recurrence and inherent risks of surgical intervention, a shift in focus of recent research in DD has been towards identifying potential molecular targets for nonsurgical alternative therapies.
The most straightforward nonsurgical treatment of DD has been to accomplish the same as surgical removal of the disease cords but by enzymatic digestion of the cord. This approach has been tried for a number of decades with variable success. In 1971, Hueston reported that enzymatic fasciotomy can achieve similar outcomes to surgical fasciotomy, and suggested that it may be an appropriate alternative for selected patients.Citation38 Enzymatic fasciotomy is the injection of a cocktail of proteolytic and anti-inflammatory enzymes, specifically trypsin, hyaluronidase, and lidocaine, to disrupt the collagenous nature of the disease environment.Citation38 This injection is followed by physical manipulation to straighten the digits, breaking the disease cord and releasing the contracture. Because the disease cords are primarily composed of Type I and Type III collagen,Citation14,Citation39,Citation40 more recently, investigators have been starting to use a mixture of clostridium-derived collagenases, Clostridium hystolyticum Type I and Type II, which specifically target the NH3 and COOH terminals and internal peptide residues, respectively, in collagen fibers. These enzymes belong to the matrixin subgroup of the metalloproteinases, requiring Zn2+ and Ca2+ for activity. A number of studies have now provided data that collagenase injection into disease cords improves finger contractures and improves joint mobility in advanced disease.Citation14,Citation41–Citation44 Marketed as Xiaflex® (Auxilium Pharmaceuticals, Inc.), these injections can be considered as a nonoperative alternative to surgery. However, like surgery, this approach targets a result of the disease process, ie, excess collagen deposition, rather than the cause of the disease, which is thought to be hyperproliferative, contractile, and collagen-producing disease cells within the palmar fascia. Finally, because collagenase does not act specifically on the disease cord structure, the long-term safety of injecting this enzyme into other structures of the hand that also contain collagen, such as tendons, ligaments, and neurovascular bundles, should also be considered. The current evidence suggests that collagenase C. hystolyticum specifically targets fibrillar collagens such as Type I and Type III (but not Type IV) collagen, the primary collagen constituent of blood vessels. The long-term rate of recurrence, as well as safety of collagenase treatment of DD, is currently being evaluated in several Phase III trials.
The use of corticosteroid injections has been advocated as a treatment for early disease or for painful nodules. Intralesional injection of a corticosteroid directly into palmar nodules can result in softening and reduction of pain.Citation45 This correlates with molecular studies which show that steroids can function as an antifibrotic agent, reducing cell proliferation, while inducing apoptosis or programmed cell death.Citation46,Citation47 The potential side effects of steroid use are skin depigmentation and dermal atrophy from collagen degradation.Citation48,Citation49 Rarely, flexor tendon ruptures have been described.
Another biologic agent to address the observed cellular proliferation and inflammation in DD is δ-interferon.Citation50 Molecular studies on cells derived from DD patients show that δ-interferon can reduce cell proliferation, collagen production, and the expression of α-smooth muscle actin, a predominant isoform of actin found in contractile cells called myofibroblasts.Citation51,Citation52 While there have been a number of studies showing the potential benefits of δ-interferon in the treatment of DD, most of these studies have been conducted in vitro and whether these translates into clinical improvements is largely unknown. One small pilot study reported a decrease in the size of the lesion(s) associated with DD and that, at least in hypertrophic scar tissue, treatment with δ-interferon resulted in a decrease of α-smooth muscle actin expression and myofibroblast formation by immunohistochemistry.Citation50 This study was not specific to DD, and included only four patients with DD in the hand, while the remainder presented with hypertrophic scars or plantar fibromatosis. Larger studies are required to determine whether the therapeutic benefits of δ-interferon in cell cultures in laboratories can translate into improvements in hand function in the clinical setting.
DD has been viewed as an exaggerated wound healing responseCitation53 and, since the wound healing response includes Type I and Type III collagen deposition, knowledge from this process has been applied to the study of DD. In this light, other biologic agents that may offer therapeutic benefits in DD, including agents that may affect the ratio between a group of specific collagenases found in wound healing, ie, matrix metalloproteinases (MMPs) and their inhibitors (tissue inhibitors of metalloproteinases, TIMPs). MMPs and their inhibitors regulate extracellular matrix (ECM) turnover and function. Studies have found correlations between MMP expression and DD progression and recurrence,Citation54 and the MMP:TIMP ratio in DD fascia has been found to be abnormal.Citation55 Treatment of cancer patients with a synthetic TIMP has been shown to result in DD,Citation56 but other studies have shown that the use of ilomastat, a broad MMP inhibitor, leads to decreased mechanical tension generated by disease nodule and cord cells.Citation57 The proposed pharmacologic manipulation of the MMP:TIMP ratio and how this affects DDCitation54,Citation57–Citation59 will require further study to determine the clinical applicability and potential effectiveness of such treatments on improving hand and joint function.
Recent molecular studies
There is a general consensus that a greater understanding of the molecular mechanism of DD will lead to the creation of more specific and effective treatment alternatives. The study of the cellular behavior of cells in diseased fascia, however, is hampered by the fact that the treatment of choice in the early stages of DD is observation. The genetic and molecular study of early-stage DD cells is thus not always feasible. The main tool to discern cellular abnormalities has been to evaluate the abnormal biologic behavior of DD cells obtained from surgical resection and to compare this with cells obtained from phenotypically normal palmar fascia or cells obtained from carpal tunnel release patients. This type of study using differential gene expression analysis, combined with molecular and functional studies of disease tissues and cells, has helped identify a number of putative abnormal mediators in DD. Several dysregulated genes in DD encode secreted ECM proteins,Citation60–Citation64 and these may play a role in disease progression or recurrence. While structural components of the ECM, such as collagens, laminin, fibronectin, and elastin are altered in DD,Citation65,Citation66 recent work has also identified proteases, including A Disintegrin and Metalloprotease (ADAM)-12, proteoglycans (notably PRG4), and “matricellular” components, including tenascin C and periostin, as well as specific members of the MMP family (MMP-2 and MMP-9) mentioned earlier, as being abnormally regulated.Citation61,Citation62,Citation64 We and others have demonstrated that periostin is abundant in the ECM of DD nodules and cordsCitation60,Citation61,Citation64,Citation67 and we have also shown that periostin induces the proliferation and apoptosis of phenotypically normal fibroblasts derived from the palmar fascia adjacent to the DD cord, and myofibroblast differentiation of DD cells.Citation64 ECM molecules, such as periostin, which initiate a differential response in DD cells and adjacent fibroblasts, may have different roles in DD progression and recurrence. The functional characterization of these ECM proteins, therefore, may identify novel therapeutic targets to prevent DD recurrence.Citation68,Citation69
Along these lines, our laboratory has chosen to focus on dysregulation of the Wnt-β-catenin pathway, because we first identified elevated total and tyrosine-phosphorylated β-catenin levels in DD.Citation70 In our studies, we also found that the ECM plays a role in expression of the disease phenotype.Citation65,Citation66 The current hypothesis that we are working on is that DD cells modify their extracellular environment by secreting (or depleting) molecules that promote (or inhibit) myofibroblast differentiation in their collagenous ECM. Perhaps, when this modified ECM is left behind after surgical resection of the DD cord, there is the potential for these secreted factors to activate fibroblasts resident in the adjacent fascia to differentiate into myofibroblasts and promote disease recurrence.Citation71 Currently, we are testing potential mediators of myofibroblast development by incorporating them into collagen substrates to mimic the in vivo environment and, in this way, we have demonstrated that a collagen-enriched substrate modifies transforming growth factor-beta (TGF-β) signaling in DD cells.Citation72 We have also demonstrated that periostin, a TGF-β-induced and abundant component of the DD ECM, promotes myofibroblast differentiation of primary DD cells and have uncovered evidence of insulin-like growth factor (IGF) and IGF binding protein (IGFBP) changes in DD (see ). The latter interactions are intriguing from several perspectives. Firstly, ADAM-12, which is abundant in the DD tissue, has been shown to cleave a subset of IGFBPs and release IGFs to stimulate cell growth and proliferationCitation73,Citation74. In parallel, another IGFBP that is not a target of ADAM-12, IGFBP-6, has been shown to be specifically and potently downregulated in desmoid tumorsCitation75 and DD (our unpublished data) by TGF-β signaling. Finally, IGF and IGFBP levels are consistently dysregulated in diabetes,Citation76–Citation79 a metabolic condition frequently linked to DD predisposition.Citation6,Citation80,Citation81 How all these findings will translate into clinical treatment is as yet unclear, but delineation of the abnormal molecular pathophysiology of DD is necessary to design rational molecular treatment methods. Moreover, while DD is a difficult clinical problem in its own right, DD is associated with other fibroproliferative diseases, including Peyronie’s disease,Citation60,Citation82 Lederhose disease,Citation83,Citation84 frozen shoulder syndrome (adhesive capsulitis),Citation85–Citation87 and desmoid tumor (aggressive polyfibromatosis).Citation88 Research into the molecular pathogenesis of these diseases has shown that many of these disorders are characterized by dysregulated cellular proliferation and myofibroblast differentiation. Therefore, identification of molecules that induce myofibroblast development in DD may have broad consequences for the treatment of these other diseases and further research into the molecular pathogenesis of DD remains important.
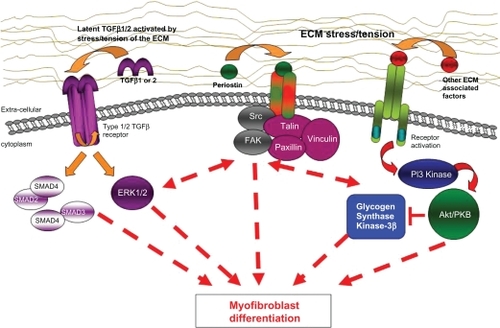
Figure 1 Proposed scheme in which TGF-β signalling, ECM stress tension, and/or other ECM-associated factors may lead to dysregulation of myofibroblast differentiation. These pathways seem to be involved in the molecular pathogenesis of Dupuytren’s disease and targeted interruption of abnormal signalling components may lead to future treatment approaches.
Disclosure
The authors report no conflict of interest in this work.
References
- PrattALByrneGThe lived experience of Dupuytren’s disease of the handJ Clin Nurs200918121793180219220604
- RayanGMDupuytren disease: Anatomy, pathology, presentation, and treatmentJ Bone Joint Surg Am200789118919817256226
- ShawRBJrChongAKZhangAHentzVRChangJDupuytren’s disease: history, diagnosis, and treatmentPlast Reconstr Surg2007120344e54e
- McFarlaneRMPatterns of the diseased fascia in the fingers in Dupuytren’s contracture. Displacement of the neurovascular bundlePlast Reconstr Surg197454131444832466
- WatsonHKPaulHJrPathologic anatomyHand Clin1991746616681769988
- RossDCEpidemiology of Dupuytren’s diseaseHand Clin19991515362vi10050242
- ChildsSGDupuytren’s diseaseOrthop Nurs2005242160163 quiz 164–16515902016
- McFarlaneRMOn the origin and spread of Dupuytren’s diseaseJ Hand Surg Am200227338539012015711
- EgawaTSenruiHHorikiAEgawaMEpidemiologoy of the Oriental patientDupuytren’s disease Biology and TreatmentEdinburgh, UKChurchill Livingstone1990239245
- GudmundssonKGArngrimssonRSigfussonNBjornssonAJonssonTEpidemiology of Dupuytren’s disease: clinical, serological, and social assessment. The Reykjavik StudyJ Clin Epidemiol200053329129610760640
- HuestonJThe Dupuytren’s diathesisDupuytren’s ContractureEdinburgh, UKChurchill Livingstone19635163
- HindochaSStanleyJKWatsonSBayatADupuytren’s diathesis revisited: Evaluation of prognostic indicators for risk of disease recurrenceJ Hand Surg [Am]2006311016261634
- CaglieroEApruzzeseWPerlmutterGSNathanDMMusculoskeletal disorders of the hand and shoulder in patients with diabetes mellitusAm J Med2002112648749011959060
- ArkkilaPEKoskinenPJKantolaIMRonnemaaTSeppanenEViikariJSDupuytren’s disease in type I diabetic subjects: investigation of biochemical markers of type III and I collagenClin Exp Rheumatol200018221521910812494
- ArafaMNobleJRoyleSGTrailIAAllenJDupuytren’s and epilepsy revisitedJ Hand Surg Br19921722212241588209
- BurgePHoyGReganPMilneRSmoking, alcohol and the risk of Dupuytren’s contractureJ Bone Joint Surg Br19977922062109119843
- GodtfredsenNSLuchtHPrescottESorensenTIGronbaekMA prospective study linked both alcohol and tobacco to Dupuytren’s diseaseJ Clin Epidemiol200457885886315485739
- GudmundssonKGArngrimssonRJonssonTDupuytren’s disease, alcohol consumption and alcoholismScand J Prim Health Care200119318619011697563
- LucasGBrichetARoquelaureYLeclercADescathaADupuytren’s disease: personal factors and occupational exposureAm J Ind Med200851191518033693
- LoganAJMasonGDiasJMakwanaNCan rock climbing lead to Dupuytren’s disease?Br J Sports Med200539963964416118302
- ThomasPRClarkeDVibration white finger and Dupuytren’s contracture: are they related?Occup Med (Lond)19924231551581345125
- LoosBPuschkinVHorchRE50 years experience with Dupuytren’s contracture in the Erlangen University Hospital – a retrospective analysis of 2919 operated hands from 1956 to 2006BMC Musculoskelet Disord200786017610744
- ElliotDThe early history of Dupuytren’s diseaseHand Clin1999151119v10050238
- RayanGMNonoperative treatment of Dupuytren’s diseaseJ Hand Surg Am20083371208121018762122
- HuestonJTThe table top testHand19821411001037060997
- RossDCGanBSAcquired diseases of the handSiemionowMTextbook of Plastic SurgeryNew York, NYSpringer2010583597
- SwartzWMLalondeDHMOC-PS(SM) CME article: Dupuytren’s diseasePlast Reconstr Surg2008121Suppl 411018379378
- McIndoeABeareRLThe surgical management of Dupuytren’s contractureAm J Surg195895219720313487940
- RowleyDICouchMChesneyRBNorrisSHAssessment of percutaneous fasciotomy in the management of Dupuytren’s contractureJ Hand Surg Br1984921631646747419
- van RijssenALWerkerPMPercutaneous needle fasciotomy in dupuytren’s diseaseJ Hand Surg Br200631549850116766101
- ChengHSHungLKTseWLHoPCNeedle aponeurotomy for Dupuytren’s contractureJ Orthop Surg (Hong Kong)2008161889018453667
- FoucherGMedinaJNavarroRPercutaneous needle aponeurotomy: complications and resultsJ Hand Surg2003285427431
- BrotherstonTMBalakrishnanCMilnerRHBrownHGLong term follow-up of dermofasciectomy for Dupuytren’s contractureBr J Plast Surg19944764404437952813
- ArmstrongJRHurrenJSLoganAMDermofasciectomy in the management of Dupuytren’s diseaseJ Bone Joint Surg Br2000821909410697321
- LarsonDJerosch-HeroldCClinical effectiveness of post-operative splinting after surgical release of Dupuytren’s contracture: a systematic reviewBMC Musculoskelet Disord2008910418644117
- EvansRBDellPCFiolkowskiPA clinical report of the effect of mechanical stress on functional results after fasciectomy for Dupuytren’s contractureJ Hand Ther200215433133912449347
- McFarlaneRMMcGroutherDAComplications and their managementMcFarlaneRMFlintDADupuytren’s DiseaseEdinburgh, UKChurchill Livingstone1990348364
- HuestonJTEnzymic fasciotomyHand19713138405098337
- BaileyAJSimsTJGabbianiGBazinSLeLousMCollagen of Dupuytren’s diseaseClin Sci Mol Med1977535499502589933
- Brickley-ParsonsDGlimcherMJSmithRJAlbinRAdamsJPBiochemical changes in the collagen of the palmar fascia in patients with Dupuytren’s diseaseJ Bone Joint Surg Am19816357877977240301
- HurstLCBadalamenteMAHentzVRInjectable collagenase clostridium histolyticum for Dupuytren’s contractureN Engl J Med20093611096897919726771
- BadalamenteMAHurstLCHentzVRCollagen as a clinical target: nonoperative treatment of Dupuytren’s diseaseJ Hand Surg Am200227578879812239666
- BadalamenteMAHurstLCEfficacy and safety of injectable mixed collagenase subtypes in the treatment of Dupuytren’s contractureJ Hand Surg Am200732676777417606053
- WattAJCurtinCMHentzVRCollagenase injection as nonsurgical treatment of dupuytren’s disease: 8-year follow-upJ Hand Surg Am2010354534539539 e53120353858
- KetchumLDDonahueTKThe injection of nodules of Dupuytren’s disease with triamcinolone acetonideJ Hand Surg Am20002561157116211119679
- PagnottaASpecchiaNSoccettiAManzottiSGrecoFResponsiveness of Dupuytren’s disease fibroblasts to 5 alpha-dihydrotestosteroneJ Hand Surg Am20032861029103414642522
- MeekRMMcLellanSReillyJCrossanJFThe effect of steroids on Dupuytren’s disease: role of programmed cell deathJ Hand Surg Br200227327027312074617
- NewmanRJLocal skin depigmentation due to corticosteroid injectionBr Med J (Clin Res Ed)1984288643217251726
- OikarinenAAutioPNew aspects of the mechanism of corticosteroid-induced dermal atrophyClin Exp Dermatol19911664164191806315
- PittetBRubbia-BrandtLDesmouliereAEffect of gamma-interferon on the clinical and biologic evolution of hypertrophic scars and Dupuytren’s disease: an open pilot studyPlast Reconstr Surg1994936122412358171142
- SandersJLDoddCGhaharyAScottPGTredgetEEThe effect of interferon-alpha2b on an in vitro model Dupuytren’s contractureJ Hand Surg Am199924357858510357539
- TanakaKSanoKNakanoTYubaKKinoshitaMSuppression of alpha smooth muscle actin expression by IFN-gamma in established myofibroblast cell linesJ Interferon Cytokine Res2007271083583917970692
- BowleyEO’GormanDBGanBSBeta-catenin signaling in fibroproliferative diseaseJ Surg Res2007138114115017109886
- JohnstonPLarsonDClarkIMChojnowskiAJMetalloproteinase gene expression correlates with clinical outcome in Dupuytren’s diseaseJ Hand Surg Am20083371160116718762113
- UlrichDHrynyschynKPalluaNMatrix metalloproteinases and tissue inhibitors of metalloproteinases in sera and tissue of patients with Dupuytren’s diseasePlast Reconstr Surg200311251279128614504511
- HutchinsonJWTierneyGMParsonsSLDavisTRDupuytren’s disease and frozen shoulder induced by treatment with a matrix metalloproteinase inhibitorJ Bone Joint Surg Br19988059079089768907
- TownleyWACambreyADKhawPTGrobbelaarAOThe role of an MMP inhibitor in the regulation of mechanical tension by Dupuytren’s disease fibroblastsJ Hand Surg Eur Vol200934678378719786408
- TownleyWACambreyADKhawPTGrobbelaarAOMatrix metalloproteinase inhibition reduces contraction by dupuytren fibroblastsJ Hand Surg Am20083391608161618984345
- PasternakBAspenbergPMetalloproteinases and their inhibitors-diagnostic and therapeutic opportunities in orthopedicsActa Orthop200980669370319968600
- QianAMealsRARajferJGonzalez-CadavidNFComparison of gene expression profiles between Peyronie’s disease and Dupuytren’s contractureUrology200464239940415302515
- RehmanSSalwayFStanleyJKOllierWEDayPBayatAMolecular phenotypic descriptors of Dupuytren’s disease defined using informatics analysis of the transcriptomeJ Hand Surg Am200833335937218343292
- ShihBBrownJJArmstrongDJLindauTBayatADifferential Gene expression analysis of subcutaneous fat, fascia, and Skin overlying a Dupuytren’s disease Nodule in comparison to control tissueHand (NY)200943294301
- SatishLLaframboiseWAO’GormanDBIdentification of differentially expressed genes in fibroblasts derived from patients with Dupuytren’s ContractureBMC Med Genomics200811018433489
- ViLFengLZhuRDPeriostin differentially induces proliferation, contraction and apoptosis of primary Dupuytren’s disease and adjacent palmar fascia cellsExp Cell Res2009315203574358619619531
- HowardJCVaralloVMRossDCElevated levels of beta-catenin and fibronectin in three-dimensional collagen cultures of Dupuytren’s disease cells are regulated by tension in vitroBMC Musculoskelet Disord200341612866952
- HowardJCVaralloVMRossDCWound healing-associated proteins Hsp47 and fibronectin are elevated in Dupuytren’s contractureJ Surg Res2004117223223815047128
- ShihBWijeratneDArmstrongDJLindauTDayPBayatAIdentification of biomarkers in Dupuytren’s disease by comparative analysis of fibroblasts versus tissue biopsies in disease-specific phenotypesJ Hand Surg Am200934112413619121738
- SedicMJurisicDStanecZHockKPavelicKKraljevic PavelicSFunctional genomics in identification of drug targets in Dupuytren’s contractureFront Biosci201015576420036806
- Kraljevic PavelicSSedicMHockKAn integrated proteomics approach for studying the molecular pathogenesis of Dupuytren’s diseaseJ Pathol2009217452453319089850
- VaralloVMGanBSSeneySBeta-catenin expression in Dupuytren’s disease: potential role for cell-matrix interactions in modulating beta-catenin levels in vivo and in vitroOncogene200322243680368412802275
- ViLGanBSO’GormanDBThe potential roles of cell migration and extra-cellular matrix interactions in Dupuytren’s disease progression and recurrenceMed Hypotheses201074351051219896280
- ViLNjarlangattilAWuYGanBSO’GormanDBType-1 Collagen differentially alters beta-catenin accumulation in primary Dupuytren’s Disease cord and adjacent palmar fascia cellsBMC Musculoskelet Disord2009107219545383
- LoechelFFoxJWMurphyGAlbrechtsenRWewerUMADAM 12-S cleaves IGFBP-3 and IGFBP-5 and is inhibited by TIMP-3Biochem Biophys Res Commun2000278351151511095942
- ShiZXuWLoechelFWewerUMMurphyLJADAM 12, a disintegrin metalloprotease, interacts with insulin-like growth factor-binding protein-3J Biol Chem200027524185741858010849447
- DenysHJadidizadehAAmini NikSIdentification of IGFBP-6 as a significantly downregulated gene by beta-catenin in desmoid tumorsOncogene200423365466414737101
- ChenXFerryRJJrNovel actions of IGFBP-3 on intracellular signaling pathways of insulin-secreting cellsGrowth Horm IGF Res2006161414816275148
- CusiKDeFronzoRRecombinant human insulin-like growth factor I treatment for 1 week improves metabolic control in type 2 diabetes by ameliorating hepatic and muscle insulin resistanceJ Clin Endocrinol Metab20008593077308410999789
- Lopez-BermejoAKhosraviJFernandez-RealJMInsulin resistance is associated with increased serum concentration of IGF-binding protein-related protein 1 (IGFBP-rP1/MAC25)Diabetes20065582333233916873698
- Mohamed-AliVPinkneyJTherapeutic potential of insulin-like growth factor-1 in patients with diabetes mellitusTreat Endocrinol20021639941015832492
- HartMGHooperGClinical associations of Dupuytren’s diseasePostgrad Med J20058195742542815998816
- ArkkilaPEKantolaIMViikariJSDupuytren’s disease: association with chronic diabetic complicationsJ Rheumatol19972411531599002027
- CarrieriMPSerrainoDPalmiottoFNucciGSassoFA case-control study on risk factors for Peyronie’s diseaseJ Clin Epidemiol19985165115159636000
- ClassenDAHurstLNPlantar fibromatosis and bilateral flexion contractures: a review of the literatureAnn Plast Surg19922854754781622023
- DonatoRRMorrisonWADupuytren’s disease in the feet causing flexion contractures in the toesJ Hand Surg1996213364366
- SmithSPDevaraj vs BunkerTDThe association between frozen shoulder and Dupuytren’s diseaseJ Shoulder Elbow Surg200110214915111307078
- BunkerTDAnthonyPPThe pathology of frozen shoulder. A Dupuytren-like diseaseJ Bone Joint Surg Br19957756776837559688
- BunkerTDReillyJBairdKSHamblenDLExpression of growth factors, cytokines and matrix metalloproteinases in frozen shoulderJ Bone Joint Surg Br200082576877310963182
- LeeYCChanHHBlackMMAggressive polyfibromatosis: a 10 year follow-upAustralas J Dermatol19963742052078961590