
Abstract
Aim
We aimed to summarize the pooled effect of early discharge compared with ordinary discharge after percutaneous coronary intervention (PCI) on the composite endpoint of re-infarction, revascularization, stroke, death, and incidence of rehospitalization. We also aimed to compare costs for the two strategies.
Methods
The study was a systematic review and a meta-analysis of 12 randomized controlled trials including 2962 patients, followed by trial sequential analysis. An estimation of cost was considered. Follow-up time was 30 days.
Results
For early discharge, pooled effect for the composite endpoint was relative risk of efficacy (RRe)=0.65, 95% confidence interval (CI) (0.52–0.81). Rehospitalization had a pooled effect of RRe=1.10, 95% CI (0.88–1.38). Early discharge had an increasing risk of rehospitalization with increasing frequency of hypertension for all populations, except those with stable angina, where a decreasing risk was noted. Advancing age gave increased risk of revascularization. Early discharge had a cost reduction of 655 Euros per patient compared with ordinary discharge.
Conclusion
The pooled effect supports the safe use of early discharge after PCI in the treatment of a heterogeneous population of patients with coronary artery disease. There was an increased risk of rehospitalization for all subpopulations, except patients with stable angina. Clinical trials with homogeneous populations of acute coronary syndrome are needed to be conclusive on this issue.
Introduction
Today, percutaneous coronary intervention (PCI) is one of the most commonly performed cardiac interventions.Citation1 The cost of treatment for acute coronary syndrome (ACS) in Western Europe is high and constitutes a considerable portion of total health care expenses. This is mainly attributed to revascularization procedures and the cost of hospital stay.Citation2,Citation3
Systematic use of stents and potent platelet inhibitors has revolutionized the success rate after PCI by drastically reducing the risk of acute occlusion in the first 24 hours after a successful procedure.Citation4 Reduced catheter sizes have made a transradial approach more feasible, which in turn has reduced bleeding incidents as well as the necessary observation time. Early discharge is routinely practiced in some parts of Europe and Canada but is rare in the US. Reasons may be concerns over patient safety and short-term clinical events, differences in procedures and use of pharmacology, as well as different systems for financial compensation.
With an increasing demand for hospital resources, the trend has moved toward the implementation of fast-track treatment pathways.Citation5 Several observational studies, and some randomized controlled trials (RCTs), have aimed to prove that same-day or early discharge after PCI is both feasible and safe. The patient populations in these studies include those with elective PCI, unstable angina pectoris (UAP), non-ST elevation myocardial infarction (NSTEMI), and ST elevation myocardial infarction (STEMI) patients.Citation6,Citation7
Cost analyses of early discharge versus ordinary discharge show that early discharge is economically favorable, primarily by eliminating the cost of overnight observation.Citation8–Citation10
Two meta-analyses and systematic reviewsCitation11,Citation12 claimed, based on observational studies and RCTs, support of programs for same-day discharge after PCI for selected groups of patients without defining the groups. The study populations in the RCTs that have been executed in this field are all relatively small. We have undertaken a systematic review and meta-analysis of only RCTs and have not considered observational studies.
The aim of this study was to summarize the pooled effect of early discharge compared with ordinary discharge after PCI on the primary composite endpoint of re-infarction, revascularization, stroke, death, and the incidence of rehospitalization. Second, we wanted to compare costs for the two strategies.
Methods
We searched the Cochrane Central Register of controlled trials (1970–2015), Embase (1980–2015), and Medline/PubMed (1966–2015). We combined the keywords outpatient, same day discharge, early discharge, percutaneous coronary intervention, PCI, angioplasty, economy, and cost. Similar strategies were used to search for previously published meta-analyses and reviews. We also screened reference lists and contacted authors. Our last update for research was done on August 5, 2015. No limitation on language was considered.
Inclusion criteria for the studies were RCTs comparing early discharge versus ordinary discharge after PCI and safety outcome data for up to 30 days following the index intervention, available for both groups separately. We included only studies from 1999 onward.
When cost analysis was available, it had to include an overview of cost related to both groups separately.
Twelve RCTs were considered eligible for this study ().Citation4,Citation13–Citation23
Figure 1 Details of the search process. Last search was performed August 5, 2015.
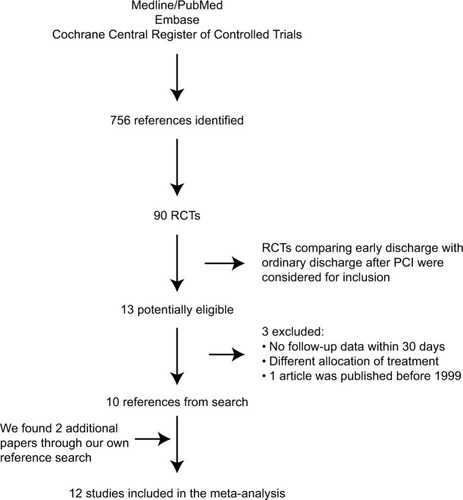
The definition of early discharge differs between the studies because of different patient populations. Eight studies have patients with stable coronary artery disease (CAD), UAP, and NSTEMI.Citation4,Citation15–Citation18,Citation20,Citation22,Citation23 They define early discharge as discharge on the same day as the intervention. The remaining four studies have patients with STEMI.Citation13,Citation14,Citation19,Citation21 Their definition of early discharge was discharge between 48 and 72 hours after the intervention.
Three of these included an analysis of cost.Citation20,Citation22,Citation23 Two additional articles with an assessment of cost were based on studies already included in the safety analysis, and we added these to our cost analyses.Citation8,Citation9 Andersen et alCitation16 originally included 399 patients in their study. In the meta-analysis of safety, we have considered only the 167 who had PCI during their index stay.
Endpoints
Our primary endpoint was the incidence of the composite cardiovascular events mortality, re-infarction, revascularization, and stroke. The secondary endpoint was rehospitalization, both endpoints within 30 days after PCI. Finally, a 30-day estimation of the cost of the two strategies was considered.
The statistical methods used for our analyses have previously been described in detail by Abdelnoor et al.Citation24
Trial sequential analysis (TSA) was used according to Pogue and YusufCitation25 and Wetterslev et al.Citation26 We used TSA as it is implemented in the STATA Program 12 (StataCorp LLC, College Station, TX, USA). This method permits to consider the accumulated number of patients to estimate the power of our cumulative meta-analysis.
Robustness of the pooled estimates was checked by sensitivity analysis. Each of the studies was individually omitted from the data set, followed in each case by recalculation of the pooled estimate of the remaining studies.
We followed the PRISMA guidelines for meta-analyses and systematic reviews of randomized trials in this report.Citation27
Results
The baseline characteristics are represented in . The 12 trials included 2962 patients, 1486 patients in the early discharge group and 1476 patients in the ordinary discharge group. Considering the study-level variables with regard to the primary endpoint, 37% had concealment of randomization, 27% had outcome blinded to the investigators, 91% used the intention-to-treat analysis, and 81% of the trials did not have drop-out during follow-up. For the outcome rehospitalization, 36% had concealment of randomization, 27% had blinding of the investigators to the outcome, 91% used the intention-to-treat analysis, and 82% of the trials did not have drop-out during follow-up.
Table 1 Baseline characteristics
The majority of the trials suffered serious methodological biases and were power deficient. Five RCTs included cost analysis and were included in the cost study. Three of these had correct concealment, one had blinding of investigator to the outcome, four followed the intention-to-treat analysis, and three had no drop-out during followup. All costs were recalculated to the value of the Euro in December 2014.
Primary composite endpoint
The pooled estimate of the efficacy ( and ) showed an estimate of relative risk [RR]=0.65, 95% confidence interval (95% CI) (0.52–0.81), p=0.0002, indicating a lower risk in the early discharge group compared to ordinary discharge group for the primary composite endpoint with no heterogeneity. There was no selection bias. We ran subgroup and meta-regression analyses on study-level and patient-level variables. Meta-regression is a method to investigate heterogeneity, and it permits to quantify the association between variables and effect of the intervention. With regard to study-level variables, none was associated with the efficacy. Considering patient-level variables, none of the covariates showed an association with the efficacy on the primary endpoint ( and ).
Table 2 Pooled estimate of RR of efficacy for ED compared to OC on the primary composite endpoint, with stratification on attrition bias and detection bias using the fixed-effect model
Table 3 Estimate of the mixed-effect regression model between logRR and primary composite endpoint and the different study-level and patient-level variables in a univariate analysis using 11 trials
A sensitivity analysis revealed the non-robustness of our results for the primary composite endpoint. Our hypothesis was a risk reduction of 15% lower incidence in the ordinary care group versus early discharge group. For an accumulated number of 2912 patients and a type I error of 5%, we have a power of the cumulative meta-analysis of 98%. For the primary composite endpoint, our meta-analysis includes enough patients and has satisfactory power.
Re-infarction and rehospitalization
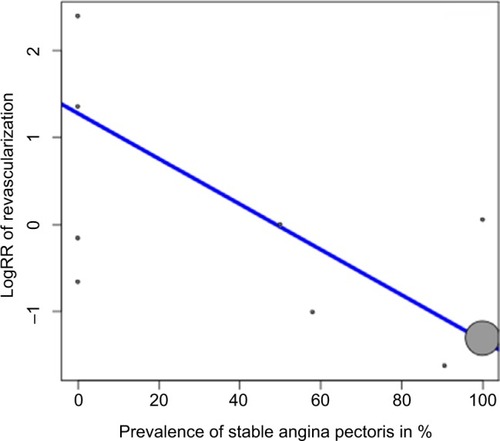
Another run of pooled efficacy and sensitivity analysis on re-infarction and incidence of revascularization showed that for re-infarction the pooled RR of efficacy was RR=0.45, 95% CI (0.31–0.66), p=0.001, for early discharge compared to ordinary discharge, with no heterogeneity considering 10 studies. A sensitivity analysis confirmed the non-robustness of our results with regard to re-infarction. With regard to revascularization, we found a pooled efficacy of RR=0.38, 95% CI (0.18–0.79), p=0.009, for early discharge compared to ordinary discharge. A sensitivity analysis pinpointed the non-robustness of our results. Meta-regression showed a significant increase of risk for revascularization in the early discharge group with increasing prevalence of NSTEMI/UAP () and the same with increasing age of the patient. With increasing prevalence of stable angina, there was a decreasing risk of revascularization in the early discharge group compared with ordinary discharge ().
Figure 2 Meta-regression for the efficacy of ED compared to OD on the incidence of revascularization versus prevalence of NSTEMI or UAP
Abbreviations: ED, early discharge; OD, ordinary discharge; NSTEMI, non-ST elevation myocardial infarction; UAP, unstable angina pectoris; RR, relative risk.
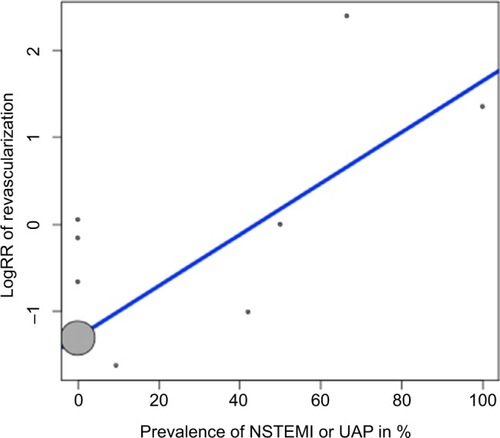
Figure 3 Meta-regression for the efficacy of ED compared to OD on the incidence of revascularization versus prevalence of stable angina pectoris.
Abbreviations: ED, early discharge; OD, ordinary discharge; RR, relative risk.
Endpoint rehospitalization
The pooled estimate of the effect of the early discharge showed an estimate of RR=1.10, 95% CI (0.88–1.38), p=0.37, with a substantial heterogeneity of 16% with no difference of efficacy in the two groups, There was no selection bias. A sensitivity analysis using the random model indicated the non-robustness of our results. We ran a subgroup analysis () and meta-regression () on study-level and patient-level variables. Regarding study-level variables, concealment (p=0.004), blinding (p=0.001), and drop-out (p=0.004) during follow-up were associated with efficacy, as also the prevalence of STEMI (p=0.005), NSTEMI/UAP (p=0.001), and stable angina (p=0.008). This indicates an association between efficacy of early discharge and those variables.
Table 4 Pooled estimate of RR of efficacy for ED compared to OD on the endpoint rehospitalization, with stratification on concealment and no drop-out using the random-effect model
Table 5 Estimate of the mixed-effect regression model between logRR and rehospitalization and the different study-level and patient-level variables in a univariate analysis using 12 trials
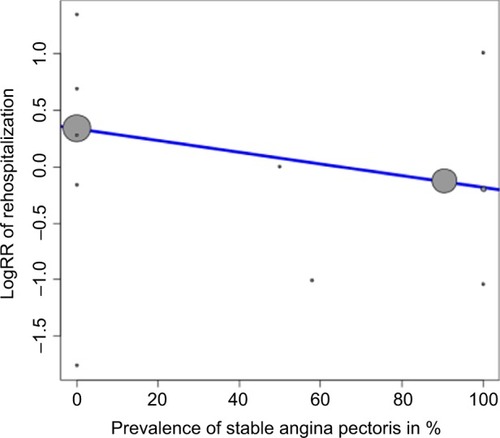
For the patient-level variables, the frequency of hypertension was associated with efficacy (p=0.004) (). This indicates increasing risk of rehospitalization for patients in the early discharge group compared to the ordinary care group with increasing frequency of hypertension, increasing prevalence of STEMI, and increasing prevalence of NSTEMI/UAP. There was a decreasing risk for rehospitalization with increasing prevalence of stable angina ().
Figure 4 Meta-regression for the efficacy of ED compared to OD on the incidence of rehospitalization versus prevalence of hypertension.
Abbreviations: ED, early discharge; OD, ordinary discharge; RR, relative risk.
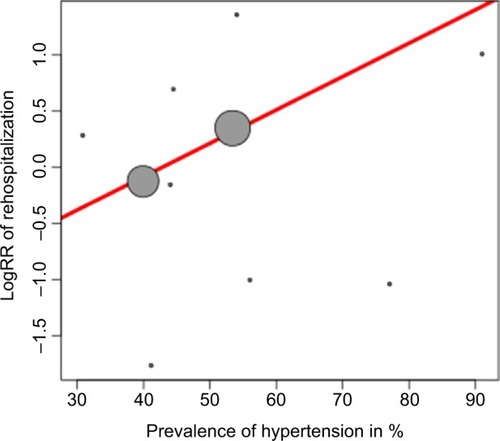
Figure 5 Meta-regression of the efficacy of ED compared to OD on the incidence of rehospitalization versus prevalence of stable angina pectoris
Abbreviations: ED, early discharge; OD, ordinary discharge; RR, relative risk.
The TSA for the endpoint rehospitalization had a hypothesis of 15% risk reduction for rehospitalization in the ordinary discharge group compared to the early discharge group. For an accumulated number of 2912 patients and a type I error of 5%, we have a power of the cumulative meta-analysis of 92%.
We can conclude that for the endpoint rehospitalization, our cumulative meta-analysis has satisfactory power.
Cost
We identified five RCTs that described the economic impact related to early discharge compared with ordinary discharge after PCI ().Citation8,Citation9,Citation20,Citation22,Citation23 Most of the studies separated procedural cost and the cost of care and observation after the intervention. Three studies described total costs. Three articles mentioned only the cost of care and observation and estimated that procedural costs would be the same in both groups. One study calculated with larger procedural cost in the early discharge group due to the use of a vascular closure device. Rehospitalization within the follow-up period was included in the costs.
Table 6 Cost between the two strategies ED and OD after PCI (Euros per patient)
All studies found a decrease in total treatment cost for the early discharge group, with a reduction of 5.2%–50.1%. In these studies, this means a saving of 294–1875 Euros per patient.
Three studies disclosed the length of stay (LOS).Citation8,Citation9,Citation23 LOS included the index stay as well as subsequent rehospitalization within 30 days. Mean LOS varied between 5.9 hours in the early discharge group to 29.8 hours in the ordinary care group.
Discussion
Safety
The results of our systematic review indicated a reduction in the composite clinical endpoint with early discharge. However, there was a possibility of increased risk of rehospitalization for early discharge compared to ordinary care patients with hypertension and an increasing risk of UAP/revascularization with increasing age of the patient.
Our results regarding the safety of early discharge compared to ordinary care on the outcomes of the primary and secondary endpoints changed when we arranged the components of trial quality. The trials were assessed individually and methodologically, and their influence on effect size was explored. It has been shown that when studies of low methodological quality are incorporated into the meta-analysis, the estimate of quality can alter the interpretation of the benefit of the intervention. We found a reduction in the primary composite endpoint for the early discharge strategy. We found a possibility of increasing risk of rehospitalization with early discharge with increasing frequency of hypertension.
When heterogeneity was present, we performed meta-regression analyses on study-level and patient-level variables. It was not performed if the number of studies was <10. We had specified patient-level variables a priori in the protocol of our meta-analysis. Only biologically plausible mechanisms were considered.Citation28,Citation29
Patient-related variables such as frequency of hypertension and age of patients can be subject to ecological fallacy and should be considered hypothesis generating,Citation30 while the study-level variables that were considered in this meta-regression (concealment of randomization, drop-out) can detect real associations between effect of the treatment and the study-level variables.Citation31
Our results show that unstable patients are more often the subject of complications and rehospitalization. Increasing age often results in co-morbidities and a higher risk. An unexpected finding was that the prevalence of hypertension should mean increased risk for rehospitalization. This indicates that extra care must be taken to assess risk and in selecting the appropriate patients suitable for early discharge.
Cost
Procedural variables are the strongest predictor of post- procedural complications.Citation32 Vavalle et alCitation33 found that the patients with longer LOS often had more co-morbidities and in-hospital complications. Analyzing procedural results can help triage patients suitable for early discharge. The use of validated risk scores such as Zwolle can be of help in identifying low-risk patients, suitable for early discharge.Citation34 The decrease in costs in the early discharge group is due to the reduction in LOS, and thus in the cost of care, both at the index stay and in the days of follow-up. This is confirmed by Le Corvoisier et al.Citation35
Bakhai et alCitation3 found that the risk of a new clinical event within 1 year after ACS treated with PCI is high among the Western European population. A finding of Korsnes et alCitation36 was that the first major adverse cardiovascular event is more costly than subsequent events. Several studies have found that most adverse events related to the intervention occur shortly post-procedure and not in an extended observational period.Citation37–Citation39 This is in line with the results of the studies included in this meta-analysis and also with our pooled results. This suggests that occurrence of adverse events is not related to the discharge procedure. It is thus possible to decrease direct expenses by reducing LOS, considering the specific diagnosis of the patient. Our results show an increased risk of rehospitalization in the early discharge group, with the exception for patients with stable angina. Despite this finding, we see a reduction of cost in the early discharge group.
The time allotted to an intervention is the same, regardless of discharge strategy. Early discharge does not free up resources in the laboratory itself. But by reduced LOS in the early discharge group, resources used for observation and monitoring of patients were made available. Unfortunately, none of the studies in our meta-analysis have explored in what way these additional resources have been utilized or in what way this affects the economy.
A limitation to this cost analysis is that not all studies disclose the total cost. The reporting of costs included is also of variable quality. We have looked at costs related to the population as a whole because the quantitative basis for differentiating between STEMI, NSTEMI, UAP, and elective procedures is too small. It is possible that cost-effectiveness may vary between the groups to a greater extent than shown here.
Strengths and limitations
The major limitations of our study were the use of heterogeneous patient populations, quality of the trials with respect to the effect estimated, heterogeneity, underpowered trials, and use of other endpoints than our primary endpoint and rehospitalization.
Conclusion
Expenses in the early discharge group were lower compared with the ordinary discharge group, mainly due to a reduction in LOS and the cost of care.
The pooled effect for the composite cardiovascular endpoint supports the safe use of early compared to ordinary discharge after PCI in the treatment of a heterogeneous population of patients with CAD. However, for the endpoint rehospitalization, an increased risk was noted in patients with STEMI, NSTEMI, or unstable angina, but not in patients with stable angina.
Clinical trials with homogeneous populations of ACS are needed to be conclusive on this issue.
Disclosure
The authors report no conflicts of interest in this work.
References
- CookSWalkerAHugliOTogniMMeierBPercutaneous coronary interventions in Europe: prevalence, numerical estimates, and projections based on data up to 2004Clin Res Cardiol200796637538217453137
- TaylorMJScuffhamPAMcCollamPLNewbyDEAcute coronary syndromes in Europe: 1-year costs and outcomesCurr Med Res Opin200723349550317355731
- BakhaiAFerrieresJIniguezAClinical outcomes, resource use, and costs at 1 year in patients with acute coronary syndrome undergoing PCI: results from the Multinational APTOR RegistryJ Interv Cardiol2012251192722150757
- KnopfWDCohen-BernsteinCRyanJHeselovKYarbroughNSteahrGOutpatient PTCA with same day discharge is safe and produces high patient satisfaction levelJ Invasive Cardiol199911529029510745532
- LautKGFoldspangAThe effects on length of stay of introducing a fast track patient pathway for myocardial infarction: a before and after evaluationHealth Serv Manage Res2012251313422323669
- DoDHDaleryKGervaisASame-day transfer of patients with unstable angina and non-ST segment elevation myocardial infarction back to their referring hospital after angioplastyCan J Cardiol200622540540916639476
- VendramettoFOberhollenzerRPitscheiderWPercutaneous coronary intervention and immediate re-transfer to the referring hospital for patients with acute coronary syndrome. A single-center experienceG Ital Cardiol (Rome)20067428128616700411
- RinfretSKennedyWALachaineJEconomic impact of same-day home discharge after uncomplicated transradial percutaneous coronary intervention and bolus-only abciximab regimenJACC Cardiovasc Interv20103101011101920965458
- AndersenJGGrepperudSKlowNEJohansenOEffects on length of stay and costs with same-day retransfer to the referring hospitals for patients with acute coronary syndrome after angiography and/or per-cutaneous coronary interventionEur Heart J Acute Cardiovasc Care20165437538026139591
- PopescuAMWeintraubWSOutpatient percutaneous coronary interventions hospital and health system costs saving while maintaining patient safetyJACC Cardiovasc Interv20103101020102120965459
- BraytonKMPatelVGStaveCde LemosJAKumbhaniDJSame-day discharge after percutaneous coronary intervention: a meta-analysisJ Am Coll Cardiol201362427528523623905
- AbdelaalERaoSVGilchristICSame-day discharge compared with overnight hospitalization after uncomplicated percutaneous coronary intervention: a systematic review and meta-analysisJACC Cardiovasc Interv2013629911223352820
- AzzaliniLSoleESansJFeasibility and safety of an early discharge strategy after low-risk acute myocardial infarction treated with primary percutaneous coronary intervention: the EDAMI pilot trialCardiology2015130212012925612789
- MelbergTJorgensenMOrnSSolliTEdlandUDicksteinKSafety and health status following early discharge in patients with acute myocardial infarction treated with primary PCI: a randomized trialEur J Prev Cardiol201522111427143425398704
- KimMMuntnerPSharmaSAssessing patient-reported outcomes and preferences for same-day discharge after percutaneous coronary intervention: results from a pilot randomized, controlled trialCirc Cardiovasc Qual Outcomes20136218619223481528
- AndersenJGKløwN-EJohansenOSafe and feasible immediate retransfer of patients to the referring hospital after acute coronary angi-ography and percutaneous coronary angioplasty for patients with acute coronary syndromeEur Heart J Acute Cardiovasc Care20132325626124222837
- FalconeAMBoseRStolerRCThe AmBulatory Closure Device Percutaneous Intervention (ABCD-PCI) study: a single-center experienceProc (Bayl Univ Med Cent)201124319219421738289
- BertrandOFDe LarochelliereRRodes-CabauJA randomized study comparing same-day home discharge and abciximab bolus only to overnight hospitalization and abciximab bolus and infusion after transradial coronary stent implantationCirculation2006114242636264317145988
- KotowyczMACosmanTLTartagliaCAfzalRSyalRPNatarajanMKSafety and feasibility of early hospital discharge in ST-segment elevation myocardial infarction – a prospective and randomized trial in low-risk primary percutaneous coronary intervention patients (the Safe-Depart Trial)Am Heart J20101591e111e116
- GlaserRGertzZMatthaiWHPatient satisfaction is comparable to early discharge versus overnight observation after elective percutaneous coronary interventionJ Invasive Cardiol200921946446719726820
- JirmarRWidimskyPCapekJHlinomazOGrochLNext day discharge after successful primary angioplasty for acute ST elevation myocardial infarction. An open randomized study “Prague-5”Int Heart J200849665365919075481
- HeydeGSKochKTde WinterRJRandomized trial comparing same-day discharge with overnight hospital stay after percutaneous coronary intervention: results of the Elective PCI in Outpatient Study (EPOS)Circulation2007115172299230617420341
- CarereRGWebbJGBullerCESuture closure of femoral arterial puncture sites after coronary angioplasty followed by same-day dischargeAm Heart J20001391 pt 1525810618562
- AbdelnoorMSandvenILimalanathanSEritslandJPostconditioning in ST-elevation myocardial infarction: a systematic review, critical appraisal, and meta-analysis of randomized clinical trialsVasc Health Risk Manag20141047749125143742
- PogueJYusufSOvercoming the limitations of current meta-analysis of randomised controlled trialsLancet1998351909547529433436
- WetterslevJThorlundKBrokJGluudCTrial sequential analysis may establish when firm evidence is reached in cumulative meta-analysisJ Clin Epidemiol2008611647518083463
- MoherDLiberatiATetzlaffJAltmanDGPRISMA GroupPreferred reporting items for systematic reviews and meta-analyses: the PRISMA statementAnn Intern Med20091514264269W26419622511
- BerlinJASantannaJSchmidCHSzczechLAFeldmanHIAnti-Lymphocyte Antibody Induction Therapy Study GroupIndividual patient-versus group-level data meta-regressions for the investigation of treatment effect modifiers: ecological bias rears its ugly headStat Med200221337138711813224
- HigginsJPGreenSCochrane Handbook for Systematic Reviews of Interventions5Wiley Online Library2008 Available from: http://handbook.cochrane.org/chapter_9/9_6_4_meta_regression.htmAccessed October 11, 2016
- MorgensternHUses of ecologic analysis in epidemiologic researchAm J Public Health19827212133613447137430
- SchmidCHStarkPCBerlinJALandaisPLauJMeta-regression detected associations between heterogeneous treatment effects and study-level, but not patient-level, factorsJ Clin Epidemiol200457768369715358396
- KochKTPiekJJPrinsMHTriage of patients for short term observation after elective coronary angioplastyHeart200083555756310768908
- VavalleJPLopesRDChenAYHospital length of stay in patients with non-ST-segment elevation myocardial infarctionAm J Med2012125111085109422921886
- KotowyczMASyalRPAfzalRNatarajanMKCan we improve length of hospitalization in ST elevation myocardial infarction patients treated with primary percutaneous coronary intervention?Can J Cardiol2009251058558819812804
- Le CorvoisierPGellenBLesaultPFAmbulatory transradial percutaneous coronary intervention: a safe, effective, and cost-saving strategyCatheter Cardiovasc Interv2013811152322744871
- KorsnesJSDavisKLArielyRBellCFMitraDHealth care resource utilization and costs associated with nonfatal major adverse cardiovascular eventsJ Manag Care Spec Pharm201521644345026011546
- JozicJOrfordJSteinhublSBergerPHsuATopolETiming and correlates of very early major adverse clinical events following percutaneous coronary interventionJ Invasive Cardiol200820311311818316826
- ThelMCCaliffRMTardiffBETiming of and risk factors for myocardial ischemic events after percutaneous coronary intervention (IMPACT-II). Integrilin to minimize platelet aggregation and coronary thrombosisAm J Cardiol200085442743410728945
- JabaraRGadesamRPendyalaLAmbulatory discharge after transradial coronary intervention: preliminary US single-center experience (Same-day TransRadial Intervention and Discharge Evaluation, the STRIDE Study)Am Heart J200815661141114619033010