
Abstract
Background
Low-molecular-weight heparin (LMWH) is a recommended anticoagulant for thromboprophylaxis after major orthopedic surgery. Dabigatran etexilate is an oral anticoagulant recognized as noninferior to LMWH. We aimed to assess the incidence of symptomatic venous thromboembolic events (VTEs) after discharge in patients who underwent joint replacement, using a hospital registry.
Patients and methods
Patients who underwent total knee and hip arthroplasty between September 2011 and March 2015 were selected. Subcutaneous enoxaparin (30 mg twice daily) was given during hospitalization. At discharge, patients received either enoxaparin 30 mg twice daily/40 mg once daily or dabigatran 220 mg/150 mg once daily. Patients were seen or called at 2, 6, and 12 weeks after surgery. Outcomes were the number of VTEs, including deep venous thrombosis, pulmonary embolism, and the number of major/minor bleeding events after discharge.
Results
After discharge, 1468 patients were prescribed enoxaparin and 904 dabigatran (1396 total knee arthroplasty and 976 total hip arthroplasty patients). Mean age was 66±10 years, and 60% were female. The cumulative incidence of VTEs during the 12-week follow-up was 0.7%. One patient sustained a VTE during the switch window. Seven patients sustained a pulmonary embolism (0.3%). There was no statistical difference between the total knee arthroplasty and total hip arthroplasty groups. The incidence of major and minor bleeding events during follow-up was 0.3% and 30.3%, respectively. These events had a higher incidence in the dabigatran group compared to the enoxaparin group after discharge (p<0.05), but not between knee and hip replacement groups for major bleeding events.
Conclusion
A pharmaceutical prophylaxis protocol using LMWH and dabigatran during the post-discharge period resulted in low incidences of VTE and equivalence between treatments. However, the increased number of major and minor bleeding events in patients taking dabigatran is of concern regarding the safety and needs to be evaluated using analyses adjusted for risk factors.
Introduction
Venous thromboembolic events (VTEs), a major health issue associated with significant mortality and morbidity, are a common complication following orthopedic surgeries, especially in total hip arthroplasty (THA) or total knee arthroplasty (TKA).Citation1,Citation2 A supplemental study of the ninth American College of Chest Physicians (ACCP) guidelines on antithrombotic therapy and prevention of thrombosis derived estimates of nonfatal symptomatic VTE rates using contemporary populations under prophylaxis from several randomized clinical trials (RCTs). They estimated a baseline risk of symptomatic VTEs, without prophylaxis after major orthopedic surgery, at 4.3% (0–35 days after surgery).Citation3 It is currently impossible to predict which patients will develop symptomatic VTE following major orthopedic surgery, hence the necessity for routine thromboprophylaxis.Citation1 The efficacy of pharmacologic prophylaxis in reducing the risk of VTEs after THA and TKA is well proven and has been standardized for over 20 years.Citation1,Citation4
The 2012 ACCP guidelines on antithrombotic therapy and prevention of thrombosis advocate a minimum of 10–14 days of thromboprophylaxis after both THA and TKA.Citation5 Given that many studies have demonstrated the importance of prolonged prophylaxis following major orthopedic surgery,Citation3,Citation6–Citation8 the ACCP recommends extended prophylaxis for up to 35 days in patients undergoing THA. This also applies to patients undergoing TKA, but with a lower level of evidence. The standard recommended anticoagulant agent for thromboprophylaxis after THA or TKA, according to the ACCP and the American Academy of Orthopedic Surgeons guidelines, is low-molecular-weight heparin (LMWH).Citation5,Citation9,Citation10 It has been shown to consistently reduce asymptomatic deep vein thrombosis (DVT) by 50%Citation3 and to be more effective than low-dose unfractionated heparin, aspirin, and vitamin K antagonists in preventing VTEs, for both types of surgery.Citation1,Citation3,Citation11–Citation13 However, LMWH requires parenteral administration, which can be problematic for long-term thromboprophylaxis in the outpatient setting,Citation14 negatively affecting patient compliance,Citation15 while also requiring home visits by health professionals for up to 20% of patients, unable to perform self-injections.Citation16
Direct oral anticoagulants have been developed to facilitate prophylaxis and the treatment of VTEs.Citation17 Among these, dabigatran etexilate, an oral direct thrombin inhibitor, has been approved in 75 countries, including Canada, but not the USA, for prophylactic use in high-risk orthopedic surgical patients.Citation18 Data from large and well-designed RCTs found it to be at least noninferior to enoxaparin, the LMWH comparator, in preventing VTEs.Citation7,Citation19,Citation20
There are ~1000 hip and knee arthroplasty procedures performed every year in our institution (Hôpital Jean-Talon, Montréal, QC, Canada). With the purpose of optimizing VTE prevention after orthopedic surgery and improving the quality of care, we aimed to evaluate the effectiveness and safety of post-discharge thromboprophylaxis up to 12 weeks after surgery as well as the treatment switch from subcutaneous enoxaparin to oral dabigatran at discharge.
Patients and methods
Study design
Using hospital registry data on thromboprophylaxis, we conducted a retrospective observational study of patients who underwent THA or TKA. The registry was implemented at Hôpital Jean-Talon from September 2011 to March 2015. The registry was authorized by the director of professional services of Hôpital Jean-Talon, and the study protocol was approved by the ethics committee of the Centre Intégré Universitaire de Santé et de Services Sociaux Nord-de-l’Île-de-Montréal. Informed consent was waived because data collection was within an implemented best clinical practice thromboprophylaxis protocol and data were gathered in a registry.
Patients were initially met at the preoperative clinic where thromboprophylaxis regimens, either enoxaparin or dabigatran etexilate, were explained and they were free to choose one or the other before discharge. However, given that dabigatran is not covered by local public insurance, only patients with private insurance, or those willing to pay, took the oral treatment. In Quebec, Canada, provincial public health insurance (Régie de l’assurance maladie du Québec) covers the drug expenses for every citizen not covered by private insurance.
Patients
All patients 18 years or older undergoing THA or TKA were included in our thromboprophylaxis registry, with no exclusion criteria, in order to maximize recruitment. For the purpose of this study, only those patients who were prescribed subcutaneous enoxaparin or oral dabigatran etexilate after discharge were selected. Thus, patients following other therapies (warfarin, rivaroxaban, apixaban) after hospital discharge were not considered for analysis. As per the protocol, patients who sustain a VTE during hospitalization are prescribed therapeutic warfarin and were, therefore, excluded from the study.
Treatment regimens/procedure
After surgery, every patient was given 30 mg subcutaneous enoxaparin twice daily, starting 12 hours postoperatively. At the time of discharge, patients either continued subcutaneous enoxaparin 30 mg twice daily or 40 mg once daily, or received a prescription of prophylactic oral dabigatran etexilate 220 mg once daily or 150 mg once daily if creatinine clearance was between 30 and 50 mL/hour, as per product description.Citation21,Citation22 On the morning of discharge, all patients received a final dose of subcutaneous enoxaparin at the hospital. The next anticoagulant dose, whether enoxaparin or dabigatran, was given 12 hours later to ensure continued appropriate thromboprophylaxis. Patients followed the treatment for a total of 14–35 days depending on the prescribing orthopedic surgeon.
Patients were followed over a 3-month period after the date of surgery. They were seen or contacted by phone at 2, 6, and 12 weeks after surgery. Collected data included age, gender, joint replaced, type of prophylaxis treatment, treatment length, patient-reported complications, VTE, and VTE history. Medical files of patients reporting a VTE were consulted to validate the event. Patients that switched from enoxaparin to dabigatran were asked specifically about the time window (2-3 days following discharge) to report the surge in VTE incidence.
Outcome measures
One of the primary outcomes was the rate of symptomatic DVT and pulmonary embolism (PE) up to 12 weeks after surgery during the post-discharge period. The other primary outcome was the rate of VTE during the switch period for patients taking dabigatran. Clinically relevant VTEs included symptomatic proximal and distal DVT and symptomatic PE. Subsegmental PE was not excluded. Patients presenting clinical signs of DVT (swelling, pain, and/or rigidity of the limb) and/or PE (desaturation, dyspnea, tachycardia, hypo- or hypertension) were investigated with duplex Doppler ultrasound imaging and ventilation–perfusion scan/computed tomography angiography, respectively. If diagnosed, they were referred to Department of Internal Medicine for treatment.
The secondary outcomes were the incidence of major and minor bleeding events registered for patients after discharge during the follow-up period. Major and minor bleeding were defined according to accepted guidelines.Citation23 Major bleeding referred to the following: fatal bleeding; clinically overt bleeding in excess, associated with ≥2 g/mL fall in hemoglobin and/or leading to transfusion of ≥2 units of packed cells or whole blood; symptomatic retroperitoneal, intracranial, intraocular, or intraspinal bleeding; and bleeding requiring treatment cessation and/or operation/hospitalization. Minor bleeding events excluded the events meeting the definition of major bleeding and included wound bleeding or discharge, spontaneous skin hematomas, spontaneous nose bleeding, spontaneous macroscopic hematuria, or blood in stools.
Statistical analysis
Demographic and clinical data were compared between TKA and THA patients as well as between patients taking enoxaparin and patients taking dabigatran after discharge using Pearson’s chi-squared/Fisher’s exact tests and independent samples Student’s t-test for categorical and continuous variables, respectively.
The total cumulative incidence of VTE, major bleeding events, and minor bleeding events after discharge were reported according to thromboprophylaxis and the joint replaced. Differences between groups were measured using absolute risk differences (ARD) with 95% CIs and Pearson’s chi-squared/Fisher’s exact tests. Statistical significance was declared when p≤0.05. All statistical analyses were completed using SPSS statistics software, version 23.0 (IBM Corporation, Armonyk, NY, USA, 2015).
Results
Patients
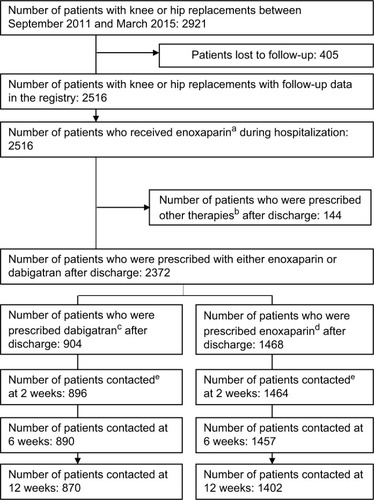
Between 2011 and 2015, 2921 patients underwent TKA or THA in our institution, with data on 2516 (86.1%) patients gathered in the registry. All 2516 received a regimen of enoxaparin thromboprophylaxis during inpatient stay. After discharge, 58.3% (n=1468) were prescribed subcutaneous enoxaparin, 35.9% (n=904) were prescribed oral dabigatran etexilate, and 5.7% (n=144) of patients were prescribed other treatments (warfarin, rivaroxaban, apixaban). After discharge, 1402 (95.5%) patients receiving enoxaparin and 870 (96.2%) receiving dabigatran were retained throughout the entire follow-up period (). During inpatient stay, 35 VTEs (30 proximal DVT, 5 distal DVT, 23 DVT that evolved to a PE) were reported. These patients were prescribed therapeutic warfarin dosage. There was a higher number of VTEs in TKA (n=31) patients than in THA patients (n=4; p<0.01).
Figure 1 Flow diagram of the registry.
Abbreviations: BID, twice daily; DIE, once daily.
Baseline characteristics
shows the characteristics of the entire cohort and those specific to the joint replaced. Overall, the mean age was 66 years and 60% of patients were female. Almost 90% of procedures were unilateral. A twice-daily dose of 30 or 40 mg once daily (mostly for THA) was equally prescribed among patients treated with enoxaparin, whereas most patients (83%) prescribed with dabigatran had a 220 mg dose once daily. TKA patients were older, with more female patients than THA patients, and there were more bilateral knee replacements than bilateral hip replacements. The number of postoperative transfusions was higher in TKA patients than in THA patients, with a total of 6% of all patients needing a transfusion. Overall, 26 deep infections (1.1%) necessitating debridement and washout were reported over 12 weeks, mostly in TKA patients (20/26 [76.9%]).
Table 1 Patient characteristics specific to the joint replaced
Patient characteristics, according to thromboprophylaxis, are presented in . Patients prescribed enoxaparin after discharge were older, and ~60% of patients on either treatment regimen underwent a knee replacement. In both treatment expositions, the proportion of patients prescribed thromboprophylaxis for 35 days averaged 80%, the rest of treatment lengths neighboring 14 days. Almost 6% of patients reported previous DVT history and <1% reported previous PE history in both groups. The number of transfusions did not differ between treatments, but the number of deep infections was significantly higher in patients taking dabigatran (16/26). Regarding treatment lengths, there was no statistically significant differences in age, gender, whether the patient had a TKA or a THA and whether the patient was prescribed enoxaparin or dabigatran after discharge. There was a higher number of total symptomatic VTEs in patients treated for 35 days (n=7) than in those treated for 14 days (n=5, p=0.002), but no significant differences for subtypes of VTEs and major/minor bleeding events.
Table 2 Patient characteristics according to thromboprophylaxis after discharge
Primary outcomes
During the 12 weeks post-discharge follow-up, the total incidence of symptomatic VTE was 0.7% (). These results were distributed as follows: 12 VTE (4 PE) at 2 weeks (0.53%), 3 VTE (2 PE) at 6 weeks (0.13%), and 1 VTE (1 PE) at 12 weeks (0.04%), with no statistical difference between patients taking enoxaparin and dabigatran.
Table 3 Thromboprophylaxis efficacy and safety outcomes for patients prescribed dabigatran or enoxaparin after joint replacement and discharge
One patient taking dabigatran sustained a VTE during the switch window (1 day after discharge, after 4 days of inpatient stay). This patient was a 72-year-old female who had undergone a TKA, with no history of VTE.
Mean time from surgery to post-discharge symptomatic VTE was 20.4 days, ranging from 5 to 84 days, with a mean time of 27.7 days for the dabigatran group and 14.7 days for the enoxaparin group. Mean time from surgery to post-discharge symptomatic VTE was 17.7 days for the TKA group and 23.9 days for the THA group. Mean time from surgery to post-discharge PE was 29.7 days, ranging from 9 to 84 days, with a mean time of 42.3 days for the dabigatran group and 20.3 days for the enoxaparin group. Mean time from surgery to post-discharge symptomatic PE was 36.7 days for the TKA group and 24.5 days for the THA group. No patient died. A PE was reported 110 days after surgery during a retrospective telephone follow-up for a patient who was not reached at 12 weeks (an 81-year-old woman anticoagulated for 35 days with dabigatran after discharge). This patient was not included in the 12-week follow-up analysis.
shows the primary and secondary outcomes for TKA and THA patients. There was no significant difference between knee and hip replacements in VTE incidence after hospital discharge.
Table 4 Thromboprophylaxis efficacy and safety outcomes after joint replacement and discharge between knee and hip replacements
Secondary outcomes
Major bleeding
During the follow-up period, the total incidence of major bleeding events was 0.3% (). There was a statistically significant increase in the number of major bleeding events in the dabigatran group (5 patients), compared to the enoxaparin group (1 patient). Among those taking dabigatran after discharge who suffered major bleeding, 2 were hospitalized 10 and 16 days after the arthroplasty for a hematoma related to dabigatran use. One of the patients that received dabigatran after discharge was hospitalized 10 days after joint replacement surgery for important vomiting and diarrhea with melena (dark black feces). Dabigatran was ceased during this second inpatient stay. Another one was hospitalized for digestive hemorrhage secondary to dabigatran use (16 days postoperatively), and the last one had to cease taking dabigatran because of significant wound bleeding 14 days after surgery (outpatient clinic). In the enoxaparin group, the only major bleeding event was that of a patient seen at the outpatient clinic 14 days after surgery with significant wound bleeding, where enoxaparin was ceased. There was no significant difference in the number of major bleeding events between TKA and THA patients ().
Minor bleeding
During the follow-up period, the total incidence of minor bleeding events was 30.3% (). The incidence of minor bleeding events was statistically significantly higher in patients taking dabigatran etexilate (33.1%) than in patients taking enoxaparin (28.5%). According to the ARD, for every 100 patients treated with dabigatran, 5 patients sustained a minor bleeding event compared to patients treated with enoxaparin. This association was more specific to hematuria and blood in stools. The most common minor bleeding events were hematomas and wound bleeding which generally occurred at 2 weeks after surgery (27%). The incidence of minor bleeding events was higher in patients with knee replacements than in patients with hip replacements, specifically for hematomas and wound bleeding ().
Discussion
These results show that thromboprophylaxis after joint arthroplasty, using subcutaneous enoxaparin or oral dabigatran etexilate, limited symptomatic VTE incidence after discharge to 0.7%. One DVT was reported during the switch window from enoxaparin to dabigatran after discharge. The overall incidence of major bleeding events post-discharge was of 0.3% and was higher in patients taking dabigatran, although the total number of events remained low. There was also a higher number of minor bleeding events in patients taking dabigatran compared to patients taking enoxaparin after discharge.
During hospitalization, the VTE incidence rates of 2.2% after TKA and 0.4% after THA were similar to data reported in RCTs and observational studies (patients taking enoxaparin). There were also 8 (0.3%) potential critical bleeding events reported during inpatient stay. A meta-analysis of 47 studies performed by Januel et al reported that the pooled incidence rates of VTE for patients treated with LMWH were 1.4% (95% CI: 1.0%–1.8%) in TKA studies and 0.6% (95% CI: 0.4%–0.8%) in THA studies.Citation24 VTE incidence after TKA was slightly higher in our registry, which could be explained by the inclusion of subsegmental PE in the efficacy outcome. Their meta-analysis also noted that the incidence rates of VTE in patients undergoing TKA are significantly heterogeneous.
Regarding the primary effectiveness and safety outcomes, our study shows that there was no statistically significant difference between treatment groups in VTE incidence during the follow-up period. Our findings were consistent with those observed in 3 prospective Phase III RCTs comparing the efficacy and safety of dabigatran to enoxaparin in THA patients (RE-NOVATE) and TKA patients (RE-MOBILIZE and RE-MODEL).Citation7,Citation19,Citation20 Pooled analysis of the 3 trials by Friedman et al demonstrated that dabigatran (220 or 150 mg) was equivalent to enoxaparin in decreasing the risk of major VTE and VTE-related mortality, as well as in terms of safety, given that each treatment had a similar bleeding profile.Citation25
The switch period between enoxaparin and dabigatran could have led to 1 DVT event among the 904 patients in our study (0.1%). Ozler et al also compared switch-therapy modalities from enoxaparin to rivaroxaban or dabigatran, to an enoxaparin monotherapy for thromboprophylaxis, after THA and TKA, and found no DVT.Citation26 Two other studies evaluated the outcomes of a VTE protocol when switching from LMWH to dabigatran, which showed promising results.Citation27,Citation28 However, all these studies had insufficient number of patients to extrapolate their findings to the general population, as opposed to this study, given the size of our patient sample.
The main reason for comparing a treatment switch instead of a dabigatran monotherapy to an enoxaparin monotherapy was that dabigatran was not included in the hospital thromboprophylaxis algorithm. Thus, patients who wanted to take the oral treatment were only able to do so after discharge. The choice of dabigatran over rivaroxaban was motivated by the higher incidence of bleeding complications and wound infections associated with the latterCitation4 and the convenience of dabigatran over LMWH for the patient in an outpatient setting. However, the increase in major and minor bleeding events (hematuria/blood in stools), which could possibly influence the infection rate, has to be investigated and considered before further use of this oral anticoagulant for thromboprophylaxis after THA and TKA.
The total incidence of major bleeding events after discharge was 0.3% and was significantly higher in patients taking dabigatran than in patients taking enoxaparin (the risk of major bleeding event was 0.5% higher when dabigatran was received rather than enoxaparin). Pedersen et al found a 0.6% risk of readmission for major bleeding 3 months postoperatively in a cohort of >83,000 patients undergoing knee or hip replacements, where most patients used heparin as thromboprophylaxis. Their definition of major bleeding included intracranial bleeding, gastrointestinal bleeding, and urinary or pulmonary bleeding.Citation29 RCTs comparing the therapies of interest did not report a difference in major bleeding event rates.Citation25 A recent Cochrane review also reported a nonsignificant difference between the use of direct oral anticoagulants and heparin (odds ratio =1.11, 95% CI: 0.79–1.54).Citation30 Consistent with the results of the previously mentioned studies, we did not find a difference in incidence of major bleeding events between TKA and THA patients. Therefore, our findings could be attributed to the study period chosen, the 3 months following surgery excluding inpatient stay, regardless of the length of treatment. In other studies, only the postoperative period was considered. Of our 2372 studied patients, 8 reported a major bleeding event during inpatient stay (n=2 were prescribed dabigatran after discharge, n=6 continued enoxaparin after discharge). If we add these results with those of the follow-up, we obtain the following ARD: −0.30 for 100 patients (95% CI: −0.97 to 0.36), similar to those of other studies. Nevertheless, the reported increase of major bleeding events during follow-up could indicate a risk when using dabigatran for extended prophylaxis.
Minor bleeding post-discharge, although defined according to the same guidelines or as not fulfilling the criteria for major or clinically significant bleeding events,Citation17,Citation31,Citation32 had a high incidence in this study (33.1% for dabigatran and 28.5% for enoxaparin) compared to that observed in other studies and in RCTs. This can be attributed to the high incidence of hematomas (22.9%) reported by patients, independently of their size and location. Indeed, except for the 2- and 6-week assessments when a majority of patients were met at the outpatient clinic or health community service center for a follow-up, most of the assessments were done over the phone. Despite nurses describing as thoroughly as possible injuries and symptoms, there was a high risk for patients to confuse a hematoma and an ecchymosis. Thus, this patient-reported outcome could be biased and overestimated. Our results show that dabigatran was associated with a significant increase in minor bleeding events, especially at 2 weeks after the surgery, where hematuria or blood in stools subtype of event was statistically significant for this group. Bloch et al found that the use of dabigatran led to an increase in wound leakage after total joint replacement, which resulted in a longer hospital stay.Citation33 In another study comparing minor bleeding events when using either dabigatran or enoxaparin, a significant increase in serous discharge was found in the dabigatran group. Thus, delayed administration of dabigatran may prevent some wound leakage, but can still increase the risk of minor bleeding events compared to LMWH therapy.Citation17
The main strength of this study was the minimal loss to follow-up, difficult to achieve given the size of our patient sample, which reduced the risk of selection bias. Nonetheless, there are several limitations to consider. As the risk for major bleeding events and VTEs is higher during the early postoperative period,Citation3 and patients with VTE events during hospitalization were excluded, it should be noted that the risk for VTEs or major bleeding events over 3 months of follow-up is probably lower for this sample, which can impact external validity by underestimating risk. Generalizability is also compromised by the fact that most patients on dabigatran had private insurance. Furthermore, the treatment period was not clearly defined within the follow-up period. Thus, there was no distinction between VTEs and bleeding events that occurred during or after the treatment period. It would also have been relevant to check compliance between the treatment groups, given that oral anticoagulants are associated with better compliance. Although symptomatic VTE and PE were all included in the registry, it is possible that asymptomatic minor VTEs were not detected, leading to an underestimation of risk. Using patient-reported outcomes implies a possibility for information bias. Finally, this is a registry-based observational study limited by the possibility of confounding variables because of a lack of randomization.
Conclusion
We found a low incidence of VTE and major bleeding events after using either subcutaneous enoxaparin or oral dabigatran etexilate after inpatient stay for joint replacement. However, dabigatran was associated with a significant increase in major and minor bleeding events. Switching treatment from LMWH to oral anticoagulants is a safe way to achieve appropriate thromboprophylaxis after joint replacement surgery discharge.
Acknowledgments
The authors would like to thank Ms. Kathleen Beaumont for her help with language format.
Disclosure
The authors report no conflicts of interest in this work.
References
- GeertsWHBergqvistDPineoGFPrevention of venous thromboembolism: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition).Chest20081336 Suppl381s453s18574271
- Markovic-DenicLZivkovicKLesicABumbasirevicVDubljanin-RaspopovicEBumbasirevicMRisk factors and distribution of symptomatic venous thromboembolism in total hip and knee replacements: prospective studyIn Orthop201236612991305
- Falck-YtterYFrancisCWJohansonNAPrevention of VTE in orthopedic surgery patients: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice GuidelinesChest20121412 Supple278S325S22315265
- JamesonSSBottleAMalviyaAMullerSDReedMRThe impact of national guidelines for the prophylaxis of venous thromboembolism on the complications of arthroplasty of the lower limbJ Bone Joint Surg Br201092112312920044690
- GuyattGHAklEACrowtherMGuttermanDDSchuunemannHJExecutive summary: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice GuidelinesChest20121412 Suppl7s47s22315257
- DahlOEGudmundsenTEPrippAHAanesenJJClinical venous thromboembolism following joint surgery: effect of extended thromboprophylaxis on its annual frequency and postoperative pattern over 22 yearsClin Appl Thromb Hemost201420211712324113492
- ErikssonBIDahlOERosencherNOral dabigatran etexilate vs. subcutaneous enoxaparin for the prevention of venous thromboembolism after total knee replacement: the RE-MODEL randomized trialJ Thromb Haemost20075112178218517764540
- WarwickDFriedmanRJAgnelliGInsufficient duration of venous thromboembolism prophylaxis after total hip or knee replacement when compared with the time course of thromboembolic events: findings from the Global Orthopaedic RegistryJ Bone Joint Surg Br200789679980717613508
- WarwickDPrevention of venous thromboembolism in total knee and hip replacementCirculation2012125172151215522547755
- LiebermanJRHeckmannNVenous thromboembolism prophylaxis in total hip arthroplasty and total knee arthroplasty patients: from guidelines to practiceJ Am Acad Orthop Surg2017251278979829176502
- GuyattGWalterSNormanGMeasuring change over time: assessing the usefulness of evaluative instrumentsJ Chronic Dis19874021711783818871
- HullRDPineoGFFrancisCLow-molecular-weight heparin prophylaxis using dalteparin extended out-of-hospital vs. in-hospital warfarin/out-of-hospital placebo in hip arthroplasty patients: a double-blind, randomized comparison. North American Fragmin Trial InvestigatorsArch Intern Med2000160142208221510904465
- MuntzJThromboprophylaxis in orthopedic surgery: how long is long enough?Am J Orthop (Belle Mead, NJ)200938839440119809604
- FriedmanRJGallusAGil-GarayEFitzGeraldGCushnerFPractice patterns in the use of venous thromboembolism prophylaxis after total joint arthroplasty–insights from the Multinational Global Orthopaedic Registry (GLORY)Am J Orthop (Belle Mead, NJ)2010399 Suppl142121290027
- WilkeTPatient preferences for an oral anticoagulant after major orthopedic surgery: results of a german surveyPatient200921394922273058
- FisherWDImpact of venous thromboembolism on clinical management and therapy after hip and knee arthroplastyCan J Surg201154534435121774881
- GombarCHorvathGGalityHSisakKTothKComparison of minor bleeding complications using dabigatran or enoxaparin after cemented total hip arthroplastyArch Orthop Trauma Surg2014134444945724488447
- FanolaCLCurrent and emerging strategies in the management of venous thromboembolism: benefit-risk assessment of dabigatranVasc Health Risk Manag20151127128226064057
- ErikssonBIDahlOEHuoMHOral dabigatran versus enoxaparin for thromboprophylaxis after primary total hip arthroplasty (RE-NOVATE II*). A randomised, double-blind, non-inferiority trialThromb Haemost2011105472172921225098
- GinsbergJSDavidsonBLCompPCOral thrombin inhibitor dabigatran etexilate vs. North American enoxaparin regimen for prevention of venous thromboembolism after knee arthroplasty surgeryJ Arthroplasty200924119
- Boehringer Ingelheim Canada LtdPradaxa product monograph. Dabigatran etexilate capsules2016 Available from: https://www.boehringer-ingelheim.ca/sites/ca/files/documents/pradaxapmen.pdfAccessed June 15, 2017
- Sanofi-aventis Canada IncLovenox product monograph. Enoxaparin sodium solution for injection2013 Available from: http://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.592.7577&rep=rep1&type=pdfAccessed June 15, 2017
- The European Agency for the Evaluation of Medicinal ProductsGuideline on clinical investigation of medicinal products for prophylaxis of high intra- and post-operative venous thromboembolic risk2007 Available from: http://www.ema.europa.eu/docs/en_GB/document_library/Scientific_guideline/2013/05/WC500143764.pdfAccessed June 15, 2017
- JanuelJMChenGRuffieuxCSymptomatic in-hospital deep vein thrombosis and pulmonary embolism following hip and knee arthroplasty among patients receiving recommended prophylaxis: a systematic reviewJAMA2012307329430322253396
- FriedmanRJDahlOERosencherNDabigatran versus enoxaparin for prevention of venous thromboembolism after hip or knee arthroplasty: a pooled analysis of three trialsThromb Res2010126317518220434759
- OzlerTUlucayCOnalAAltintasFComparison of switch-therapy modalities (enoxaparin to rivaroxaban/dabigatran) and enoxaparin monotherapy after hip and knee replacementActa Orthop Traumat Turc2015493255259
- SubramanianPKantharubanSShilstonSPearceOJA 12 month review of a modified protocol using low dose Dabigatran Etexilate in postoperative thromboembolic prophylaxis in joint replacement surgeryThromb J20121011422916689
- WurnigCClemensARauscherHSafety and efficacy of switching from low molecular weight heparin to dabigatran in patients undergoing elective total hip or knee replacement surgeryThromb J2015133726612979
- PedersenABMehnertFSorensenHTEmmeluthCOvergaardSJohnsenSPThe risk of venous thromboembolism, myocardial infarction, stroke, major bleeding and death in patients undergoing total hip and knee replacement: a 15-year retrospective cohort study of routine clinical practiceBone Joint J201496-b447948524692614
- ForsterRStewartMAnticoagulants (extended duration) for prevention of venous thromboembolism following total hip or knee replacement or hip fracture repairCochrane Database Syst Rev20163CD00417927027384
- ErikssonBIDahlOERosencherNOral dabigatran etexilate versus enoxaparin for venous thromboembolism prevention after total hip arthroplasty: pooled analysis of two phase 3 randomized trialsThromb J2015133626578849
- RosencherNSamamaCMFeuringMDabigatran etexilate for thromboprophylaxis in over 5000 hip or knee replacement patients in a real-world clinical settingThromb J201614827042163
- BlochBVPatelVBestAJThromboprophylaxis with dabigatran leads to an increased incidence of wound leakage and an increased length of stay after total joint replacementBone Joint J201496-b1122126