
Abstract
Poor adherence to statin therapy is linked to significantly increased risk of cardiovascular events and death. Unfortunately, adherence to statins is far from optimal. This is an alarming concern for patients prescribed potentially life-saving cholesterol-lowering medication, especially for those at high risk of cardiovascular events. Research on statin adherence has only recently garnered broader attention; hence, major reasons unique to adherence to statin therapy need to be identified as well as suggestions for countermeasures. An integrated approach to minimizing barriers and enhancing facilitation at the levels of the patient, provider, and health system can help address adherence issues. Health care professionals including physicians, pharmacists, and nurses have an obligation to improve patient adherence, as routine care. In order to achieve sustained results, a multifaceted approach is indispensable.
Nonadherence to statin therapy: a growing concern in prevention of cardiovascular disease
Cardiovascular disease (CVD) is the number one cause of death globally. About 17.7 million people died from CVD in 2015, representing 31% of global mortality.Citation1 Of these deaths, coronary heart disease (CHD) and stroke contributed to 7.4 and 6.7 million deaths, respectively.Citation1
High cholesterol, especially elevated low-density lipoprotein cholesterol (LDL-C) levels, increases the risk of heart disease and stroke.Citation2–Citation5 Globally, a third of ischemic heart disease is attributable to high cholesterol and responsible for 2.6 million deaths a year.Citation6
More than three-quarters of deaths due to CVD occur in low- and middle-income countries.Citation1 It is predicted that CVD will be responsible for even more deaths in the developing world than the current common causes of diseases added together and will continue to dominate mortality trends in the foreseeable future.Citation7–Citation9 Increased incidence and prevalence of CVD has seen an upsurge of health care expenditures in many countries due to rising number of patients and costs of preventive measures and treatment.Citation8
The improved awareness and management of cardiovascular risk factors has resulted in a 50% decrease in deaths from CHD over the past 30 years.Citation10 Medical advances in the past decade, particularly the introduction of potent statins such as atorvastatin and rosuvastatin, have made achieving lower LDL-C levels within reach for most individuals at risk of CVD.Citation11 However, more and more patients are not at LDL-C target; nonadherence to medicines is said to be responsible for the failure to achieve, but more importantly, to retain LDL-C targets.Citation11 This prioritizes the need to identify problems with adherence in a clinical context.
Adherence to prescribed medicines predicts outcomes, and better outcomes significantly lower associated health care costs.Citation12–Citation14 In a cohort study of 59,000 new statin users in the Netherlands, compliance with statin therapy for at least 2 years was associated with a 30% reduction in risk of hospitalization for acute myocardial infarction with an increase in protective effect with higher doses.
Likewise, a systematic review of 19 studies reported a relative risk of statin discontinuation ranging from 1.22 to 5.26 for CVD and 1.25 to 2.54 for death.Citation15 Another retrospective cohort study conducted in >229,000 patients reported a direct association between survival and adherence to statin therapy.Citation13 Current estimates suggest that statin nonadherence generates US $44 billion extra, but avoidable, health care costs in the USA.Citation16
Despite the evidence of improved outcomes, adherence to guideline-recommended statin therapy is suboptimal, and almost 80% of high-risk patients do not reach guideline-recommend LDL-C targets.Citation8,Citation17,Citation18 Two key issues appear to be at play. First is the lack of high-intensity statin prescriptions in the appropriate dosage by physicians starting treatment,Citation19 resulting in a significant proportion of un(der)treated high-risk patients.Citation18 Second is the under-use of statins by patients.Citation20 A recent real-world evidence study assessing the effectiveness of lipid-lowering therapy on LDL-C in high CVD risk patients in a primary care setting in Italy found only 61% adherent to therapy 3 months after the initial statin prescription, and barely 55% were adherent after 6 months.Citation21 Approximately 50% of patients with CVD and/or its major risk factors demonstrate poor adherence to their prescribed medicines.Citation22 Even in the immediate period following acute coronary events, adherence is not optimal.Citation23 In a cohort study using linked population-based data from Ontario, 60% of patients with post-acute coronary syndrome (N=22,379) discontinued their statin therapy within 2 years of hospitalization.Citation24
For a treatment with such well-documented CVD morbidity and mortality benefits, these rates are strikingly low.Citation25 Novel methods to help patients improve their adherence to existing evidence-based cardiovascular drug therapies have a powerful potential to improve patient outcomes and reduce associated health care expenditure.Citation23
Role of statins in the prevention of CVD
Standard of care
Since their introduction in 1987, statins have been considered one of the key interventions associated with the decline of cardiovascular morbidity and mortality.Citation25 By lowering LDL-C, statins have significantly decreased cardiovascular events in both primary and secondary CVD prevention trials.Citation14 Statins also help stabilize arterial plaques present in the blood vessels of the brain and heart, reducing the risk of stroke and CHD-related events.Citation26
The use of statins has increased as a result of expanding indications, guidelines emphasizing intensification of LDL-C lowering goals, rising number of generics, as well as recommendations on earlier screening and treatment.Citation14 Clearly, statins have now become the universally accepted standard of atherosclerotic cardiovascular disease care, to the extent that clinical trials of new lipid-lowering drugs are being conducted as add-ons to statins rather than as novel stand-alone therapies.Citation14,Citation27
The benefits of statin therapy observed in randomized clinical trials can only be realized if patients adhere to the prescribed treatment regimens.Citation14 For those who discontinue statin treatment, the number needed to harm (NNH) based on mortality is 1 excess death for every 83 patients.Citation25 The NNH with reference to CVD is 59 per year.Citation25
Medicine-related adverse events
Statins are generally very well tolerated with three major documented side effects linked to their use. Serious adverse events (AEs) associated with statin therapy include myopathy, new-onset diabetes mellitus (NODM), and hemorrhagic stroke.Citation28 Five cases of myopathy may be seen when 10,000 patients are treated for 5 years with statins as recommended by guidelines; 50–100 new cases of diabetes or 5–10 cases of hemorrhagic strokes may result as well.Citation28
Statin-associated muscle symptoms
Statin-associated muscle symptoms (SAMS) can be myalgia, myopathy, or rhabdomyolysis (). Rhabdomyolysis is the most severe manifestation and can lead to further complications such as renal failure.Citation28,Citation29 In very rare cases, an autoimmune myopathy develops in patients treated with statins; this autoimmune disorder is characterized by muscle symptoms, evidence of muscle-cell necrosis on biopsy, and the presence of autoantibodies against 3-hydroxy-3-methylglutaryl coenzyme A (HMG-CoA) reductase. This is estimated to occur in ~2 or 3 of every 100,000 patients treated with statins.Citation30 In most cases, patients exhibit only mild-to-moderate muscle weakness. Some patients may have progressive weakness that may require immunosuppressive therapy ().Citation30 If creatinine kinase levels persist ≥10 times the upper limit of normal for 8 weeks after discontinuation of the statin or if symptoms progress after statin discontinuation, autoantibodies for HMG-CoA reductase should be tested.Citation31
Table 1 Classification of SAMS
The development of SAMS does not always suggest intolerance to statins. Not all reported muscle complaints are caused by statins per se. With aging, muscular-skeletal pathology can manifest and be misinterpreted as statin related.Citation32 Some patients are able to tolerate SAMS at a lower dose, with a longer dosing interval, or with an alternative statin.Citation33 Rechallenged patients who discontinued statin therapy as a result of reported statin-associated effects were able to tolerate statins for a long term.Citation34 It is therefore vital for health providers to determine if an individual is truly intolerant to statins or not.
New-onset diabetes mellitus
There is a reported 10%–12% increase in NODM among patients receiving statins; this risk increases with more intensive treatment and in patients with prediabetes.Citation35 Earlier and more persistent use of high-dose, high-intensity statins appears to correlate with a greater increase in the risk of NODM. This, however, is offset by the proportionally larger reduction in cardiovascular events and death.Citation36
Statins are prescribed on the basis of CVD risk and individual patient characteristics; diet and lifestyle interventions should be emphasized to help mitigate the risk of NODM.Citation35 For instance, weight control has been recommended to prevent statin-related NODM.Citation36
Hemorrhagic stroke
In observational studies, blood cholesterol concentrations have been negatively associated with rates of hemorrhagic stroke.Citation28 Conversely, in a meta-analyses of large statin trials, no increased risk of intracerebral hemorrhage (ICH) was found, most likely as a consequence of a low absolute risk of ICH.Citation37 Based on the SPARCL trial, an increased risk of ICH may only be associated with elderly patients who have a history of ICH and poorly controlled hypertension particularly while using high-dose statins.Citation38
Acute memory loss has also been reported with the use of statins. However, these findings have been inconsistent, and studies of long-term statin use have found either improved memory or no effect.Citation28,Citation39
Statin intolerance
Statin intolerance can be defined as the occurrence of muscle symptoms or other AEs that lead to the discontinuation of statin therapy.Citation40 Although muscle-related AEs may occur with statins, “true” statin intolerance is uncommon.Citation41 Statin intolerance may prevent a large proportion of patients from continuing statin therapy for a long term. Placebo-controlled randomized trials show that most AEs that are attributed to statin therapy in routine practice are not actually caused by it.Citation28 These claims of AEs are based on nonrandomized observational studies and are not supported by the evidence from randomized-controlled trials.Citation29 It is vital, but challenging, to differentiate between individuals who are truly intolerant to statins and those who can actually tolerate them.Citation40 This is because management of “true” statin intolerance requires a totally different approach. “True” statin intolerance is suggested if a patient has unacceptable muscle-related symptoms that resolve with discontinuation of therapy and occur with rechallenge on at least two to three statins and one of which is prescribed at the lowest approved dose.Citation41 Most guidelines recommend restarting at a lower dose and/or a different statin (maximally tolerated statin dose) after symptoms subside combined with non-statin lipid-lowering therapies to attain recommended LDL targets.Citation42–Citation44 In 2017, the Expert Consensus Decision Pathway writing committee of the American College of Cardiology (ACC) provided updated recommendations on the use of non-statins. Addition of a non-statin cholesterol-lowering therapy (either ezetimibe or a proprotein convertase subtilisin/kexin 9 [PCSK9] inhibitor) is recommended for high-risk patients who are statin intolerant. Bile acid sequestrants are recommended only in patients intolerant to ezetimibe.Citation41
The lipid-lowering capability of the two recommended non-statin medications, ezetimibe and evolocumab (a PCSK9 inhibitor), was compared in the GAUSS-3 (Goal Achievement After Utilizing an Anti-PCSK9 Antibody in Statin Intolerant Subjects 3) trial in patients with documented clinical statin intolerance.Citation45 Evolocumab resulted in significantly greater reduction in LDL-C after 24 weeks compared with ezetimibe. Subcutaneously administered PCSK9 inhibitors have demonstrated marked reduction in LDL-C both as a monotherapy and when combined with statin and/or ezetimibe therapy.Citation46 National Lipid Association 2017 Expert Panel on treatment with PCSK9 inhibitors recommend these agents in selected very-high-risk statin-intolerant patients.Citation46 A recent meta-analysis has also concluded their efficacy, safety, and tolerability in statin-intolerant patients.Citation47
However, there are several arguments against treating statin-intolerant patients with PCSK9 inhibitors.Citation48 First, PCSK9 inhibitors are not approved for this indication.Citation48 Second, these agents do not have successful long-term outcomes like statins yet. Third, some statin-intolerant patients still may report muscle-related adverse effects as seen in GAUSS-3 trial, and lastly, they are very expensive, and pharmacoeconomic analysis is required to identify patient sub-groups where “value for money” can be clearly demonstrated.Citation45
Hence, it is vital for physicians to ensure that their patients are aware of the possible statin-associated side effects when prescribing the medicine. This should be done without raising any unnecessary negative expectations and at the same time encouraging patients’ understanding of benefits of statin treatment to promote adherence to therapy.Citation33
Interracial variation and statin intolerance
It has been reported that Asians respond differently to statins than Western populations.Citation49 Several studies have demonstrated an increased systemic exposure with rosuvastatin in Asians.Citation50–Citation52 Data indicate that polymorphisms in the SLCO1B1 and ABCG2 genes contribute to this difference.Citation49,Citation53,Citation54 However, this phenomenon is not a class effect among other high-intensity statins and should not be seen as a barrier to prescription of higher doses of other statins. No difference has been identified in systemic exposure with atorvastatin between Asians and Caucasians.Citation55 Atorvastatin (10–80 mg) has been found to be equally efficacious and safe in Asian and Western populations.Citation56,Citation57 Therefore, there is no regulatory warning about the dose of atorvastatin in Asians.Citation57
The nocebo response
In patients presenting with only mild myalgia, a nocebo response should be considered.Citation58 A nocebo response refers to the induction or worsening of symptoms induced by patients’ expectations of administered therapies.Citation59 This can affect the outcome of a given therapy in a negative way, similar to how placebo affects outcome in a positive way.Citation60
In a recent study by Gupta et al, AEs reported with atorvastatin therapy during a blinded, randomized, placebo- controlled phase were compared with those during an unblinded, nonrandomized phase when open-labeled treatment with atorvastatin was continued.Citation61 The study found an excess rate of muscle-related AEs when patients and their doctors knew that they were on statin therapy in comparison to when they were blinded.Citation61 These observations should provide assurance to both physicians and patients that most AEs linked with statins do not actually have a causal relationship.Citation61
Patients who commonly experience these adverse reactions (the nocebo response) either challenge their physician about the risks of treatment or simply stop the treatment.Citation58 Although patients do experience statin-associated side effects, the majority of these complaints may represent the nocebo response.Citation25 Physicians should evaluate patients’ existing knowledge or perceptions of statin therapy and try to counter the negative perception of exaggerated claims about statin-related side effects.Citation33 With the nocebo response being so prominent, and yet underrecognized in clinical practice, physicians need to be informed on how to detect and handle this effect.Citation62
Why is nonadherence to statins unique?
Cholesterol-lowering medicines as a class are associated primarily with nonadherence.Citation8 Furthermore, adherence to medicines for treatment of a symptomless condition, such as high lipid levels, is a challenge to both doctor and patient.Citation14 It follows that statins may be discontinued at rates higher than for other oral medicines used for chronic therapy. For example, the more frequent screening of blood glucose levels compared with cholesterol levels encourages patients to be more adherent to their diabetic medication than to statins.Citation14
Patients’ beliefs about medicines or how recent the treatment was initiated were also found to be significant predictors of adherence.Citation11 Correspondingly, the nocebo response reflects alterations in human psychobiology (brain, body, and behavior) rather than the effect of the medicine.Citation58 For example, reporting of SAMS can be a consequence of negative media reports about statins or an improper understanding by patients of possible statin-associated adverse effects.Citation33
AEs are cited as the most frequent cause of statin discontinuation.Citation14 In a focus group of 18 participants, nonadherence was primarily due to concerns about experiencing AEs.Citation63 Concerns were raised from information on the Internet, uncertainty about the benefits or importance of statins, the inconvenience of taking a medicine, and obtaining lipid profile tests on a routine basis.Citation63 In general, unfavorable reports found on both social and professional media are a major cause for discontinuation of statin therapy. This is because the AEs of statins are frequently reported and mostly overstated.Citation8 The proliferation of absurd and unscientific but seemingly persuasive criticism of statins on the Internet has created a bad reputation for statins in the public eye.Citation25 Information on the Internet can be made available by anyone with little or no scientific expertise, and usually promotes statin denial, the proposition that cholesterol is not related to heart disease, and statin fear, which is the notion that lowering serum cholesterol levels will cause serious AEs, such as muscle or liver toxicity.Citation25 A study of 6,74,900 patients revealed that early statin discontinuation was associated with negative media attention on statins.Citation64
The adherence problem is exacerbated by hesitation among doctors to discuss and prescribe statins when there are harmful media reports, and compounded by reduced patient compliance as a result of increased awareness of perceived side effects.Citation65 Failure to correct misleading claims about side effects quickly and completely leads patients to stop their statin therapy even though they are at high risk of cardiovascular events.Citation64,Citation66
Predictors for statin nonadherence
The causes of nonadherence are certainly complex and can be broadly classified into three categories: patient related, physician related, and health care system related (). Among these, patient-related factors may be the strongest and may be further differentiated into voluntary and involuntary factors.Citation14 Treatment burden (requirement of daily medication), lack of symptomatic benefit, large time lag to benefit, and perceived or real AEs are perhaps the key causes of nonadherence.
Figure 1 Factors associated with statin nonadherence.
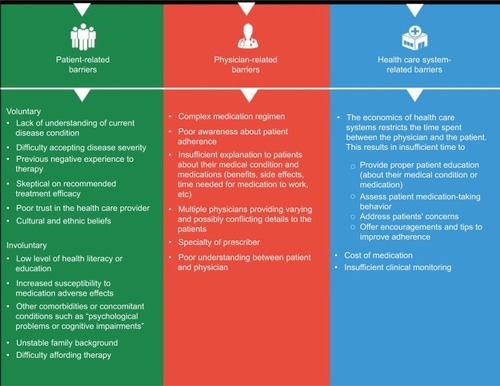
Several factors such as copayment, statin use for either primary or secondary prevention, female gender, age, and belonging to a minority race are also predictive of nonadherence and statin discontinuation. The number of appointments with cardiologists, frequency of LDL tests performed, and the simplicity of the medication regimen are linked with improved statin adherence.Citation20
A meta-analysis showed that age as a predictor of nonadherence follows a U-shaped curve, with the youngest (<50 years) and oldest (≥70 years) showing lower adherence than those in between.Citation14,Citation67,Citation68 Existing comorbidities such as diabetes and hypertension are associated with improved adherence.Citation14 Persistence with statin therapy in older patients declines substantially over time, with the greatest drop occurring in the first 6 months of treatment.Citation68 Forgetfulness is a common reason but there are many factors that can lead up to it, such as insufficient prioritization of the importance of medication intake or simply disliking the need to swallow a pill.Citation14
Overall, nonadherence is influenced by an interaction between various factors, such as patient education, communication between patients and physicians, medication regimen, as well as access to health care.Citation69
Measuring adherence
Adherence is defined as the percentage of pills a patient takes as prescribed. By convention, a cutoff point of 80% is used to categorize adherence to cardiovascular medications into good and poor adherence groups.Citation70 Patients are also categorized as nonadherent if they discontinue a medication before a certain time period. In primary nonadherence, a patient “discontinues” a medication even before filling a prescription once.Citation23
While there is no recognized gold standard method to measure adherence, a combination of direct and indirect methods can be used to get an accurate measurement of adherence in actual practice ().Citation14
Table 2 Measures to quantify medication adherence
Interventions to improve medication-taking behaviors
Generally, about 33% of patients will be adherent to therapy just by being given a prescription and asked to take it by their physicians, while about 15%–25% will be nonadherent despite any intervention.Citation71 Interventions to improve adherence are aimed at the middle 50% of patients who may adhere if given support and encouragement.Citation14
Identifying specific barriers for each patient and adopting suitable techniques to overcome them are necessary to improve medication adherence.Citation22 However, individual interventions, as distinct from a shared responsibility between the clinician and patient, tend to be associated with poor improvements in adherence. Alternatively, multifaceted approaches designed for individual patients are more likely to improve long-term adherence to medication.Citation69
A personalized, patient-focused program involving frequent interactions with a health care professional or a combination of techniques that make use of physician communication and pharmacist involvement have shown to improve medication adherence and ultimately, better health outcomes.Citation72 summarizes various interventions to improve medication adherence.
Figure 2 Interventions for improving medication adherence.
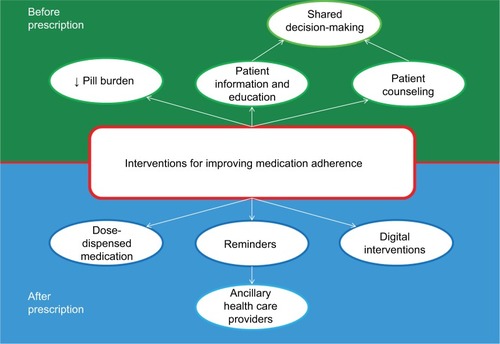
We have not analyzed the cost-effectiveness of individual strategies. Comparing costs of different adherence strategies or technologies would be a relevant topic for a costs- effectiveness analysis, but this is beyond the scope of this review.
Shared decision-making
Current evidence-based clinical guidelines often do not take into account specific individual issues. Values, goals, and preferences need to be taken into account. Clinical decisions should be made based on the concept of “shared decision-making”.Citation73 Providing positive reassurances that the patient is making a good effort to lower risk of a cardiovascular event has neither been assessed nor addressed in existing guidelines.Citation73 Understanding the patient’s apprehensions about therapy is vital to improve adherence. Patient-specific factors such as perceptions about their condition, perceived efficacy of treatment, and other elements that have been associated with nonadherence need to be discussed to avoid poor adherence and adverse treatment outcomes. Health care providers need to come up with an educational strategy, tailored to each patient’s needs.
The development of shared decision-making tools will allow current clinical evidence to be portrayed in simple terms such that it allows physicians to help their patients make appropriate decisions related to medication use.Citation73
Counseling
Strategies such as hospital staff, other than the physician, conducting regular phone counseling on medication adherence, were shown to have an impact on patient survival.Citation74 Data strongly suggest medication adherence can be improved as a result of this method of weekly communication.Citation13 Predictors of nonadherence can also be used to identify those at high risk of statin discontinuation for targeted counseling.Citation14 Recent international guidelines such as those from the “American College of Cardiology/American Heart Association (2013)” and the “European Society of Cardiology (2016)” recommend that physicians, and allied health care professionals, should regularly monitor patients’ adherence to statin therapy.Citation75–Citation77
Patients in whom knowledge and understanding of statins and CVD risk factors were improved, adherence to therapy was better and the number of people reaching their LDL-C goals increased.Citation78 Motivational interviewing techniques can help the patient develop a list of treatment goals.Citation8 Likewise, physicians can also advocate good practices by encouraging patients to set medication reminders, organize medicines in pill boxes, and maintain a medicine tracker sheet to help improve adherence.
Patient information and education
Enhancing communication between physician and patient is crucial to improve patient education and allow patients to clarify and resolve any concerns or misconceptions.Citation79 It is important for physicians to empower patients to become informed medication consumers by educating patients as well as family members about their medical condition and medicines.Citation8 Educational videos, mobile apps, and audio books can help improve knowledge about their conditions.Citation8,Citation80
Suggested topics for patient education can highlight the importance of a medicine’s benefit, for example, long-term benefits in prevention of CVD with statins. Physicians must abandon commonly used fear tactics, as scaring the patient will more likely result in decreased adherence.Citation81 Information about statins (reasons for prescription, benefits, risks, etc.), additional time for discussion with the clinician, and written or trustworthy online information about statin risks, side effects, and drug interactions, can also help improve adherence.Citation14
Education on harmful pseudoscience will also prove useful. Products promoted on the Internet commonly imply benefits that have no evidence from formal clinical studies and could potentially be harmful as well.Citation25 For instance, patients are promised that adhering to a certain diet or taking exotic food supplements can result in a reversal of heart disease. These diets are aggressively promoted to patients as an alternative to statin medication, promising all the benefits without any risk, when in fact there is no scientific basis for these claims.
Reminders
Medication reminders by pharmacists, nurses, or therapists can improve adherence.Citation13 Techniques commonly involve phone calls, SMS texts, mail, and the use of calendar reminders. Telephone reminders when used together with educational materials were shown to be the most effective strategies.Citation16
A Cochrane database review by Schedlbauer et al concluded that “reminding” or “re-enforcement” appeared to be the most promising intervention tactic to improve adherence to lipid-lowering drugs.Citation8,Citation82 In another study, Derose et al investigated statin adherence in 5,216 participants who had discontinued statin use within the previous year and found that the group that received periodic automated telephone calls had a significantly better adherence to statins within the year of the study.Citation83
Dose-dispensed medicine
Overall, the use of various types of pill box did not show any improvement in adherence by patients when compared to usual practices.Citation84 However, this method could be more effective when it is used in combination with other forms of intervention.Citation84 Multiple studies have reported significant improvement in adherence when a drug reminder packaging was used with results being much more distinct when it was part of a multifaceted approach compared with a single-faceted approach.Citation85
Dose-dispensed medicines such as the time-specific blister packs contain the patient’s medication for each time point of the day.Citation86 Patient-specific multidose adherence packs also contain the medications required for a week and are labeled with the day and time of drug administration. Their use maintains the ability for individual choice of drug and dose.Citation13
Evidence suggests that the combination of weekly dose-dispensed blister packs with regular pharmacy counseling on adherence demonstrates an absolute increase in adherence of one-third when compared with the standard prepacked medication in blister cards.Citation13 One study showed that drug reminder packaging significantly reduced the mean hospitalization rate, a more relevant marker of adherence for patients on polypharmacy.Citation85
Reducing pill burden or simplification of the drug regimen
A complex medication regimen and high pill burden can also lead to nonadherence. Careful reduction in the use of unnecessary or unsafe medications, and use of combination and once-daily formulations are effective strategies in managing polypharmacy and reducing pill burden.Citation87 One such strategy is the use of a polypill. Polypills are the combination of multiple classes of preventive medications in one pill. Their use has demonstrated significant improvement in adherence when used instead of usual care in patients with CVD.Citation88 Less-intensive strategies, such as prescribing products that simplify the medication regimen, achieve relatively smaller improvements in compliance.Citation89
Digital interventions
Digital interventions that involve the use of modern technology to develop approaches to improve adherence such as smartphone apps are novel solutions.Citation69 By incorporating physical physician–patient interactions with technology-driven medication adherence reminders, electronic medication reconciliation, and the usage of pharmaceutical databases, adherence to medicines may be improved as well.Citation90 A recent example is the ACC Statin Intolerance App, which was developed to guide physicians how to manage and treat patients who experience muscle symptoms while on statin therapy. Physicians would be able to determine if a patient is really intolerant to their statin medication, follow guidelines in managing and treating muscle symptoms while on statins, and compare between different statin characteristics or any potential drug interactions.Citation91
Upcoming potential digital interventions also include technotherapeutics. Technologies are gradually expanding in the health care arena to capture previously unavailable data and to generate new knowledge about patients.Citation92 The use of new technological devices even allows for previously unavailable data to be recorded on a continuous basis and transmitted via a tiny microchip inserted into the body. This information can then be transmitted to health care professionals.Citation92 They have the potential to track physiological responses and treatment adherence with exact precision. A prompt signal will be transmitted when there is nonadherence to a medication regimen.Citation92 This new technological device may be able to improve the therapeutic management of chronic conditions, maximize clinical outcomes, facilitate communication with health care providers, and individualize patient care.Citation92 Technotherapeutics is, however, expensive and complex. Also, its design has limitations as it places the responsibility of adherence primarily on the patient.
Importance of combined pharmacist and/or nurse participation
Pharmacists are uniquely positioned to interact more frequently with patients than other health care providers. Pharmacists are better able to emphasize proper medication-taking behaviors and address issues about the patient’s medication adherence by using their access to medication refill information.Citation93 By enlisting ancillary health care providers such as pharmacists, additional motivation to patients can be provided.
Some techniques include phone calls, counseling, medication review, home visits, and comprehensive pharmacy care focusing on patient education and the importance of adherence. Another technique can involve the implementation of a reward system by providing positive feedback whenever a treatment goal is attained according to the treatment plan.Citation8 Ultimately, this could even include reduced payments for health insurance schemes.
Based on multiple studies, integration of pharmacist and/or specialized nurse practitioner counseling with a focus on adherence demonstrated the most noteworthy improvements in medication habits.Citation16 The use of specialized nurse practitioners for follow-up has even led to a reduction in LDL-C of about 0.9 mmol/L from baseline.Citation86 Integration of a pharmacy/nurse program is likely to achieve substantial improvements in medication adherence and significant LDL-C reductions.
Conclusion
Nonadherence to statins is exceptionally common and has been undervalued by the majority health care professionals as well as professional organizations responsible for formulating lipid management guidelines. Identifying at-risk patients and initiating treatment remains a priority, but if medication adherence is ignored, this will result in wasted efforts, resources and lives. We have to intensify our efforts to overcome this formidable barrier if our goal is to preserve our patients’ health. We need to empower our patients so they can recognize sham information found on the Internet that promote alternative remedies, created by people with little or no scientific expertise. The only way to address this challenge is allocating time to talk and interact with patients. This can be done by physicians or dedicated hospital staff on an individual basis or in groups. Support from health authorities for educating the public and enlisting media support should complement individualized strategies.
Specific guidelines to improve adherence are urgently needed. Evidence-based interventions to improve adherence are available and should be effectively integrated in patient management. Various health care providers including physicians, pharmacists, and nurses need to collaborate and communicate with patients to address concerns and discuss the risks and benefits of long-term statin therapy. Identification of relevant approaches and techniques by health care providers can improve adherence, but most importantly, physician and patient need to create a trusting alliance; this will promote statin adherence and ultimately reduce morbidity and increase life expectancy.
Author contributions
All authors were involved in conception, design, analysis, and interpretation of data. All authors were also involved in the preparation of the manuscript, revising it for important intellectual content, and final approval before submitting for publication.
Acknowledgments
The authors would like to thank Ms Tanaya Bharatan, Pfizer, for her editorial support for this article.
Disclosure
Dr Zhen-Vin Lee has received honoraria from Aspen, Astra Zeneca, Bayer, Boehringer Ingelheim, Merck Serono, Merck, Sharp & Dohme, and Pfizer. Mr Andre Lee underwent indirect patient care pharmacy training for 3 months at Pfizer, Singapore. Dr Sajita Setia and Dr Kannan Subramaniam are employees of Pfizer. Professor Lansberg has received consultancy and speaker honorarium payments from Pfizer and Sanofi. The authors report no other conflicts of interest in this work.
References
- World Health OrganizationCardiovascular Diseases (CVDs). Fact Sheet2017 Available from: http://www.who.int/mediacentre/fact-sheets/fs317/enAccessed March 22, 2018
- StamlerJWentworthDNeatonJDIs relationship between serum cholesterol and risk of premature death from coronary heart disease continuous and graded? Findings in 356,222 primary screenees of the Multiple Risk Factor Intervention Trial (MRFIT)JAMA198625620282328283773199
- The Lipid Research Clinics Coronary Primary Prevention Trial results. I. Reduction in incidence of coronary heart diseaseJAMA198425133513646361299
- The Lipid Research Clinics Coronary Primary Prevention Trial results. II. The relationship of reduction in incidence of coronary heart disease to cholesterol loweringJAMA198425133653746361300
- PsatyBMAndersonMKronmalRAThe association between lipid levels and the risks of incident myocardial infarction, stroke, and total mortality: the cardiovascular health studyJ Am Geriatr Soc200452101639164715450039
- World Health OrganizationGlobal Health Observatory (GHO) Data: Raised Cholesterol2017 Available from: http://www.who.int/gho/ncd/risk_factors/cholesterol_text/en/Accessed 22 March, 2018
- BeagleholeRBonitaRGlobal public health: a scorecardLancet200837296541988199618945485
- VonbankAAgewallSKjeldsenKPComprehensive efforts to increase adherence to statin therapyEur Heart J201738322473247928077470
- World Health OrganizationWorld Health Statistics 2009 Available from: http://www.who.int/whosis/whostat/2009/en/Accessed March 22, 2018
- FordESAjaniUACroftJBExplaining the decrease in U.S. deaths from coronary disease, 1980–2000N Engl J Med2007356232388239817554120
- BerminghamMHaydenJDawkinsIProspective analysis of LDL-C goal achievement and self-reported medication adherence among statin users in primary careClin Ther20113391180118921840055
- OsterbergLBlaschkeTAdherence to medicationN Engl J Med2005353548749716079372
- LaufsURettig-EwenVBöhmMStrategies to improve drug adherenceEur Heart J201132326426820729544
- ManingatPGordonBRBreslowJLHow do we improve patient compliance and adherence to long-term statin therapy?Curr Atheroscler Rep201315129129123225173
- De VeraMABholeVBurnsLCLacailleDImpact of statin adherence on cardiovascular disease and mortality outcomes: a systematic reviewBr J Clin Pharmacol201478468469825364801
- GatwoodJBaileyJEImproving medication adherence in hypercholesterolemia: challenges and solutionsVasc Health Risk Manag20141061562525395859
- YanATYanRTTanMVascular Protection (VP) and Guidelines Oriented Approach to Lipid Lowering (GOALL) Registries InvestigatorsContemporary management of dyslipidemia in high-risk patients: targets still not metAm J Med2006119867668316887414
- VonbankASaelyCHReinPSturnDDrexelHCurrent cholesterol guidelines and clinical reality: a comparison of two cohorts of coronary artery disease patientsSwiss Med Wkly2013143w1382823832393
- GislasonGHRasmussenJNAbildstrømSZLong-term compliance with beta-blockers, angiotensin-converting enzyme inhibitors, and statins after acute myocardial infarctionEur Heart J200627101153115816399775
- EllisJJEricksonSRStevensonJGBemsteinSJStilesRAFendrickMASuboptimal statin adherence and discontinuation in primary and secondary prevention populations: should we target patients with the most to gain?J Gen Intern Med200419663864515209602
- GuglielmiVBelliaAPecchioliSEffectiveness of adherence to lipid lowering therapy on LDL-cholesterol in patients with very high cardiovascular risk: a real-world evidence study in primary careAtherosclerosis2017263364128599257
- JimmyBJoseJPatient medication adherence: measures in daily practiceOman Med J201126315515922043406
- KronishIMYeSAdherence to cardiovascular medications: lessons learned and future directionsProg Cardiovasc Dis201355659060023621969
- JackeviciusCAMamdaniMTuJVAdherence with statin therapy in elderly patients with and without acute coronary syndromesJAMA2002288446246712132976
- NissenSEStatin denial: an internet-driven cult with deadly consequencesAnn Intern Med2017167428128228738422
- BaigentCKeechAKearneyPMCholesterol Treatment Trialists’ (CTT) CollaboratorsEfficacy and safety of cholesterol-lowering treatment: prospective meta-analysis of data from 90,056 participants in 14 randomised trials of statinsLancet200536694931267127816214597
- StoneNJRobinsonJLichtensteinAHAmerican College of Cardiology/American Heart Association Task Force on Practice Guidelines2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Practice GuidelinesJ Am Coll Cardiol20146325 Pt B2889293424239923
- CollinsRReithCEmbersonJInterpretation of the evidence for the efficacy and safety of statin therapyLancet2016388100592532256127616593
- SathasivamSLeckyBStatin induced myopathyBMJ2008337a228618988647
- MammenALStatin-associated autoimmune myopathyThe N Engl J Med2016374766466926886523
- SweidanAJLeungAKaiserCJA case of statin-associated autoimmune myopathyClin Med Insights Case Rep201710117954761668823128469499
- van der PloegMAPoortvlietRKEvan BlijswijkSCEStatin use and self-reported hindering muscle complaints in older persons: a population based studyPloS One20161112e016685727911918
- Pedro-BotetJRubies-PratJStatin-associated muscle symptoms: beware of the nocebo effectLancet2017389100882445244628476289
- ZhangHPlutzkyJSkentzosSDiscontinuation of statins in routine care settings: a cohort studyAnn Intern Med2013158752653423546564
- BetteridgeDJCarmenaRThe diabetogenic action of statins - mechanisms and clinical implicationsNat Rev Endocrinol20161229911026668119
- WangKLLiuCJChaoTFRisk of new-onset diabetes mellitus versus reduction in cardiovascular events with statin therapyAm J Cardiol2014113463163624360773
- VersmissenJScheeleMDippelDWvan den MeirackerAHSta-tine na een hersenbloeding: is dit veilig?Nederlands tijdschrift voor geneeskunde2015159A856326083841
- MaYLiZChenLLiXBlood lipid levels, statin therapy and the risk of intracerebral hemorrhageLipids Health Dis2016154326932585
- StromBLSchinnarRKarlawishJHennessySTealVBilkerWBStatin therapy and risk of acute memory impairmentJAMA Intern Med201517581399140526054031
- StulcTCeškaRGottoAMStatin intolerance: the clinician’s perspectiveCurr Atheroscler Rep201517126926490078
- Lloyd-JonesDMMorrisPBBallantyneCM2017 Focused Update of the 2016ACCExpert Consensus Decision Pathway on the Role of Non-Statin Therapies for LDL-Cholesterol Lowering in the Management of Atherosclerotic Cardiovascular Disease Risk: a Report of the American College of Cardiology Task Force on Expert Consensus Decision PathwaysJ Am Coll Cardiol201770141785182228886926
- StroesESThompsonPDCorsiniAEuropean Atherosclerosis Society Consensus PanelStatin-associated muscle symptoms: impact on statin therapy-European Atherosclerosis Society Consensus Panel Statement on Assessment, Aetiology and ManagementEur Heart J201536171012102225694464
- ManciniGBTashakkorAYBakerSDiagnosis, prevention, and management of statin adverse effects and intolerance: Canadian Working Group Consensus updateCan J Cardiol201329121553156824267801
- RosensonRSBakerSKJacobsonTAKopeckySLParkerBAThe National Lipid Association’s Muscle Safety Expert PanelAn assessment by the statin muscle safety task force: 2014 updateJ Clin Lipidol201483 SupplS58S7124793443
- NissenSEStroesEDent-AcostaREEfficacy and tolerability of evolocumab vs ezetimibe in patients with muscle-related statin intolerance: the GAUSS-3 randomized clinical trialJAMA2016315151580159027039291
- OrringerCEJacobsonTASaseenJJUpdate on the use of PCSK9 inhibitors in adults: recommendations from an Expert Panel of the National Lipid AssociationJ Clin Lipidol201711488089028532784
- QianLJGaoYZhangYMChuMYaoJXuDTherapeutic efficacy and safety of PCSK9-monoclonal antibodies on familial hypercholesterolemia and statin-intolerant patients: a meta-analysis of 15 randomized controlled trialsSci Rep20177123828331223
- WatersDDHsuePYBangaloreSPCSK9 inhibitors for statin intolerance?JAMA2016315151571157227039138
- NaitoRMiyauchiKDaidaHRacial differences in the cholesterol-lowering effect of statinJ Atheroscler Thromb2017241192527733728
- TzengTBSchneckDWBirminghamBKPopulation pharmacokinetics of rosuvastatin: implications of renal impairment, race, and dyslipidaemiaCurr Med Res Opin20082492575258518674408
- NakamuraHArakawaKItakuraHMEGA Study GroupPrimary prevention of cardiovascular disease with pravastatin in Japan (MEGA Study): a prospective randomised controlled trialLancet200636895421155116317011942
- LeeERyanSBirminghamBRosuvastatin pharmacokinetics and pharmacogenetics in white and Asian subjects residing in the same environmentClin Pharmacol Ther200578433034116198652
- BirminghamBKBujacSRElsbyRRosuvastatin pharmacokinetics and pharmacogenetics in Caucasian and Asian subjects residing in the United StatesEur J Clin Pharmacol201571332934025630984
- LiuJELiuXYChenSSLCO1B1 521T > C polymorphism associated with rosuvastatin-induced myotoxicity in Chinese coronary artery disease patients: a nested case-control studyEur J Clin Phar-macol2017731114091416
- GandelmanKFungGLMessigMLaskeyRSystemic exposure to atorvastatin between Asian and Caucasian subjects: a combined analysis of 22 studiesAm J Ther201219316417320975528
- SetiaSFungSS-WWatersDDDoctors’ knowledge, attitudes, and compliance with 2013 ACC/AHA guidelines for prevention of atherosclerotic cardiovascular disease in SingaporeVasc Health Risk Manag20151130331026082642
- YanPTanEKKChooJCJLiewCFSLauTWatersDDStatin-centric versus low-density lipoprotein-centric approach for atherosclerotic cardiovascular disease prevention: a Singapore perspectiveSingapore Med J201657736036727439304
- TobertJANewmanCBThe nocebo effect in the context of statin intoleranceJ Clin Lipidol201610473974727578103
- HäuserWHansenEEnckPNocebo Phenomena in medicine: their relevance in everyday clinical practiceDtsch Arztebl Int20121092645946522833756
- PlanèsSVillierCMallaretMThe nocebo effect of drugsPharmacol Res Perspect201642e0020827069627
- GuptaAThompsonDWhitehouseAAdverse events associated with unblinded, but not with blinded, statin therapy in the Anglo-Scandinavian Cardiac Outcomes Trial-Lipid-Lowering Arm (ASCOT-LLA): a randomised double-blind placebo-controlled trial and its non-randomised non-blind extension phaseLancet2017389100882473248128476288
- RizosCVElisafMSStatin myopathy: navigating the mazeCurr Med Res Opin201733232732927805428
- FungVSinclairFWangHDaileyDHsuJShaberRPatients’ perspectives on nonadherence to statin therapy: a focus-group studyPerm J2010141410
- NielsenSFNordestgaardBGNegative statin-related news stories decrease statin persistence and increase myocardial infarction and cardiovascular mortality: a nationwide prospective cohort studyEur Heart J2016371190891626643266
- Picker Institute EuropePerceptions of statins: research with patients, GPs and cardiologists 2016 Available from: http://www.picker.org/wp-content/uploads/2016/07/P2941-BHF-Statins_Final-Report_Publication.pdfAccessed March 22, 2018
- MatthewsAHerrettEGasparriniAImpact of statin related media coverage on use of statins: interrupted time series analysis with UK primary care dataBMJ2016353i3283
- MannDMWoodardMMuntnerPFalzonLKronishIPredictors of non-adherence to statins: a systematic review and meta-analysisAnn Pharmacother20104491410142120702755
- BennerJSGlynnRJMogunHNeumannPJWeinsteinMCAvornJLong-term persistence in use of statin therapy in elderly patientsJAMA2002288445546112132975
- TajouriTHDriverSLHolmesDRJr“Take as directed” – strategies to improve adherence to cardiac medicationNat Rev Cardiol201411530430724343567
- KarveSClevesMAHelmMHudsonTJWestDSMartinBCGood and poor adherence: optimal cut-point for adherence measures using administrative claims dataCurr Med Res Opin20092592303231019635045
- Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final reportCirculation2002106253143342112485966
- WoutersHVan DijkLGeersHCUnderstanding statin non-adherence: knowing which perceptions and experiences matter to different patientsPloS One2016111e014627226808151
- BarrettBRiccoJWallaceMKieferDRakelDCommunicating statin evidence to support shared decision-makingBMC Fam Pract2016174127048421
- WuJYLeungWYChangSEffectiveness of telephone counselling by a pharmacist in reducing mortality in patients receiving polypharmacy: randomised controlled trialBMJ2006333756752216916809
- StoneNJRobinsonJGLichtensteinAH2013ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice GuidelinesCirculation201412925 Suppl 2S1S4524222016
- PiepoliMFHoesAWAgewallS2016European Guidelines on cardiovascular disease prevention in clinical practice: the Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts) Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR)Eur Heart J201637292315238127222591
- DeshpandeSQuekRGWForbesCAA systematic review to assess adherence and persistence with statinsCurr Med Res Opin201733476977828076703
- YilmazMBPinarMNaharciIBeing well-informed about statin is associated with continuous adherence and reaching targetsCardiovasc Drugs Ther200519643744016435071
- GawATolmieELindsayGMThe statin breakthrough – remembering to involve the patientCardiovasc Drugs Ther200418534334415717135
- GosseyJTWhitneySNCrouchMAJibaja-WeissMLZhangHVolkRJPromoting knowledge of statins in patients with low health literacy using an audio bookletPatient Prefer Adherence2011539740321949603
- RuddPClinicians and patients with hypertension: unsettled issues about complianceAm Heart J19951303 Pt 15725797661077
- SchedlbauerADaviesPFaheyTInterventions to improve adherence to lipid lowering medicationCochrane Database Syst Rev20103Cd00437120238331
- DeroseSFGreenKMarrettEAutomated outreach to increase primary adherence to cholesterol-lowering medicationsJAMA InternMed201317313843
- ChoudhryNKKrummeAAErcolePMEffect of reminder devices on medication adherence: the REMIND randomized clinical trialJAMA InterMed20171775624631
- BoeniFSpinatschESuterKHersbergerKEArnetIEffect of drug reminder packaging on medication adherence: a systematic review revealing research gapsSyst Rev201432924661495
- HersbergerKEBoeniFArnetIDose-dispensing service as an intervention to improve adherence to polymedicationExpert Rev Clin Pharmacol20136441342123927669
- FarrellBFrench MerkleyVIngarNReducing pill burden and helping with medication awareness to improve adherenceCan Pharm J (Ott)2013146526226924093037
- WebsterRPatelASelakVSPACE CollaborationEffectiveness of fixed dose combination medication (“polypills”) compared with usual care in patients with cardiovascular disease or at high risk: a prospective, individual patient data meta-analysis of 3140 patients in six countriesInt J Cardiol201620514715626736090
- PetrillaAABennerJSBattlemanDSTierceJCHazardEHEvidence-based interventions to improve patient compliance with antihypertensive and lipid-lowering medicationsInt J Clin Pract200559121441145116351677
- GrangerBBBosworthHBMedication adherence: emerging use of technologyCurr Opin Cardiol201126427928721597368
- American College of CardiologyACC Statin Intolerance App2017 Available from: http://www.acc.org/StatinIntoleranceAppAccessed March 22, 2018
- GagnonMJacobJDGutaATreatment adherence redefined: a critical analysis of technotherapeuticsNurs Inq2013201607022381079
- CalvertSBKramerJMAnstromKJKaltenbachLAStaffordJAAllen LaPointeNMPatient-focused intervention to improve long-term adherence to evidence-based medications: a randomized trialAm Heart J20121634657665.e65122520532