Abstract
Background:
Patients with systemic lupus erythematosus (SLE) are 5–8 times more likely to develop coronary heart disease than the general population. The aim of this study was to find out the prevalence of the small dense low-density lipoprotein (LDL) cholesterol particle in patients with SLE.
Methods:
We recruited 50 consecutive patients with SLE who had no evidence of hypertension or renal failure. Fifty age- and gender-matched healthy controls were also recruited. We measured serum lipid levels and LDL particle diameters by gradient gel electrophoresis in both patients and controls.
Results:
Patients with SLE had significant dyslipidemia, characterized by elevated plasma triglycerides, LDL cholesterol, Apoprotein B, triglyceride:high-density (HDL) lipoprotein cholesterol ratio, and decreased plasma concentrations of HDL cholesterol. The LDL particle size in SLE (24.8 ± 1.23 nm) was significantly (P < 0.01) smaller than that in controls (26.1 ± 1.31 nm). The prevalence of the LDL phenotype B (the atherogenic phenotype) was 52% in SLE but only 20% in healthy controls.
Conclusion:
We conclude that the high prevalence of small dense LDL in SLE may contribute to the high incidence of coronary heart disease seen in this disorder.
Introduction
Systemic lupus erythematosus (SLE) is a systemic autoimmune disease characterized by the activation of T and polyclonal B lymphocytes, the production of autoantibodies, and the formation of immune complexes causing tissue and organ damage.Citation1,Citation2 Although its exact etiology is unknown, its clinical consequences can be devastating. For example, in prospective cohorts where incidence cases have been recorded, the prevalence of coronary heart disease in SLE has been 6%–10%Citation3–Citation5 and the estimated incidence of new coronary heart disease events is approximately 1.2%–1.5% per annum. Manzi et alCitation1 utilized data from the Pittsburgh lupus cohort and compared them with data from women followed in the Framingham Offspring study. Overall, women with SLE had a 5–6-fold increased risk of coronary heart disease. Moreover, women with SLE aged 35–44 years were 52 times more likely to develop coronary heart disease. Employing data from the California Discharge Database, WardCitation5 found that women with SLE aged 18–44 years were more likely than aged-matched controls to have myocardial infarction, congestive heart failure, or stroke. Extrapolating from the population prevalence of SLE, Ward estimated that, overall, myocardial infarction, heart failure, and stroke were 8.5, 13.2, and 10.1 times more likely in women with SLE. In a case-control study from the UK General Practice Research Database, Fischer et alCitation6 also reported that patients with SLE were at higher risk of developing coronary heart disease.
The pathogenesis of coronary heart disease in SLE is likely to be multifactorial, and may be related to vasculitis, corticosteroid use, renal disease, hypertension, hyperlipidemia, or thrombosis associated with antiphospholipid antibodies. Patri et alCitation2 reported that patients with SLE were more likely to have a sedentary lifestyle, obesity, and hypercholesterolemia, while Borha et alCitation7,Citation8 found that, compared with controls, patients with SLE had lower high-density lipoprotein (HDL) cholesterol as well as higher very low-density lipoprotein (VLDL) cholesterol, triglycerides, and lipoprotein (a) concentrations. Increased carotid intima thickness, increased plasma concentrations of circulating oxidized LDL and homocysteine, as well as endothelial defects, have all been incriminated in the premature coronary heart disease seen in patients with SLE.Citation9–Citation11
Human plasma low-density lipoproteins (LDL) are a heterogenous collection of particles which vary in buoyant density, size, and lipid and protein composition.Citation12–Citation14 Small-sized LDL cholesterol has been associated with coronary heart disease in some case-control studies,Citation15–Citation18 although other studies have not found this association.Citation19,Citation20
There are only two reports in the literature on LDL particle size in SLE. Using nuclear magnetic resonance to measure LDL particle sizes in patients with SLE, both Chung et alCitation21 and Hua et alCitation22 did not find any differences in small dense LDL particle size between patients with SLE and controls. Therefore, we decided to use a different method to measure LDL particle size in 50 patients with SLE and 50 healthy controls. We measured LDL particle diameters by gradient gel electrophoresis (Quantimatrix Lipoprint™ LDL System, Quantimetrix Corporation, Redondo Beach, CA) in both patients and controls.
Methods and materials
Subjects
Fifty patients (all women) meeting the 1997 revised criteria of the American College of Rheumatology for SLE were recruited from the rheumatology clinic at the Al-Amiri Teaching Hospital in Kuwait over a period of one year from December 2005–December 2006. Inclusion criteria were disease onset at age <18 years and current age >22 years. Exclusion criteria were pregnancy, use of lipid-lowering drugs, current smoking, proteinuria, a plasma creatinine concentration >120 μmol/L, abnormal liver function, and a fasting plasma glucose >6.1 mmol/L. At initial presentation, the disease activity of each patient was assessed by the SLE Disease Activity Index. The patients were then treated with glucocorticoid and/or immunosuppressive agents until they were stable. Fifty age-matched healthy controls (again all women) were also recruited. The controls were matched with the SLE patients for body mass index (BMI). Informed consent was obtained from each participant before the study. The protocol for the study was approved by the local ethics committee.
Collection of blood samples
Following an overnight 12-hour fast (9 pm–9 am), 10 mL of blood was collected in citrated containers from each patient (before and after treatment) and control, and plasma was separated and kept frozen at −80°C until ready for analysis. The following tests were done on plasma samples from patients (before and after treatment) and controls.
Laboratory analysis
Erythrocyte sedimentation rate was measured using a modified Westergren method. Anti-double-stranded DNA antibody levels were measured using a commercial enzyme-linked immunoassay kit (Inova Diagnostics, San Diego, CA). The Beckman LX20 automated analytical system (Beckman-Coulter, Brea, CA) was used to measure glucose by the hexokinase method, total cholesterol and HDL cholesterol by the cholesterol esterase method, and triglycerides by the lipase method. Apolipoprotein B (ApoB) was measured by a nephelometric method on a Beckman IMMAGE automated analytical system (Beckman-Coulter). LDL cholesterol was calculated from total cholesterol, HDL-cholesterol, and triglyceride values using the formula, LDL cholesterol = total cholesterol-HDL-triglycerides/2.2.Citation23
LDL subclass analysis
A modified tube gel electrophoresis technique, the Lipoprint System (Quantimetrix Corporation)Citation24 was used. A serum sample (25 μL) was applied to the “ready to use” polyacrylamide gel tube along with 200 μL of a loading gel solution containing a lipophilic dye. The sample loading gel mixture was photopolymerized for 30 minutes prior to electrophoresis at a constant of 3 mA/tube for one hour. This system resolved up to 12 serum lipoprotein fractions as follows: VLDL (1), mid-band (3), LDL (7), and HDL (1). HDL migrated the fastest (retention factor [Rf] = 1), while VLDL migrated the slowest to the top of gel (Rf = 0). Mid-band and LDL subfractions migrated at various Rfs between VLDL and HDL. Lipoware computer software (Quantimetrix Corporation) was used to analyze the gel images. The bands were partitioned into discrete segments, and the relative area under the curve calculated for each lipoprotein band. The program also calculated the cholesterol concentration for each lipoprotein fraction using a total cholesterol value obtained for each sample by the routine assay mentioned under analysis.
Using the Lipoprint method, VLDL remained at the origin (Rf = 0.0), whereas HDL migrated at the front (Rf = 1.0). In between, several bands could be detected, ie, mid-bands C, B, and A, which corresponded mainly to intermediate-density lipoproteins, as well as up to seven LDL bands. The LDL1 and LDL2 bands corresponded to large buoyant LDL particles, whereas bands LDL3–7 corresponded to small dense LDL particles. According to the LDL electrophoretic profile, two phenotypes are defined, ie, A and non-A. The LDL particle size was estimated using the Lipoprint System by means of the algorithm developed by Kazumi et al.Citation25 The size cutoff was ≥26.8 nm for phenotype A (normal LDL size) and less than this for non-A (designated as phenotype B). It is likely that the temperature gradient gel electrophoresis method overestimated LDL particle size in comparison with other methods and, therefore, this method’s size cutoff is probably equivalent to the gradient gel electrophoresis cutoff of 25.7 nm for small dense LDL.Citation26
Quality control
The internal quality of routine analyses was monitored at two levels of concentration, ie, normal and pathological. Glucose and lipid parameters were included in the Kuwait National and Biorad external quality assurance schemes. For LDL subclass analysis, the quality control material (Liposure) used was obtained from Quantimetrix Corporation, the manufacturers of the Lipoprint gel tube electrophoresis system.
Data analysis
Assessment of differences between the means, correlations between chosen parameters, and regression analyses were carried out using SPSS 15 for Windows. Significance was set at the level of P < 0.05.
Results
shows that patients with SLE and healthy controls were well matched with respect to age, gender, hypertension, BMI, and fasting blood sugar. This was done to eliminate these parameters as confounding variables in the analysis of the lipid data. Compared with controls, patients with SLE had significantly higher plasma total cholesterol (6.62 ± 0.84 versus 5.24 ± 0.64 mmol/L), LDL cholesterol (4.72 ± 0.68 versus 3.30 ± 0.53 mmol/L), triglycerides (2.53 ± 0.24 versus 1.85 ± 0.18 mmol/L), Apo B (0.96 ±0.18 versus 0.73 ±0.10 mmol/L), and triglyceride:HDL cholesterol ratio (3.29 ± 0.42 versus 1.68 ± 0.31), but had significantly lower plasma HDL cholesterol (0.77 ± 0.22 versus 1.10 ± 0.23 mmol/L) and LDL particle size (24.8 ± 1.23 versus 26.1 ± 1.31 nm) than healthy controls. The LDL subclass analysis showed that 26 of the 50 patients with SLE were phenotype B, while only 10 of the 50 healthy controls were phenotype B. The remaining 24 of the SLE patients and 40 of the healthy controls were phenotype A. Thus, the prevalence of the LDL phenotype B among patients with SLE was 52% and was only 20% among healthy controls. This difference was statistically significant (P < 0.01). and represent pattern A and B, respectively.
Figure 1 The densitometric scan of LDL subfraction (Pattern A) obtained in controls.
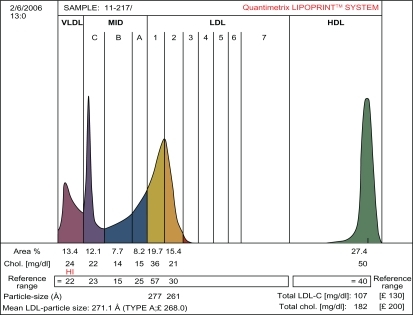
Figure 2 The densitometric scan of LDL subfractions (Pattern B) obtained in patients with SLE.
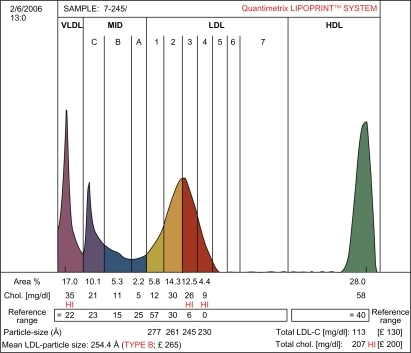
Table 1 Demographic and metabolic characteristics of patients with SLE and healthy controls
Discussion
We have demonstrated in this study that our patients with SLE had significantly higher plasma concentrations of VLDL, triglycerides, LDL, and ApoB, but lower plasma HDL than healthy controls. Two distinct types of dyslipoproteinemia in SLE have been described in the literature. The first type is characterized by high levels of VLDL triglycerides and VLDL cholesterol, and low levels of HDL. This lipid profile is usually seen in untreated or inactive SLE, but can also be seen in patients with active disease.Citation27–Citation30 Our patients fall into this category. Little is known about the mechanisms behind this lipid disorder, although decreased activity of endothelial lipoprotein lipase and impaired chylomicron removal from plasmaCitation29 are two factors present in SLE patients which may contribute to elevations of triglycerides. Antibodies to ApoA1 are also detected in some SLE patients and may contribute to low levels of HDL.Citation30,Citation31 However, we did not estimate antibodies to ApoA1 in our patients. The second pattern of lipid disturbance often seen in SLE arises as a complication of steroids.Citation32 Steroid treatment induces an increase in total cholesterol (including both LDL and HDL) and a more modest elevation of triglycerides.Citation33 Patients with renal disease also have increased levels of total and LDL cholesterol, together with triglycerides and HDL. It is unlikely that our patients had renal disease because none of them had proteinuria or a plasma creatinine concentration >120 μmol/L.
We have demonstrated using the Lipoprint LDL system that patients with SLE have a smaller denser LDL particle size than healthy controls. The generation of small dense LDL particles occurs due to elevation of mild to moderate hyperglyceridemia.Citation34 Under these conditions, triglycerolrich VLDL increases due to overproduction in the liver or defective clearance from the circulation. Cholesteryl ester transfer protein removes cholesteryl ester and replaces it with triacylglycerol as the protein shuttles between VLDL, LDL, and HDL particles. Triacylglycerol-enriched LDL is a better substrate for hepatic lipase, which removes triacylglycerol from small lipoprotein particles. When the hepatic lipase activity is high enough, lipolysis generates smaller and denser LDL particles. LDL oxidation is an important factor in atherosclerosis, and small dense LDL particles are easier to oxidize than larger, less dense particles. As a result of oxidation, a variety of immunogenic neoepitopes are formed on the oxidized LDL. For example, oxidation of phosphorylcholine containing phospholipids renders them antigenic. Oxidized LDL forms ligands on oxidized LDL particles recognized by macrophages, leading to enhanced uptake of oxidized LDL particles and foam cell formation.Citation36–Citation38 Through this route, macrophages become lipid-laden and develop into the characteristic foam cells of atherosclerotic lesions. Oxidized LDL is also chemotactic, immunostimulatory, and has toxic properties that promote local inflammatory processes in atherosclerotic lesions.Citation39,Citation40 Furthermore, oxidized LDL elicits a humoral immune response with production of autoantibodies to oxidation-specific epitopes of oxidized LDL. Therefore, the presence of small dense LDL subfractions in patients with SLE may be an independent risk factor for the development of premature atherosclerosis.
Disclosure
The authors report no conflicts of interest in this work.
References
- ManziSMeilahnENRairieJEAge-specific incidence rates of myocardial infarction and angina in women with systemic lupus erythematosus: Comparison with the Framingham studyAm J Epidemiol19971454084159048514
- PetriMSpenceDBoneLRHochbergMCCoronary artery disease risk factors in the Johns Hopkins Lupus Cohort: Prevalence, recognition by patients and preventive practicesMedicine1992712913021522805
- EsdaileJMAbrahamowiczMGrodzickyTTraditional Framingham risk factors fail to fully account for accelerated atherosclerosis in systemic lupus erythematosusArthritis Rheum2001442331233711665973
- BruceINUrowitzMBGladmanDDHallettDCNatural history of hypercholesterolemia in systemic lupus erythematosusJ Rheumatol1999262137214310529129
- WardMMPremature morbidity from cardiovascular and cerebrovascular diseases in women with systemic lupus erythematosusArthritis Rheum2002462010201912209502
- FischerLMSchliengerRGMatterCJickHMeierCREffect of rheumatoid arthritis or systemic lupus erythematosus on the risk of first-time acute myocardial infarctionAm J Cardiol20049319820014715346
- BorbaEFBonfaEDyslipoproteinemia in systemic lupus erythematosus: Influence of disease activity and anticardiolipin antibodiesLupus199765335399256312
- BorbaEFSantosRDBonfaELipoprotein (a) levels in systemic lupus erythematosusJ Rheumatol1994212202238182628
- Martínez-BerriotxoaARuiz-IrastorzaGEgurbideMVRuedaMAguirreCHomocysteine, antiphospholipid antibodies and risk of thrombosis in patients with systemic lupus erythematosusLupus20041392793315645748
- FrostegardJSvenungssenRWuRLipid peroxidation is enhanced in patients with systemic lupus erythematosus and is associated with arterial and renal manifestationsArthritis Rheum20055219220015641060
- SelzerFSutton-TyrrellKFitzgeraldSGComparison of risk factors for vascular disease in the carotid artery and aorta in women with systemic lupus erythematosusArthritis Rheum20045015115914730611
- LindgrenFTJensenLCWillsRDFreemanNKFlotation rates, molecular weights and hydrated densities of the low density lipoproteinsLipids196943373445823713
- AdamsGHSchumakerVNPolydispersity of human low-density lipoproteinsAnn N Y Acad Sci19691641301465259642
- HammondMGFisherWRThe characterisation of a discrete series of low-density lipoproteins in the disease, hyper-pre β-lipoproteinemiaJ Biol Chem1971246545454554999356
- LeeDMIsolation and characterization of low-density lipoproteinsDayCELevyRSLow Density LipoproteinsNew York, NYPlenum Press1976
- ShenMSKraussRMLindgreeenFTForteTMHeterogeneity of serum low-density lipoproteins in normal human subjectsJ Lipid Res1981222362447240955
- BaurowichGMDashJHensleyWJTurtleJRGradient gel electrophoresis of human plasma lipoproteinsClin Chem1973194154184350149
- CamposHGranestJJJrBilijieventsELow density lipoprotein particle size and coronary artery diseaseArterioscler Thromb1992121871951543692
- CoreshJKwiteroviwichPOJrSmithHHBachorikPSAssociation of plasma triglyceride concentration and LDL particle diameter, density and chemical composition with premature coronary artery disease in men and womenJ Lipid Res19933418871897
- AustinMABreslowJLHennekensCHBuringJEWilletWCKraussRMLow-density lipoprotein subclass patterns and risk of myocardial infarctionJAMA1988260191719213418853
- ChungCPOeserARaggiPLipoprotein subclasses and particle size determined by nuclear magnetic resonance spectroscopy in systemic lupus erythematosusJ Rheumatol2009371633163820516025
- HuaXSuJSvenungssonEDyslipidaemia and lipoprotein pattern in systemic lupus erthematosus (SLE) and SLE-related cardiovascular diseaseScand J Rheumatol20093818418919165647
- FriedwaldWTLevyRIFredricksonDSEstimation of the concentration of low-density lipoprotein cholesterol in plasma without use of preparative ultracentrifugeClin Chem1972184995024337382
- HoefnerDMHodelSDO’BrienJFDevelopment of a rapid, quantitative method for LDL subfractionation with the use of the Quantimetrix Lipoprint LDL SystemClin Chem20014726627411159775
- KazumiTKawaguchiAHozumiTLow density lipoprotein particle diameter in young, nonobese, normolipidemic Japanese menAtherosclerosis19991421131199920512
- MunizNDuncanDNeyerGNormal reference ranges for serum lipoproteins and their subfractions for the Lipoprint™ LDL SystemPresented at the American Association of Clinical Chemistry, 53rd Annual MeetingChicago, ILJuly 29–August 2, 2001
- BorbaEFBonfaEDyslipoproteinemias in systemic lupus erythematosus: Influence of disease, activity, and anticardiolipin antibodiesLupus199765335399256312
- IlowiteNTSamuelPGinzlerEJacobsonMSDyslipoproteinemia in pediatric systemic lupus erythematosusArthritis Rheum1988318598633134897
- BorbaEFBonfaEVinagreCGRamiresJAMaranhaoRCChylomicron metabolism is markedly altered in systemic lupus erythematosusArthritis Rheum2000431033104010817556
- MerrillJTRivkinEShenCLahitaRGSelection of a gene for apolipoprotein A1 using autoantibodies from a patient with systemic lupus erythematosusArthritis Rheum199538165516597488287
- DinuAMerrillJShenCAntonovIMyonesBLahitaRFrequency of antibodies to the cholesterol transport protein apolipoprotein A1 in patients with SLELupus199873553609696140
- PetriMLakattaCMagderLGoldmanDEffect of prednisone and hydroxychloroquine on coronary artery disease risk factors in systemic lupus erythematosus: A longitudinal data analysisAm J Med1994962542598154514
- EttingerWHGoldbergAPApplebaum-BowdenDHazzardWRDyslipoproteinemia in systemic lupus erythematosus: Effect of corticosteroidsAm J Med19872112641267
- AustinMAKingMCVranizanKMKraussRMAtherogenic lipoprotein phenotype. A proposed genetic marker for coronary heart disease riskCirculation1990824955062372896
- WitztumJLThe oxidation hypothesis of atherosclerosisLancet19943447937957916078
- WuRHuangYHElinderLSFrostgardJLysophosphatidyl choline is involved in the antigenicity of oxidized LDHArterioscler Thromb Vasc Biol1998186266309555869
- BinderCJChangMKShawPXInnate and acquired immunity in atherogenesisNat Med200281218122612411948
- HorkkoSBirdDAMillerEMonoclonal autoantibodies specific for oxidized phospholipids or oxidized phospholipids-protein adducts inhibit macrophage uptake of oxidized low-density lipoproteinsJ Clin Invest19991031171289884341
- SteinbergDAtherogenesis in perspective: Hypercholesterolemia and inflammation as partners in crimeNat Med200281211121712411947
- GlassCKWitztumJLAtherosclerosis: The road aheadCell200110450351611239408