
Abstract
Aortic intramural hematoma (AIH) is an entity within the acute aortic syndrome. Combination of a priori probability, clinical history, laboratory blood test and imaging techniques are the basis for diagnosis of AIH. This review is focused on all aspects related to diagnosis of patients with AIH, from clinical to imaging and analytical.
Introduction
Aortic intramural hematoma (AIH) is an entity within the acute aortic syndrome (AAS). Under this denomination, we consider several pathologies with a common clinical presentation: classic aortic dissection, intramural hematoma, penetrating aortic ulcer, and incomplete dissection.Citation1,Citation2 The underlying pathophysiological mechanism is different in each of those elements. Any of them may evolve to another and, in some patients, they can coexist.Citation1
AIH accounts for up to one third of patients with AAS.Citation3,Citation6 Classically it has been defined as a type of classic aortic dissection without an entrance tear.Citation1,Citation7 Histologically, AIH consists of a haemorrhage within the aortic media of variable thickness and extension.Citation8,Citation10 Controversy still exists about the origin and the physiopathology of aortic intramural hematoma. Classic hypothesis of hemorrhage of vasa vasorum is now under discussion. With the current imaging techniques it is possible to observe small intimal disruptions in some patients with AIH. The exact significance and prognostic implications of those focal disruptions is under study.Citation11,Citation15
Diagnosis of AAS requires a high level of clinical suspicion. Clinical presentation may be highly variable.Citation1,Citation13,Citation14,Citation16 Although chest pain is the most common clinical symptom in patients with AAS, the clinical picture of these patients may be confusing, leading to misdiagnosis.Citation15,Citation17,Citation19 Combination of a priori probability, clinical history, laboratory blood test, and imaging techniques are the basis for a diagnosis of AIH.Citation12,Citation13,Citation18,Citation19
This revision is focused on all aspects related to diagnosis of patients with AIH, from clinical to histopathological. In addition, we will address some important issues on the imaging follow-up.
Clinical Presentation and Differential Diagnosis
Compared to classic aortic dissection (AD), patients with AIH are older and they show a higher number of cardiovascular risk factors.Citation3,Citation20 Thereby, hypertension, diabetes, and hyperlipidemia are usually present in a greater proportion among patients with AIH.Citation3 On the contrary, clinical history of Marfan syndrome is strongly associated with AD. Regarding gender, it is well known that AAS is more frequent in males.Citation13,Citation14,Citation16 However, when comparing AIH with AD, the proportion of females is higher in the group of AIH (56% vs 44%), as found by Matsushita et al.Citation21
In patients with AAS, the clinical presentation, as well as the therapeutic approach and prognosis, is usually determined by the involvement of the ascending aorta (Stanford type A). In this sense, AIH exclusively affects the descending aorta in a greater proportion than the AD, where the Stanford type A is more frequent (73 vs 27%).Citation3,Citation20
Chest pain is the most common clinical symptom among patients with AAS.Citation12,Citation13 This chest pain, so called “aortic pain”, is described as abrupt, sharp, intense, tearing, frequently radiating in the direction of the aortic affectation and the aortic branches involved.Citation22 The most frequent location of pain is the chest in patients with type A AAS, whereas aortic pain is usually located in the back in patients with type B AAS.Citation1,Citation13,Citation15,Citation17 Surprisingly, comparison between AIH and AD evinces that chest or back pain are more prevalent among patients with type B AIH (80% vs 68.9% and 79% vs 69.8%, respectively), whereas the presence of pain is present in a similar proportion of patients with type A AIH and AD.Citation3,Citation21,Citation23
The clinical picture of patients with AAS is highly variable. Signs and symptoms at presentation are related to arterial branch involvement, organ impairment, and other AAS-related complications. Although the clinical profile of patients with AIH and AD may be similar, there are some differences that remain constant throughout the different series and deserve mention.Citation3,Citation21,Citation23 Clinical symptoms of heart failure are present in a lesser proportion among AIH patients than in those with AD. The explanation for this is the lower proportion of aortic regurgitation in patients with AIH and ascending aorta affectation, as compared to AD patients.
Clinical presentation of AAS may be related to arterial branches involvement and organ malperfusion. Neurological symptoms, bowel ischemia, peripheral pulse deficit, and limb ischemia are less common in AIH patients than in AD. Myocardial ischemia appears in 10–15% of patients with AD. This complication may be the result of a propagation of the dissecting hematoma to the coronary artery, dynamic occlusion caused by the intimomedial flap or involvement of the coronary ostia.Citation13,Citation24 Differential diagnosis may be complicated in the presence of myocardial ischemia. Eventual misdiagnosis could lead to a wrong treatment administration and potentially lethal complications. Although myocardial ischemia may occur in the AIH setting, this complication is less frequent than in patients with AD. On the contrary, periaortic hematoma and its potential consequences, such as pleural and pericardial effusion, are more prevalent in AIH.Citation3,Citation21,Citation23
Gathering all these features we are able to build a clinical profile of patients with AIH, as compared to those with AD: they are older, and they have more cardiovascular risk factors. Ascending aorta is less involved and therefore aortic regurgitation is less presented. Malperfusion symptoms occur less frequently, but periaortic hematoma and subsequently pericardial effusion are more common in patients with AIH.
Acute coronary syndrome and pulmonary embolism together with AAS should be considered in the differential diagnosis of patients with chest pain admitted to the emergency service.Citation25
The first step after medical history is the performance of an EKG and chest X-ray. It should be mentioned that a normal chest X-ray does not rule out an AAS as the cause of chest pain.Citation26 In fact, we must consider the AAS in patients complaining of chest pain when the EKG does not show ischemic changes and troponin levels are normal or mildly elevated. Biomarkers and imaging tests will be essential in the diagnostic workup.
Biomarkers
Current clinical practice guidelines collect a series of biomarkers that should be measured in all patients admitted with chest pain for differential diagnosis or detection of complications.Citation12,Citation13 Among them, red and white blood cell count will help to identify serious blood loss, anemia, and the presence of concomitant infection and inflammatory response, respectively. High levels of aspartate transaminase and alanine aminotransferase may indicate the presence of liver ischemia, as is the case with creatinine in renal malperfusion. Nevertheless, all these biomarkers are non-specific of AAS or AIH. In patients with AAS they are useful as prognostic markers and for the identification of potential AAS-derived complications.Citation12,Citation13
Plasma D-dimer is a degradation product of cross-linked fibrin which has proved utility in diagnosis of pulmonary embolism.Citation27,Citation28 The upper normal limit is 500 ng/mL. D-dimers are also useful in diagnosis of suspected AAS, mainly during the first 24 hours after symptoms onset.Citation29 Diagnostic accuracy of D-dimer decreases when the blood sample is obtained too early after the onset of pain or when measurements are performed later than 7 days. Repeated measurement could be helpful when the initial determination results are negative.Citation30
The usefulness of D-dimer in the diagnosis of AD has been widely proved in numerous studies.Citation18,Citation29,Citation31,Citation34,Citation36 A metanalysis combining the results of seven studies including 734 patients showed that the sensibility and specificity of D dimer in diagnosis of AD were 97% and 56%, respectively.Citation32 A high negative predictive value (NPV) is the main power of D-dimer. The NPV of D-dimer slightly varies throughout the studies and is placed at 96% for a cutting value of 500 ng/mL in the previously mentioned meta-analysis.
The available data regarding the diagnostic accuracy of D-dimer in patients with AIH are not so vast as for AD. Gorla et alCitation30 performed serial measurements of D-dimer levels in 231 patients, of which 35 had an AIH, and compared them to 291 controls without AAS admitted for chest pain. D-dimer resulted in a useful marker for the diagnosis of AAS, both in AD and AIH. The area under the curve in patients with AIH was 0.98 (P<0.001). When using a cutoff value of 500 ng/mL, D-dimer showed excellent diagnostic properties for detection of AIH: sensibility 100%, specificity 67%. In patients with isolated penetrating aortic ulcer the diagnostic performance was not so good.Citation30
When included in an algorithm based in the a priori probability of AAS, D-dimer levels increase the diagnostic value of the strategy.Citation18,Citation33 Thus, when a particular patient does not show any of the risk factors for AAS and the D-dimer is negative, the failure rate for rejection of AAS diagnosis is 0.3%, similar to when the patient has one risk factor but the D-dimer is also negative.Citation18 In terms of diagnostic accuracy, the strategy based on the combination of pre-test probability of AAS plus D-dimer yielded a NPV of 99.7%, whereas sensibility and specificity results were 98.8% and 57.3%, respectively.Citation18
Serial D-dimer measurements may also be helpful during hospitalization of patients with type B AIH.Citation34 A significant re-elevation of D-dimer levels can be associated with progression of the disease. In patients with AIH, this re-elevation may indicate transformation into a classic AD, the extension of damage, the formation of new ulcer-like lesions or the enlargement of previous ones.Citation34,Citation35 D-dimer re-elevation could also be related to the thrombotic process, such as deep vein thrombosis or pulmonary embolism that sometimes appear as complications of the process.Citation35,Citation36
D-dimer has also proved to have an association with prognosis, not only the level at admission, but also measurements during hospitalization.Citation30 Then, higher levels of D-dimer at admission and during in-hospital follow-up are associated with a worse prognosis and higher mortality. Indeed, a D-dimer level >9 mg/L (9,000 ng/mL) resulted in an independent factor of greater mortality among patients with AAS.Citation30
A number of biomarkers have been assessed in the setting of AAS. Such is the case of smooth muscle myosin, soluble fragments of elastin, calponin, or matrix metalloproteinase 8.Citation37,38,Citation39,Citation42 They still remain in a research phase and their use has not been incorporated to clinical practice yet. All of them have been evaluated for diagnosis in patients with classic AD and there are no available data on AIH.
Imaging Test
Imaging techniques are the cornerstone for diagnosis of patients with AAS, and more precisely those with AIH. Chest X-ray is mandatory in all patients with suspected AAS. However, the diagnostic ability of this technique is quite poor. Computed tomography (CT) is the best choice in case of high suspicion of AAS. Both CT and magnetic resonance imaging (MRI) are the leading imaging techniques in diagnosis of AIH-patients. The different diagnostic test used in diagnosis of AIH will be discussed in detail through this section.
Echocardiography
Considering its wide availability and readiness, transthoracic echocardiography (TTE) at bedside must always be the first imaging test to be done in patients with high suspicion of AIH.Citation13 This statement is especially meaningful in unstable patients in whom rapid TTE can be done in the emergency department. TTE will not only help in diagnosis of AIH, but also will give some important clues for the differential diagnosis with acute coronary syndrome and pulmonary embolism.Citation40
TTE enables evaluation of some segments of the aorta, such as the aortic root and the proximal segment of the ascending aorta ().Citation41,Citation42 In some cases, it is also possible to obtain images of the aortic arch, proximal descending aorta, and some segments of the abdominal aorta. Although in patients with classic AD it is well documented that there is a sensibility of 75–90% for type A AD which decreases to 31–55% in type B AD,Citation13,Citation42 this is not the case for AIH, where sensibility is less than 40%.Citation43,Citation44 Even with contrast administration, diagnostic competence of TTE in AIH is low. Therefore, isolated TTE is not recommended for diagnosis of AIH.
Figure 1 (A) Parasternal long axis view showing a thickened aortic wall in a patient with type A intramural aortic hematoma (arrowhead). (B) Same view with color doppler. Notice a significant aortic regurgitation.
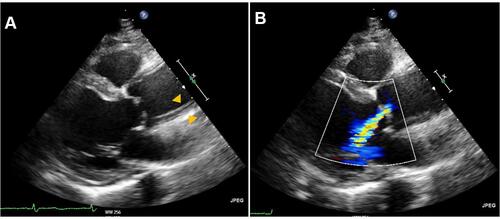
However, some complications of AIH, as pericardial effusion, are excellently detected with TTE.Citation3,Citation41,Citation44,Citation46,Citation47 Pericardial effusion appears in up to 60% of patients with type A AIH.Citation3,Citation45 In some cases, pericardial effusion is a sign of aortic rupture, whereas in some others it resulted from blood extravasation through an irritated adventitia.Citation46 In any case, the presence of pericardial effusion in patients with AIH is associated with a worse prognosis.Citation1,Citation3,Citation6 TTE also allows evaluation of the aortic valve and aortic regurgitation ().Citation13,Citation42,Citation44,Citation46 Thirty-five percent of patients with type A AIH have some grade of aortic regurgitation.Citation3 In such cases, the severity of the aortic regurgitation will have important implications on the surgical technique.
TTE is sometimes limited by acoustic interferences, rib cage abnormalities, and lung interposition. These may be overcome with the transoesophageal echocardiography (TOE). Nevertheless, TOE requires a higher level of expertise in the operator for image acquisition and in interpretation.Citation46 In AIH, TOE is a reliable technique with a 96.5–99.6% sensibility and 92.3–98.5% specificity.Citation42,Citation46,Citation48 A >5 mm aortic wall thickness is accepted as a diagnostic criterion in the presence of a compatible clinical setting.Citation43 Normal aortic wall thickness is placed at 3 mm or less.Citation43 Mean aortic wall thickness has been placed at 12 mm for type A AIH and 10 mm for type B, throughout the series.Citation43,Citation49 Medial displacement of the intimal calcium may be identified by TOE and is helpful in the differential diagnosis with a mural thrombus. Identification of patent flow in both the true and the false lumen is a typical sign of classic AD, as a difference to AIH. However, when the false lumen is completely thrombosed, differentiation between both entities is not so easy. TOE is an essential tool in the operating room for the assessment of aortic valve injury. TOE is clearly superior to TTE in the evaluation of the aortic valve and identification of the aortic regurgitation mechanism.Citation50
Compared to other imaging techniques, such as the CT and MRI, TOE does not provide complete information of the whole aorta extension and aortic branch injury. Other disadvantages of the TOE are the need for patient sedation, the presence of artifacts and reverberations that may simulate an intimal flap. These reverberations appear in 44–55% of studies.Citation51 The TOE must be performed by experienced staff in order to make a proper diagnostic assessment and to avoid potential diagnostic errors.
Computed Tomography
CT has several advantages that make it the preferred technique for patients with suspected acute AIH. CT images have rapid examination times and are extensively available in emergency services of most hospitals. CT also allows full anatomic assessment of the whole aorta and aortic branch vessels. For all these reasons CT is the most widely used imaging technique for diagnosis of patients with AAS and AIH.Citation3,Citation41,Citation52 CT sensitivity in the diagnosis of AIH rounds 100%.Citation47,Citation52,Citation55 Results from the IRAD series showed that 85% of patients with type A AIH and 92% with type B AIH underwent CT. None of the patients in this series had a normal CT.Citation3
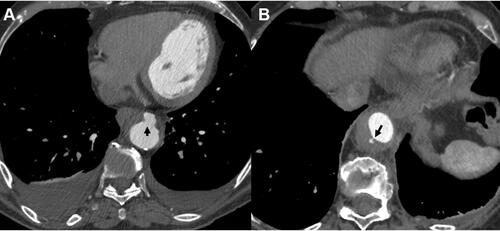
For diagnosis of AIH both unenhanced and contrast-enhanced images must be obtained.Citation53 On unenhanced CT images AIH appears as a circular or crescentic hyperattenuating thickening in the aortic wall. This thickening is usually >7 mm and attenuation is 60–70 HU ().Citation53 After contrast administration, the AIH typically appears as non-enhanced circular or crescent-shaped aortic wall thickening.Citation1,Citation7,Citation47,Citation49 When present, intimal calcifications are characteristically displaced inward as a difference with mural thrombus (). AIH may coexist with penetrating aortic ulcers, associated with atherosclerosis. Classic AD is also observed in some aortic segments in patients with AIH.
Figure 2 (A) Unenhanced computed tomography image where aortic intramural hematoma appears as a crescentic hyperattenuating thickening in the aortic wall (asterisk). (B) Same slice after contrast administration. The aortic intramural hematoma can be observed as non-enhanced crescent-shaped aortic wall thickening. Intimal calcification is characteristically displaced inward (arrowhead).

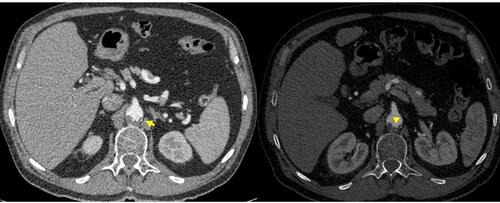
With current CT equipment it is possible to identify some relevant details in patients with AIH. Although classically AIH was thought to be the result of an intramedial haemorrhage of the vasa vasorum without an entrance intimal tear, the underlying pathophysiological mechanism is still a controversial issue.Citation2,Citation6,Citation54,Citation55 In fact, intimal tears have been found intraoperatively in the ascending aorta in up to 73% of patients initially diagnosed of type A AIH submitted to surgery.Citation21,Citation56 In some patients with AIH these tiny intimal tears are evident on the CT slices, whereas in some others they remain invisible on the imaging test. Ulcer-like projections (ULP), also called focal intimal disruptions, may also be observed within the thickened aortic wall of patients with AIH ().Citation11,Citation13,Citation55 These lesions should be distinguished from tiny intimal disruptions, which correspond to artery branch ostia (). Among these last, characteristically the orifice size is less than 3 mm and it is possible to follow the path of the vessel emerging from the aorta.Citation54
Figure 3 (A) Ulcer-like projection in the descending aorta of a patient with aortic intramural hematoma (arrow). (B) Tiny intimal disruption corresponding to an artery branch ostium (arrow).
The origin and pathophysiology of ULP is not completely understood.Citation11,Citation13,Citation55 The underlying mechanism will probably be different depending on the moment of occurrence.Citation54,Citation55 The presence of ULP in the acute phase of the AIH is associated with an increased risk of aortic rupture. Conversely, when these lesions are observed in a subacute or chronic phase, they tend to reabsorb or to evolve towards aortic dilation.Citation54 In such cases of ULP appearing in the chronic phase of AIH, the most probable mechanism is the parietal stretching as a consequence of the intramedial hematoma. Among those ULP observed at presentation in the acute moment, it has been hypothesized that they could be truly entry tears of an aortic dissection with thrombosed false lumen. Previous studies in patients initially diagnosed with type AIH who underwent surgery in whom an intimal tear was observed in the ascending aorta support this hypothesis.Citation21,Citation56
One of the main characteristics of AIH is its evolving nature.Citation35,Citation49 It is hard to make predictions about the evolution of the AIH in a particular patient. Therefore, performing serial control CT scans during hospitalization and follow-up after discharge will be essential.Citation57,Citation58 There are no formal recommendations on when to perform control CT scans. Decision-making should be individualized in each case, and participation of the aortic multidisciplinary team is mandatory. It is recommended to perform a control CT scan 48–72 h after initial diagnosis and in the case of new onset symptoms or hemodynamic instability.
Patients with AIH can result in stabilization or even evolve to complete resorption.Citation35 In some patients, AIH remodeling may lead to aortic dilation and aneurism formation.Citation1,Citation6,Citation49 It is not so rare that classic aortic dissection could appear during the follow-up in patients with AIH.Citation7,Citation59 Actually, in some patients both entities can coexist at the moment of acute presentation. The most feared complication of AIH is the aortic rupture. CT scan enables identification of some features of the AIH associated with a worse prognosis. Ascending aorta involvement, maximum hematoma thickness >11 mm, and maximum aortic diameter >50 mm have been linked to a higher risk of complicationsCitation7,Citation13,Citation59 Some other details, such as pleural or pericardial effusion, organ ischemic signs are also noticed by CT scan. As mentioned above, the identification of focal intimal disruptions or ULP in the acute phase entails a higher risk of aortic rupture and the invasive treatment should be considered.Citation13,Citation54 ULP >10 mm in depth associates a greater risk of complications. Considering new onset ULP in the chronic phase, the optimal treatment is controversial. While some authors stand for an invasive approach with endoprosthesis implantation in order to stabilize lesions, some others recommend a more conservative strategy based on serial control CT scans, leaving surgical or endovascular treatment for those patients who present significant aortic enlargement.Citation7,Citation11,Citation14 The appearance of classic aortic dissection in certain aortic segments is also associated with an increased risk of rupture and the invasive alternative must be considered.
Radiologically, differential diagnosis of AIH include the classic AD with thrombosed false lumen and the mural thrombus. Differences between AD with fully thrombosed false lumen and AIH are difficult to recognize. Identification of an entrance tear or the presence of certain segments with patent flow in the false lumen are both properties of classic AD. In some patients, the true diagnosis can only be confirmed in theatre when patients undergo surgery.Citation56 Regarding the mural thrombus, hyper-attenuation is typically not observed on the unenhanced images.Citation60 The inline of the mural thrombus is usually irregular, compared to the smooth border of AIH. Unlike the AIH where intimal calcium is displaced inward, calcification is usually placed externally to the mural thrombus ().
Figure 4 Two computed tomography slices showing a mural thrombus. As a difference to aortic intramural hematoma, intimal calcium remains external to the thrombus (arrow). Borders are usually irregular (arrowhead).
Differential diagnosis of AIH must include the aortitis.Citation61 Although the clinical picture is generally different and is helpful to guide the diagnosis, there are several cases reported in the literature of aortitis simulating an AIH. There are some clues that could be useful for radiological diagnosis. ULP or intramural blood pools are not observed among patients with aortitis on the angio-CT images. Therefore, those focal lesion may be useful in differentiating AIH from aortitis.Citation11,Citation13,Citation55 Circular, and not crescent-shaped, aortic wall thickening is more common in aortitis. However, some of the typical imaging signs of AIH may be present in patients with aortitis. Such is the case of central displacement of intimal calcification, hyperintensity in non-contrast images, and the absence of enhancement after contrast administration.Citation62,Citation63 In this sense, positron emission tomography-CT (PET-CT) may have the key for diagnosis. An increased glucose uptake and subsequent hyper-enhanced corresponding to the thickened aortic wall is diagnostic of aortitis.Citation61 AIH could also be present in patients with a known medical history of vasculitis, which makes it even more difficult to diagnose.Citation64 The clinical picture is that D-dimer levels and inflammatory markers could be helpful. Histopathologic study could be especially helpful in such cases to determine the degree of aortic inflammation.
Incomplete dissection refers to a situation in which the intimomedial tear is not followed by separation of the medial layers.Citation1,Citation64 Incomplete dissection is usually accompanied by some degree of sub-adventitial hematoma whose radiological appearance may be confounded with an AIH (). Differentiation of both entities can be really difficult. Identification of an eccentric bulge near the tear and concomitant aortic dilation are typical features of incomplete dissection.Citation60 Electrocardiogram-gated CT imaging may help in the differential diagnosis of AIH and other aortic pathologies as it better defines the aortic wall and eliminates pulsation artefacts. Prospective acquisition significantly reduces radiation doses. Unenhanced CT sequences are also essential for detection of AIH among other aortic pathologies.
Figure 5 Incomplete dissection with some degree of sub-adventitial hematoma on a computed tomography slice. Notice the intimal tear (arrow).

Magnetic Resonance Imaging
The diagnostic accuracy of MRI for AIH is comparable to that of a CT scan and sensibility reaches 100%.Citation53 However, MRI is not routinely used for diagnosis of AIH in the acute setting. Results from the IRAD series showed that MRI was the diagnostic technique in 14.1% of patients with type A AIH and 17.8% of type B AIH.Citation3 Main reasons for this difference with CT lie on the lower availability of MRI in the emergency departments and the longer time required for image acquisition and post-processing. In high-experienced centres, MRI usually take about 30 minutes to obtain images needed for AIH diagnosis. MRI is incompatible with some devices required for life support of unstable patients, which also limit its use.
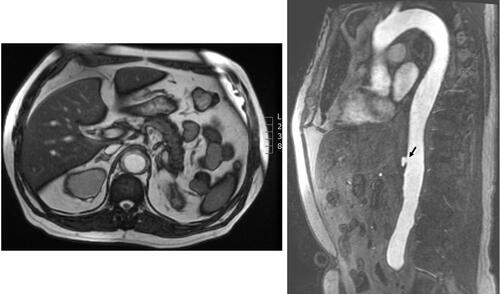
MRI does not require ionizing radiation, so this is a significant advantage for the follow-up imaging studies. Thus, young patients affected of AIH will require at least one annual imaging test to monitor AIH evolution.Citation12,Citation13 In addition, MRI gives important functional information of the aortic valve. This technique also allows identification of pleural and pericardial effusion. Precise measurements of the aortic diameter and aortic wall thickness can be obtained with MRI images (). On echo-gradient sequences, AIH appears isointense, whereas it becomes T1-hyperintense over time due to methaemoglobin formation. The absence of these evolutive changes suggests maintained hemorrhage.Citation65 Dynamic and contrast-enhanced sequences show patent flow in the false lumen, as different to AIH.Citation54
Figure 6 Magnetic resonance images (echo-gradient sequence, axial and sagittal views) showing intramural aortic hematoma. An ulcer-like projection is observed at the abdominal aorta (arrow).
Pathology
Histopathologic examination of the aortic pieces is the ultimate and definitive step in diagnosis. As mentioned above, in some patients initially diagnosed of type A AIH, surgical examination revealed a tiny intimomedial entrance tear with a thrombosed false lumen.Citation56 In these cases, the false channel has not been decompressed by a re-entrance tear and an immediate thrombosis of the false lumen occurred.Citation1 Thus, either macroscopic or microscopic observation of the aortic pieces are essential to determine the right diagnosis, to correlate the clinical picture with the anatomic findings, and to understand the pathophysiology of the acute aortic syndrome.Citation66,Citation67
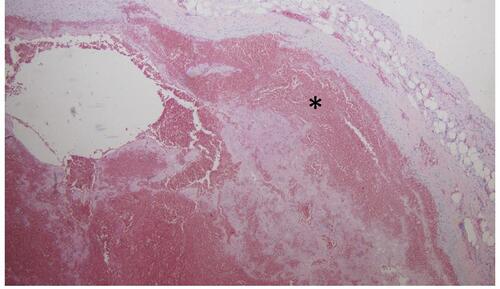
In anatomic pieces of patients with AIH, a hematoma disrupting the aortic media is well documented on histological analysis (). This hematoma is usually intramedial, but in some aortic segments it may be subadventitial, representing a contained aortic rupture.Citation1 The rupture of sick vasa vasorum and traumatic rupture of healthy ones may be involved in the development of the intramedial hemorrhage. Pathology is also essential in establishing the differential diagnosis with other aortic entities such as aortitis, where a marked thickening of the aortic wall with peri-aortic inflammation, but without signs of intramural haemorrhage, can be observed.
Figure 7 Histological section (hematoxylin eosin staining) of a patient with intramural hematoma. Hematoma (asterisk) within the aortic media is well documented.
Prognostic Markers in AIH
As mentioned above, AIH is characterized by a highly variable evolution that makes it difficult to anticipate the clinical course. When compared to classic AD, patients with AIH usually have a better prognosis with lower in-hospital and midterm mortality.Citation20
It is well known that AIH may progress to classic AD and aortic rupture. Besides, in some patients aortic remodeling can lead to aortic dilation and aneurysm formation, whereas complete resorption of the intramedial hematoma has been also well documented.Citation1 There are several features that have been associated with an increased risk of complications. Such is the case of ascending aorta involvement or aortic diameter >50 mm which have been strongly associated with a greater risk of progression to aortic dissection and aortic rupture.Citation3,Citation59 Moreover, AIH thickness (>11 mm) and increasing aortic diameter (>5 mm/year) in repeated imaging tests have also been related to a worse prognosis.Citation45 A number of studies have focused on the appearance and prognostic impact of intimal defects and ulcer like projections. Some of them have delved into the underlying pathophysiological mechanism and have suggested that in some patients those intimal defects could be true entrance tears and such AIH would be classic aortic dissection with thrombosed false lumen.Citation21,Citation56 Recent studies underscore the relevance of the exact moment of occurrence.Citation54 Either way, ulcer-like projection in the setting of AIH requires close clinical and image monitoring.
A decision on when to intervene, either with open surgery or endovascular aortic repair, is beyond the scope of this review focused on diagnosis. However, an aggressive approach should be considered in type B AIH in the following clinical scenarios: appearance of focal intimal disruptions or ulcer-like projections in the acute phase (<14 days after symptoms onset), large intimal erosion (>20 mm), refractory hypertension and uncontrolled pain, progressive pleural effusion, maximum aortic diameter of >45 mm in the acute phase or >50 mm in the chronic phase, significant aortic enlargement during the follow-up (>5 mm/year), and AIH progression to the ascending aorta.Citation1,Citation13,Citation68 Therapeutic decisions must be taken by the aortic multidisciplinary team.
Conclusion
Diagnosis of AIH requires a high level of clinical suspicion. Combination of clinical history, laboratory blood test and imaging techniques are the cornerstone of diagnosis. D-dimer is a useful marker in the differential diagnosis of patients with chest pain at the emergency department. Imaging tests are crucial to achieve a right diagnosis. TTE should be the first imaging approach, but CT will be definitive for diagnosis. Evaluation of the entire aorta extension and aortic branches is mandatory. Serial control CT images are necessary to monitor AIH evolution.
Disclosure
The authors report no conflicts of interest in this work.
References
- Vilacosta I, Aragoncillo P, Cañadas V, San Román JA, Ferreirós J, Rodríguez E. Acute aortic syndrome: a new look at an old conundrum. Heart. 2009;95(14):1130–1139. doi:10.1136/hrt.2008.153650
- Macura KJ, Corl FM, Fishman EK, Bluemke DA. Pathogenesis in acute aortic syndromes: aortic dissection, intramural hematoma, and penetrating atherosclerotic aortic ulcer. AJR Am J Roentgenol. 2003;181(2):309–316. doi:10.2214/ajr.181.2.1810309
- Harris KM, Braverman AC, Eagle KA, et al. Acute aortic intramural hematoma: an analysis from the International Registry of Acute Aortic Dissection. Circulation. 2012;126(11 Suppl 1):S91–6. doi:10.1161/CIRCULATIONAHA.111.084541
- Kang DH, Song JK, Song MG, et al. Clinical and echocardiographic outcomes of aortic intramural hemorrhage compared with acute aortic dissection. Am J Cardiol. 1998;81(2):202–206. doi:10.1016/S0002-9149(97)00885-0
- Zahn R, Erbel R, Nienaber CA, et al. Endovascular aortic repair of thoracic aortic disease: early and 1-year results from a German multicenter registry. J Endovasc Ther. 2013;20(3):265–272. doi:10.1583/12-4107R.1
- Ganaha F, Miller DC, Sugimoto K, et al. Prognosis of aortic intramural hematoma with and without penetrating atherosclerotic ulcer: a clinical and radiological analysis. Circulation. 2002;106(3):342–348. doi:10.1161/01.CIR.0000022164.26075.5A
- Vilacosta I, San Román JA, Ferreirós J, et al. Natural history and serial morphology of aortic intramural hematoma: a novel variant of aortic dissection. Am Heart J. 1997;134(3):495–507. doi:10.1016/S0002-8703(97)70087-5
- Tsai TT, Nienaber CA, Eagle KA. Acute aortic syndromes. Circulation. 2005;112(24):3802–3813. doi:10.1161/CIRCULATIONAHA.105.534198
- Mohr-Kahaly S, Erbel R, Kearney P, Puth M, Meyer J. Aortic intramural hemorrhage visualized by transesophageal echocardiography: findings and prognostic implications. J Am Coll Cardiol. 1994;23(3):658–664. doi:10.1016/0735-1097(94)90751-X
- Agricola E, Slavich M, Bertoglio L, et al. The role of contrast enhanced transesophageal echocardiography in the diagnosis and in the morphological and functional characterization of acute aortic syndromes. Int J Cardiovasc Imaging. 2014;30(1):31–38. doi:10.1007/s10554-013-0290-y
- Sueyoshi E, Matsuoka Y, Imada T, Okimoto T, Sakamoto I, Hayashi K. New development of an ulcerlike projection in aortic intramural hematoma: CT evaluation. Radiology. 2002;224(2):536–541. doi:10.1148/radiol.2242011009
- Hiratzka LF, Bakris GL, Beckman JA, et al. 2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM Guidelines for the diagnosis and management of patients with thoracic aortic disease. A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, American Association for Thoracic Surgery, American College of Radiology,American Stroke Association, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of Thoracic Surgeons,and Society for Vascular Medicine. J Am Coll Cardiol. 2010;55(14):e27–e129. doi:10.1016/j.jacc.2010.02.015
- Erbel R, Aboyans V, Boileau C, et al. ESC Committee for Practice Guidelines. 2014 ESC Guidelines on the diagnosis and treatment of aortic diseases: document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. The Task Force for the Diagnosis and Treatment of Aortic Diseases of the European Society of Cardiology (ESC). Eur Heart J. 2014;35(41):2873–2926. doi:10.1093/eurheartj/ehu281
- Hagan PG, Nienaber CA, Isselbacher EM, et al. The International Registry of Acute Aortic Dissection (IRAD): new insights into an old disease. JAMA. 2000;283(7):897–903. doi:10.1001/jama.283.7.897
- Klompas M. Does this patient have an acute thoracic aortic dissection? JAMA. 2002;287(17):2262–2272. doi:10.1001/jama.287.17.2262
- Trimarchi S, Tolenaar JL, Tsai TT, et al. Influence of clinical presentation on the outcome of acute B aortic dissection: evidences from IRAD. J Cardiovasc Surg. 2012;53(2):161–168.
- Morentin Campillo B, Molina Aguilar P, Monzó Blasco A, et al. Sudden death due to thoracic aortic dissection in young people: a multicenter forensic study. Rev Esp Cardiol. 2019;72(7):553–561. doi:10.1016/j.recesp.2018.05.036
- Nazerian P, Mueller C, Soeiro AM, et al. Diagnostic accuracy of the aortic dissection detection risk score plus d-Dimer for acute aortic syndromes: the advised prospective multicenter study. Circulation. 2018;137(3):250–258. doi:10.1161/CIRCULATIONAHA.117.029457
- Rogers AM, Hermann LK, Booher AM, et al. Sensitivity of the aortic dissection detection risk score, a novel guideline-based tool for identification of acute aortic dissection at initial presentation: results from the international registry of acute aortic dissection. Circulation. 2011;123(20):2213–2218. doi:10.1161/CIRCULATIONAHA.110.988568
- Ahn JM, Kim H, Kwon O, et al. Differential clinical features and long-term prognosis of acute aortic syndrome according to disease entity. Eur Heart J. 2019;40(32):2727–2736. doi:10.1093/eurheartj/ehz153
- Matsushita A, Fukui T, Tabata M, Sato Y, Takanashi S. Preoperative characteristics and surgical outcomes of acute intramural hematoma involving the ascending aorta: a propensity score-matched analysis. J Thorac Cardiovasc Surg. 2016;151(2):351–358. doi:10.1016/j.jtcvs.2015.09.055
- Wooley CF, Sparks EH, Boudoulas H. Aortic pain. Prog Cardiovasc Dis. 1998;40(6):563–589. doi:10.1016/S0033-0620(98)80004-2
- Tolenaar JL, Harris KM, Upchurch GR, et al. The differences and similarities between intramural hematoma of the descending aorta and acute type B dissection. J Vasc Surg. 2013;58(6):1498–1504. doi:10.1016/j.jvs.2013.05.099
- Jánosi RA, Buck T, Erbel R. Mechanism of coronary malperfusion due to type-A aortic dissection. Herz. 2009;34(6):478. doi:10.1007/s00059-009-3272-z
- Kohn MA, Kwan E, Gupta M, Tabas JA. Prevalence of acute myocardial infarction and other serious diagnoses in patients presenting to an urban emergency department with chest pain. J Emerg Med. 2005;29(4):383–390. doi:10.1016/j.jemermed.2005.04.010
- von Kodolitsch Y, Nienaber CA, Dieckmann C, et al. Chest radiography for the diagnosis of acute aortic syndrome. Am J Med. 2004;116(2):73–77. doi:10.1016/j.amjmed.2003.08.030
- Kearon C, de Wit K, Parpia S, et al. Diagnosis of pulmonary embolism with d-Dimer adjusted to clinical probability. N Engl J Med. 2019;381(22):2125–2134. doi:10.1056/NEJMoa1909159
- Righini M, Van Es J, Den Exter PL, et al. Age-adjusted D-dimer cutoff levels to rule out pulmonary embolism: the ADJUST-PE study. JAMA. 2014;311(11):1117–1124. doi:10.1001/jama.2014.2135
- Eggebrecht H, Naber CK, Bruch C, et al. Value of plasma fibrin D-dimers for detection of acute aortic dissection. J Am Coll Cardiol. 2004;44(4):804–809. doi:10.1016/j.jacc.2004.04.053
- Gorla R, Erbel R, Kahlert P, et al. Diagnostic role and prognostic implications of D-dimer in different classes of acute aortic syndromes. Eur Heart J Acute Cardiovasc Care. 2017;6(5):379–388. doi:10.1177/2048872615594500
- Shimony A, Filion KB, Mottillo S, Dourian T, Eisenberg MJ. Meta-analysis of usefulness of d-dimer to diagnose acute aortic dissection. Am J Cardiol. 2011;107(8):1227–1234. doi:10.1016/j.amjcard.2010.12.027
- Watanabe H, Horita N, Shibata Y, Minegishi S, Ota E, Kaneko T. Diagnostic test accuracy of D-dimer for acute aortic syndrome: systematic review and meta-analysis of 22 studies with 5000 subjects. Sci Rep. 2016;6:26893. doi:10.1038/srep26893
- Gorla R, Erbel R, Kahlert P, et al. Accuracy of a diagnostic strategy combining aortic dissection detection risk score and D-dimer levels in patients with suspected acute aortic syndrome. Eur Heart J Acute Cardiovasc Care. 2017;6(5):371–378. doi:10.1177/2048872615594497
- Jo Y, Anzai T, Ueno K, et al. Re-elevation of D-dimer as a predictor of re-dissection and venous thromboembolism after Stanford type B acute aortic dissection. Heart Vessels. 2010;25(6):509–514. doi:10.1007/s00380-010-0028-x
- Ferrera C, Vilacosta I, Suárez-Barrientos A, et al. Aortic intramural hematoma. All-in-one complications. Int J Cardiol. 2013;167(4):e97–8. doi:10.1016/j.ijcard.2013.03.155
- Suzuki T, Distante A, Zizza A, et al. Diagnosis of acute aortic dissection by D-dimer: The International Registry of Acute Aortic Dissection Substudy on Biomarkers (IRAD-Bio) experience. Circulation. 2009;119(20):2702–2707. doi:10.1161/CIRCULATIONAHA.108.833004
- Giachino F, Loiacono M, Lucchiari M, et al. Rule out of acute aortic dissection with plasma matrix metalloproteinase 8 in the emergency department. Crit Care. 2013;17(1):R33. doi:10.1186/cc12536
- Suzuki T, Distante A, Zizza A, et al. Preliminary experience with the smooth muscle troponin-like protein, calponin, as a novel biomarker for diagnosing acute aortic dissection. Eur Heart J. 2008;29(11):1439–1445. doi:10.1093/eurheartj/ehn162
- Nozato T, Sato A, Hirose S, et al. Preliminary study of serum tenascin-C levels as a diagnostic or prognostic biomarker of type B acute aortic dissection. Int J Cardiol. 2013;168(4):4267–4269. doi:10.1016/j.ijcard.2013.04.211
- Chenkin J, Atzema CL. Contemporary application of point-of-care echocardiography in the emergency department. Can J Cardiol. 2018;34(2):109–116. doi:10.1016/j.cjca.2017.08.018
- Evangelista A, Rabasa JM, Mosquera VX, et al. Diagnosis, management and mortality in acute aortic syndrome: results of the Spanish Registry of Acute Aortic Syndrome (RESA-II). Eur Heart J Acute Cardiovasc Care. 2018;7(7):602–608. doi:10.1177/2048872616682343
- Evangelista A, Flachskampf FA, Erbel R, et al. Echocardiography in aortic diseases: EAE recommendations for clinical practice. Eur J Echocardiogr. 2010;11:645–658. doi:10.1093/ejechocard/jeq056
- Song JK. Diagnosis of aortic intramural haematoma. Heart. 2004;90(4):368–371. doi:10.1136/hrt.2003.027607
- Cecconi M, Chirillo F, Costantini C, et al. The role of transthoracic echocardiography in the diagnosis and management of acute type A aortic syndrome. Am Heart J. 2012;163(1):112–118. doi:10.1016/j.ahj.2011.09.022
- Song JM, Kim HS, Song JK, et al. Usefulness of the initial noninvasive imaging study to predict the adverse outcomes in the medical treatment of acute type A aortic intramural hematoma. Circulation. 2003;108(Suppl 1):II324–8. doi:10.1161/01.cir.0000087651.30078.38
- Evangelista A, Maldonado G, Gruosso D, et al. The current role of echocardiography in acute aortic syndrome. Echo Res Pract. 2019;6(2):R53–R63. doi:10.1530/ERP-18-0058
- Mussa FF, Horton JD, Moridzadeh R, et al. Acute aortic dissection and intramural hematoma: a systematic review. JAMA. 2016;316(7):754–763. doi:10.1001/jama.2016.10026
- Keren A, Kim CB, Hu BS, et al. Accuracy of biplane and multiplane transesophageal echocardiography in diagnosis of typical acute aortic dissection and intramural hematoma. J Am Coll Cardiol. 1996;28(3):627–636. doi:10.1016/0735-1097(96)00186-6
- Ferrera C, Vilacosta I, Gómez-Polo JC, et al. Evolution and prognosis of intramural aortic hematoma. Insights from a midterm cohort study. Int J Cardiol. 2017;249:410–413. doi:10.1016/j.ijcard.2017.09.170
- Movsowitz HD, Levine RA, Hilgenberg AD, Isselbacher EM. Transesophageal echocardiographic description of the mechanisms of aortic regurgitation in acute type A aortic dissection: implications for aortic valve repair. J Am Coll Cardiol. 2000;36(3):884–890. doi:10.1016/S0735-1097(00)00766-X
- Pepi M, Campodonico J, Galli C, et al. Rapid diagnosis and management of thoracic aortic dissection and intramural haematoma: a prospective study of advantages of multiplane vs. biplane transoesophageal echocardiography. Eur J Echocardiogr. 2000;1(1):72–79. doi:10.1053/euje.2000.0002
- Yoshida S, Akiba H, Tamakawa M, et al. Thoracic involvement of type A aortic dissection and intramural hematoma: diagnostic accuracy–comparison of emergency helical CT and surgical findings. Radiology. 2003;228(2):430–435. doi:10.1148/radiol.2282012162
- Chao CP, Walker TG, Kalva SP. Natural history and CT appearances of aortic intramural hematoma. Radiographics. 2009;29(3):791–804. doi:10.1148/rg.293085122
- Moral S, Cuéllar H, Avegliano G, et al. Clinical implications of focal intimal disruption in patients with type B intramural hematoma. J Am Coll Cardiol. 2017;69(1):28–39. doi:10.1016/j.jacc.2016.10.045
- Jang YM, Seo JB, Lee YK, et al. Newly developed ulcer-like projection (ULP) in aortic intramural haematoma on follow-up CT: is it different from the ULP seen on the initial CT? Clin Radiol. 2008;63(2):201–206. doi:10.1016/j.crad.2007.07.020
- Park KH, Lim C, Choi JH, et al. Prevalence of aortic intimal defect in surgically treated acute type A intramural hematoma. Ann Thorac Surg. 2008;86(5):1494–1500. doi:10.1016/j.athoracsur.2008.06.061
- Wu MT, Wang YC, Huang YL, et al. Intramural blood pools accompanying aortic intramural hematoma: CT appearance and natural course. Radiology. 2011;258(3):705–713. doi:10.1148/radiol.10101270
- Li Z, Lu B, Chen Y, et al. Acute type B aortic intramural hematoma: the added prognostic value of a follow-up CT. Eur Radiol. 2019;29(12):6571–6580. doi:10.1007/s00330-019-06254-0
- von Kodolitsch Y, Csösz SK, Koschyk DH, et al. Intramural hematoma of the aorta: predictors of progression to dissection and rupture. Circulation. 2003;107(8):1158–1163. doi:10.1161/01.CIR.0000052628.77047.EA
- Gutschow SE, Walker CM, Martínez-Jiménez S, Rosado-de-Christenson ML, Stowell J, Kunin JR. Emerging concepts in intramural hematoma imaging. Radiographics. 2016;36(3):660–674. doi:10.1148/rg.2016150094
- Pérez-García CN, Olmos C, Vivas D, et al. IgG4-aortitis among thoracic aortic aneurysms. Heart. 2019;105(20):1583–1589. doi:10.1136/heartjnl-2018-314499
- Aranda-Michel E, Kilic A, Bianco V, Gleason TG, Sultan I. Aortitis masquerading as intramural hematoma of the ascending aorta. Ann Thorac Surg. 2019;107(5):e353. doi:10.1016/j.athoracsur.2018.12.049
- Byeon K, Han J, Kim JS, et al. Immunoglobulin G4-related periaortitis mimicking an intramural hematoma. Ann Thorac Surg. 2011;92(4):1506–1508. doi:10.1016/j.athoracsur.2011.03.141
- Svensson LG, Labib SB, Eisenhauer AC, Butterly JR. Intimal tear without hematoma: an important variant of aortic dissection that can elude current imaging techniques. Circulation. 1999;99(10):1331–1336. doi:10.1161/01.CIR.99.10.1331
- Murray JG, Manisali M, Flamm SD, et al. Intramural hematoma of the thoracic aorta: MR image findings and their prognostic implications. Radiology. 1997;204(2):349–355. doi:10.1148/radiology.204.2.9240519
- Subramaniam K, Sheppard MN. Thoracic aortic dissection. Death may not always be due to rupture with haemorrhage. Unusual complications which can be missed at autopsy. J Forensic Leg Med. 2018;54:127–129. doi:10.1016/j.jflm.2018.01.005
- Gómez-Polo JC, Vilacosta I, Aguilar-Navarro E, et al. Atrial septum hematoma-another way to die in acute aortic dissection. Circ J. 2017;81(9):1370–1372. doi:10.1253/circj.CJ-16-1205
- Maslow A, Atalay MK, Sodha N. Intramural hematoma. J Cardiothorac Vasc Anesth. 2018;32(3):1341–1362. doi:10.1053/j.jvca.2018.01.025