Abstract
Background
By increasing the intracellular prooxidant burden, gamma-glutamyltransferase (GGT) may accelerate atherosclerotic vascular disease. That noxious influence may be reflected by circulating enzyme levels, a correlate of cardiovascular risk factors, and a predictor of incident events. To evaluate this hypothesis, we tested the association between circulating GGT and common carotid intima-media thickness (CIMT), a surrogate index of systemic atherosclerotic involvement, in a large and well-characterized group of patients at risk of cardiovascular disease (CVD).
Patients
This study analyzed 548 patients with hypertension and/or diabetes and a widely prevalent history of CVD. Subjects with known hepatic disease and abnormal GGT values were excluded.
Methods
CIMT (B-mode ultrasonography) values were the mean of four far-wall measurements at both common carotids. Metabolic syndrome (MetS) was diagnosed according to National Cholesterol Education Program-Adult Treatment Panel III criteria. Due to inherent sex-related differences in GGT levels, the data were analyzed separately in males and females in samples dichotomized by the median.
Results
The age-adjusted CIMT values did not differ by GGT levels in males or females. In contrast, the carotid wall was consistently thicker in patients with a history of CVD and MetS independent of age and concurrent GGT values. In both sexes, GGT was associated with key components of the MetS such as triglycerides, fasting plasma glucose, and body mass index.
Conclusion
The data collected in this mixed group of hypertensive and/or diabetic patients with widely prevalent history of CVD do not support the concept of a direct pathophysiological link between GGT levels within reference limits and atherosclerotic involvement.
Introduction
Consistent evidence associates increased circulating serum gamma-glutamyltransferase (GGT), a parameter conventionally used for diagnosing hepatobiliary diseases and alcohol abuse,Citation1 with incident cardiovascular disease (CVD)Citation2 and major proatherogenic risk factors.Citation3 For this reason, GGT determination has been added to the array of biomarkers useful for stratifying cardiometabolic risk.Citation4 Furthermore, the enzyme’s active involvement in the atherogenic process was hypothesized on the basis of its potential to increase the intracellular prooxidant burden through the iron-reducing properties of cysteinylglycine moieties generated during GGT-catalyzed glutathione hydrolysis.Citation5 The identification of prooxidant GGT activity in atheromatous plaques of carotid and coronary arteriesCitation6 adds to the need for further clinical evaluation.
Since the first demonstration of its close correlation with directly measured arterial wall thickness, carotid intima-media thickness (CIMT) determinationCitation7 has become an easily obtained and noninvasive standard surrogate measure of systemic atherosclerosis and a prognostic and therapeutic end-point in epidemiological and pharmacological trials.Citation8 Therefore, ultrasound-derived CIMT offers a way to assess the relationship between GGT levels and atherosclerotic vascular disease. This rarely addressed issue was evaluated in this retrospective cross-sectional analysis of a large and well-characterized sample of patients screened at our institution.
Materials and methods
Patients
This study examined 548 consecutive Caucasian subjects who were referred to our department between January 2006 and June 2010 for hypertension and/or diabetes. provides clinical and demographic characteristics of the sample. Subjects with history of liver disease, self-reported alcohol abuse, history of hepatitis B or C, anticonvulsants, and microsomal enzyme-inducing drugs active on hepatic GGT releaseCitation1 were excluded. Only patients with GGT levels within the reference values of our laboratory (<60 e 40 U/L for males and females, respectively) were included in the analysis. Statin and antihypertensive (mostly angiotensin-converting enzyme inhibitors (ACEIs), angiotensin-receptor blockers (ARBs), and calcium channel blockers) treatment at the time of the visit was retrieved from the records. presents the relative percentages.
Table 1 Demographic and clinical characteristics by sex
Carotid-scanning protocol
The patients were screened while in supine position with the head and neck gently rotated 45 degrees from the side where the scanning was performed. The examination started by visualizing the longitudinal image of the midportion of the common carotid arteries in the supraclavicular region by moving and rotating the transducer until the sonographer demonstrated and marked the bifurcation with the cursor. Next, the sonographer focused on the interfaces required for the measurements of the arterial wall thickness of the common carotid artery (CCA) segment within 40 mm proximal to the carotid bulb. Patients with arteries in which the references were unidentifiable, tortuous, or calcified were excluded. All measurements were made with the image at the maximum depth of focus. The operator set up the gains and image pre- and post-processing options for every patient and for each artery to obtain the best possible image. Measurements of the distance from the leading edge of the first echogenic luminal, bright line to the leading edge of the second echogenic line were taken manually from frozen images as indicated by PignoliCitation7 in order to express the distances in mm. Scanning and measurements were obtained by a Philips ie33® instrument (Philips, Eindhoven, The Netherlands) equipped with a linear 7.5 MHz probe (axial resolution: 0.1 mm) and by the same observer (MN, within-observer variability: 5.3%, the average variation coefficient of 20 triplicate measurements in control subjects).
Biochemistry
GGT was measured colorimetrically by the nitroanilide method on a Cobas Mira Plus (Roche, Mannheim, Germany) chemistry instrument. Alanine aminotransferase (ALT), fasting plasma glucose (FPG), total cholesterol (CHOL), low-density lipoprotein-cholesterol (LDL-CHOL), high-density lipoprotein-cholesterol (HDL-CHOL), and triglycerides were assessed by automated standard enzymatic and colorimetric methods. All the samples were processed in the same laboratory, and quality control was ensured by the regional branch of the National Health System (Regione Toscana, Controllo di Qualità in Medicina di LaboratorioCitation9).
The systolic (S) and diastolic (phase V Korotkoff) blood pressure (BP) values refer to sphygmomanometric measurements taken in sitting position at the time of CIMT determination. Body weight was measured to the nearest 0.1 kg on a scale with an attached height measurement device.
Definitions
Cardiovascular disease (CVD) includes coronary heart disease (previous myocardial infarction, unstable and stable angina, coronary artery bypass graft, or angioplasty), peripheral arterial disease (previous lower limb surgery, angioplasty, or current claudication confirmed by echo-Doppler studies, angiograms, or others), and carotid disease (previous endarterectomy or carotid stenosis >50% at echo-Doppler imaging) (). Diabetes and hypertension were either diagnosed based on ongoing treatment or by the presence of fasting plasma glucose >125 mg/dL and BP >130/85 respectively. Metabolic syndrome (MetS) was defined according to National Cholesterol Education Program-Adult Treatment Panel III (NCEP-ATP III) criteriaCitation10 in the presence of at least three of the following criteria: antihypertensive treatment or BP >130/85 mmHg, triglycerides ≥150 mg/dL, HDL-C <40 mg/dL in males and <50 mg/dL in females, glucose-lowering treatment, or FPG >110 mg/dL, abdominal obesity. The thresholds for abdominal obesity were BMI ≥29.5 kg/m2 and ≥27.2 kg/m2 in men and women, respectively since those values corresponded to 102 cm and 88 cm of waist circumference in men and women, respectively, in a regression of BMI on the waist as validated previously.Citation11 Smokers were either categorized as current smokers independent of the number of cigarettes they had per day or as never/previous smokers, meaning tobacco-free for at least 6 months.
Table 2 Distribution (absolute numbers and percentages) by type of vascular disease (n = 174) in descending order of frequency
Data processing
The data were analyzed by sex-specific median GGT values (cutoffs: 15 U/L and 27 U/L for females and males, respectively). CIMT was the average of the four values measured bilaterally approximately 1 cm from the other at the far wall of the CCA, provided that these points were free of plaque. Plaques (a local thickening exceeding 1.4 mm and protruding into the lumen) were excluded from the measurements. BMI was calculated as weight/height2 (Kg/m2). For the sake of clarity, only the SBP values were reported since diastolic BP did not vary across comparisons.
Statistics
Differences in continuous and categorical variables were assessed by one-way analysis of variance and chi-square statistics, respectively, and were adjusted for age by analysis of covariance and logistic regression. Unless otherwise specified, descriptive statistics were mean ± standard deviation or median (interquartile range) for skewed data and percentages for categorical variables. The limit for statistical significance was P < 0.05.
Results
Clinical and demographic characteristics by gender
CIMT, GGT ALT, triglycerides, FPG, BMI were higher and diabetes, active smoking, history of CVD, and pharmacological treatment more frequent in males than females whereas total and fractionated CHOL showed opposite trends. Age, SBP, and history of hypertension did not differ by gender ().
Clinical and demographic characteristics by GGT status in males and females
In contrast to the homogeneous distribution of such parameters in men, thicker carotid walls (), higher SBP, and more frequent hypertension and statin treatment distinguished women with above from those below median GGT levels (). However, differences in CIMT (Age-corrected means [95% confidence interval (CI)]: 0.80 [0.77–0.83] versus 0.79 [0.76–0.81] mm) and in other parameters (data not shown) were abolished by accounting for the older age of the female subgroup (). In both sexes, above-median GGT levels were associated with higher ALT, triglycerides, FPG, and BMI ().
Figure 1 Box-and-whisker plots of carotid intima-media thickness (CIMT) by above- and below-median gamma-glutamyltransferase (GGT) levels in females (left panel) and males (right panel).
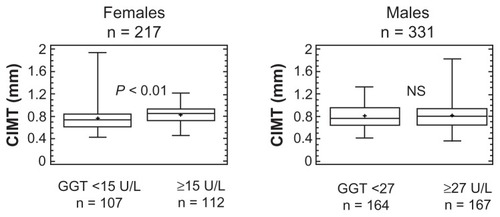
Table 3 Demographic and clinical characteristics by above- and below-median sex-specific GGT levels
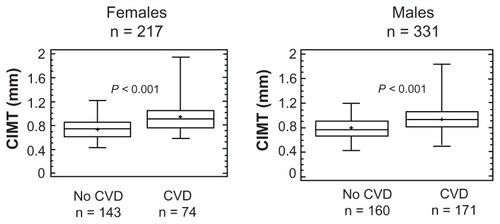
The flat behavior of CIMT by GGT levels diverged quite sharply from the carotid thickening shown by patients with a history of CVD as compared with those without, a statistically significant (P < 0.001) pattern unaffected by the adjustment for age (). Circulating GGT levels were comparable in patients with a history of CVD and not, either females (17 [9] versus 14 [8] U/L, n = 41 versus 176 respectively, NS) or males (26 [20] versus 28 [19] U/L, n = 133 versus 198 respectively, NS).
Figure 2 Box-and-whisker plots of CIMT by history of cardiovascular disease (CVD) in females (left panel) and males (right panel).
Clinical and demographic characteristics by MetS status
Besides the expected liver enzyme elevationsCitation4 and definition-relatedCitation10 modifications of the metabolic and pressor profile (), CIMT was higher in patients with MetS () and was unchanged after adjusting for GGT levels (GGT-corrected means [95% CI]: 0.82 [0.80–0.84] versus 0.88 [0.86–0.92] mm, P < 0.01).
Figure 3 Box-and-whisker plot of carotid intima-media thickness (CIMT) by National Cholesterol Education Program-Adult Treatment Panel III defined metabolic syndrome (MetS) status.Citation10
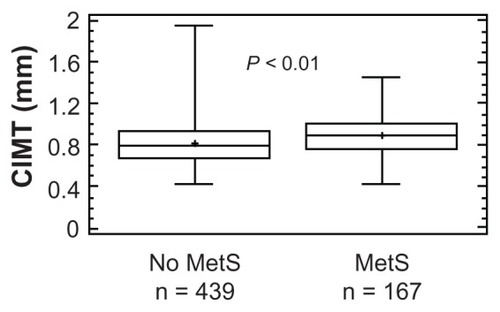
Table 4 Demographic and clinical characteristics by MetS status
Discussion
The lack of relationship between GGT and CIMT
Our cross-sectional evaluation of a large and rather heterogeneous group of hypertensive and/or diabetic patients widely affected by CVD shows a lack of association between circulating GGT levels and CIMT, a surrogate measure of systemic atherosclerosis.Citation8 This negative result was immediately evident in men and emerged quite clearly in women after accounting for the older age of those with higher GGT. That demographic influence was consistent with previous reportsCitation1 of trends toward declining values in elderly males whose large representation in our sample may explain why age and GGT showed a different association profile between sexes. One might also ask whether the effect of statins on liver enzymesCitation12 might have contributed to the divergent pattern, but this is unlikely since statin treatment did not differ by GGT levels in males, and was appropriately more frequent in older females with higher GGT levels. The strength of these findings is augmented when contrasted with the carotid thickening that characterized patients with a history of CVD, a reassuring piece of evidence in agreement with the concept of carotid imaging as an indicator of the atherosclerotic burden across different vascular beds.Citation8
Our results are inconsistent with the active contribution of GGT in the initiation and progression of atherosclerotic vascular disease, at least to the extent reflected by carotid imaging. This issue has been addressed by a few studies biased by low statistical strength of the reported correlations, limited sample size, unbalanced male-to-female ratios and, most importantly, missing adjustment for sex and age.Citation13–Citation15 This latter limitation is of particular relevance when considering the confounding effect of demographic variables on CIMT in our study. This is in agreement with Volzke et al’s study on a large sample of patients with nonalcoholic fatty liver disease (NAFLD)Citation16 in which anatomic alterations ranging from mere liver steatosis to steatohepatitis coexisted with elevated GGT and related metabolic abnormalities.Citation17,Citation18 Our conclusions are further supported by negative results reported in several series of patients with NAFLD,Citation19–Citation22 a condition that affected also an undefined but large portion of our patients, particularly those with higher ALT, a measure of hepatic fat accumulation.Citation23 It must be recognized, however, that the issue of the NAFLD as a marker of more advanced carotid atherosclerosis is controversialCitation24 and our data cannot provide any evidence in favor or against that possibility since we have no information about the liver status of our patients.
GGT, CIMT, and MetS
The clustering of elevated GGT and ALT levels with higher BMI, FPG, triglycerides, and BP by the NCEP-ATP III definition of MetSCitation10 agrees with the findings of previous epidemiological observationsCitation25 linking the liver, the primary source of those enzymes,Citation17,Citation18 to a biological phenotype at high risk of CVD and diabetes.Citation26 In concordance with previous studiesCitation27,Citation28 based on similar diagnostic criteria,Citation10 we found evidence of more advanced subclinical atherosclerosis in patients with MetS. More importantly, in light of our specific aims, the persistence of that difference after accounting for GGT implies an overcoming influence of metabolic abnormalities on atherosclerotic progression, which is fully concordant with other studies.Citation29,Citation30
Limitations of the study
The conclusions of our study must be considered in the context of some important limitations. First and more importantly, cross-sectional studies such as this one may establish associations or lack thereof, but are weak tools for assessing mechanistic links. Second, the common carotid arteries might be less prone to atherosclerosis than the bulb or the internal carotid arteriesCitation31 and the impact of cardiovascular risk factors may differ across carotid segments.Citation32 Moreover, carotid plaques, which were not considered in our study, could relate to GGT more tightly than CIMTCitation16 as a reflection of different biological and genetic determinants of the atherosclerotic process.Citation33 Third, the pervasive use of statins as well as ACEIs and ARBs – a group of drugs endowed with pleiotropic anti-inflammatory and antioxidant propertiesCitation34,Citation35 – may have obscured associations discernible in untreated conditions. That source of confounding is impossible, however, to be circumvented in retrospective studies as ours. Fourth, circulating GGT includes several heterogeneous molecular fractions that are undifferentiated by routine assays of which only the b-fraction may be associated with cardiovascular risk factors and may penetrate the atherosclerotic plaque.Citation36 Fifth, the impact of GGT on CIMT may only be evident in patients with pathological GGT elevations that were excluded from our series to avoid confounding from liver disease other than NAFLD, given the absence of ultrasound or biopsy verification. However, this possibility applies, by definition, to a minority of subjects.
In conclusion, higher GGT values bore no relationship to common carotid IMT, a surrogate measure of atherosclerotic vascular disease, in this large group of high-risk subjects. The data do not support the concept of a pathophysiological link between GGT levels within reference limits and atherosclerotic involvement although further studies are needed to evaluate this possibility.
Author contributions
MN measured CIMT, PS and CG retrieved data from clinical records, GDO supervised clinical processing, AB provided input to result interpretation, RP wrote the paper and acted as senior author.
Disclosure
The authors have no actual or potential conflict of interests including any financial, personal, or other relationships with people or organizations within 3 years of beginning the work submitted that could inappropriately influence their work.
References
- WhitfieldJBGamma glutamyl transferaseCrit Rev Clin Lab Sci20013826335511563810
- WannametheeGEbrahimSShaperAGGamma-glutamyltransferase: determinants and association with mortality from ischemic heart disease and all causesAm J Epidemiol19951426997087572939
- LeeDHJacobsDRJrGrossMGamma-glutamyltransferase is a predictor of incident diabetes and hypertension: the Coronary Artery Risk Development in Young Adults (CARDIA) StudyClin Chem2003491358136612881453
- GrundySMGamma-glutamyl transferase: another biomarker for metabolic syndrome and cardiovascular riskArterioscler Thromb Vasc Biol2007274717185620
- DrozdzRParmentierCHachadHLeroyPSiestGWellmanMGamma-glutamyltransferase-dependent generation of reactive oxygen species from a glutathione/transferrin systemFree Radic Biol Med1998257867929823544
- PaolicchiAEmdinMGhliozeniEHuman atherosclerotic plaques contain gamma-glutamyl transpeptidase enzyme activityCirculation20041091440144315037540
- PignoliPTremoliEPoliAOrestePPaolettiRIntimal plus medial thickness of the arterial wall: a direct measurement with ultrasound imagingCirculation198674139914063536154
- O’LearyDHBotsMLImaging of atherosclerosis: carotid intima-media thicknessEur Heart J2010311682168920542989
- Azienda Ospedaliero Universitaria di Careggi - Firenze S.O.D. Sicurezza e QualitàVEQ – Valutazione esterna di Qualità Available from: http://www.ao-careggi.toscana.it/crrveq/Accessed April 12, 2012
- Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in AdultsExecutive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III)JAMA20012852486249711368702
- Dell’OmoGPennoGDel PratoSMarianiMPedrinelliRDysglycaemia in non-diabetic hypertensive patients: comparison of the impact of two different classifications of impaired fasting glucose on the cardiovascular risk profileJ Hum Hypertens20092333233819078990
- BrownWVSafety of statinsCurr Opin Lipidol20081955856218957877
- YagmurJErmisNAcikgozNElevated serum gamma-glutamyl transferase activity in patients with cardiac syndrome X and its relationship with carotid intima media thicknessActa Cardiol20106551551921125972
- ErogluSSadeLEPolatEBozbasHUlusTMuderrisogluHAssociation between serum gamma-glutamyltransferase activity and carotid intima-media thicknessAngiology20116210711021220370
- NakagawaHIsogawaATateishiRSerum gamma-glutamyltransferase level is associated with serum superoxide dismutase activity and metabolic syndrome in a Japanese populationJ Gastroenterol201247187194
- VolzkeHRobinsonDMKleineVHepatic steatosis is associated with an increased risk of carotid atherosclerosisWorld J Gastroenterol2005111848185315793879
- AnguloPNonalcoholic fatty liver diseaseN Engl J Med20023461221123111961152
- VanniEBugianesiEKotronenADe MinicisSYki-JärvinenHSvegliati-BaroniGFrom the metabolic syndrome to NAFLD or vice versa?Dig Liver Dis20104232033020207596
- McKimmieRLDanielKRCarrJJHepatic steatosis and subclinical cardiovascular disease in a cohort enriched for type 2 diabetes: the Diabetes Heart StudyAm J Gastroenterol20081033029303518853970
- PetitJMGuiuBTerriatBNonalcoholic fatty liver is not associated with carotid intima-media thickness in type 2 diabetic patientsJ Clin Endocrinol Metab2009944103410619584186
- SalviPRuffiniRAgnolettiDIncreased arterial stiffness in nonalcoholic fatty liver disease: the Cardio-GOOSE studyJ Hypertens2010281699170720467324
- PoantaLIAlbuAFodorDAssociation between fatty liver disease and carotid atherosclerosis in patients with uncomplicated type 2 diabetes mellitusMed Ultrason20111321521921894292
- SchindhelmRKDiamantMDekkerJMTushuizenMETeerlinkTHeineRJAlanine aminotransferase as a marker of non-alcoholic fatty liver disease in relation to type 2 diabetes mellitus and cardiovascular diseaseDiabetes Metab Res Rev20062243744316832839
- TargherGDayCPBonoraERisk of cardiovascular disease in patients with nonalcoholic fatty liver diseaseN Engl J Med20103631341135020879883
- NilssenOFørdeOHBrennTThe Tromsø Study. Distribution and population determinants of gamma-glutamyltransferaseAm J Epidemiol19901323183261973595
- EckelRHMechanisms of the components of the metabolic syndrome that predispose to diabetes and atherosclerotic CVDProc Nutr Soc200766829517343775
- TzouWSDouglasPSSrinivasanSRIncreased subclinical atherosclerosis in young adults with metabolic syndrome: the Bogalusa Heart StudyJ Am Coll Cardiol20054645746316053958
- HassinenMKomulainenPLakkaTAMetabolic syndrome and the progression of carotid intima-media thickness in elderly womenArch Intern Med200616644444916505265
- KimHCKimDJHuhKBAssociation between nonalcoholic fatty liver disease and carotid intima-media thickness according to the presence of metabolic syndromeAtherosclerosis200920452152518947828
- KoskinenJMagnussenCGKähönenMAssociation of liver enzymes with metabolic syndrome and carotid atherosclerosis in young adults. The Cardiovascular Risk in Young Finns StudyAnn Med201244218719521254896
- FinnAVKolodgieFDVirmaniRCorrelation between carotid intimal/medial thickness and atherosclerosis: a point of view from pathologyArterioscler Thromb Vasc Biol20103017718119679833
- PolakJFPersonSDWeiGSSegment-specific associations of carotid intima-media thickness with cardiovascular risk factors: the Coronary Artery Risk Development in Young Adults (CARDIA) studyStroke20104191519910544
- SpenceJDTechnology Insight: ultrasound measurement of carotid plaque – patient management, genetic research, and therapy evaluationNat Clin Pract Neurol2006261161917057748
- Del FiorentinoACianchettiSCeliADell’OmoGPedrinelliRThe effect of angiotensin receptor blockers on C-reactive protein and other circulating inflammatory indices in manVasc Health Risk Manag2009523324219436669
- GenserBGrammerTBStojakovicTSiekmeierRMärzWEffect of HMG CoA reductase inhibitors on low-density lipoprotein cholesterol and C-reactive protein: systematic review and meta-analysisInt J Clin Pharmacol Ther20084649751018826864
- FranziniMPaolicchiAFornaciariICardiovascular risk factors and gamma-glutamyltransferase fractions in healthy individualsClin Chem Lab Med20104871371720158443