
Abstract
Platelet activation with subsequent aggregation is a complex process leading to thrombus formation, which remains a key component for atherothrombotic manifestations, in particular myocardial infarction. Therefore, antiplatelet therapies are pivotal for the treatment of these patients. Current oral antiplatelet therapies used for secondary prevention of ischemic recurrences include aspirin and adenosine diphosphate P2Y12 platelet-receptor antagonists. However, despite these therapies, patients who have experienced a myocardial infarction remain at risk for ischemic recurrences. Therefore, more aggressive secondary prevention measures have been an area of research, including identifying additional targets modulating platelet-activation and -aggregation processes. Among these, thrombin-mediated platelet activation via protease-activated receptors (PARs) has been subject to extensive clinical investigation. Several PAR-1 receptor antagonists have been developed. However, vorapaxar is the only one that has completed large-scale clinical investigation. The present manuscript will provide an overview on the role of thrombin-mediated signaling, the impact of PAR-1 blockade with vorapaxar on ischemic and bleeding outcomes, and the potential role for vorapaxar in clinical practice.
Introduction
Platelets have a crucial role in the pathogenesis of atherothrombotic disease manifestations, such as acute coronary syndrome (ACS), stroke, and peripheral artery disease (PAD).Citation1,Citation2 Multiple signaling pathways are implied in this process.Citation1,Citation2 Thromboxane (Tx) A2 and adenosine diphosphate (ADP) receptors have represented the main targets for current antiplatelet therapies used as the standard of care for patients with atherothrombotic disease manifestations.Citation3 In particular, aspirin and clopidogrel are the most commonly used antiplatelet therapies among these patients. However, despite these therapies, rates of ischemic recurrences, especially in patients with ACS, remain high.Citation4–Citation6 More potent ADP P2Y12-inhibiting strategies, such as prasugrel and ticagrelor, have been shown to reduce ischemic event rates further compared with clopidogrel among ACS patients, albeit at the expense of an increased risk of bleeding.Citation7,Citation8 These observations may occur given the impact of P2Y12-mediated signaling on modulating hemostatic processes.Citation9–Citation11 Overall, these findings have led investigations in the field to assess alternative platelet signaling pathways to target, with the goal of optimizing clinical outcomes. Among these, thrombin-mediated platelet activation via protease-activated receptors (PARs) has been subject to extensive clinical investigation. In human platelets, PAR-1 has a key role in mediating platelet activation at low concentrations of thrombin.Citation12 Several PAR-1 receptor antagonists have been developed.Citation13 However, vorapaxar is the only one that has completed large-scale Phase III clinical investigation.Citation14,Citation15 The present manuscript provides an overview of the role of thrombin-mediated signaling, the impact of PAR-1 blockade with vorapaxar on ischemic and bleeding outcomes, and the potential role for vorapaxar in clinical practice.
Mechanism of thrombin-receptor antagonism for platelet inhibition
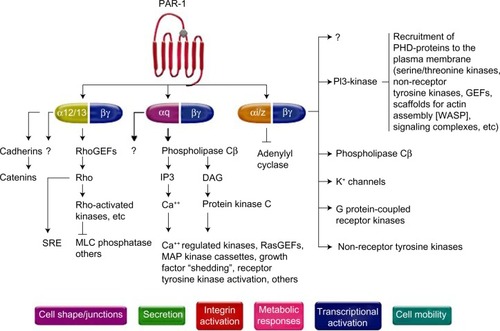
The role of PARs has been established in the field of vascular biology, atherothrombosis, and hemostasis as the receptor for thrombin, a potent agonist of platelet activation and aggregation.Citation16,Citation17 PAR is a G-protein-coupled receptor; it is constituted of a proteolytic enzyme that cleaves the extracellular loop of the receptor, and then the newly unmasked N-terminus binds to the proximally located transmembrane loop of the receptor itself.Citation18 To date, four types of human PARs have been identified (PAR-1, -2, -3, and -4), and among these, only PAR-1 and PAR-4 are expressed on human platelets.Citation19,Citation20 PAR-1 has the principal role of mediating platelet activation at low concentrations of thrombin, while PAR-4 reacts at high concentrations.Citation20–Citation22 There are several signaling pathways for thrombin to activate PAR-1 (). Once activated by thrombin, various phenotypic effects occur, which include Tx A2 production, ADP release, serotonin and adrenalin release, activation/mobilization of P-selectin and CD40 ligand, and finally platelet activationCitation16–Citation29 ().
Figure 1 Pathways of platelet protease-activated receptor (PAR)-1 activation.
Abbreviations: GEFs, guanine nucleotide exchange factors; IP3, inositol trisphosphate 3; PI3-kinase, phosphoinositide-3 kinase; MAP, mitogen activated kinase; DAG, diacylglycerol; WASP, Wiskott–Aldrich syndrome protein; SRE, serum response element; MLC, myosin light chain; PHD, prolyl hydroxylase domain.
The key difference of PAR-1 in the development of pathologic atherothrombosis, compared to normal hemostasis, is that it lacks the ability to propagate the platelet-rich thrombus beyond the initial monolayer to become an occlusive clot, which is not found in aberrantly activated PAR-1.Citation12 The prototype PAR-1 antagonist, FR 171113 was first tested in a guinea pig model.Citation30 In this study, the use of FR 171113 did not inhibit ADP- or collagen-induced platelet aggregation, suggesting that PAR-1 antagonism does not affect other platelet signaling pathways. Preclinical studies with different molecules have been subsequently tested, and include SCH 530348 (vorapaxar; Merck, Whitehouse Station, NJ, USA), SCH 205831, SCH 602539, and E 5555 (atopaxar; Eisai, Tokyo, Japan). Among these, only vorapaxar and atopaxar have been tested in Phase II studies,Citation13 and only vorapaxar has been tested in large-scale Phase III clinical investigations.Citation14,Citation15 The scope of this manuscript is to elaborate on vorapaxar. Details of other compounds go beyond the scope of this manuscript, and are described in more detail elsewhere.Citation12,Citation13
Pharmacokinetics and pharmacodynamics of vorapaxar
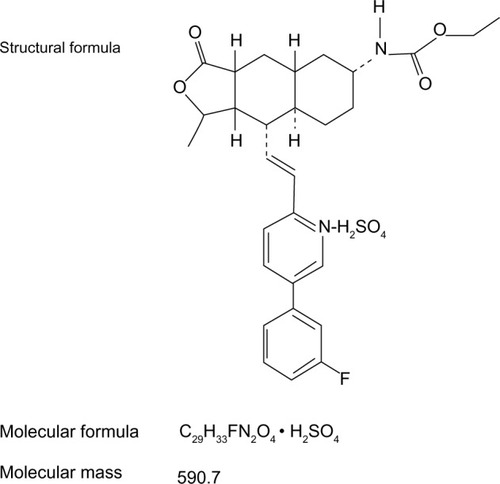
Vorapaxar (formerly known as SCH 530348) is a synthetic tricyclic 3-phenylpyridine analog of himbacine, a natural product that has been modified as a crystalline salt ().Citation12,Citation31,Citation32 It is a potent antagonist of the PAR-1 receptor, blocking thrombin-mediated platelet activation without interfering with thrombin-mediated cleavage of fibrinogen. In particular, vorapaxar is a nonprotein small molecule with high affinity, and is an orally active, competitive inhibitor of PAR-1.Citation12,Citation31,Citation32 After oral administration, this drug is absorbed rapidly with high bioavailability. In pharmacokinetic studies, vorapaxar showed a dissociation half-life as long as 20 hours, thereby providing consistent antiplatelet effects. The route of elimination is mainly feces and secondarily by urine (less than 5%).Citation17 Vorapaxar is metabolized by cytochrome P450 (CYP) 3A4; therefore, coadministration of drugs interfering with CYP 3A4 activity (such as ketoconazole or rifampin) could potentially affect its antiplatelet effects.Citation33
Figure 2 Chemical structure of vorapaxar.
In a Phase I study with 50 healthy volunteers, a single oral dose of vorapaxar (5–40 mg) was able to produce >90% mean inhibition of thrombin receptor-agonist peptide (TRAP)-induced platelet aggregation in all subjects for >72 hours, with low interindividual variability in plasma concentrations.Citation34 Another Phase I study showed that a single 40 mg dose of vorapaxar was safe and well tolerated in healthy Caucasian and Japanese subjects, exhibiting >80% inhibition of TRAP-induced platelet aggregation in both populations.Citation35,Citation36 These findings encouraged further investigation of vorapaxar in clinical settings, as follows.
Clinical trial data
Phase II
Thrombin Receptor Antagonist Percutaneous Coronary Intervention (TRA-PCI) was a Phase II, randomized, double-blind, placebo-controlled trial with vorapaxar in patients undergoing non-urgent PCI or coronary angiography with planned PCI (n=1,030).Citation37 In this trial, different loading doses of vorapaxar (10, 20, and 40 mg) were compared with matched placebo (3:1 ratio) on top of standard antiplatelet-treatment regimens, which included many patients on standard dual-antiplatelet therapy (DAPT) with aspirin and clopidogrel. The vorapaxar group, who subsequently underwent PCI (primary PCI cohort), continued taking a maintenance dose (0.5, 1, or 2.5 mg per day), and the placebo group continued placebo for 60 days. Bleeding events according to the Thrombosis In Myocardial Infarction (TIMI) scale represented the primary end point. The study showed no increased bleeding with vorapaxar (as a whole and according to each dosing regimen) compared with placebo. The secondary ischemic end point (composite of death, myocardial infarction [MI], and stroke) among PCI-treated patients (primary PCI cohort) was nonsignificantly lower with vorapaxar at each dosing regimen compared with placebo (placebo 9%, 10 mg 8%, 20 mg 5% and 40 mg 5%; odds ratio 0.67, 95% confidence interval [CI] 0.33–1.34). Overall, these findings suggest vorapaxar to have a favorable safety profile, which then led to Phase III clinical investigation.
Phase III
Two large-scale Phase III clinical studies have been conductedCitation14,Citation15: the TRACER (Thrombin Receptor Antagonist for Clinical Event Reduction in Acute Coronary Syndrome) and the TRA 2°P – TIMI 50 (Thrombin Receptor Antagonist in Secondary Prevention of Atherothrombotic Ischemic Events - Thrombolysis in Myocardial Infarction 50) trials. The key findings of these trials as well as the most recent updates in the literature derived from these pivotal investigations on vorapaxar are summarized in the following sections.
TRACER
The TRACER trial compared vorapaxar, at a loading dose of 40 mg and a daily maintenance dose of 2.5 mg thereafter, with placebo in 12,944 patients with ACS without ST-segment elevation (non-STE ACS) on top of standard treatment regimens, including DAPT with aspirin and clopidogrel.Citation14 The primary composite end point comprised death from cardiovascular causes, MI, stroke, recurrent ischemia with hospitalization, or urgent coronary revascularization. The primary safety end points were a composite of moderate or severe bleeding according to the Global Use of Strategies to Open Occluded Coronary Arteries (GUSTO) classification and clinically significant bleeding according to the TIMI classification, defined as TIMI major or minor bleeding or bleeding that required unplanned medical or surgical treatment or laboratory evaluation.Citation14 The primary composite ischemic end point was nonsignificantly lower in patients randomized to vorapaxar compared with placebo (18.5% versus 19.9%, hazard ratio [HR] 0.92, 95% CI 0.85–1.01; P=0.07) at 2-year follow-up. A key secondary ischemic end point represented by the composite of death from cardiovascular causes, MI, or stroke occurred significantly less frequently with vorapaxar (14.7% versus 16.4%, HR 0.89, 95% CI 0.81–0.98; P=0.02) (). However, this occurred at the expense of increased bleeding (GUSTO moderate-to-severe bleeding) with vorapaxar compared with placebo (7.2% versus 5.2%, HR 1.35, 95% CI 1.16–1.58; P<0.001). Importantly, the rate of intracranial bleeding was over threefold higher with vorapaxar (1.1% versus 0.2%, HR 3.39, 95% CI 1.78–6.45; P<0.001) (). In January 2011, due to these safety concerns, the Data and Safety Monitoring Board (DSMB) decided to terminate the study prematurely.Citation38 Overall, the results from this trial led to the conclusion that antiplatelet therapy with vorapaxar on top of standard antiplatelet-treatment regimens, including mostly patients on DAPT, provides only marginal ischemic beneficial effects, and is hampered by significantly increased bleeding rates, including intracranial hemorrhage, in patients with non-STE ACS.Citation14 However, important predefined subgroup and post hoc analysis have been reported, providing important insights on the impact of vorapaxar on clinical outcomes.
Table 1 Efficacy and safety end points in the TRACER (at 2 years) trial
MI analysis
A key driver of the reduction of ischemic events with vorapaxar was from MI rates. A blinded, independent central end-point adjudication committee prospectively defined and classified MI according to the universal MI definition.Citation39,Citation40 During follow-up, 1,580 MIs occurred in 1,319 patients. The majority (n=1,025, 64.9%) were type 1 (spontaneous) MI, followed by type 4a (periprocedural, n=352, 22.3%). Vorapaxar reduced the hazard of first MI of any type by 12% (HR 0.88, 95% CI 0.79–0.98; P=0.021) and the hazard of total MIs by 14% (HR 0.86, 95% CI 0.77–0.97; P=0.014), and these effects were sustained over time.Citation39 Of note, vorapaxar reduced type 1 MI by 17% (HR 0.83, 95% CI 0.73–0.95; P=0.007), whereas there was no significant effect on type 4a MI (HR 0.90, 95% CI 0.73–1.12; P=0.35) compared with placebo, suggesting that vorapaxar is beneficial for the prevention of clinically relevant MI. Although exploratory in nature, this post hoc analysis suggests the potential role of vorapaxar in the management of patients with ACS to prevent future MI events.
CABG analysis
The TRACER trial was selectively performed in non-STE ACS patients. Therefore, the management of these patients could vary and include patients undergoing PCI (placebo 57.4% versus vorapaxar 58.1%), medical management (placebo 32.2% versus vorapaxar 32.0%), and coronary artery bypass graft (CABG; placebo 10.4% versus vorapaxar 9.9%).Citation14 Most recently, an analysis of the subgroup of patients undergoing CABG (n=1,312, 10.1% of total TRACER population) during the index hospitalization was reported.Citation41 This analysis showed that vorapaxar was associated with a 45% relative risk reduction in the primary end point compared with placebo (HR 0.55, 95% CI 0.36–0.83; P=0.005), with a positive interaction among these subjects (P=0.012). Notably, CABG-related TIMI major bleeding was numerically higher with vorapaxar, but not significantly different between vorapaxar and placebo (9.7% versus 7.3%, HR 1.36, 95% CI 0.92–2.02; P=0.12), without excess in fatal bleeding (0% versus 0.3%) or need for reoperation (4.7% versus 4.6%).Citation41 These findings suggest that CABG patients in whom thrombin generation is known to be accelerated may represent a potential target for the use of vorapaxar, thereby increasing the risk of thrombotic complications such as graft occlusion or native coronary thrombosis.Citation42–Citation44 However, there are several considerations to be made of this analysis.Citation45 The lack of differences in bleeding outcomes may be simply attributed to the small sample size of the CABG cohort (10.8% of TRACER population), making it insufficiently powered to draw any definitive conclusions. Clopidogrel was also held prior to CABG, with only 39% receiving the drug within 5 days of surgery. Upon discharge, clopidogrel use in this CABG cohort was only 18%, compared with 84% in the non-CABG cohort. Therefore, the benefits observed with vorapaxar may be attributed to the fact that the control arm was not on optimal secondary prevention therapy. Whether CABG patients represent a niche specific for vorapaxar requires further investigation.
PCI analysis
The safety and efficacy of vorapaxar were also assessed in a subgroup of TRACER patients who underwent PCI as a primary treatment strategy, in which data were analyzed according to stent type.Citation46 Among 12,944 TRACER patients, 7,479 (58%) underwent PCI, with either bare-metal stent (BMS) or drug-eluting stent (DES) during index hospitalization. The type of stent (BMS or DES) used in the vorapaxar and placebo groups was well balanced. In line with current clinical practice, the duration of thienopyridine therapy was longer among patients treated with DES than those with BMS (median 221 versus 133 days). At 1 year, the primary end point occurred in 10.4% of patients with vorapaxar versus 10.6% of those with placebo (HR 0.96, 95% CI 0.83–1.10; P-interaction for primary end point =0.605). The key secondary end point (cardiovascular death, MI, or stroke) occurred in 6.8% with vorapaxar and 7.3% with placebo (HR 0.89, 95% CI 0.75–1.05; P-interaction for key secondary end point =0.72). The rate of Academic Research Consortium-defined definite or probable stent thrombosis was no different between vorapaxar and placebo (1.7% versus 1.5%, HR 1.12, 95% CI 0.78–1.62; P=0.54).Citation14 There was a trend for interaction on cardiovascular death, MI, and stroke between stent type, with patients receiving BMS showing a relatively greater effect from vorapaxar (HR 0.70 versus 0.96; P-interaction =0.069).Citation46 GUSTO moderate/severe bleeding was increased overall with vorapaxar, with no statistical interaction (P-interaction =0.316), although the relative increase appeared less with BMS (HR 1.27, 95% CI 0.85–1.90) than with DES (HR 1.70; 95% CI 1.14–2.53), likely attributed to the different duration in clopidogrel use.
Analysis according to ischemic and bleeding risk
A recent post hoc analysis evaluated the risk–benefit profile of vorapaxar by categorizing patients according to their risk of ischemic events and bleeding complications.Citation47 In particular, patients were categorized into four groups: low bleeding/low ischemia, low bleeding/high ischemia, high bleeding/low ischemia, and high bleeding/high ischemia. The risk of bleeding and ischemia were derived post hoc from the TRACER population. The net benefit, defined as the difference in ischemic and bleeding event rates, was assessed. In this study, a large proportion of patients were categorized as low bleeding/low ischemia risk (63%), in whom there was a neutral effect with vorapaxar (net benefit −0.1%). Regardless of ischemic risk (high or low), patients at high bleeding risk (cumulatively representing 11% of the total population) had more harm than benefit (net benefit ranged from −2.93% to −3.83%). Ultimately, among patients categorized as low bleeding/high ischemia risk, representing 26% of the TRACER population, there was a net benefit (+2.76%) with vorapaxar. The results of this analysis, although post hoc in nature, do emphasize the potential for harm of vorapaxar among patients at high risk of bleeding, irrespective of their ischemic risk, but also suggest a potential role for vorapaxar in patients at low risk of bleeding and high risk of ischemic events. However, the risk score used in this analysis needs to be externally validated, and dedicated prospective studies need to be performed to support these post hoc findings.
Impact of thienopyridines
Another analysis that was performed to elucidate factors affecting the risk of bleeding in patients treated with vorapaxar was an assessment of patients on DAPT. In the TRACER trial 11,307 (87%) patients were on DAPT with aspirin and a thienopyridine, mostly represented by clopidogrel (91.8%), whereas 1,637 (13%) patients were not on a thienopyridine. Patients without thienopyridine therapy had a lower risk of bleeding, as assessed by all bleeding scales: GUSTO moderate/severe (HR thienopyridine, 1.45 versus no thienopyridine, 0.95; P-interaction =0.044), TIMI significant (HR 1.46 versus 1.24; P-interaction =0.25), GUSTO severe (HR 1.71 versus 1.43; P-interaction =0.60), and TIMI major (HR 1.62 versus 1.15; P-interaction =0.25).Citation48 The high rate of thienopyridine use is in line with the fact that the TRACER trial enrolled patients with ACS, many undergoing PCI, in whom the use of DAPT forms part of the standard of care. It is important to note that the design of the TRACER trial was to evaluate the impact of more comprehensive platelet blockade by adding vorapaxar to standard antiplatelet-treatment regimens, including DAPT. Therefore, based on this analysis, we cannot infer a potential for the use of vorapaxar without a thienopyridine, because this would require a dedicated trial.
Impact of aspirin dosing
Aspirin-dosing regimens have been a subject of interest in recent years. In particular, studies have shown that high-dose aspirin does confer added benefit, but can increase the risk of bleeding when used in combination with clopidogrel.Citation49,Citation50 Although aspirin dosing has not been shown to impact outcomes in patients treated with prasugrel,Citation51 reduced ischemic benefits have been shown in ticagrelor-treated patients when high-dose (≥300 mg) aspirin was used.Citation52 This has indeed raised interest in understanding the impact of aspirin dosing on clinical outcomes in patients treated with vorapaxar in the TRACER trial.Citation53 Overall, 96% (n=12,515) of the entire TRACER population was on aspirin at randomization at the following dosing regimens: low dose (≤100 mg, n=7,523, 60%), medium dose (100–300 mg, n=1,049, 8.4%), and high dose (≥300 mg, n=3,943, 31%). Compared with low-dose aspirin, high-dose aspirin was associated with a trend to a higher hazard of bleeding (adjusted HR for GUSTO severe bleeding: 1.88 [high dose] versus 1.63 [low dose]; P-interaction=0.954) and less efficacy (adjusted HR for primary efficacy end-point event: 1.05 [high dose] versus 0.90 [low dose]; P-interaction=0.140) with vorapaxar compared with placebo, although this did not reach statistical significance.Citation53
Pharmacodynamic substudy
A pharmacodynamic substudy enrolling a total of 249 patients in TRACER was conducted.Citation54 Pharmacodynamic assessments were conducted at baseline and 1 month after study enrollment in patients on aspirin and clopidogrel, and included light-transmission aggregometry following stimuli with a variety of agonists (20 μM ADP, 15 μM TRAP, and combination of 2.5 μg/mL collagen-related peptide, 5 μM ADP, and 15 μM TRAP (CAT)) and vasodilator-stimulated phosphoprotein (VASP).Citation54 TRAP and CAT-induced platelet aggregation were significantly inhibited with vorapaxar compared with placebo, while nonsignificant reductions in platelet aggregation were observed following ADP stimuli. The platelet-reactivity index determined by VASP, which is regarded as most specific to P2Y12-receptor function, was significantly lower in both treatment arms at 1 month compared with baseline, although numerically lower in the vorapaxar group. These results suggest that PAR-1 receptor inhibition mediated by vorapaxar may have some synergistic effects on P2Y12 receptor-mediated signaling. This supports prior studies suggesting an interplay between these two pathways,Citation55 which can lead to enhanced P2Y12-inhibitory effects in patients concomitantly treated with vorapaxar and clopidogrel.Citation54
TRA 2°P – TIMI 50
The TRA 2°P – TIMI 50 trial was a secondary prevention study that enrolled 26,449 patients with atherothrombotic disease.Citation15 Eligible patients had to have a history of atherosclerosis, which was defined as a spontaneous MI or ischemic stroke within the previous 2 weeks to 12 months or PAD associated with a history of intermittent claudication in conjunction with either ankle-brachial index of less than 0.85 or previous revascularization for limb ischemia. Patients were randomized to receive vorapaxar (2.5 mg daily dose) or matching placebo on top of standard-of-care therapy, which could include aspirin and/or clopidogrel, with an expected follow-up period up to 30 months.Citation15 The primary end point was determined as the composite of death from cardiovascular causes, MI, or stroke. After 3 years, the primary end point was achieved, with lower event rate with vorapaxar compared with placebo (9.3% versus 10.5%, HR 0.87, 95% CI 0.80–0.94; P<0.001). In addition, a key secondary end point represented by the composite of cardiovascular death, MI, stroke or recurrent ischemia leading to revascularization also occurred less frequently with vorapaxar (11.2% versus 12.4%, HR 0.88, 95% CI 0.82–0.95; P=0.001). The ischemic benefit observed with vorapaxar was driven by a reduction in MI rates (5.2% versus 6.1%, HR 0.83, 95% CI 0.74–0.93; P=0.001) (). There was a trend towards a positive interaction (P=0.058) among patients who had a prior MI (0.80 [0.72–0.89]) as a qualifying event to enter the study compared with patients with a prior stroke (1.03 [0.85–1.26]) or established PAD (0.94 [0.78–1.14]). The details of these subgroups are described below. However, at a median of 24 months of follow-up after completion of enrollment, the DSMB of TRA 2°P – TIMI 50 reported an excess of intracranial bleeding in patients with a history of stroke in the vorapaxar group, and recommended discontinuation of the drug in all patients with previous stroke, including those with a new stroke during the trial. The DSMB also recommended continuation of the trial in patients without a history of stroke.Citation15 After 3 years, there was increased bleeding (GUSTO moderate and severe) with vorapaxar compared with placebo (4.2% versus 2.5%, HR 1.66, 95% CI 1.43–1.93; P=0.001). The rate of intracranial bleeding was almost twofold higher with vorapaxar (1.0% versus 0.5%, HR 1.94, 95% CI 1.39–2.70; P<0.001) (). Similarly to the TRACER trial, there were important analyses deriving from the TRA 2°P trial that are useful for understanding the potential role of vorapaxar as an adjunct antiplatelet therapy for secondary prevention of ischemic events.
Table 2 Efficacy and safety end points in the TRA 2°P – TIMI 50 (at 3 years) trial
Analysis in patients with prior stroke
A total of 4,883 patients enrolled in TRA 2°P had a history of prior ischemic stroke.Citation56 In these patients, vorapaxar was associated with an increased risk of intracranial hemorrhage compared with placebo (2.5% versus 1.0%, HR 2.52, 95% CI 1.46–4.36; P<0.001), as well as GUSTO moderate and severe bleeding (4.2% versus 2.4%, HR 1.93, 95% CI 1.33–2.79; P<0.001). This occurred without any significant improvement in the primary ischemic end point (13.0% versus 11.7%, P=0.75), including ischemic stroke (8.6% versus 7.1%, HR 0.99, 95% CI 0.78–1.25; P=0.90).Citation56 Overall, these data indicate the potential for harm with vorapaxar in patients with prior stroke, discouraging the potential role of this agent in this setting.Citation56
Analysis in patients with prior MI
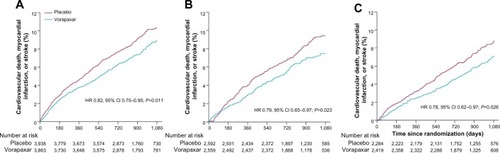
Patients with a previous MI represented the largest subgroup of subjects enrolled in the trial (n=17,779 patients, 67% of the entire TRA 2°P – TIMI 50 population), and drove most of the benefit with vorapaxar compared with patients with prior stroke or PAD (P-interaction =0.058). In this cohort of patients, the benefit of vorapaxar on reducing the primary ischemic end point was more profound compared with placebo (8.1% versus 9.7%, HR 0.80, 95% CI 0.72–0.89; P<0.0001) ().Citation57 Furthermore, this benefit was consistent regardless of qualifying MI from the time of randomization: <3 months (HR 0.82, 95% CI 0.70–0.95; P=0.011), 3–6 months (HR 0.79, 95% CI 0.65–0.97; P=0.023), and >6 months (HR 0.78, 95% CI 0.62–0.97; P=0.026) ().Citation57 This was also confirmed in a landmark analysis assessing patients before (3.2% versus 4.0%, HR 0.79, 95% CI 0.67–0.92; P=0.003) and after 1 year (5.5% versus 6.5%, HR 0.82, 95% CI 0.71–0.94; P=0.004) from randomization. These findings were consistent in the all key subgroups, including qualifying MI (non-ST-elevation MI or ST-elevation MI, with or without thienopyridine use, with or without prior stent).
Figure 3 Kaplan–Meier curve of estimated occurrence of cardiovascular death, myocardial infarction, or stroke in TRA 2°P – TIMI 50 prior myocardial infarction cohort.
Abbreviations: HR, hazard ratio; CI, confidence interval; TIMI, Thrombolysis in Myocardial Infarction.
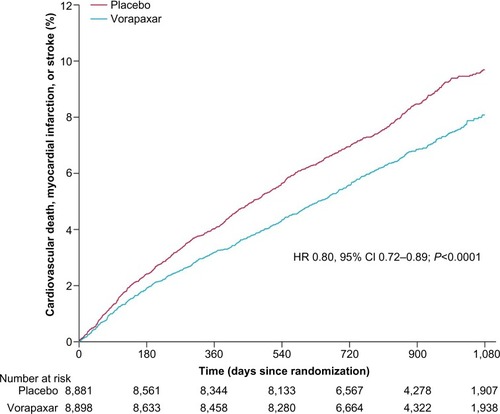
Figure 4 Kaplan–Meier estimates of cardiovascular death, myocardial infarction, or stroke according to time from qualifying myocardial infarction to randomization: <3 months (A), 3–6 months (B), and >6 months (C) in the TRA 2°P–TIMI 50 prior myocardial infarction cohort.
Abbreviations: HR, hazard ratio; CI, confidence interval; TIMI, Thrombolysis in Myocardial Infarction.
However, GUSTO moderate or severe bleeding was more common in the vorapaxar group than the placebo group (3.4% versus 2.1%, HR 1.61, 95% CI 1.31–1.97; P<0.0001). Similarly, TIMI non-CABG major (2.2% versus 1.6%, HR 1.29, 95% CI 1.02–1.64; P=0.033) and TIMI clinically significant bleeding (15.1% versus 10.4%, HR 1.49, 95% CI 1.36–1.63; P<0.0001) were also increased with vorapaxar.Citation57 However, there was only a trend for increased intracranial bleeding with the vorapaxar group, which was infrequent overall (0.6% versus 0.4%, HR 1.54, 95% CI 0.96–2.48; P=0.076), and there were no differences in fatal bleeding (0.2% versus 0.1%, HR 1.56, 95% CI 0.67–3.60; P=0.30). The net clinical outcome (presented as a composite of primary efficacy outcome and GUSTO moderate or severe bleeding) was in favor of vorapaxar compared with placebo (12.5% versus 13.4%, HR 0.91, 95% CI 0.84–0.99; P=0.038).Citation57
A further analysis of the MI cohort assessed outcomes excluding patients at high risk of bleeding. In particular, patients with prior transient ischemic attack/stroke, <60 kg, and >75 years of age (factors that in another pivotal trial of prasugrel in ACS patients were shown to be associated with an increased risk of bleedingCitation6) were identified. In the TRA 2°P trial, these subjects also had high rates of bleeding overall, and rates were further increased among patients treated with vorapaxar compared with placebo (6.9% versus 3.9%). In an analysis excluding such patients (n=14,909), known as a low-bleeding-risk cohort, the primary combined ischemic end point was significantly reduced with vorapaxar compared with placebo (6.8% versus 8.6%, HR 0.75, 95% CI 0.66–0.85; P<0.0001), and there was also a significant reduction in cardiovascular death (1.5% versus 2.0%, HR 0.73, 95% CI 0.56–0.95; P=0.02). GUSTO moderate or severe bleeding was lower than in the overall trial, although still higher with vorapaxar than placebo (2.7% versus 1.8%).Citation59 Overall, this analysis conducted among patients who were randomized in the TRA 2°P trial indicates that among appropriately selected patients, prolonged treatment with vorapaxar when added to aspirin with or without a thienopyridine may be beneficial for long-term secondary prevention in patients with prior MI.
Diabetic subgroup analysis
Another subgroup analysis evaluated patients with prior MI according to the presence or absence of diabetes mellitus (DM).Citation58 In this analysis, patients with DM (n=3,936) had a higher risk of both ischemic and bleeding events compared with non-DM (n=13,843) subjects, consistent with prior investigations. Vorapaxar showed consistent effects on reducing ischemic event rates, irrespective of DM status (P-interaction =0.51). In particular, vorapaxar reduced adverse events compared with placebo patients with DM (12.6% versus 15.7%, HR 0.77; P=0.004) and without DM (6.8% versus 7.9%, HR 0.83; P=0.005). The benefit of vorapaxar in patients with DM was driven by a reduction in MI (8.6% versus 11.4%, HR 0.73, 95% CI 0.59–0.91; P=0.01, P-interaction =0.38), and severe recurrent ischemia (3.9% versus 5.6%; HR 0.63, 95% CI 0.46–0.86; P=0.004, P-interaction =0.02). GUSTO moderate/severe bleeding was increased in DM patients (4.7% versus 2.8%, HR 1.59, 95% CI 1.09–2.32; P=0.02) and non-DM (3.0% versus 1.9%, 95% CI 1.27–2.06, HR 1.62; P<0.001) patients treated with vorapaxar than placebo, which was not different between DM and non-DM patients (HR 1.59 versus 1.62, P-interaction =0.95).Citation58
PAD subgroup analysis
The PAD cohort of the TRA 2°P trial represented 14.3% of the study population (n=3,787). Vorapaxar failed to reduce the primary efficacy end point compared with placebo (11.3% versus 11.9%, HR 0.94, 95% CI 0.78–1.14; P=0.53).Citation59 However, vorapaxar did reduce the rate of hospitalization for acute limb ischemia (2.3% versus 3.9%, HR 0.58, 95% CI 0.39–0.86; P=0.006) and peripheral artery revascularization (18.4% versus 22.2%, HR 0.84, 95% CI 0.73–0.97; P=0.017). This occurred at the expense of more frequent GUSTO moderate and severe bleeding (7.4% versus 4.5%, HR 1.62, 95% CI 1.21–2.18; P=0.001).Citation59 Given that PAR-1 receptors are also present on a number of cells (including endothelial cells) other than platelets, it could be hypothesized that these study findings may be attributed to an effect of vorapaxar on vascular remodeling and vascular perfusion.Citation59 However, these findings warrant further investigation.
Impact of thienopyridines
In contrast to TRACER, in the TRA 2°P study comparing patients with and without thienopyridine (n=15,356 [58%] versus n=11,093 [42%]), there were no differences in bleeding complications among patients treated with vorapaxar.Citation60 However, this may be attributed to differences in baseline characteristics. In fact, in TRACER patients presented with an ACS leading to early use of DAPT, which occurred in approximately nearly 90% of patients.
Impact of aspirin dosing
In the substudy of TRA 2°P – TIMI 50 by Scirica et al, including patients with prior MI, they divided the group according to each different dose of aspirin (<100 mg, 100–162 mg, >162 mg). A total of 6,988 patients (40%) received <100 mg aspirin daily, 7,704 patients (44%) 100–162 mg, and 2,755 patents (16%) >162 mg. Of note, the relative risk of bleeding was not higher with vorapaxar at the higher aspirin doses.Citation61 Apparently, the different criteria of aspirin doses in both the TRACER and TRA 2°P – TIMI 50 studies influenced the bleeding outcome. As we mentioned before, low-dose aspirin would be an appropriate option with the combined use of vorapaxar.
Conclusion and future directions
Patients with MI remain at risk for ischemic recurrences, underscoring the need for aggressive secondary preventive measures. Intensifying antithrombotic treatment regimens by means of using more potent P2Y12-receptor antagonists,Citation6,Citation7 adding an anticoagulant agent to standard DAPT,Citation62–Citation64 or adding a third antiplatelet agentCitation14,Citation15,Citation65 have all represented treatment strategies tested in clinical trials. While these strategies aim to reduce ischemic recurrences, they all come at the risk of increased bleeding complications. Vorapaxar has been tested as an add-on strategy for patients on standard antiplatelet-treatment regimens, mostly represented by aspirin and clopidogrel. The clinical trial data clearly indicate a potential for harm in certain subgroups, such as patients with a prior cerebrovascular event, but also indicate subjects, such as those with prior MI, in whom there may be adjunctive benefit. Whether findings from key subgroups of patients identified from large clinical trial data can be translated into clinical practice remains unknown at this time, and will require experience from real-world clinical practice. Most recently, vorapaxar has been recommended by the US Food and Drug Administration Drug Advisory Committee for clinical use in the management of a select group of patients with a history of MI, excluding those with a history of stroke, transient ischemic attack, intracranial hemorrhage, or active pathologic bleeding.Citation66 In this context, vorapaxar will represent an agent to add to the armamentarium of agents used to reduce the long-term risk of MI patients. Indeed, further studies are warranted, although the current evidence suggests vorapaxar is most likely to have a niche use after careful patient selection, in light of the availability of other novel antiplatelet therapies that have also been shown to reduce the risk of recurrent MI.Citation67
Disclosure
DJA received payment as an individual for: consulting fees or honoraria from Bristol-Myers Squibb, Sanofi-Aventis, Eli Lilly, Daiichi Sankyo, The Medicines Company, AstraZeneca, Merck, Evolva, Abbott Vascular, and PLx Pharma; participation in review activities from Johnson and Johnson, St Jude, and Sunovion; institutional payments for grants from Bristol-Myers Squibb, Sanofi-Aventis, GlaxoSmithKline, Otsuka, Eli Lilly, Daiichi Sankyo, The Medicines Company, AstraZeneca, Evolva, and Gilead; and has other financial relationships with Esther and King Biomedical Research Grant. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed. No writing assistance was utilized in the production of this manuscript.
References
- DavìGPatronoCPlatelet activation and atherothrombosisN Eng J Med20073572424822494
- AngiolilloDJUenoMGotoSBasic principles of platelet biology and clinical implicationsCirc J201074459760720197627
- UenoMKodaliMTello-MontoliuAAngiolilloDJRole of platelets and antiplatelet therapy in cardiovascular diseaseJ Atheroscler Thromb201118643144221427504
- AngiolilloDJThe evolution of antiplatelet therapy in the treatment of acute coronary syndromes: from aspirin to the present dayDrugs201272162087211623083110
- AngiolilloDJFernandez-OrtizABernardoEVariability in individual responsiveness to clopidogrel: clinical implications, management, and future perspectivesJ Am Coll Cardiol200749141505151617418288
- TantryUSBonelloLAradiDConsensus and update on the definition of on-treatment platelet reactivity to adenosine diphosphate associated with ischemia and bleedingJ Am Coll Cardiol201362242261227324076493
- WiviottSDBraunwaldEMcCabeCHPrasugrel versus clopidogrel in patients with acute coronary syndromesN Engl J Med2007357202001201517982182
- WallentinLBeckerRCBudajATicagrelor versus clopidogrel in patients with acute coronary syndromesN Engl J Med2009361111045105719717846
- LeonCAlexMKlockeAPlatelet ADP receptors contribute to the initiation of intravascular coagulationBlood2004103259460012969982
- van der MeijdenPEFeijgeMAGiesenPLHuijbertsMvan RaakLPHeemskerkJWPlatelet P2Y12 receptors enhance signalling towards procoagulant activity and thrombin generation. A study with healthy subjects and patients at thrombotic riskThromb Haemost20059361128113615968399
- AngiolilloDJCapranzanoPDesaiBImpact of P2Y(12) inhibitory effects induced by clopidogrel on platelet procoagulant activity in type 2 diabetes mellitus patientsThromb Res2009124331832219012950
- AngiolilloDJCapodannoDGotoSPlatelet thrombin receptor antagonism and atherothrombosisEur Heart J2010311172819948715
- CapodannoDBhattDLGotoSSafety and efficacy of protease-activated receptor-1 antagonists in patients with coronary artery disease: a meta-analysis of randomized clinical trialsJ Thromb Haemost201210102006201522845871
- TricociPHuangZHeldCThrombin-receptor antagonist vorapaxar in acute coronary syndromesN Engl J Med20123661202322077816
- MorrowDABraunwaldEBonacaMPVorapaxar in the secondary prevention of atherothrombotic eventsN Engl J Med2012366151404141322443427
- MartorellLMartínez-GonzálezJRodríguezCGentileMCalvayracOBadimonLThrombin and protease-activated receptors (PARs) in atherothrombosisThromb Haemost200899230531518278179
- UenoMFerreiroJLAngiolilloDJMechanism of action and clinical development of platelet thrombin receptor antagonistsExpert Rev Cardiovasc Ther2010881191120020670195
- CoughlinSRProtease-activated receptors in hemostasis, thrombosis and vascular biologyJ Thromb Haemost2005381800181416102047
- KahnMLZhengYWHuangWA dual thrombin receptor system for platelet activationNature199839466946906949716134
- VuT-KHHungDTWheatonVICoughlinSRMolecular cloning of a functional thrombin receptor reveals a novel proteolytic mechanism of receptor activationCell1991646105710681672265
- KahnMLNakanish-MatsuiMShapiroMJIshiharaHCoughlinSRProtease-activated receptors 1 and 4 mediate activation of human platelets by thrombinJ Clin Invest1999103687988710079109
- XuWFAndersonHWhitemoreTECloning and characterization of human protease-activated receptor 4Proc Natl Acad Sci U S A19989512664266469618465
- HenriksenRAHanksVKPAR-4 agonist AYPGKF stimulates thromboxane production by human plateletsArterioscler Thromb Vasc Biol200222586186612006403
- CovicLSinghCSmithHKuliopulosARole of PAR4 thrombin receptor in stabilizing platelet-platelet aggregates as revealed by a patient with Hermansky-Pudlak syndromeThromb Haemost200287472272712008957
- LovaPCampusFLombardiRContribution of protease-activated receptors 1 and 4 and glycoprotein Ib-IX-V in the G(i)-independent activation of platelet Rap1B by thrombinJ Biol Chem200427924252992530615078882
- SmithCCWilsonAPPrichardBNBetteridgeDJStimulus-induced release of endogenous catecholamines from human washed plateletsClin Sci (Lond)19867054955003698518
- HennVSlupskyJRGrafeMCD40 ligand on activated platelets triggers an inflammatory reaction of endothelial cellsNature199839166675915949468137
- StenbergPEMcEverRPShumanMAJacquesYVBaintonDFA platelet alpha-granule membrane protein (GMP-140) is expressed on the plasma membrane after activationJ Cell Biol198510138808862411738
- OffermannsSToombsCFHuYHSimonMIDefective platelet activation in G alpha(q)-deficient miceNature199738966471831869296496
- KatoYKitaYHirasawa-TaniyamaYInhibition of arterial thrombosis by a protease-activated receptor 1 antagonist, FR171113, in the guinea pigEur J Pharmacol20034732–316316912892834
- ChackalamannilSDaviesRJAsberomTDollerDLeoneDA highly efficient total synthesis of (+)-himbacineJ Am Chem Soc19961184098129813
- DollerDChakalamannilSCzarnieckiMMcQuadeRRupertoVDesign, synthesis, and structure-activity relationship studies of himbacine derived muscarinic receptor antagonistsBioorg Med Chem Lett19999690190610206558
- XiaYChackalamannilSGreenleeWJDiscovery of a vorapaxar analog with increased aqueous solubilityBioorg Med Chem Lett201020226676667920888225
- KosoglouTReydermanLTiessenRTRAP-induced platelet aggregation following single and multiple rising doses of SCH 530348, a novel thrombin receptor antagonist, in healthy volunteersPharmacol Ther200985Suppl 1S21
- KosoglouTReydermanLTiessenRGPharmacodynamics and pharmacokinetics of the novel PAR-1 antagonist vorapaxar (formerly SCH 530348) in healthy subjectsEur J Clin Pharmacol201268324925821935705
- KosoglouTReydermanLKasserraCNo differences in the pharmacodynamics and pharmacokinetics of the thrombin receptor antagonist vorapaxar between healthy Japanese and Caucasian subjectsEur J Clin Pharmacol201268329130021969227
- BeckerRCMoliternoDJJenningsLKSafety and tolerability of SCH 530348 in patients undergoing non-urgent percutaneous coronary intervention: a randomized, double-blind, placebo-controlled phase II studyLancet2009373966791992819286091
- Business WireMerck says additional information provided to investigators in clinical study of vorapaxar2011 Available from: http://www.businesswire.com/news/home/20110119006900/en/Merck-Additional-Information-Investigators-Clinical-Study-VorapaxarAccessed January 3, 2014
- LeonardiSTricociPWhiteHDEffect of vorapaxar on myocardial infarction in the thrombin receptor antagonist for clinical event reduction in acute coronary syndrome (TRACER) trialEur Heart J201334231723173123530022
- ThygesenKAlpertJSJaffeASSimoonsMLChaitmanBRWhiteHDThird universal definition of myocardial infarctionJ Am Coll Cardiol201260161581159822958960
- WhellanDJTricociPChenEVorapaxar in acute coronary syndrome patients undergoing coronary artery bypass graft surgery: subgroup analysis from the TRACER trialJ Am Coll Cardiol Epub1162013
- BoyleEMJrLilleSTAllaireEClowesAWVerrierEDEndothelial cell injury in cardiovascular surgery: atherosclerosisAnn Thorac Surg19976338858949066432
- ReillyCFMcFallRCPlatelet-derived growth factor and transforming growth factor beta regulate plasminogen activator inhibitor-1 synthesis in vascular smooth muscle cellsJ Biol Chem199126615941994272033043
- VerrierEDBoyleEMJrEndothelial cell injury in cardiovascular surgeryAnn Thorac Surg19966239159228784042
- Ben-YehudaOVorapaxar in patients undergoing CABG: insights from a subgroup analysisJ Am Coll Cardiol Epub1162013
- ValgimigliMTricociPHuangZVorapaxar, a platelet thrombin-receptor antagonist, in patients with non-ST-segment elevation acute coronary syndrome undergoing percutaneous coronary intervention: results from the TRACER trialCirculation2012126A18805
- TricociPHuangZvan de WerfFNet clinical benefit of vorapaxar in NSTE ACS: role of ischemic and bleeding risk stratificationCirculation2012126A19049
- TricociPHuangZvan de WerfFVorapaxar with and without thienopyridine use in acute coronary syndromes: results from the TRACER trialEur Heart J20123349549621951627
- PetersRJMehtaSRFoxKAEffects of aspirin dose when used alone or in combination with clopidogrel in patients with acute coronary syndromes: observations from the Clopidogrel in Unstable angina to prevent Recurrent Events (CURE) studyCirculation2013108141682169714504182
- CURRENT-OASIS 7 InvestigatorsMehtaSRBassandJPDose comparisons of clopidogrel and aspirin in acute coronary syndromesN Engl J Med20103631093094220818903
- KohliPUdellJAMurphySADischarge aspirin dose and clinical outcomes in patients with acute coronary syndromes treated with prasugrel versus clopidogrel: an analysis from the TRITON-TIMI 38 study (Trial to Assess Improvement in Therapeutic Outcomes by Optimizing Platelet Inhibition with Prasugrel-Thrombolysis In Myocardial Infarction 38)J Am Coll Cardiol201463322523224140678
- MahaffeyKWWojdylaDMCarrollKTicagrelor compared with clopidogrel by geographic region in the Platelet Inhibition and Patient Outcomes (PLATO) trialCirculation2011124554455421709065
- MahaffeyKWHuangZWallentinLAssociation of aspirin dose and vorapaxar safety and efficacy in patients with non-ST-segment elevation acute coronary syndrome (from the TRACER Trial)Am J Cardiol Epub12252013
- StoreyRFKothaJSmythSEffects of vorapaxar on platelet reactivity and biomarker expression in non-ST-elevation acute coronary syndromes. The TRACER Pharmacodynamic SubstudyThromb Haemost20141115
- DorsamRTTulucMKunapuliSPRole of protease-activated and ADP receptor subtypes in thrombin generation on human plateletsJ Thromb Haemost20042580481215099288
- MorrowDAAlbertsMJMohrJPEfficacy and safety of vorapaxar in patients with prior ischemic strokeStroke201344369169823396280
- SciricaBMBonacaMPBraunwaldEVorapaxar for secondary prevention of thrombotic events for patients with previous myocardial infarction: a prespecified subgroup analysis of the TRA 2°P-TIMI 50 trialLancet201238098501317132422932716
- SciricaBMBonacaMPMoraisJVorapaxar in patients with diabetes and prior MI: findings from the TRA 2P-TIMI 50 trialCirculation2013128A10398
- BonacaMPSciricaBMCreagerMAVorapaxar in patients with peripheral artery disease: results from TRA2°P-TIMI 50Circulation2013127141522152923501976
- BonacaMPSciricaBMBraunwaldEEfficacy of vorapaxar is not modified by thienopyridine therapy: results from TRA 2P-TIMI 50 trialCirculation2012126A18595
- SciricaBMBonacaMPBraunwaldEVorapaxar for secondary prevention after myocardial infarction according to aspirin dose – insights from the TRA 2P-TIMI 50 trialCirculation2012126A14508
- AlexanderJHLopesRDJamesSApixaban with antiplatelet therapy after acute coronary syndromeN Engl J Med2011365869970821780946
- OldgrenJBudajAGrangerCBDabigatran vs. placebo in patients with acute coronary syndromes on dual antiplatelet therapy: a randomized, double-blind, phase II trialEur Heart J201132222781278921551462
- MegaJLBraunwaldEWiviottSDRivaroxaban in patients with a recent acute coronary syndromeN Engl J Med2012366191922077192
- FriedlandSNEisenbergMJShimonyAMeta-analysis of randomized controlled trials on effect of cilostazol on restenosis rates and outcomes after percutaneous coronary interventionAm J Cardiol2012109101397140422381162
- US Food Drug AdministrationVorapaxar Advisory Committee briefing document2014 Available from: http://www.fda.gov/downloads/advisorycommittees/committeesmeetingmaterials/drugs/cardiovascularandrenaldrugsadvisorycommittee/ucm381330.pdfAccessed January 31, 2014
- FerreiroJLAngiolilloDJNew directions in antiplatelet therapyCirc Cardiovasc Interv20125343344522715450