
Abstract
Background
In the United States, echocardiography is an essential component of the care of many cardiac patients. Recently, increased attention has been given to the accuracy of interpretation of cardiac-based procedures in different specialties, amongst them the field of cardiac anesthesiology and primary echocardiographers for transesophageal echocardiogram (TEE). The purpose of this study was to assess the TEE skills of cardiac anesthesiologists in comparison to primary echocardiographers, either radiologists or cardiologists. In this systematic review, we evaluated available current literature to identify if cardiac anesthesiologists interpret TEE procedures at an identical level to that of primary echocardiographers.
Methods
A PRISMA systematic review was utilized from PubMed from the years 1952–2022. A broad keyword search of “Cardiology Anesthesiology Echocardiogram” and “Echocardiography Anesthesiology” to identify the literature was used. From reviewing 1798 articles, there were a total of 9 studies included in our systematic review, 3 of which yielded quantitative data and 6 of which yielded qualitative data. The mean accuracy from each of these three qualitative studies was calculated and used to represent the overall accuracy of cardiac anesthesiologists.
Results
Through identified studies, a total of 8197 TEEs were interpreted by cardiac anesthesiologists with a concordance rate of 84% to the interpretations of primary echocardiographers. Cardiac anesthesiologists had a concordance rate of 83% when compared to radiologists. On the other hand, cardiac anesthesiologists and cardiologists had a concordance rate of 87% in one study and 79% in another study.
Conclusion
Based on these studies, cardiac anesthesiologists are shown to interpret TEEs similarly to that of primary echocardiographers. At this time, there is no gold standard to evaluate the accuracy of TEE readings. One way to address this is to individually assess the TEE interpretation of anesthesiologists and primary echocardiographers with a double-blind study.
Introduction
In the recent literature, cardiology based training in different procedures and techniques has been garnering a lot of attention.Citation1–3 As of 2019 over 90,000 physicians specialize in cardiac-based procedures and interpretation in the United States. One such procedure is echocardiography, and physicians who specialize in interpreting them are called primary echocardiographers, which include cardiologists and radiologists.Citation4 22,521 active physicians practice in the field of cardiology and 28,025 active physicians practicing in radiology.Citation5 In comparison, there are only 1667 anesthesiologists who practice cardiac anesthesia as a subspecialty.Citation6 Subspecialization in cardiac anesthesiology requires at least 4 years of training in an anesthesiology residency program and at least 1 year of a cardiac anesthesiology fellowship.Citation7–16
During their residency and fellowship years, most anesthesiologists will be trained in the use of echocardiography. One such type of echocardiography is transthoracic echocardiogram (TTE), in which a handheld transducer is held outside the heart.Citation17,Citation18 Although other forms of echocardiograms exist, such as intracardiac echo and stress echo, a transesophageal echocardiogram is often the approach in the perioperative setting. Compared to TTE, a transesophageal echocardiogram can be more sensitive at identifying etiologies of an embolic stroke.Citation19–21 One study suggests that TEE may be more suitable than TTE for detecting infective endocarditis.Citation22 Transesophageal echocardiograms can assess the heart’s function and detect symptoms of atherosclerosis, cardiomyopathy, heart failure, and more.Citation23,Citation24 This is because an ultrasound probe is guided into the esophagus, providing a closer view of the heart.Citation25–30 Interpreting TEEs have a significant impact throughout perioperative care in order to make a proper diagnosis.Citation31 Although cardiac anesthesiologists, cardiologists, and radiologists are all trained in interpreting transesophageal echocardiography, an overwhelming majority of perioperative TEEs are performed by cardiac anesthesiologists. A study by Poterack recognized that out of 98 institutions surveyed, 54% of them have anesthesiologists in charge of TEE interpretations.Citation32 Therefore, it is of utmost importance that cardiac anesthesiologists are well-trained in these procedures.
TEE specifically has seen major growth in terms of technology, use, and indications since its introduction to the medical community nearly half a decade ago.Citation33 These advancements include the increase in TEE use from 29% in 2009 to 45% in 2011, and upgrades in technology such as the 3-D TEE systems.Citation34 3-D TEE imaging has been shown to improve detecting infective endocarditis in a study by Chahine et al.Citation35 Additional advancements include continuous TEE monitoring, strain imaging, and diastolic function assessment.Citation36 These advancements have also increased the complexity of the procedure itself. For this reason, diagnostic evaluation of the TEE exams may vary disparately depending on who delivers the procedure and the expertise of the examiner.Citation37 Despite the active role that cardiac anesthesiologists have in the perioperative setting, there is limited literature on the assessment of their ability to interpret intraoperative TEE. Our paper conducts a systematic literature review to assess the effectiveness with which cardiac anesthesiologists interpret TEE examinations compared to primary echocardiographers, such as cardiologists and radiologists.
Methods
The PRISMA systematic review model was used to execute this study and identify relevant literature.Citation38 A comprehensive search was used on the MED-LINE database (PubMed) to yield articles used for our study. Step 1 included using a broad keyword search using the phrases “Cardiology Anesthesiology Echocardiogram” and “Echocardiography Anesthesiology” to produce 1114 and 684 articles, respectively, dating from 1952 to 2022. The criteria for inclusion and exclusion are shown below in including but not limited to articles being written in the English language.
Figure 1 Study flow chart.
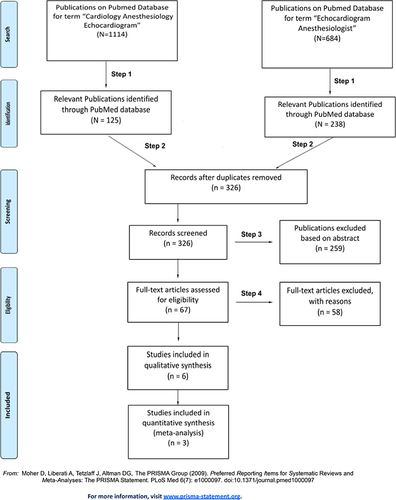
From the search, a total of 363 articles were included based on the relevance of the title (, step 1), and duplicates were then removed (, step 2). The remaining articles were then screened based on their abstract (, step 3). The last step executed was reading the full article to determine which publications will be used in the study (, step 4). This process yielded a combination of quantitative and qualitative information that amounted to a total of 9 relevant articles for our topic of interest. Three researchers carried out the procedures to obtain the final sample. The investigation team agreed on the final selection of the literature ().
Table 1 Publications Included in the Systematic Review
After assembly of the 9 articles, they were divided according to whether they contained quantitative or qualitative data. There were three quantitative data containing the accuracy of cardiac anesthesiologists’ TEE readings. Accuracy is defined as the degree to which cardiac anesthesiologists’ TEE interpretation agreed with that of primary echocardiographers. The quantitative studies examined different parameters as part of the TEE procedure and also used different methods to assess accuracy. Cohen’s kappa coefficient and high-fidelity videotape evaluation were the methods of analysis used to evaluate the accuracy of the interpretation of these parameters. The number of correctly interpreted TEEs and the total number of TEEs were obtained from each of the three quantitative studies. These numbers were then used to calculate the mean accuracy in the interpretation of all TEEs to represent the overall accuracy of cardiac anesthesiologists ().
Table 2 Results of Transesophageal Echocardiogram Results in Systematic Review
Results
PRISMA systematic review yielded a total of 3 quantitative studies and 6 qualitative studies for a total of 9 relevant studies. The three quantitative studies contained comparisons between cardiac anesthesiologists and radiologists, cardiac anesthesiologists and cardiologists, and cardiologists and radiologists.
Mathew et al contained the concordance rate of TEE interpretations amongst cardiac anesthesiologists, cardiologists, and radiologists. In the study, radiologists interpreted the same number of TEEs as cardiac anesthesiologists. For this reason, we decided to compare anesthesiologists to radiologists in this study. They found that anesthesiologists with less than 5 years of experience underestimated left ventricular fractional area change (FAC). On the other hand, anesthesiologists with greater experience had higher levels of concordance with radiologists, particularly in the assessment of the aorta, right atrium, pulmonary vein flow, and transmitral flow. Furthermore, cardiac anesthesiologists correctly interpreted 83% of TEEs when compared specifically to radiologists. Out of 2464 TEE exams, this comes out to a total of 2045 correctly interpreted TEEs. Nevertheless, comparisons between anesthesiologists and cardiologists (80% concordance) and cardiologists and radiologists (82% concordance) were all similar.
The study by Mishra et al contained information regarding the concordance between online interpretation by cardiac anesthesiologists and offline analysis by cardiologists. This study specifically examined left ventricle regional wall motion, valve function, and left and right ventricle function. 3620 out of 4161 TEEs were correctly interpreted by the cardiac anesthesiologists, amounting to an accuracy rating of 87%. Although this study did not state the number of anesthesiologists involved, they examined 3217 TEEs in a group of patients who underwent coronary bypass graftings and 629 TEEs in a group of patients who underwent valve procedures, yielding a total of 3846 TEEs that were interpreted.
The final quantitative study by Miller et al compared the performance of anesthesiologists to an expert cardiologist in recording and interpreting TEEs. Parameters measured in this study included size of the heart chambers, FAC, and degree of stenosis or insufficiency of heart valves. They found that their cardiac anesthesiologists correctly interpreted 1242 out of 1572 TEEs, a 79% accuracy rating. As indicated in , these three studies totaled 8197 interpreted TEEs by cardiac anesthesiologists, 84% of which were correctly interpreted.
Discussion
The American Society of Echocardiography suggests that non-cardiologists such as radiologists and cardiac anesthesiologists who provide optimal TEE services should ideally undergo 6 months of full-time training in an active echocardiography training institution.Citation39 They recommend being involved in 300 total TEE exams and performing at least 150 of those exams, and 15 h of TEE within 3 years per Continuing Medical Education (CME) standards. Thus, all physicians who were not formally trained in TEE should adhere to these standards. It may also be advisable to consider facilitating close interactions between cardiac anesthesiologists and cardiologists or radiologist echocardiographers, at least in the initial training phases.Citation40
In our study design, we chose to compare the evaluation of TEE studies between attending anesthesiologists to primary attending echocardiographers, either cardiologists or radiologists. A prospective observational cohort study was performed between 1993 and 1997 meant to evaluate TEE as a safe and reliable technique during cardiac surgery.Citation41 3217 TEEs were administered to 944 patients who underwent coronary artery bypass grafting (CABG) procedures, and another 629 TEES to 142 patients who underwent heart valve procedures. The attending anesthesiologists who performed the TEE had a minimum hands-on experience of performing and interpreting 500 TEE studies each. Although the study did not disclose the number of anesthesiologists included in the study, they found that there was a rather high concordance between anesthesiologists and cardiologists (87%). This suggests that anesthesiologists can interpret and perform TEE studies in a manner comparable to that of cardiologists.
Another study was done at Duke University Medical Center that assessed the concordance of TEE interpretation in a continuous quality improvement (CQI) program.Citation4 In this study, 10 cardiac anesthesiologists conducted a total of 154 TEE studies that included the estimation of FAC using Bland-Altman methods. Fractional area change is a measure of right ventricular systolic function. It is clinically significant because it can be used to measure any impairments to right ventricle function, such as after a pulmonary valve replacement.Citation42 All 154 of the TEE studies were reviewed by radiologists, 50 of which were also reviewed by cardiologists. Cardiac anesthesiologists were found to underestimate the FAC when compared to radiologists, especially if the anesthesiologist had less than 5 years of TEE experience. Anesthesiologists with more experience, however, were found to have higher levels of concordance with the radiologists. Ultimately, the high levels of concordance of anesthesiologists to radiologists (83%) and cardiologists (80%) suggest that anesthesiologists are proficient in TEE interpretation.
A prospective study done at the Madigan Army Medical Center evaluated the ability of anesthesiologists to perform and interpret TEE after revisions were made to their examination protocol.Citation43 Namely, these revisions entailed going from a standard 10 view TEE examination to a 12 view in which 8 were from the original and 4 assessed with color Doppler. Eight cardiac anesthesiologists performed 135 TEE examinations, which were then compared with a final expert evaluation by a cardiologist, yielding an accuracy of 79%. Although this is considerably lower than the other studies we analyzed, this is inclusive of TEE examinations with omitted diagnoses (blanks on evaluation sheets). If these TEE examinations had not been included in the study, the rate of correct interpretation would have been 94%.
It has been shown in a study done at Aarhus University Hospital that anesthesiologists are capable of providing valuable information in interpreting TEE.Citation44 A TEE was successfully performed on 525 children undergoing cardiac surgery and according to the results, interpretations of TEE performed by anesthesiologists resulted in a total of 184 alterations to treatment in 143 patients. Additionally, anesthesiologists were able to add 37% of new information and add 8% of decisive information out of all the TEEs interpreted.
Although our study indicates how effective anesthesiologists can be in perioperative care, there have been multiple studies that have shown experience and training is still valuable in both carrying out the TEE procedure and interpreting the results. One study compared the length of time it takes to obtain a TEE exam and how accurate the interpretation was between certified anesthesiologists and anesthesiology residents.Citation45 Attending physicians and residents were recruited from both the Vanderbilt School of Medicine and The Icahn School of Medicine at Mount Sinai for a total of 15 residents and 11 attending physicians. Participants were required to obtain 10 standard views using TEE. The certified anesthesiologists were able to interpret 5 out of 10 images better than the residents, whereas the remaining 5 views were comparable to the residents. Results also indicated that certified anesthesiologists were able to acquire TEE images more quickly, suggesting that experience is necessary to become a proficient echocardiographer.
A study done at Mahidol University concurred with this by showing improvement in acquiring TEE images as the procedure was performed more often.Citation46 An additional study performed at The Icahn School of Medicine at Mount Sinai suggested that more experienced anesthesiologists were able to score higher on multiple-choice questions that involved TEEs.Citation47 Evidently, experience in echocardiography improves both the theoretical knowledge and the practical application of the skills involved in TEE.
Limitations to our study include the circumstances of assessment in our quantitative studies. Specifically, comparisons were made between on-line assessments by anesthesiologists and off-line assessments of the primary echocardiographers. It is plausible that there could have been a higher level of agreement between the two groups if they interpreted TEEs under the same circumstances. For example, there may have been higher concordance if the anesthesiologists evaluated TEE results after operation. Another limitation to our study is that most of our quantitative data were published nearly 20 years ago. If these studies were to be done today, it may be the case that we would see higher concordance between cardiac anesthesiologists and primary echocardiographers, especially because of the guidelines that were established since then.Citation39 Another notable limitation of this study is that there were variations in the gold standard for interpreting TEEs. Some studies used expert echocardiographers as the gold standard, while others relied on the degree to which there was consensus amongst attending echocardiographers.
Quality Improvement
A possible method of improving clinical evaluation is by refining current indications for the use of echocardiography. For example, echocardiography currently plays a major role in the diagnosis and management of infective endocarditis (IE) as part of Duke’s criteria. However, many patients are initially misclassified even though IE is a life-threatening emergency.Citation48–50 This is partly because a negative echocardiogram does not rule out IE and a false-positive result is not unusual with these tests. The fault here is not so much in the conductor of the test, but the test itself. Therefore, in these cases, it may be worth considering other imaging techniques. An 18F-FDG PET/CT scan has instead shown promising results with these patients.Citation51–56
Conclusion
Based on the studies presented, it is clear that anesthesiologists have an important role in the perioperative stages of patient care by performing and interpreting transesophageal echocardiograms. With continuous quality improvement, cardiac anesthesiologists are shown to function at a level equivalent to that of primary echocardiographers. The implementation of software programs to routinely test physician TEE skills and the implementation of standardized AI interpretation as a possible gold standard are noteworthy considerations for future investigation.
Disclosure
The authors declare no competing interests in this work.
References
- Zhitny V, Iftekhar N, Alexander L, Ahsan C. Cardiology fellow diagnostic accuracy and data interpretation outcomes: a review of the current literature. Vasc Health Risk Manag. 2020;16:429–435. PMID: 33116553; PMCID: PMC7585513. doi:10.2147/VHRM.S266510
- Kohan LC, Nagarajan V, Millard MA, Loguidice MJ, Fauber NM, Keeley EC. Impact of around-The-clock in-house cardiology fellow coverage on door-to-balloon time in an academic medical center. Vasc Health Risk Manag. 2017;13:139–142. PMID: 28458558; PMCID: PMC5403126. doi:10.2147/VHRM.S132405
- Spahillari A, McCormick I, Yang JX, Quinn GR, Manning WJ. On-call transthoracic echocardiographic interpretation by first year cardiology fellows: comparison with attending cardiologists. BMC Med Educ. 2019;19(1):213. PMID: 31200721; PMCID: PMC6567532. doi:10.1186/s12909-019-1634-7
- Mathew JP, Fontes ML, Garwood S, et al. Transesophageal echocardiography interpretation: a comparative analysis between cardiac anesthesiologists and primary echocardiographers. Anesth Analg. 2002;94(2):302–309. PMID: 11812688. doi:10.1097/00000539-200202000-00013
- AAMC. Number of people per active physician by specialty; 2019. Available from: https://www.aamc.org/what-we-do/mission-areas/health-care/workforce-studies/interactive-data/number-people-active-physician-specialty-2019. Accessed: June 13, 2022.
- Adult cardiac anesthesiology. Careers in medicine; 2022. Available from: https://www.aamc.org/cim/explore-options/specialty-profiles/adult-cardiac-anesthesiology?check_logged_in=1#workforce. Accessed June 19, 2022.
- Massachusetts General Hospital. Guide to cardiac anesthesia; 2022. Available from: https://www.massgeneral.org/heart-center/treatments-and-services/cardiac-surgery/guide-to-cardiac-anesthesia#:~:text=A%20cardiac%20anesthesiologist%20is%20a,a%20cardiac%20anesthesia%20fellowship%20program. Accessed November 21, 2022.
- Penn State College of Medicine Residencies and Fellowships. Cardiac anesthesia fellowship; 2022. Available from: https://residency.med.psu.edu/programs/cardiac-anesthesia-fellowship/. Accessed March 31, 2023.
- Department of Anesthesiology. Cardiothoracic anesthesiology fellowship; 2022. Available from: https://anesthesiology.weill.cornell.edu/education/fellowships/cardiothoracic-anesthesiology. Accessed March 31, 2023.
- Cardiothoracic Anesthesia Fellowship - Brigham and Women’s Hospital. Adult cardiothoracic anesthesia fellowship; 2022. Available from: https://www.brighamandwomens.org/anesthesiology-and-pain-medicine/clinical-fellowships/cardiothoracic2/cardiothoracic-fellowship-landing#:~:text=The%20fellowship%20is%20either%2012,%2D%20to%2024%2Dmonth%20program. Accessed March 31, 2023.
- Cardiothoracic Anesthesiology Fellowship. Anesthesiology; 2022. Available from: https://keck.usc.edu/anesthesiology/training-education/fellowship-programs/cardiothoracic-anesthesiology-fellowship. Accessed March 31, 2023.
- Department of Anesthesiology, Perioperative and Pain Medicine. Adult cardiothoracic anesthesia; 2022. Available from: https://med.stanford.edu/anesthesia/education/fellowships/clinical-fellows/acta.html. Accessed March 31, 2023.
- Wdelaney. Adult cardiothoracic anesthesiology fellowship. Medical School - University of Minnesota; 2018. Available from: https://med.umn.edu/anesthesiology/education-training/fellowship-programs/cardiothoracic-anesthesiology-fellowship. Accessed March 31, 2023.
- Department of Anesthesia & Critical Care | The University of Chicago. Adult cardiothoracic fellowship; 2022. Available from: https://anesthesia.uchicago.edu/education/adult-cardiothoracic-fellowship. Accessed November 21, 2022.
- Johns Hopkins Anesthesiology and Critical Care Medicine. Cardiac anesthesiology and interventional echocardiography fellowship; 2022. Available from: https://anesthesiology.hopkinsmedicine.org/accm-homepage/cardiac-anesthesia/cardiac-anesthesia-fellowship/. Accessed November 21, 2022.
- Adult Cardiothoracic Anesthesiology (ACTA) Fellowship. Department of Anesthesiology and Perioperative Medicine. University of Pittsburgh; 2022. Available from: https://www.anesthesiology.pitt.edu/education/clinical-fellowships/adult-cardiothoracic-anesthesiology-acta-fellowship. Accessed November 21, 2022.
- Stanford Health Care (SHC) - Stanford Medical Center. Types; 2020. Available from: https://stanfordhealthcare.org/medical-tests/e/echocardiogram/types.html. Accessed June 13, 2022.
- Phoenix Heart Center. Echocardiograms: transthoracic (TTE) & Transesophageal (TEE); 2017. Available from: http://www.phoenixheartcenter.com/echocardiograms-tte-tee/. Accessed November 10, 2022.
- de Bruijn SF, Agema WR, Lammers GJ, et al. Transesophageal echocardiography is superior to transthoracic echocardiography in management of patients of any age with transient ischemic attack or stroke. Stroke. 2006;37(10):2531–2534. PMID: 16946152. doi:10.1161/01.STR.0000241064.46659.69
- Thomsen J. To TTE or Tee? European Stroke Organisation; 2021. Available from: https://eso-stroke.org/to-tte-or-tee/#:~:text=TEE%20is%20considered%20more%20sensitive,visualization%20of%20left%20ventricular%20thrombus. Accessed October 24, 2022.
- Kapral MK, Silver FL. Preventive health care, 1999 update: 2. Echocardiography for the detection of a cardiac source of embolus in patients with stroke. Canadian Task Force on Preventive Health Care. CMAJ. 1999;161(8):989–996. PMID: 10551199; PMCID: PMC1230713.
- Noor A, Suffoletto M. An echocardiogram battle: tte vs tee in the diagnosis of infective endocarditis; 2019. Available from: https://shmabstracts.org/abstract/an-echocardiogram-battle-tte-vs-tee-in-The-diagnosis-of-infective-endocarditis/. Accessed November 10, 2022.
- Johns Hopkins Medicine. Transesophageal echocardiogram; 2021. Available from: https://www.hopkinsmedicine.org/health/treatment-tests-and-therapies/transesophageal-echocardiogram. Accessed June 19, 2022.
- UPMC. Echocardiography - purpose, types, and what to expect: UPMC in central PA. Available from: https://www.upmc.com/services/south-central-pa/heart-vascular/heart/diagnosis/screenings/echo. Accessed March 31, 2023.
- Heart and Stroke Foundation of Canada. Transesophageal Echocardiogram (TEE); 2022. Available from: https://www.heartandstroke.ca/heart-disease/tests/transesophageal-echocardiogram-tee. Accessed June 19, 2022.
- Stanford Health Care (SHC) - Stanford Medical Center. Transesophageal Echocardiogram (TEE); 2017. Available from: https://stanfordhealthcare.org/medical-tests/t/transesophageal-echocardiogram.html. Accessed June 19, 2022.
- Transesophageal echocardiography (TEE); 2021. Available from: https://www.heart.org/en/health-topics/heart-attack/diagnosing-a-heart-attack/transesophageal-echocardiography-tee. Accessed November 10, 2022.
- Memorial Sloan Kettering Cancer Center. About Your Transesophageal Echocardiogram (TEE). Available from: https://www.mskcc.org/cancer-care/patient-education/patient-guide-transesophageal-echocardiogram-tee. Accessed March 31, 2023.
- Healthline, Healthline Media. Transesophageal Echocardiogram (TEE). Available from: https://www.healthline.com/health/tee-procedure#reasons. Accessed March 31, 2023.
- Transthoracic Echocardiography (TTE) or Transesophageal. Available from: https://mountnittany.org/wellness-article/transthoracic-echocardiography-tte-or-transesophageal-echocardiography-tee-when-------your-child-needs. Accessed March 31, 2023.
- American society of Anesthesiologist. Statement on transesophageal echocardiography; 2022. Available from: https://www.asahq.org/standards-and-guidelines/statement-on-transesophageal-echocardiography. Accessed June 19, 2022.
- Poterack KA. Who uses transesophageal echocardiography in the operating room? Anesth Analg. 1995;80(3):454–458. PMID: 7864407. doi:10.1097/00000539-199503000-00004
- Peterson GE, Brickner ME, Reimold SC. Transesophageal echocardiography. Circulation. 2003;107(19):2398–2402. doi:10.1161/01.cir.0000071540.97144.89
- DAIC. Advances in transesophageal echo. DAIC; 2021. Available from: https://www.dicardiology.com/article/advances-transesophageal-echo. Accessed June 13, 2022.
- Chahine J, Montane B, Alzubi J, et al. Improved diagnostic performance of contemporary transesophageal echocardiography with three-dimensional imaging for infective endocarditis. Circulation. 2020;142(Suppl_3):A13434–A13434. doi:10.1161/circ.142.suppl_3.13434
- Maxwell C, Konoske R, Mark J. Emerging concepts in transesophageal echocardiography. F1000Res. 2016;5:F1000Faculty Rev–340. PMID: 26998250; PMCID: PMC4792209. doi:10.12688/f1000research.7169.1
- Fatima H, Sharkey A, Qureshi N, et al. Three-dimensional transesophageal echocardiography simulator: new learning tool for advanced imaging techniques. J Cardiothorac Vasc Anesth. 2022;36(7):2090–2097. PMID: 34275733. doi:10.1053/j.jvca.2021.05.050
- Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. 2009;339:b2535. doi:10.1136/bmj.b2535
- Hahn RT, Abraham T, Adams MS, et al. Guidelines for performing a comprehensive transesophageal echocardiographic examination: recommendations from the American Society of Echocardiography and the Society of Cardiovascular Anesthesiologists. J Am Soc Echocardiogr. 2013;26(9):921–964. PMID: 23998692. doi:10.1016/j.echo.2013.07.009
- Rafferty T, LaMantia KR, Davis E, et al. Quality assurance for intraoperative transesophageal echocardiography monitoring: a report of 846 procedures. Anesth Analg. 1993;76(2):228–232. PMID: 8424496. doi:10.1213/00000539-199302000-00005
- Mishra M, Chauhan R, Sharma KK, et al. Real-time intraoperative transesophageal echocardiography--how useful? Experience of 5016 cases. J Cardiothorac Vasc Anesth. 1998;12(6):625–632. PMID: 9854658. doi:10.1016/s1053-0770(98)90232-4
- DiLorenzo MP, Bhatt SM, Mercer-Rosa L. How best to assess right ventricular function by echocardiography. Cardiol Young. 2015;25(8):1473–1481. doi:10.1017/S1047951115002255
- Miller JP, Lambert AS, Shapiro WA, Russell IA, Schiller NB, Cahalan MK. The adequacy of basic intraoperative transesophageal echocardiography performed by experienced anesthesiologists. Anesth Analg. 2001;92(5):1103–1110. PMID: 11323329. doi:10.1097/00000539-200105000-00005
- Sloth E, Pedersen J, Olsen KH, Wanscher M, Hansen OK, Sørensen KE. Transoesophageal echocardiographic monitoring during paediatric cardiac surgery: obtainable information and feasibility in 532 children. Paediatr Anaesth. 2001;11(6):657–662. PMID: 11696140. doi:10.1046/j.1460-9592.2001.00737.x
- Bick JS, Jr DS, Kennedy JD, et al. Comparison of expert and novice performance of a simulated transesophageal echocardiography examination. Simul Healthc. 2013;8(5):329–334. PMID: 24030477. doi:10.1097/SIH.0b013e31829068df
- Sawasdiwipachai P, Thanasriphakdeekul S, Raksamani K, Vacharaksa K, Chaithiraphan V. Learning curve for the acquisition of 20 standard two-dimensional images in advanced perioperative transesophageal echocardiography: a prospective observational study. BMC Med Educ. 2022;22(1):412. PMID: 35637456; PMCID: PMC9153196. doi:10.1186/s12909-022-03280-3
- Konstadt SN, Reich DL, Rafferty T. Validation of a test of competence in transesophageal echocardiography. J Cardiothorac Vasc Anesth. 1996;10(3):311–313. PMID: 8725408. doi:10.1016/s1053-0770(96)80088-7
- Sarrazin JF, Trottier M, Tessier M. Accuracy of PET/CT for detection of infective endocarditis: where are we now? J Nucl Cardiol. 2019;26(3):936–938. PMID: 29143245. doi:10.1007/s12350-017-1126-2
- Prendergast BD. Diagnostic criteria and problems in infective endocarditis. Heart. 2004;90(6):611–613. PMID: 15145855; PMCID: PMC1768277. doi:10.1136/hrt.2003.029850
- Pecoraro AJK, Herbst PG, Pienaar C, et al. Modified Duke/European Society of Cardiology 2015 clinical criteria for infective endocarditis: time for an update? Open Heart. 2022;9:e001856. doi:10.1136/openhrt-2021-001856
- Mahmood M, Kendi AT, Ajmal S, et al. Meta-analysis of 18F-FDG PET/CT in the diagnosis of infective endocarditis. J Nucl Cardiol. 2019;26(3):922–935. PMID: 29086386. doi:10.1007/s12350-017-1092-8
- Ten HD, Slart RHJA, Sinha B, Glaudemans AWJM, Budde RPJ. 18F-FDG PET/CT in infective endocarditis: indications and approaches for standardization. Curr Cardiol Rep. 2021;23(9):130. PMID: 34363148; PMCID: PMC8346431. doi:10.1007/s11886-021-01542-y
- Rouzet F, Iung B, Duval X, et al. 18F-FDG PET/CT in infective endocarditis. J Am Coll Cardiol. 2019;74(8):1041–1043. doi:10.1016/j.jacc.2019.06.049
- Swart LE, Gomes A, Scholtens AM, et al. Improving the diagnostic performance of 18F-fluorodeoxyglucose positron-emission tomography/computed tomography in prosthetic heart valve endocarditis. Circulation. 2018;138(14):1412–1427. PMID: 30018167. doi:10.1161/CIRCULATIONAHA.118.035032
- Wang TKM, Sánchez-Nadales A, Igbinomwanhia E, Cremer P, Griffin B, Xu B. Diagnosis of infective endocarditis by subtype using 18F-fluorodeoxyglucose positron emission tomography/computed tomography: a contemporary meta-analysis. Circ Cardiovasc Imaging. 2020;13(6):e010600. PMID: 32507019. doi:10.1161/CIRCIMAGING.120.010600
- Orvin K, Goldberg E, Bernstine H, et al. The role of FDG-PET/CT imaging in early detection of extra-cardiac complications of infective endocarditis. Clin Microbiol Infect. 2015;21(1):69–76. doi:10.1016/j.cmi.2014.08.012