Abstract
Background
Adverse drug events (ADE) occur frequently during treatment with vitamin K antagonists (AVK) and contribute to increase hemorrhagic risks.
Methods
A retrospective study was conducted over a period of 2 years. Patients treated with AVK and admitted to the emergency room of a tertiary care hospital in Beirut were included. The aim of the study was to identify ADE characterized by a high international normalized ratio (INR) and to determine the predictive factors responsible for these events. Statistical analysis was performed with the SPSS statistical package.
Results
We included 148 patients. Sixty-seven patients (47.3%) with an INR above the therapeutic range were identified as cases. The control group consisted of 81 patients (54.7%) with an INR within the therapeutic range. Hemorrhagic complications were observed in 53.7% of cases versus 6.2% of controls (P < 0.0001). No significant difference was noticed between cases and controls regarding the indication and the dose of AVK. Patients aged over 75 years were more likely to present an INR above the therapeutic range (58.2%, P = 0.049). Recent infection was present in 40.3% of cases versus 6.2% of controls (P < 0.0001) and hypoalbuminemia in 37.3% of cases versus 6.1% of controls (P < 0.0001). Treatment with antibiotics, amiodarone, and anti-inflammatory drugs were also factors of imbalance (P < 0.0001).
Conclusion
Many factors may be associated with ADE related to AVK. Monitoring of INR and its stabilization in the therapeutic range are important for preventing these events.
Vitamin K antagonists (AVK) have been shown to be an effective preventive or therapeutic strategy for arterial and venous thromboembolism. About 1% of the French population is currently treated with AVK.Citation1 In the Western world approximately 15 to 20 per 1000 subjects use AVK, and this number is increasing, probably due to aging of the population and increasing adherence to guidelines.Citation2 An important complication of treatment with these agents is hemorrhage, which may be life threatening. In France there are 17,000 hospitalizations per year for AVK-related bleeding events.Citation3 The ENEIS study showed that AVK are responsible for almost 50% of the serious adverse events caused by anticoagulants and about 17% of the total serious adverse drug reactions that are more often the result of therapeutic errors, such as inadequate prescription or administration, inappropriate monitoring, absence of treatment resulting from poor adherence, or absence of prescription or administration.Citation4 A study carried out at Beirut Governmental Hospital, Lebanon, showed that anticoagulants were responsible for 7.4% of adverse drug events.Citation5 Among 101 hospitalized patients with major bleeding, 50 patients had excessive anticoagulation and the overall mortality at 60 days was 26% (increased effect was seen with the group using AVK versus other anticoagulants). As a result, excessive AVK therapy was a significant predictor of mortality as well as morbidityCitation6
The French Society of Clinical Pharmacy defines an adverse drug event (ADE) as an injury occurring during the patients’ drug therapy whether resulting from appropriate care or from unsuitable or suboptimum care.Citation7
The goal of our study was to identify ADE characterized by a high value of international normalized ratio (INR) and to determine the predictive factors of therapeutic imbalance responsible for these accidents.
Patients and methods
We conducted a retrospective study of patients who were hospitalized at Beirut Governmental Hospital, Lebanon, and treated with AVK between March 1, 2009 and February 28, 2011. Inclusion criteria were an age of 18-years old or more and an INR within or higher than the therapeutic range. The cases consisted of patients who had an INR above the therapeutic range while using AVK, while the control group consisted of patients having their INR within the therapeutic range while using AVK.
Selection of patients was done using the computerized patient files. These files were used in order to retrieve the necessary information for the study. The research support was a questionnaire completed for each patient and composed of three parts:
One part related to patient and treatment characteristics, including age, sex, alcohol consumption, smoking status, past medical history of the patient, prescribed mole cule, indication, dose and frequency of administration, laboratory data at admission (INR levels of hemoglobin, platelets, albumin). The dose was considered as the daily intake of AVK (mg/day). INR higher than the therapeutic range or within the therapeutic range was based on the recommendations of Agence Française de Sécurité Sanitaire des Produits de Santé (AFSSAPS).Citation8 Low hemoglobin count was defined as a level of hemoglobin below 13.5 g/dL in males or 12 g/dL in females; low hematocrit as a hematocrit count below 41% in males or 36% in females; low platelet level as a platelet count below 150,000/mm;Citation3 high creatininemia as a creatinine level above 1.2 mg/dL; and hypoalbuminemia as an albumin level below 3.5 g/dL.Citation9
One part related to health care professionals who prescribed or dispensed the drug, including
— prescribing without taking into consideration the medical history of the patient: presence of absolute or relative contraindications to AVK therapy according to AFSSAPS.Citation10
— presence of drug–drug interactions: Presence of drug interactions was defined when a precaution for use is recommended the drug interaction should be taken into account or the use of one or more drugs is discouraged or contraindicated. Drug interactions were evaluated according to the Thesaurus des interactions médicamenteuses.Citation11
One part related to bleeding signs and management of bleeding or nonbleeding patients with a high INR: For all patients, signs of hemorrhage and internal bleeding were indicated such as epistaxis, gastrointestinal bleeding, intracranial hemorrhage, hematuria, melena, hematoma, palpitations, syncope, or fatigue. Possible treatment strategies in the management of a high INR included in our questionnaire were those recommended by AFSSAPS, such as INR monitoring, withholding AVK, withholding any other drug supposed to interact with the AVK and cause this bleeding, administering vitamin K, transfusion of fresh frozen plasma, restoration of red blood cell mass, and transfusion of pooled plasma products.Citation12
Statistical analysis
Comparison of ordinal variables between cases and control groups was evaluated using the Chi-square test. For all statistical tests, P < 0.05 was considered statistically significant. We also used multivariate logistic regression modeling to determine the impact of multiple factors of imbalance (independent variables) presented simultaneously to predict the dependent variable, which was an INR higher than the therapeutic range. Prior to model fitting, a matrix correlation analysis was utilized to evaluate the relationship between the dependent variables and investigate any potential collinearity. In the event of significant collinearity (ie, r > 0.7) between two variables, only one of the two variables was chosen and was reported in the analysis. Statistical analysis was performed using SPSS version 17 (IBM Corporation, Armonk, NY, USA).
Results
We included 148 patients (67 [45.3%] cases and 81 [54.7%] controls) using AVK in our study.
Characteristics of patients on AVK treatment
Fifty-eight percent of the cases were over 75-years old versus 40.7% of the controls (P = 0.049). Characteristics of cases and controls for which significant differences between the two groups were found are shown in . Twenty-seven of the cases (40.3%) developed an infection prior to their admission versus 6% of the controls (P < 0.0001). Significant differences between the two groups were observed when comparing low levels of hemoglobin (P < 0.0001), low levels of albumin (P < 0.0001), and high creatininemia (P = 0.002).
Table 1 Characteristics of patients on treatment with vitamin K antagonists
Comparison of drug–drug interactions between cases and controls
A drug–drug interaction was observed in 91% of the cases versus 77.7% of the controls (P = 0.029); 35.8% of the cases were on antibiotic therapy versus 11% of the controls (P < 0.0001). Most of these drug–drug interactions required precaution for use. The antibiotics of most concern were penicillins (P = 0.039) and quinolones (P = 0.031). Significant differences were shown with concomitant use of anti-inflammatory drugs (P < 0.0001), anticoagulants or antiplatelet agents (P = 0.002), and amiodarone (P < 0.0001) ().
Table 2 Comparison of drug–drug interactions between cases and controls
Comparison of signs of bleeding between cases and controls
Thirty-six of the cases developed a hemorrhage (53%) versus 6% of the controls (P < 0.0001). Hematuria, hematoma, intracranial bleeding, and decreased levels of hemoglobin were predominant among patients showing a high INR. Other signs of hemorrhage, such as melena, hemoptysis, and epistaxis, were not significantly associated with an INR level above the therapeutic range. In contrast, a significant difference was seen when comparing signs of internal bleeding, such as fatigue, pallor, palpitations, syncope, and dizziness, between cases and controls ().
Table 3 Comparison of signs of bleeding between cases and controls
Management of bleeding or nonbleeding patients with high INR values
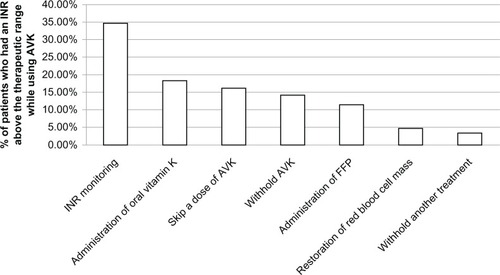
Management of bleeding or nonbleeding patients with a high INR was individualized depending on the severity, localization of the hemorrhage, and the INR value. INR monitoring was carried out for 34.5% of the patients, while 18.2% of the patients received oral vitamin K ().
Figure 1 Management of bleeding or nonbleeding patients with a high INR.
Multivariate logistic regression coefficient for INR higher than the therapeutic range
Multivariate logistic regression analysis used to quantify the relationship between these risk factors and the occurrence of ADE characterized by a high INR showed that a drug–drug interaction increased by sixfold the probability of having an INR higher than the therapeutic range (P = 0.0065). This probability was twice the value when a recent infection was present (P = 0.003), five times higher when there was concomitant use of aspirin (P = 0.0074), five times higher when there was concomitant use of amiodarone (P = 0.008), and 4.5 times higher in the case of hypoalbuminemia (P = 0.0005) ().
Table 4 Logistic regression coefficient for values of INR higher than the therapeutic range
Discussion
The risk of having an INR above the therapeutic range during AVK therapy was higher in patients over 75 years of age (P = 0.049). Similar results were found in a study that evaluated the relationship of age and other risk factors to the incidence of major bleeding during warfarin therapy.Citation13 Major bleeding occurred more frequently in patients > 75 years of age (5.1% annually) than in younger patients (1% annually), and multivariate analysis indicated that age > 75 years was the only variable independently related to primary bleeding during warfarin therapy (bleeding unrelated to organic lesion).Citation13 The mechanism of how aging causes anticoagulant-related bleeding is not known, but the elderly are the major users of AVK because the two most common indications for such treatment, atrial fibrillation and venous thromboembolism, are most prevalent in the elderly.Citation14 Another study suggested that older individuals are at a greater risk of bleeding than their younger counterparts with similar diagnoses because of increasing comorbidities.Citation15 Age is not directly responsible for increased risk of bleeding; correlates of aging, such as comorbidities and polypharmacy, may be the culprits. No gender differences were found between patients who showed an INR above therapeutic range and those who showed a normal INR. A comparison with observational studies enrolling patients with various indications for AVK showed that our findings were similar. No significant difference in bleeding rate was found between males and females.Citation16 However, a univariate analysis indicated a higher frequency of major bleeding in females treated for atrial fibrillation.Citation13
Patient-related factors, such as comorbidity and state of disease, may represent other significant risk factors for therapeutic imbalance during AVK treatment. In our study only a history of recent infection seemed to be significantly related to an INR higher than the therapeutic range (P < 0.0001). Our results were similar to those of a case-control study conducted in order to study the risk factors for a high INR range with or without bleeding complications; a significant association was found between the presence of an infectious disease or a fever and the occurrence of a hemorrhagic stroke (odds ratio [OR] = 6; P = 0.007).Citation17 Our interpretation is that infectious diseases require the use of antibiotics, which cause decreased production of vitamin K by intestinal fora and increased sensitivity to AVK. Increased catabolism of vitamin K-dependent clotting factors can be found in hypermetabolic states, such as fever, and an increased intake of nonsteroidal inflammatory drugs, frequently prescribed in the case of fever, may also increase the anticoagulant effect.Citation18 Monitoring INR should be increased in these high-risk situations.
Other comorbidities, such as high creatininemia, were significantly associated with an INR above the therapeutic range. A recent analysis of a clinical trial on treatment of patients with atrial fibrillation (the Atrial Fibrillation Follow-up Investigation of Rhythm Management [AFFIRM] study) reported that congestive heart failure, hepatic or renal disease, and diabetes were conditions, among others, significantly associated with major bleeding.Citation19 Other studies showed that a history of bleeding (especially in the gastrointestinal tract) is the patient-related factor most frequently reported to be predictive for a risk of further bleeding complications,Citation20 and that liver diseases potentiate the response to AVK by impairing synthesis of coagulation factors and usually make control of anticoagulation more difficult. In a recent review,Citation21 a history of bleeding, history of myocardial infarction, and previous cerebrovascular events were all factors associated with a higher risk of bleeding complications. Blood pressure was a critical factor for bleeding complications during AVK therapy in some,Citation22 though not all, studies.Citation23
Clinical factors, such as low hemoglobin, were found to be highly associated with an INR above the therapeutic range (P < 0.0001), and a low hemoglobin level is an indicator of ongoing hemorrhage occurring in patients with an INR above the therapeutic range. Hypoalbuminemia was also significantly associated with an INR above the therapeutic range (P < 0.0001). AVK are highly bound to plasma proteins, primarily to albumin, and hypoalbuminemia may increase the free fraction of AVK, leading to an enhanced anticoagulant effect. Our findings were similar to those of a retrospective study in which 30.2% of the cases with a high INR suffered from protein malnutrition.Citation24 In contrast, a prospective evaluation of an index for predicting major bleeding in outpatients treated with warfarin showed that bleeding risk associated with warfarin therapy can be estimated by elevated serum creatinine > 1.5 mg/dL and hematocrit < 30%.Citation25
Treatment-related factors, such as the prescribed molecule, dose, and the pathology which led to AVK treatment, were not factors of therapeutic imbalance in our study. However, the majority (98%) of patients were treated with acenocoumarol, while only 2% used warfarin since warfarin was withdrawn from the market in 1999; this made it difficult to find any association between the type of prescribed molecule and a high INR. A previous study comparing acenocoumarol with warfarin in a group of 103 patients who were treated with acenocoumarol and then changed to warfarin showed that warfarin did not appear to be better than acenocoumarol for anticoagulation in terms of INR within the therapeutic range per patient.Citation26 The majority of patients included in our study (80%) were taking 0.5 to 3 mg of acenocoumarol once daily (less than one tablet of Sintrom 4 mg). This dose was determined based on the relatively older population in our study, and thus we found no significant dose-related association. A study showed an increased risk of hemorrhage under AVK treatment when the dose of AVK was higher than that recommended.Citation27 No significant association was found between values of INR above the therapeutic range and the type of pathology that leads to AVK treatment. Our results were similar to a study on whether AVK treatment influences bleeding risk; no difference between bleeding risks was seen between patients treated for venous thromboembolism or atrial fibrillation.Citation28
Another factor of therapeutic imbalance found in our study was the use of concomitant medications (P = 0.029). This involved antibiotics (P < 0.0001), mainly penicillins and quinolones (P = 0.039 and P = 0.031, respectively). Anti-arrhythmic medications, such as amiodarone, were also significantly associated with an INR above the therapeutic range (P < 0.0001).
Siguret and collaborators showed that 69% of overdosing cases are associated with antivitamin K-potentiating drugs,Citation29 particularly anti-infectious drugs and amiodarone.Citation29 Antibiotics are commonly used in elderly patients and are classically identified as antivitamin K-potentiating drugs.Citation30 The occurrence of hemorrhage when antivitamin K is associated with antibiotics can be explained by the destruction of intestinal fora and the decrease in synthesis of vitamin K, decrease in metabolism of antivitamin K by enzymatic inhibition (fuconazole, itraconazole, and erythromycin), or decrease in protein binding (fluoroquinolones).Citation31
The occurrence of an infectious episode with metabolic changes is a risk factor for imbalance of antivitamin K. In this case it is not possible to distinguish the part related to intercurrent disease and that related to anti-infectious drugs.Citation32 Another interaction was seen with analgesics, primarily anti-inflammatory drugs (P < 0.0001), as a result of their partial inhibition of platelet activation and gastric mucosal damage causing increased risks of gastrointestinal hemorrhage.Citation33 A third interaction concerning antiplatelet agents was found (P = 0.002), especially when aspirin was used concomitantly (P = 0.006). No significant associations were found with concomitant use of antifungals or with statins or paracetamol. Among the four types of drug–drug interactions cited previously, only interactions that require precaution for use were significantly associated with an INR above the therapeutic range (P = 0.026). Two meta-analyses found a relative risk of major bleeding when AVK were combined with aspirin.Citation34,Citation35 A nested case-control study confirmed the high risk of upper gastrointestinal bleeding in patients using AVK in combination with aspirin and/or clopidogrel and reported that acetaminophen was associated with excessive warfarin anticoagulation.Citation36 A systemic overview of drug interactions with warfarin showed that co-administration with antibiotics, nonsteroidal anti-inflammatory drugs, lipid-lowering agents, and amiodarone should either be avoided or closely monitored.Citation37
Signs of bleeding were present in 53% of cases (versus 6% of controls; P < 0.0001). One study showed that 79% of patients with an INR above the therapeutic range developed a hemorrhage compared to only 16% of those with an INR within the therapeutic range (P < 0.0001).Citation27 The risk of bleeding is exacerbated by the intensity of anticoagulation; the incidence of major bleeding approximately doubled with each INR point.Citation38,Citation39 Each unit increase in INR compared with the value of INR < 2 was associated with a 42% increase in major bleedingCitation40 and 54% increase of bleeding in general.Citation39
In our study, management of patients showing a high INR with or without hemorrhagic events included INR monitoring, administration of oral vitamin K, interruption of AVK therapy, omitting one dose of AVK, and administration of fresh frozen plasma even though volume overload may make it difficult to administer an adequate fresh frozen plasma dose, particularly since these patients often have compromised cardiovascular systems.Citation41 Pooled plasma products containing factors II, IX, and X with variable amounts of factor VII and natural anticoagulant proteins C and S were not available at the tertiary care hospital in Beirut even though they are recommended when vitamin K fails to normalize the INR.Citation42
Under multivariate logistic regression analysis, significant factors for high values of INR under AVK treatment were as follows: recent infection (P = 0.003), low albumin level (P = 0.0005), concomitant use of amiodarone (P = 0.008) or aspirin (P = 0.0074), and drug–drug interaction (P = 0.0065). Multivariate analysis of another study showed similar results that excessive anticoagulation under AVK treatment was significantly associated with previous history of gastrointestinal hemorrhage (OR = 4.345, P = 0.022), fever (OR = 6.018, P = 0.007), recent antibiotic therapy (OR = 12.932, P = 0.03), and therapy with amiodarone (OR = 3.575, P = 0.022).Citation17
The interpatient and intrapatient variability in dose response, the narrow therapeutic index, and the numerous drug and dietary interactions associated with these agents have led clinicians and investigators to search for alternative agents. Three new orally administered anticoagulants (apixaban, dabigatran, and rivaroxaban) are now on the market. Apixaban and rivaroxaban are specific inhibitors of factor Xa, while dabigatran inhibits factor IIa. The predictable pharmacological profile of these new agents will allow physicians to use these drugs without the need for routine coagulation monitoring, which is the mainstay of AVK therapy. In addition, these new agents have not been shown to have any food interactions and have limited drug–drug interactions due to their minimal metabolism through the CYP450 system.Citation43
Our study is a survey conducted retrospectively and has biases related to the method and the study population. The majority of our study population had an age greater than 65 years and was a heterogeneous population with multiple pathologies and polypharmacy, making the analysis more difficult. This was especially true in cases of dementia where the patient was not aware of his/her medical history and medications, generating a high number of missing data for the collection sheet. Data such as the patient’s diet and patient’s compliance, not included in the computerized patient files, were not considered in our study, although studies have shown a significant association between these two factors and the occurrence of hemorrhagic adverse drug events under AVK. Further studies that take into account these weak points are necessary to confirm our results. Nevertheless, a strong point in our study is that the INR, the main criteria for defining a case and a control, was measured in the same laboratory, thus avoiding measurement biases from different laboratories.
Conclusion
Many factors associated with ADE pertaining to AVK are related to the patient, to the treatment itself, or to the awareness of health care professionals when prescribing and dispensing this type of oral anticoagulant. Some risk factors of therapeutic imbalance were identified, including patient’s age, intercurrent diseases, drug interactions, and the specific dose required for a particular individual to reach appropriate INR levels. Close monitoring of INR and its stabilization in the therapeutic range is required for any dose modification of AVK and acute episodes, including intercurrent infection.
Disclosure
The authors report no conflicts of interest in this work.
References
- DrouetLFiessingerJNBoneauBDecoususHMobilisation pour les antivitamines K. [Mobilization for vitamin K antagonists]Sang Thrombose Vaisseaux200012347349 French
- PatersonJMMamdaniMJuurlinkDNNaglieGLaupacisAStukelTAClinical consequences of generic warfarin substitution: an ecological studyJAMA20062961969197217062858
- PouyannePHaramburuFImbsJLBégaudBFrench Pharmacovigilance CentresHospitalisations due to adverse drug reactions: a cross sectional study in medical departmentsBMJ2000320103610764362
- ENEISAdverse events related to health care 2005 Available from: http://www.drees.sante.gouv.fr/IMG/pdf/article201017.pdfAccessed June 25, 2012
- MajorSBadrSBahlawanLDrug-related hospitalization at a tertiary teaching centre in Lebanon. Incidence, associations, and relation to self-medicating behaviorClin Pharmacol Ther19986444504619797802
- KooSKucherNNguyenPLFanikosJMarksPWGoldhaberSZThe effect of excessive anticoagulation on mortality and morbidity in hospitalized patients with anticoagulant-related major hemorrhageArch Intern Med20041641557156015277289
- Société Française de Pharmacie CliniqueDictionnaire français de l’erreur médicamenteuse. [French dictionary of medical errors] 2006 Available from: http://www.omedit-basse-normandie.fr/gallery_files/site/1533/1534/1571/2192/2824/4679.pdfAccessed Jun 2012
- AFSSAPSAntivitamine K: Fiche de transparenceParis2004 Available from: http://afssaps.sante.frAccessed June 25, 2012
- KratzAFerraroMSlussPMLewandrowskiKBLaboratory reference valuesNEJM20043511548156315470219
- Agence Nationale de Sécurité du Médicament et des Poduits de SantéAppropriate use of vitamin K antagonists 2009 Available from: http://ansm.sante.fr/Dossiers-thematiques/Anti-vitamine-K-AVK/Information-pour-les-professionnels-de-sante/(offset)/2Accessed June 25, 2012
- Thesaurus des Interactions Médicamenteuses 2012 Available from: http://ansm.sante.fr/var/ansm_site/storage/original/application/58ddaf245abd2cd75105272d69ecf5f2.pdfAccessed June 25, 2012
- Haute Autorité de SantéManagement of overdose, risk situations and hemorrhagic accidents in patients treated with vitamin K antagonists in city and hospitalSTV2008201102
- PengoVLegnaniCNoventaFPalaretiGOral anticoagulant therapy in patients with nonrheumatic atrial fibrillation and risk of bleeding – a multicenter inception cohort studyThromb Haemost20018541842211307807
- FangMCGoASHylekEMAge and the risk of warfarin-associated hemorrhage: the anticoagulation and risk factors in atrial fibrillation studyJ Am Geriatr Soc2006541231123616913990
- TornMBollenWLVan der MeerFJMVan der WallEERosendaalFRRisks of oral anticoagulant therapy with increasing ageArch Intern Med20051651527153216009869
- PalaretiGLealiNCoccheriSBleeding complications of oral anticoagulant treatment: an inception-cohort, prospective collaborative study (ISCOAT). Italian study on complications of oral anticoagulant therapyLancet19963484234288709780
- CadiouGTiretILevesqueHRisk factors for overdose of vitamin K antagonists: a case-control study conducted in patients not Selected admitted to an emergency departmentJ Clin Pharm20092827381
- JacobsLGWarfarin pharmacology, clinical management, and evaluation of hemorrhagic risk for the elderlyCardiol Clin20082615716718406992
- DiMarcoJPFlakerGWaldoALFactors affecting bleeding risk during anticoagulant therapy in patients with atrial fibrillation: observations from the Atrial Fibrillation Follow-up Investigation of Rhythm Management (AFFIRM) studyAm Heart J200514965065615990748
- McMahanDASmithDMCareyMAZhouXHRisk of major hemorrhage for outpatients treated with warfarinJ Gen Intern Med1998133113169613886
- HughesMLipGYHRisk factors for anticoagulation-related bleeding complications in patients with atrial fibrillation: a systematic reviewQJM200710059960717846060
- AbdelhafizAHWheeldonNMResults of an open-label, prospective study of anticoagulant therapy for atrial fibrillation in an outpatient anticoagulation clinicClin Ther2004261470147815531009
- LipGYFrisonLGrindMEffect of hypertension on anticoagulated patients with atrial fibrillationEur Heart J20072875275917289744
- DelayeVLes Anti-Vitamines K chez le Sujet ÂgéVal-de-MarneUniversité Paris2006
- BeythRJQuinnLMLandefeldCSProspective evaluation of an index for predicting the risk of major bleeding in outpatients treated with warfarinAm J Med1998105291999727814
- BarcellonaDVanniniMLFenuLBalestrieriCMaronqiuFWarfarin or acenocoumarol: which is better in the management of oral anticoagulants?Thromb Haemost19988068999029869157
- Al–HajjeACalopNBossonJLCalopJAllenetBWhich factors associated to hemorrhagic adverse drug events related to anti vitaminK. Ann Pharm Fr20106813643
- Van Der HeijdenJFRekkéBHuttenBANon-fatal major bleeding during treatment with vitamin K antagonists: influence of soluble thrombomodulin and mutations in the propeptide of coagulation factor IXThromb Haemost20042711041109
- SiguretVEsquirolCDebrayMSurdosage en anti-vitamine K dans une population de patients hospitalisés âgés de plus de 70 ans: enquête prospective sur un an. [Overdoses vitamin K antagonists in a population of hospitalized patients aged over 70 years: A one-year prospective study]Presse Med200332972977 French12876525
- SanoskiCABaumanJLClinical observations with the amiodarone/warfarine interaction: Dosing relationships with long-termChest2002121192311796427
- VittecoqDAnti-vitamines K (AVK): Texte approuvé par la commission d’AMM de l’AFSSAPS.2008. [Vitamin K antagonists (VKA): Text approved by the AMM committee of AFSSAPS. 2008] Available from: http://www.afssaps.fr/var/afssaps_site/storage/original/application.pdfAccessed June 25, 2012 French
- SiguretVEsquirolCDebrayMOverdoses vitamin K antagonists in a population of hospitalized patients aged over 70 years: A one-year prospective studyPresse Med20033297297712876525
- HartRGBenaventeOPearceLAIncreased risk of intracranial hemorrhage when aspirin is combined with warfarin: a meta-analysis and hypothesisCerebrovasc Dis19999421521710393408
- FinstererJStollbergerCStrategies for primary and secondary stroke prevention in atrial fibrillationNeth J Med20086632733318809979
- HallasJDallMAndriesAUse of single and combined antithrombotic therapy and risk of serious upper gastrointestinal bleeding: population based case-control studyBMJ200633372616984924
- HylekEHeimanHSkatesSSheehanMSingerDAcetaminophen and other risk factors for excessive warfarin anticoagulationJAMA199827996576629496982
- HolbrookAPereiraJLabirisRSystematic overview of warfarin and its drug and food interactionsArch Intern Med2005165101095110615911722
- LevineMNRaskobGLandefeldSKearonCHemorrhagic complications of anticoagulant treatmentChest2001119SupplS108S121
- Van der MeerFJMRosendaalFRVandenbrouckeJPBleeding complications in oral anticoagulant therapy: an analysis of risk factorsArch Intern Med1993153155715628323419
- Van der MeerFJMRosendaalFRVandenbrouckeJPBrietEAssessment of a bleeding risk index in two cohorts of patients treated with oral anticoagulantsThromb Haemost19967612168819244
- BoulisNMBobekMPSchmaierAHoffJTUse of factor IX complex in warfarin-related intracranial hemorrhageNeurosurgery1999451113111810549927
- PindurGMorsdorfSThe use of prothrombin complex concentrates in the treatment of hemorrhages induced by oral anticoagulationThromb Res199995SupplS57S6110499910
- GarciaDLibbyECrowtherMAThe new oral anticoagulantsBlood20101151152019880491