
Abstract
Introduction
Cardiovascular diseases (CVD) are the leading cause of mortality in Kazakhstan. In the last decade, Kazakhstan has carried out a number of reforms in the healthcare sector, in particular, to reduce mortality from significant diseases, including CVD. This study aimed to provide the trend of avoidable mortality from CVD in Kazakhstan.
Methods
We extracted data from the Bureau of National Statistics of the Agency for Strategic Planning and Reforms of the Republic of Kazakhstan on population by age; mortality rates from chronic rheumatic heart disease (I05-I09); hypertensive diseases (I10-I15); ischaemic heart disease (I20-I25); cerebrovascular diseases (I60-I69) from 2011 to 2021, by gender and 5-year age group (0, 1–4, 5–9, 74). We applied join point regression to calculate the average annual percentage change (AAPC). In addition, crude mortality and trends were calculated per 100,000 population.
Results
The avoidable mortality rates, including treatable and preventable mortality decreased between 2011 and 2019 and then increased in the last two years (2020 and 2021) in all four studied disease groups. The AAPC showed that total avoidable mortality rates decreased between 2011 and 2021–6.0 points (−10.6 to – 1.1) (p = 0.017), whereas in males −4.2 (−8.3 to 0.1) and females – 5.1 (−8.8 to −1.3) (p = 0.009). Avoidable mortality rates from ischemic heart disease, cerebrovascular and hypertensive disease has been reduced stronger in male compared to female. The crude mortality declined over the period given; however, among young people mortality is still high.
Discussion
Our findings showed that avoidable mortality from CVD decreased over the last years, which could be related to the policy on strengthening the primary care on early diagnosis and detection of CVD and its risk factors. However, primary healthcare facilities need to improve activities on health literacy (drug adherence, risk factors) of the population, including the prevention of CVD.
Introduction
Cardiovascular diseases (CVDs) are the leading cause of mortality worldwide. According to the World Health Organization annually, 17.9 million deaths relate to CVDCitation1 and this number increased over the 19 years (from 12.1 million in 1990, to 18.6 million in 2019).Citation2 In Europe CVD causes 3.9 million deaths,Citation3 in Kazakhstan the overall mortality rate from CVD was 219 per 100,000 in 2015,Citation4 which is higher than in developed countries.Citation5 Studies have shown that the provision of timely preventive care to patients with CVD can reduce complications and the costs associated with the treatment.Citation6,Citation7
A comprehensive analysis of health indicators allows to monitor the performance of the healthcare system and identify the strategy to improve the health of the population. Rutstein et alCitation8 presented in 1976 a tool for measuring the quality of medical care by introducing the concept of “unnecessary premature death”, where it was proposed that conditions in which death should not occur if “timely and effective” medical care is provided. Canada,Citation9 the United KingdomCitation10 and the European UnionCitation11 have introduced measures of avoidable mortality that allow the evaluation of healthcare systems in reducing premature mortality from various diseases.Citation12 Avoidable mortality includes causes of death from preventable mortality (can be avoided through effective public health and primary prevention interventions) and treatable mortality (can be avoided through timely and effective health care interventions, including secondary prevention and treatment).Citation12
Kazakhstan adheres to the policy of implementing the Astana Declaration and universal health coverage (UHC).Citation13 Hence, government policy is aimed to strengthen primary care, where special attention is paid to the provision of person-centered care.Citation14 Currently, a number of screening programs (for early detection of arterial hypertension, coronary heart disease and diabetes, and early detection of behavioral risk factors), as well as disease management programs (primary hypertension, diabetes mellitus and chronic heart failure)Citation15 are being implemented in the primary care. Earlier studies presented the results of age-standardized data on CVD mortality by sex and regions of Kazakhstan.Citation4,Citation16 However, no data is available on avoidable mortality from CVD. Thus, in this study, we described trends in avoidable mortality from CVD in Kazakhstan from 2011 to 2021.
Methods
Data Source
From the Bureau of National Statistics of the Agency for Strategic Planning and Reforms of the Republic of Kazakhstan (https://stat.gov.kz), the following data was obtained to analyse the mortality rates: population by age categories in the Republic of Kazakhstan; mortality rates due to CVD from 2011 to 2021, by gender and 5-year age group (0, 1–4, 5–9, 10–14, 70–74). The causes of mortality were classified according to the 10th revision of the International Classification of Diseases—ICD 10 and included Chronic rheumatic heart disease (I05-I09); Hypertensive diseases (I10-I15); Ischaemic heart disease (I20-I25); Cerebrovascular diseases (I60-I69). The definition of avoidable mortality was used from the UK Office of National Statistics.Citation17 Selection of causes of death for the lists of preventable and treatable causes was based on Organisation for Economic Cooperation and Development (OECD)/Eurostat lists of preventable and treatable causes of death (January 2022 version).Citation18 Avoidable mortality includes two components: preventable (causes of death that can be mainly avoided through effective public health and primary prevention interventions) and treatable (causes of death that can be mainly avoided through timely and effective health care interventions, including secondary prevention and treatment) mortality.Citation18 In this study, we analyzed preventable and treatable mortality for four types of diseases separately and by sex.
Statistical Analysis
We used the age-standardised death rates given from the OECD 2015,Citation12 and corresponding 95% confidence intervals (95% CIs) were calculated for the age group 0–74 years and gender.
To calculate preventable, treatable and avoidable mortality, there is a need to sum the standardized mortality rate (tst) by age group, including the causes of death.
for i=1. m causes of death included as preventable.
for i=1. m causes of death included as treatable.
for i=1. m causes of death included as avoidable.
The standardized death rate is calculated as follows:
where “n” number of age groups considered for adjustment;
standard population
age group (j=1, …, n)
is the total standardized population;
and
is a weight indicator
age group, where
the number of deaths in
age group (j = 1, · · ·, n);
population
age group measured per 100,000 inhabitants.
To identify changes in avoidable mortality rate trends for the period 2011–2021, join point regression (Joinpoint Regression Program 4.9.1.0) was used to calculate the average annual percentage change (AAPC)Citation19,Citation20 for every age and sex group. Joinpoint calculates the trend in segments whose start and end are defined to best fit the data; sometimes, it is useful to summarize the trend over a fixed specified interval. Crude mortality rates were calculated per 100,000 population. The trend function in Excel was used to calculate a linear trend line based on a given linear data set (the forecast values of Y (years) were taken for the given values of the array × (number of deaths).
Results
The contribution of age-adjusted avoidable, treatable and preventable mortality from cardiovascular disease during 2011–2021 is shown in “”. The age-adjusted avoidable mortality rates decreased between 2011 and 2019, from 267.6 (95% CI: 264.1–271.1) to 126.4 (95% CI: 124.2–128.5) per 100,000 population (pop.), after which there has been an increase up to 165.8 (95% CI: 163.5–168.2) per 100,000 pop. in 2021 (). Preventable (from 132.2 (95% CI: 129.8–134.7) to 62.6 (95% CI: 61.1–64.1)) and treatable mortality from 135.3 (95% CI: 132.9–137.8) to 63.8 (95% CI: 62.3–65.3)) dropped about twice from 2011 to 2019, following an increase in 2021 of 82.4 (95% CI: 80.8–84.1) and 83.4 (95% CI: 81.7–85.0), respectively (see Supplementary Table 1).
Figure 1 Age-adjusted avoidable, treatable and preventable mortality rate from cardiovascular disease.
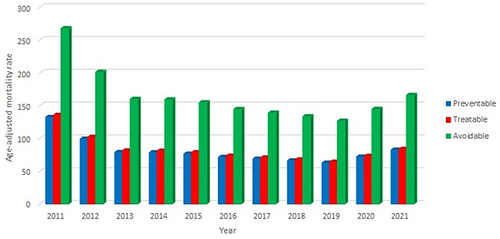
Males consistently experienced higher (about twice) avoidable mortality rate compared to females (). The AAPC showed that total avoidable mortality rates decreased between 2011 and 2021 from −10.6 to – 1.1 (– 6.0 points) (p = 0.017), whereas in males −4.2 (−8.3 to 0.1) and in females – 5.1 (−8.8 to −1.3) (p = 0.009). Significant changes can be seen in the first five years (2011–2015) in both genders, in males −11.2 (−14.6 to −7.5) (p < 0.001) and in females −12.8 (−20.2 to −4.8) (p = 0.002), ().
Table 1 Number and Rate of Avoidable Mortality from Cardiovascular Disease (100,000 Population), by Age and Sex in Kazakhstan from 2011 to 2021
In all four diseases, the avoidable mortality rate (AMR) decreased over the given period of time. The most common cause of death was ischemic heart disease, which declined from 127.8 (95% CI: 125.4–130.2) to 86.7 (95% CI: 85.0–88.4) per 100,000 pop. and cerebrovascular diseases 115.7 (95% CI: 113.4–118.0) to 71.6 (95% CI: 70.1–73.1) per 100,000 pop. AAPC in ischemic heart disease mortality declined to −5.5 (95% CI: −11.1 to 0.4) and in cerebrovascular diseases to −5.5 (95% CI: −9.1 to – 1.7) (p = 0.005) respectively ().
Table 2 Trends in Age-Adjusted Rates of Avoidable Mortality Attributed to Cardiovascular Disease in Kazakhstan, 2011–2021
The AMR for hypertensive diseases and chronic rheumatic heart disease were relatively low compared to ischemic heart disease and cerebrovascular disease. AMR for hypertensive diseases dropped about three times during 2011 and 2021 from 21.0 (95% CI: 21.1–22.0) to 6.6 (95% CI: 6.1–7.1) per 100,000 pop.; AAPC −9.6 (95% CI: −17.4 to 1.0) (p = 0.029). AMR for chronic rheumatic heart disease decreased from 3.1 (95% CI: 2.7–3.5) to 1.0 (95% CI: 0.8–1.1) per 100,000 pop. and AAPC −11.0 (95% CI: −13.2 to −8.8) (p < 0.001) per 100,000 pop. ().
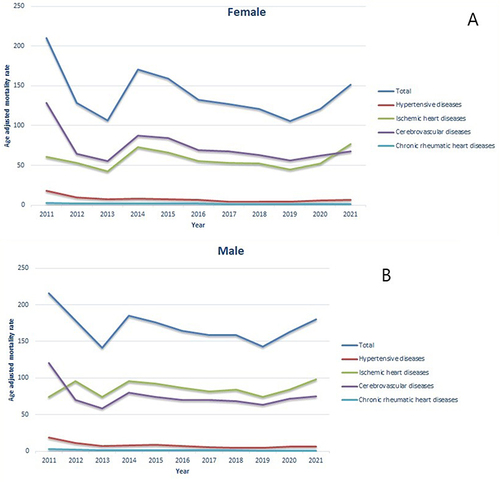
AMR from hypertensive disease was higher in males compared to females. In males, it has decreased rapidly by about twice in the first year (from 26.8 (95% CI: 25.1–28.5) to 16.8 (95% CI: 15.7–18.0)), after which the number has declined, reaching a peak of 5.8 (95% CI: 5.0–6.5) in 2019, following that it was observed an increase up to 8.5 (95% CI: 7.6–9.3) in 2021. Among females, a noticeable decline has been observed between 2011 and 2013 from 16.7 (95% CI: 15.6–17.9) to 7.9 (95% CI: 7.2–8.6), after which there has been a stable decrease until 2019 of 3.1 (95% CI: 2.7–3.6) and an increase up to 5.2 (95% CI: 4.7–5.8) by 2021. AMR from chronic rheumatic heart diseases slightly prevails among females in the most studied years and in both groups the rate decreased. By contrast, the ischemic heart diseases were higher among males, which has decreased from 202.0 (95% CI: 197.3–206.7) to 104.2 (95% CI: 101.2–107.2), and in females from 73.4 (95% CI: 71.0–75.8) to 29.8 (95% CI: 28.5–31.2) between 2011 and 2019 and then rose in both genders to 132.6 (95% CI: 129.3–135.9) and 53.2 (95% CI: 51.5–54.9), respectively. Cerebrovascular diseases were higher among males (about twice) in comparison to females in all years. The rates decreased from 158.0 (95% CI: 153.7–162.2) to 85.2 (95% CI: 82.5–88.0) in males and from 85.9 (95% CI: 83.3–88.5) to 40.5 (95% CI: 38.9–42.1) in females until 2019, after which increased to 101.8 (95% CI: 98.9–11.9) and 49.7 (95% CI: 48.1–51.4) per 100,000 pop. (“ and )” and Supplementary Table 2).
Figure 2 (A) Age-adjusted mortality rate from cardiovascular diseases in Kazakhstan, 2011–2021 (in female). (B) Age adjusted mortality rate from cardiovascular diseases in Kazakhstan, 2011–2021 (in male).
Crude Mortality
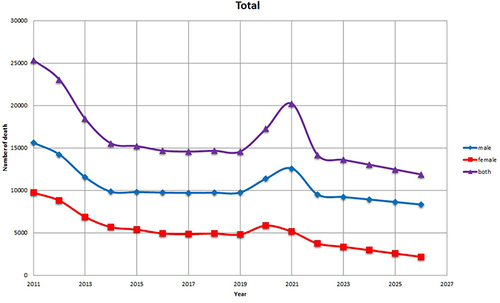
For all four diseases (Chronic rheumatic heart disease (I05-I09); Hypertensive diseases (I10-I15); Ischaemic heart disease (I20-I25); Cerebrovascular diseases (I60-I69)), mortality rates have been reduced between 2011 and 2019, after which an increase was observed between 2020 and 2021. Trends for all four diseases are expected to decline by 2027 (“”, “Supplementary Figure 1”). In general, the mortality rate for males was higher than for females. Only mortality from chronic rheumatic heart diseases was higher in females compared to males (Supplementary Table 3).
Figure 3 Trends in crude mortality from circulatory system disease (Chronic rheumatic heart disease (I05-I09); Hypertensive diseases (I10-I15); Ischaemic heart disease (I20-I25); Cerebrovascular diseases (I60-I69).).
Mortality from ischaemic heart diseases in all age groups decreased from 2011 to 2019. An increase in mortality since 2019 has been observed in the age group over 50–54 years old, whereas an increase in mortality under 50 years of age has been registered in 2020 (Supplementary Table 3).
A slight increase in mortality from cerebrovascular diseases was observed in the age group of 40–49 years in the period 2018–2020, after which it could be seen a sharp increase. In the group over 50 years of age, a sharp increase in mortality began in 2020 (Supplementary Table 3). Mortality rate from hypertensive diseases doubled between 2020 and 2021 in the group of over 50 years.
Discussion
This study found an overall decrease in avoidable and crude mortality from CVD during 2011 and 2021 in Kazakhstan. Gregory A. Roth et al note that there is a decrease in burden of CVD in several countries.Citation21 In Korea, it was found consistent decreasing trends for mortalities from rheumatic heart disease and hypertensive heart disease, which is similar to Kazakhstan.Citation22
In Kazakhstan, this can be related to the policy to support the provision of UHC, and the strengthening of primary care in Kazakhstan.Citation23 The implementation of the policy on early diagnosis has begun within the introduction of State programs, which include screening programs for the early detection of CVD and risk factors, which has led to an increase in morbidity rates and a decrease in mortality.Citation24 Moreover, the positive dynamics may be associated with the implementation of disease management programs (DMPs);Citation25 for instance, the World Bank report indicates that 75% of patients with hypertension participating in the DMP stabilized their blood pressure, improved performance of patients with diabetes, and reduced hospitalization rates for patients with heart failure.Citation26 However, the avoidable mortality in Kazakhstan from CVD remains high compared to developed countries.Citation27,Citation28
Aringazina et al identified that for Central Asian countries, the leading cause of premature mortality from CVD was due to ischemic heart disease and stroke.Citation4 Similarly, in studies in developed countries, we also found a higher avoidable mortality rate from ischemic heart disease and cerebrovascular disease and a higher rate among males compared to females.Citation19,Citation29 A high mortality rate from CVD among males could be due to the ethnic characteristics of the Kazakh population,Citation16 as well as to a higher commitment to a healthy lifestyle in women compared to men.Citation30 Moreover, Sharma et alCitation31 identified a number of risk factors affecting the occurrence of CVD in women, which indicates the needs of different group approaches to care depending on gender characteristics.
On the other hand, it is worth noting that over the past two years (from 2019 to 2021), we have seen a negative growth trend, which is most likely due to the COVID pandemic similar to other countries, when the health sector faced the difficulty of providing timely care for chronic patients.Citation32,Citation33
Nevertheless, in some primary healthcare facilities in Kazakhstan, there has been identified the need to strengthen the work (as screening programs on CVD, etc) to provide comprehensive care to patients with CVD.Citation34 In addition, Kulkaeva et al observed the low awareness of the Kazak population regarding CVD risk factors,Citation35 which led to intensify the work in this area, including among rural residents.Citation36 Other factors which influence high levels of mortality can include low adherence of patients with arterial hypertension to treatment, and very low clinical efficacy.Citation37 Increasing health literacy of the population, including the prevention of CVD, is important to reduce mortality rates. Considering that primary care in Kazakhstan has departments for disease prevention, managers should make it an important priority to increase literacy among the population served by this medical organization. High mortality rate from CVD among the male population deserves special attention and primary health care needs to consider separate programs for this category based on international practice.Citation37
Future direction: A more in-depth study of the avoidable causes of mortality is needed, depending on the location (urban or rural area), the influence of social status (high and low living standards), the level of education, health literacy. This will allow decision makers to justify in greater details the allocation of available health resources. Moreover, other avoidable circulatory system diseases (Venous thromboembolism (I26, I80, I82.9); Other atherosclerosis (I70, I73.9); Aortic aneurysm (I71)) can be calculated in future works.
Conclusion
In the last decade, Kazakhstan has achieved significant progress in decreasing the avoidable mortality from CVD. However, high differences in mortality rate are still observed between genders. Fortunately, the State policies and strategies allow the implementation of programs that promote early detection and provide person-centered care, which can subsequently contribute to reduction in CVD mortality rates.
Ethical Approval
The study was approved by the Local Ethics Committee of Kazakh National Medical University (Protocol number 4 (140) 03 May 2023), Almaty, Kazakhstan. Data accessed complied with relevant data protection and privacy regulations.
Disclosure
The authors declare that they have no competing interests in this work.
Acknowledgment
The authors would like to thank Giselle Sarganas (PhD) and Kamshat Tolganbayeva for externally reviewing the article and providing recommendations for its improvement.
Additional information
Funding
References
- Available from: https://www.who.int/health-topics/cardiovascular-diseases#tab=tab_1. Accessed April 18, 2023.
- Roth GA, Mensah GA, Johnson CO, et al. Global burden of cardiovascular diseases and risk factors, 1990–2019: update from the GBD 2019 study. J Am Coll Cardiol. 2020;76(25):2982–3021. doi:10.1016/j.jacc.2020.11.010
- Wilkins E, Wilson L, Wickramasinghe K, et al. European Cardiovascular Disease Statistics 2017. Brussels: European Heart Network; 2017.
- Aringazina A, Kuandikov T, Arkhipov V. Burden of the cardiovascular diseases in Central Asia. Cent Asian J Glob Health. 2018;7(1):321. doi:10.5195/cajgh.2018.321
- Movsisyan NK, Vinciguerra M, Medina-Inojosa JR, Lopez-Jimenez F. Cardiovascular diseases in Central and Eastern Europe: a call for more surveillance and evidence-based health promotion. Ann Glob Health. 2020;86(1):21. doi:10.5334/aogh.2713
- Uthman OA, Al-Khudairy L, Nduka CU, et al. Determining optimal strategies for primary prevention of cardiovascular disease: systematic review, cost-effectiveness review and network meta-analysis protocol. Syst Rev. 2020;9(1):105. doi:10.1186/s13643-020-01366-x
- Gheorghe A, Griffiths U, Murphy A, Legido-Quigley H, Lamptey P, Perel P. The economic burden of cardiovascular disease and hypertension in low- and middle-income countries: a systematic review. BMC Public Health. 2018;18(1):975. doi:10.1186/s12889-018-5806-x
- Rutstein DD, Berenberg W, Chalmers TC, et al. Measuring the quality of medical care. N Engl J Med. 1976;294(11):7. doi:10.1056/NEJM197603112941104
- Canadian Institute for Health Information. Health indicators 2012. Ottawa, Ontario: Canadian Institute for Health Information; 2012. Available from: https://secure.cihi.ca/free_products/health_indicators_2012_en.pdf. Accessed August 15, 2023.
- Office for National Statistics. Avoidable mortality in England and Wales, 2011. Newport, Wales: Office for National Statistics; 2013. Available from: http://www.ons.gov.uk/ons/dcp171778_311826.pdf. Accessed August 15, 2023.
- AMIEHS. Avoidable mortality in the European Union: towards better indicators for the effectiveness of health systems. Rotterdam, Netherlands: 2011. Available from: http://amiehs.lshtm.ac.uk/publications/reports/amiehs%20final%20report%20vol%20i.pdf.
- OECD Health Statistics Definitions, sources and methods; 2022. Available from: https://stats.oecd.org/index.aspx?queryid=96018. Accessed August 15, 2023.
- Kluge H, Kelley E, Birtanov Y, et al. Implementing the renewed vision for primary health care in the declaration of Astana: the time is now. Prim Health Care Res Dev. 2019;20:e137. doi:10.1017/S1463423619000719
- World Health Organization European Centre For Primary Health Care. Annual report 2020–2021 WHO European Centre For Primary Health Care Document number: WHO/EURO:2022-5652-45417-64995 Available from: https://www.who.int/europe/teams/centre-for-primary-health-care-(kaz). Accessed August 15, 2023.
- Kazakhstan health sector technology transfer and institutional reform (P101928 Report No: ICR00003816). Available from: https://projects.worldbank.org/en/projects-operations/document-detail/P101928?type=projects. Accessed August 15, 2023.
- Davletov K, McKee M, Berkinbayev S, Battakova Z, Vujnovic M, Rechel B. Regional differences in cardiovascular mortality in Kazakhstan: further evidence for the ‘Russian mortality paradox’? Eur J Public Health. 2015;25(5):890–894. doi:10.1093/eurpub/ckv019
- Olatunde O, Windsor-Shellard B, Campbell A. Revised definition of avoidable mortality. UK Office for National Statistics; 2016. Available from: https://www.ons.gov.uk/file?uri=/aboutus/whatwedo/statistics/consultationsandsurveys/allconsultationsandsurveys/reviewofavoidablemortalitydefinition/reviseddefinitionofavoidablemortalityandnewdefinitionforchildrenandyoungpeople.doc. Accessed August 15, 2023.
- Avoidable mortality: OECD/Eurostat lists of preventable and treatable causes of death (January 2022 version); 2022. Available from: https://www.oecd.org/health/health-systems/Avoidable-mortality-2019-Joint-OECD-Eurostat-List-preventable-treatable-causes-of-death.pdf. Accessed August 15, 2023.
- Wilson L, Bhatnagar P, Townsend N. Comparing trends in mortality from cardiovascular disease and cancer in the United Kingdom, 1983–2013: joinpoint regression analysis. Popul Health Metr. 2017;15(1):23. doi:10.1186/s12963-017-0141-5
- Centers for Disease Control and Prevention (CDC). Vital signs: avoidable deaths from heart disease, stroke, and hypertensive disease – United States, 2001–2010. MMWR Morb Mortal Wkly Rep. 2013;62(35):721–727.
- Roth GA, Johnson C, Abajobir A, et al. Global, regional, and national burden of cardiovascular diseases for 10 causes, 1990 to 2015. J Am Coll Cardiol. 2017;70(1):1–25. doi:10.1016/j.jacc.2017.04.052
- Lee SW, Kim HC, Lee HS, Suh I. Thirty-year trends in mortality from cardiovascular diseases in Korea. Korean Circ J. 2015;45(3):202–209. doi:10.4070/kcj.2015.45.3.202
- Fleck F. Rocky road from the Semashko to a new health model. Bull World Health Organ. 2013;91:320–321. doi:10.2471/BLT.13.030513
- Mukasheva G, Abenova M, Shaltynov A, et al. Incidence and mortality of cardiovascular disease in the Republic of Kazakhstan: 2004–2017. Iran J Public Health. 2022;51(4):821–830. doi:10.18502/ijph.v51i4.9243
- Ministry of Health of the Republic of Kazakhstan. On the implementation of the program for the management of chronic noncommunicable diseases in the pilot regions. Order No. 211; 2013. Available from: https://online.zakon.kz/Document/?doc_id=31436570. Accessed August 15, 2023.
- World Bank. Implementation completion and results report 4883-KZ, Report No: ICR00003816; 2017. Available from: http://documents.worldbank.org/curated/en/823341515169244215/pdf/Implementation-Completion-and-Results-Report-ICR-Document-P101928-2017-12-28-16-26-01022018.pdf. Accessed August 15, 2023.
- Lenzi J, Reno C, Skrule J, et al. Excess cardiovascular mortality in Latvia: a novel approach based on patient-level data to estimate the separate contributions of primary prevention, accessibility and quality of hospital care. Int J Health Policy Manag. 2022;11(6):820–828. doi:10.34172/ijhpm.2020.229
- OECD avoidable mortality. Available from: https://stats.oecd.org/index.aspx?queryid=96018. Accessed August 15, 2023.
- Feller A, Schmidlin K, Clough-Gorr KM. Trends and socioeconomic inequalities in amenable mortality in Switzerland with international comparisons. Swiss Med Wkly. 2017;147:w14478. doi:10.4414/smw.2017.14478
- Walli-Attaei M, Joseph P, Rosengren A, et al. Variations between women and men in risk factors, treatments, cardiovascular disease incidence, and death in 27 high-income, middle-income, and low-income countries (PURE): a prospective cohort study. Lancet. 2020;396(10244):97–109. doi:10.1016/S0140-6736(20)30543-2
- Sharma S, Wood MJ. The global burden of cardiovascular disease in women. Curr Treat Options Cardiovasc Med. 2018;20(10):81. doi:10.1007/s11936-018-0676-1
- Sidney S, Lee C, Liu J, Khan SS, Lloyd-Jones DM, Rana JS. Age-adjusted mortality rates and age and risk-associated contributions to change in heart disease and stroke mortality, 2011–2019 and 2019–2020. JAMA Netw Open. 2022;5(3):e223872. doi:10.1001/jamanetworkopen.2022.3872
- Bae S, Kim SR, Kim M, Shim WJ, Park S-M. et al Impact of cardiovascular disease and risk factors on fatal outcomes in patients with COVID-19 according to age: a systematic review and meta-analysis. Heart. 2021;107:373–380. doi:10.1136/heartjnl-2020-317901
- Bekbergenova Z, Derbissalina G, Umbetzhanova A, Koikov V, Bedelbayeva G. Evaluating the effectiveness of a screening program for cardiovascular diseases in Kazakhstan. Eur J Public Health. 2019;29(Supplement_4):ckz186.229. doi:10.1093/eurpub/ckz186.229
- Kulkayeva G, Harun-Or-Rashid M, Yoshida Y, Tulebayev K, Sakamoto J. Cardiovascular disease risk factors among rural Kazakh population. Nagoya J Med Sci. 2012;74(1–2):51–61.
- Shayakhmetov SS, Toguzbayeva KK, Ismailova AA, Tabibi R, Derbishalieva ZK, Dzhusupov KO. Health literacy of rural population of Kazakhstan. Iran J Public Health. 2020;49(7):1269–1277. doi:10.18502/ijph.v49i7.3580
- Rosu MB, Oliffe JL, Kelly MT. Nurse practitioners and men’s primary health care. Am J Mens Health. 2017;11(5):1501–1511. doi:10.1177/1557988315617721