
Abstract
Lipids disorder is the principal cause of atherosclerosis and may present with several forms, according to blood lipoprotein prevalence. One of the most common forms is combined dyslipidemia, characterized by high levels of triglycerides and low level of high-density lipoprotein. Single lipid-lowering drugs may have very selective effect on lipoproteins; hence, the need to use multiple therapy against dyslipidemia. However, the risk of toxicity is a concerning issue. In this review, the effect and safety of an approved combination therapy with simvastatin plus fenofibrate are described, with an analysis of pros and cons resulting from randomized multicenter trials, meta-analyses, animal models, and case reports as well.
Introduction
Cardiovascular disease (CVD) represents the first cause of death and morbidity of the western countries, despite the progress occurred in the treatment and prevention during the last decades; its prevalence is foreseen to remain stable until 2020, as recent projections illustrate,Citation1 and is continuously increasing also in new developing countries, probably on the basis of the bad influence of western lifestyle and poor awareness of cardiovascular risk among people.Citation1–Citation4
The principal cause of CVD is atherosclerosis, whose development is largely conditioned also by modifiable risk factors, such as smoke, impaired metabolism of lipids and carbohydrates, hypertension, sedentary life, and obesity.Citation2–Citation8
The role of high levels of cholesterol in atherosclerosis pathogenesis is unquestionedCitation5–Citation8 and, while some of the aforementioned risk factors can be directly prevented and treated, dyslipidemia (impaired metabolism of lipids) is hardly manageable for two main reasons: 1) it could have a genetic/familiar component in its genesis and 2) many other extra-cardiac diseases at relatively high incidence and prevalence can engender impairment in lipid control aside from alimentary intake (diabetes mellitus [DM], hypothyroidism, HIV/AIDS, chronic kidney disease, Cushing syndrome, drugs, and alcohol abuse).Citation9,Citation10
Even if the use of statins has been well established in clinical practice for primary and secondary prevention,Citation11,Citation12 CVD risk still remains high in some populations. Fibrates may therefore represent a further pharmacological tool against dyslipidemia. Current international guidelines suggest lowering low-density lipoprotein (LDL) as the principal goal of the therapy for primary and secondary preventionCitation13,Citation14 and non-high-density lipoprotein (HDL) cholesterol, mainly triglyceride (TG) levels, is set as a secondary target of prevention. Since statins contribute to TG decrease is limited, the co-administration of fibrates can further reduce the CVD risk. Experts, however, prudently recommend combined therapy in statin-resistant patients (level of recommendation IIb; class C) because data in favor of double-drug therapy efficacy compared to monotherapy are not conclusive. Among the many possible and existing combinations, the most widely used is simvastatin plus fenofibrate. Nevertheless, the real and net benefit of this specific pharmacological association is still debated.
Other biomarkers (C-reactive protein, fibrinogen, and homocysteine) strongly correlate with dyslipidemia and CV risk, and the effect of these lipid-lowering drugs on such biomarkers is also described in this review.
Methods
Until April 2016, an online search was carried out on PubMed using the following keywords in combination: “adverse effects, cardiovascular disease, combined dyslipidemia, diabetes mellitus, dyslipidemia, fenofibrate, fenofibric acid, fibrate, mixed dyslipidemia, lipid-lowering medications, simvastatin, simvastatin and fenofibrate, statin, statin and fibrate.” After a thorough search, the most relevant randomized clinical trials and comments with regard to reviews, original papers, and case reports were included.
Definition of combined dyslipidemia (CD)
Mixed dyslipidemia or CD is qualitatively defined as an impairment of lipid metabolism characterized by high levels of TG carried within very-low-density lipoprotein (VLDL) and intermediate-density lipoprotein (IDL), low levels of HDL and higher amount of small and dense LDL (sd-LDL) than normal.Citation15 TG-rich lipoproteins (included Lp-a) are also named Apo-B fraction, since it is the prevalent apo-protein expressed on its surface and constitutes a more accurate measurement of TG-rich lipoprotein because of stoichiometric relation compared to whole LDL concentration.Citation16,Citation17 Furthermore, high values of Apo-B correlate with atherosclerosis and coronary heart disease (CHD).Citation18
A quantitative definition of CD is missing because different cutoff levels were used in studies that recruited people of different age and ethnicity. This disorder is related to a high atherogenic risk profile (hence “atherogenic dyslipidemia”) and is usually associated with other dysmetabolic patterns such as insulin resistance or overt diabetes and obesity, whose essential pathological features are endothelial dysfunction and high risk of thrombosis.Citation15,Citation19 Non-HDL cholesterol represents the sum of IDL, LDL, and VLDL, and sd-LDL is a particular type of LDL characteristically linked to mixed dyslipidemia: the reduction in cholesterol esters and the increase in TG reduce LDL diameter; atherogenic potential is elevated since they are less affine to LDL receptor and the small size increases the accessibility to subintimal space.Citation20,Citation21 Additionally, in type 2 DM (DM2) patients (a condition frequently associated with this phenotype),Citation22 they are more prone to glycation, which further increases its atherogenic effect.Citation23 On the other hand, HDL in the same context of DM2 can be modified by oxidative stress, becoming less protective.Citation24
Epidemiologically, CD prevalence has been estimated to be present in one out of ten subjects in general population and in 15% of statin-treated patients.Citation17 The overlap with DM2 increases the incidence of CD to >50% and the CVD risk is three to four times compared to nondiabetic people and, moreover, many interracial difference exist.Citation17,Citation25
The reduction in LDL only halves the CHD risk; therefore, other lipoproteins are involved in the ongoing atherosclerosis.Citation15 Consequently, although LDL-C has been controlled with optimal statin therapy and/or diet, patients with dysfunctional HDL and elevated TG and sd-LDL maintain a hidden CV risk, namely, the “residual CVD risk.”Citation24
Simvastatin
Statins are the most efficacious lipid-lowering agents. Competitive inhibition of 3-hydroxy-3-methyl-glutaryl-coenzyme A reductase, enzyme catalyzing the conversion of HMG-coA to mevalonic acid, blocks a necessary step in the biosynthesis of cholesterol thanks to a mevalonic-acid-like terminal. Low intra-hepatic levels of cholesterol increase LDL-C receptor expression and therefore removal of this lipoprotein from blood. Some studies indicate that hepatic VLDL production is also decreased due to cholesterol synthesis reduction, cholesterol being a basic component of VLDL; accordingly statins lower TG contained in VLDL, perhaps through direct activation of peroxisome proliferator-activated receptor (PPAR)-α, the same molecular target of fibrates.Citation26,Citation27
Simvastatin was discovered in 1979 as semisynthetic fermentation product of Aspergillus terreus. It is administered as a prodrug, which is rapidly converted in the liver from inactive lactone to its acid form (). LDL reduction ranges by 20%–48%, from the lowest (10 mg) to the highest dose (80 mg).Citation28–Citation31
Table 1 Pharmacokinetic profile
Simvastatin reduces CV risk as confirmed in large trials. Single study observation reports that simvastatin is able to increase HDL more than atorvastatin.Citation32 Statins are able to stabilize atherosclerotic plaque, and simvastatin has provided evidence of its important contribute.Citation33,Citation34 Furthermore it can, independently from dosages, decrease hs-CRP levels in CHD patientsCitation35 and also prevent organ damage (cardiac remodeling after ischemic and nonischemic injury).Citation36,Citation37
The 4S trial,Citation38 a multicenter, randomized, double-blind, placebo-controlled study, showed that cardiovascular risk mortality was reduced by 42% because of the daily dosage of 20–40 mg of simvastatin over a 5-year long period and myocardial revascularization risk decreased by 37%. Moreover, cerebrovascular events and acute myocardial infarction risk were lowered to about a third.
The Heart Protection Study,Citation39 a larger trial, demonstrated the evident benefit of simvastatin 40 mg in high-risk population (previous CV events, DM1 and DM2, hypertension): as primary endpoint mortality was reduced by 13%. Secondary endpoints were nonfatal myocardial infarction and stroke: both resulted significantly improved (risk reduction was 35% and 28%, respectively). Another relevant study aimed at showing the reduction of coronary plaques through quantitative coronary angiography, the Multicenter Anti-Atheroma Study, reported a significant decrease in number of new lesions and an increase of mean lumen area compared to previous angiograms, and, in addition, a slowed progression of CHD in the group treated with simvastatin 20 mg/day compared to placebo recipients.Citation40
As described, simvastatin plays a chief role as lipid-lowering medication in terms of primary and secondary prevention of the main clinical outcomes using mean dosages of 20–40 mg. These dosages are the same in combination therapy with fibrates.
Even though high dosages of the most potent statins, including simvastatin, are related to an increased risk of new onset diabetes, a meta-analysis concluded that the potential risk is outright balanced from the real clinical benefit of statins.Citation41 Moreover, simvastatin, as typical of its class, is characterized by several pleiotropic effects on different organs and systems: according to some reports, simvastatin might exhibit a superior antidepressant effect in post-CABG-treated patients compared to atorvastatin and be a promising coadjuvant agent in oncology.Citation42,Citation43
Fenofibrate
Fenofibrate is a pro-drug transformed into its active form – fenofibric acid – in the liver. As agonists binding to PPAR-α, fibrates regulate genetic expression of numerous enzymes involved in lipids metabolism.Citation44 Fenofibrate pharmacokinetic profile is summarized in .
The increased synthesis of lipoprotein lipase (LPL) enhances free fatty acids (FFA) oxidation from TG in adipose tissue.Citation44 Liver production of ApoC-III, a component of VLDL and a LPL inhibitor, is reduced; therefore, first, less-circulating VLDLs are released from hepatocellular compartment and, second, peripheral oxidation is facilitated.Citation44–Citation46 Additionally, de novo FFA and VLDL production is reduced due to acetyl-CoA-carboxylase, fatty acids synthase, and ApoB under-expression. Furthermore, fibrates, particularly fenofibrate, reduce LDL and increase size and density of sd-LDL; also, Lp-PLA1 (lipoprotein – phospholipase A1) reduction diminishes LDL oxidation.Citation44,Citation45
On the other hand, ApoA-I and ApoA-II overtranscription increases HDL levels, and the same effect is achieved via a decrease of cholesteryl ester transfer protein (CETP) activity, reducing the transfer of cholesterol from HDL to VLDL.Citation44–Citation46 HDL, however, can even decrease for not completely clear reasons, if thiazolidinediones are co-administered.Citation47
Eventually the net effect of fibrate is the reduction of TG-rich lipoprotein and elevation of HDL; hence, its indication in nonalcoholic fatty liver disease treatment.Citation48 LDL trend can show a paradoxical pattern: in fact in case of severe hypertriglyceridemia, catabolism of TG induced by fibrate can convert VLDL to LDL rapidly, leading to initial LDL elevation and shift to less-buoyant LDL particles.Citation44
Weak results were obtained in glucose control: in some studies, fenofibrate improved insulin sensitivity and glucose level in metabolic syndrome, DM2 and CD patients.Citation49–Citation52 The underlying mechanism could be an increase of adiponectin (insulin sensitizer) in adipose tissue.Citation53
Also, other studies showed antithrombotic and fibrinolytic properties of fenofibrate (decrease in PAI and fibrinogen),Citation54 neo-angiogenesis reduction, and, on the other side, increase of flow-mediated dilation consistent with beneficial improvement of nitric oxide production, as proved in vitro.Citation44
Last, markers of inflammation as CRP, interleukins (mostly interleukin-6 [IL-6] and tumor necrosis factor-α [TNF-α]), adhesion molecules (VCAM and ICAM) and uric acid were reduced with the administration of fenofibrate in a high-risk group.Citation52–Citation54
On account of what stated, two main trials have been carried out with regard to real clinical efficacy of lipid-lowering effect of fenofibrate and both investigated the efficacy in DM2 population because of frequent incidence of CD with DM.
The FIELD (Fenofibrate Intervention and Event Lowering in Diabetes) study enrolled patients with well-controlled DM2, among which <40% had diagnosis of dyslipidemia and about a fifth had previous diagnosis of CHD.Citation55 The comparison with placebo did not result in superiority of fenofibrate 200 mg/day in terms of primary composite outcomes (CHD events); however, while failed to present minor rates of CHD mortality significantly, fenofibrate-treated group showed a reduction in nonfatal myocardial infarction (hazard ratio, HR: 0.76). Total mortality, total stroke, and total CVD mortality reduced nonsignificantly, whereas fenofibrate decreased the incidence of coronary revascularization and first minor amputation as well as delayed first treatment for any retinopathy or maculopathy (present only in 8% of baseline sample). Apparently, the lack of efficacy of fenofibrate compared to placebo should be related to higher number of randomized placebo patients who were already on treatment with statins. Considering this bias, a successive analysis revealed an improvement in the relative reduction of total CVD events to 15% and a post hoc analysis reported that subgroups affected by marked hypertriglyceridemia, CD, and metabolic syndrome experienced greater benefit of fenofibrate treatment.Citation56 Unexpectedly, fenofibrate slowered glomerular filtration rate (GFR) decline and reduced albuminuria rate.Citation44
The DAIS trial (Diabetes Atherosclerosis Intervention Study) was designed to demonstrate a slower CHD progression in subjects treated with fenofibrate compared to placebo group.Citation57 Although the ambitious endpoint was not satisfied, due to diffuse disease, minimum lumen diameter of focal atherosclerosis appeared higher in fenofibrate recipients, however, similarly to FIELD, fenofibrate decreased albuminuria rate.
Combination therapy
Efficacy
The ACCORD Lipid, a double-blind, randomized, open-label trial, aimed to verify the superiority of fenofibrate plus simvastatin versus placebo plus simvastatin in 5518 patients with DM2 at high risk of CVD.Citation58 The final results showed no significant variations between the two groups for primary and secondary endpoints (). Beneficial effect on minor outcomes as renal disease progression, measured as micro and macro-albuminuria, was instead confirmed.
Table 2 ACCORD LIPID and EYE TRIAL outcomesCitation58,Citation60
Lipid values were overall reduced; nevertheless, at subgroup analysis, the primary endpoint was reduced in the top tertile of TG and in the lowest tertile of HDL patients (17% of total cohort), thus showing the major benefit in the highest risk CD population (relative risk reduction =31%).Citation59,Citation60 Slight gender differences for primary endpoint were reported, as women were more protected than men (9.1% vs 11.2% in combination therapy groups of respective gender).Citation59 Part of the subjects enrolled in ACCORD Lipid was recruited for the ACCORD Eye trial, which assessed subjects with diabetic retinopathy.Citation60 As previously demonstrated in the FIELD,Citation55 fenofibrate in combination therapy showed its protective effect with regard to this common complication with a substantial relative risk reduction (40%). Furthermore, an ancillary study,Citation61 based on the observations that post-prandial TGs are predictors of CHD,Citation62,Citation63 investigated the supposed superiority of fenofibrate plus simvastatin in lowering non-fasting TG compared to placebo associated with simvastatin: the hypothesis was rejected, but, however, Apo-B48, marker of postprandial chylomicrons, was reduced in a greater extent in subject with high fasting TG at the baseline.
According to SAFARI trial (study of simvastatin plus fenofibrate for combined hyper-lipidemia), simvastatin 20 mg plus fenofibrate 160 mg improved the overall lipid profile:Citation64 in particular, while HDL almost doubled, TGs were reduced by 43% in the combination treatment group. Moreover, as previously reported, the addition of fenofibrate caused a shift to larger, buoyant, and less dangerous LDL particles.
In a post hoc analysis, the same investigators assessed a correlation between non-HDL and Apo-B in the co-treated group and suggested a possible role of non-HDL cholesterol as surrogate marker of Apo-B content, thus supporting its use as a secondary target of the lipid-lowering therapy.Citation65
In addition to SAFARI, smaller studies supported existing data with regard to lipid profile: Mohiuddin et alCitation66 used the lowest dose of fenofibrate than the other studies did (135 vs 160 mg in the SAFARI and 200 mg in the ACCORD) associated with simvastatin 20 and obtained favorable results in comparison with statin alone: HDL-C increased (+17.8% vs 7.2%) and TG decreased drastically (−37.4% vs −14.2%). Percentages approximately equivalent were found in fenofibrate 135 mg plus simvastatin 40 mg.
The DIACOR (Diabetes and Combined Lipid Therapy Regimen) study compared the combination therapy with both monotherapies: results showed that the supplemental advantage in HDL rise and TG decrease are derived merely from fenofibrate addition.Citation67 Furthermore, an analysis from DIACOR study confirmed positive modifications found during SAFARI at expense of pro-atherogenic sd-LDL.Citation68
Stefanutti et al reached consistent conclusions: all four groups treated with different double-drug combinations (from simvastatin 10 mg to simvastatin 30 mg plus fenofibrate 200–300 mg) showed improvement in lipid profile, albeit the more statistically significant overall benefit was obtained with simvastatin 20 mg/fenofibrate 200 mg, and no serious adverse reactions were noted in any group.Citation69 If slight differences among various dose combinations might exist, no remarkable disparity was assessed between daily co-administration and alternate day use.Citation70 Outstanding results can be obtained with a new fixed-dose combination with fenofibrate 145 mg in a new nanotechnology formulation compared to single medications.Citation71 As observable from all the studies referred, the higher the baseline dyslipidemia level, the better the effect of combined drugs is.
Mean relative total cholesterol level reduction values are given in ; meta-regression analysis of such studies is plotted in . Three months is generally required to achieve a substantial cholesterol reduction. A mild, direct, nonsignificant correlation between fenofibrate dosage and total cholesterol reduction is also evident (linear weighted regression analysis).
Figure 1 Mean relative reduction of total cholesterol levels by adding fibrates.
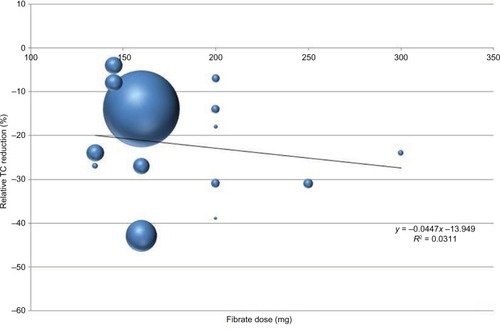
Table 3 Mean relative reduction of total cholesterol levels by adding fibrates.
Pleiotropic effects of both drugs act synergistically on novel different biomarkers and risk factors. Combination therapy reduces fibrinogen after 3 months of treatment for an acute coronary syndrome, and this is attributed mainly to fenofibrate addition.Citation72,Citation73 Nevertheless, clinical validations are still expected.
An analysis carried out on animals fed with high fat content diet and treated separately with simvastatin and fenofibrate compared to untreated controls provided preliminary results with regard to metabolomic effects: aside from cholesterol, levels of various small endogenous molecules (aminoacids, fatty acids, carbohydrate, and catabolites) significantly changed, among which important markers involved in CVD genesis (ie, a precursor of vaso-protective prostaglandins, linoleic acid, increased, while creatinine, renal damage marker, decreased).Citation74 However, dosages in animals were different than those generally used in humans, and these data require further confirmations.
Administered together, simvastatin and fenofibrate potentiate their own anti-inflammatory properties in DM2 patients, as proven by a decrease in a greater extent than single monotherapy of monocyte and lymphocyte released atherogenic cytokines (IL-1b, IL-6, IL-2, interferon [IFN]-γ, and TNF-α) and, hence hs-CRP, probably via the same cellular pathways.Citation52,Citation75 Moreover, the effect was exactly more prominent and statistically more significant in patients with overt CD.
Safety
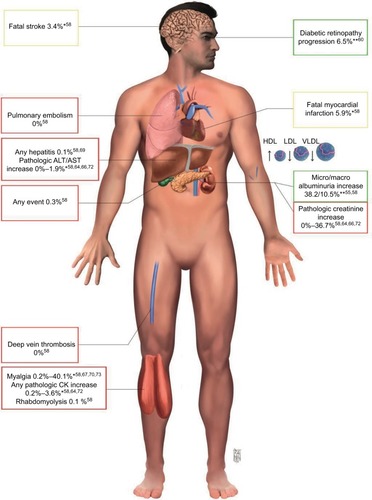
The most common adverse reactions characteristic of statins group are hepato- and myotoxicity, either clinically silent or evident (). The association with fibrate can increase the risk of serious adverse reaction for both pharmacodynamic and pharmacokinetic interaction.Citation76
Figure 2 Principal side effects and clinical benefit of combination therapy.
Abbreviations: ALT, alanine amino transferase; AST, aspartate amino transferase; HDL, high-density lipoprotein; LDL, low-density lipoprotein; VLDL, very-low-density lipoprotein.
Statins can affect muscles through different mechanisms (membrane integrity perturbation, apoptosis induction, mythocondrial dysfunction, impairment in calcium homeostasis, or rarely autoimmune reaction); however, the incidence according to a meta-analysis of 26 statins trials is 1: 10,000 compared to placebo.Citation77,Citation78
Liver injury is usually asymptomatic and apparently due to elevated membrane permeability, secondary to low cholesterol production, which permits leakage of hepatocellular content, while autoimmune mechanism is quite uncommon.Citation79
Fibrate-related skeletal muscle damage is probably ascribed to reactive oxygen species derived from β-oxidation and mitochondrial dysfunction induced by fibrate, as shown in animal models which were treated with both potent and weak (fenofibrate) compounds;Citation80,Citation81 however, experimental doses are extremely higher than those used in humans. Similar origin for hepatotoxicity has been speculated, even if recent evidences suggest that PPAR-α agonist can directly increase alanine amino transferase (ALT) and aspartate amino transferase (AST) gene expression and can also shift hepatic metabolism into a more ALT/AST-dependent one.Citation82 On the contrary, PPAR activators likely protect against acetaminophen oxidative stress.Citation83 As was observed in FIELD study, fibrates increase cholelithiasis risk, altering cholesterol biliary efflux, and accordingly pancreatitis is significantly more probable.Citation84 Indeed, gallbladder disease is a contraindication to the use of fibrates.
Pharmacokinetic interaction is univocal: fibrates can generally increase statin half-life therefore augmenting the risk of statin side effects. Gemfibrozil, but not fenofibrate, inhibits OATP1B1 (organic anion-transporting polypeptide), a cellular transporter from blood stream to hepatic cells, increasing simvastatin concentration and its adverse effects; thus this association should be avoided.Citation85
When combined, both in fixed dose and in staggered dose, fenofibrate decreases simvastatin AUC (area under the plasma concentration curve) by ~30%, as reported in two isolated studies, while simvastatin acid was not affected.Citation86 Many pharmacological mechanisms have been postulated; however, since the intentional reduction of cholesterol is unaltered with both dosing schedules and no life-threatening reactions occurred, the authors concluded that this unaccountable drug–drug interaction is clinically irrelevant, and risk of myopathy can be considered theoretic. Clinicians and primary care physicians should also mind about other drugs administration (ie, cyclosporine, an OATP1B1 inhibitor) and choose case by case which drug discontinuation provides the best benefit/risk ratio.
Also, in all the aforementioned trials, serious adverse reactions were isolated cases: for instance in the SAFARI trial (618 patients over 12 weeks), there was no significant difference of frequency of muscle symptoms between combined therapy versus monotherapy (1.4% vs 1.5%) and no case of rhabdomyolysis was recorded.Citation64 In the ACCORD Lipid study (with the longest follow-up and the highest number of patients enrolled), the incidence of myotoxicity (myopathy, myositis, and rhabdomyolysis) in the treatment group was equally balanced to placebo plus simvastatin recipients (0.1% for both).Citation58 Although nephroprotective effect resulted in long term, fibrate co-administration caused transient creatinine elevation (>1.3 mg/dL for women; >1.5 mg/dL for men), but no cases of acute renal failure were reported. Despite collateral homocysteine increase, any deep venous thrombosis or pulmonary embolism occurred, in contrast to data recorded in the FIELD study. Additionally, absolute number of deaths was definitely comparable between the two groups (203 in the fenofibrate plus simvastatin group vs 221 in placebo). Overall risk of myotoxicity was very low in combination therapy, including asymptomatic and occasional creatinine phosphokinase (CPK) increment >5 or >10 times the upper limit of normal (ULN, usually between 0.3% and 2.2%).Citation58
Alanine amino transferase (ALT) is more sensitive in case of liver injury compared to AST (present also in muscle tissues), and an increase of its value per three times the ULN should induce to analyze fractionated bilirubin level before drug discontinuations, because bilirubin is a more reliable indicator of damage, as National Lipid Association’s (NLA) Liver Expert Panel recommends.Citation87 In the ACCORD study, ALT elevation occurred because of drug discontinuation in only four patients in combination therapy group and no difference in gallbladder-related events occurred between the two groups.Citation58 However, gallbladder ultrasound should be performed before initiating the therapy.
Minor drug adverse reactions (DAEs), such as allergy, cataract, and interstitial lung disease, have been described in sporadic cases. Obviously, new onset diabetes related to simvastatin could not be evaluated in these statistics because diabetes was a chief inclusion criterion.
Finally, despite overall rarity of DAEs (mostly the serious ones) and the net beneficial effect of lipid-lowering medications in terms of primary and secondary CVD prevention as confirmed by a recent meta-analysis, physicians should be aware of safety aspects and frequently monitor patients on high dosage of statins and other toxic drugs whose interferences may be harmful (almost exclusively for simvastatin) or with preexisting risk factors (chronic kidney disease, hepatic insufficiency, muscular disease, age, and hypothyroidism).Citation88 It is generally recommended to measure ALT and CPK at the baseline and after some weeks of treatment or at the first suspected symptoms in healthy subjects. Food and Drug Administration suggests to test renal function periodically in elderly patients or those with renal insufficiency.Citation89 Transaminases and CPK should be monitored periodically in any case.
Comparison of simvastatin with other fibrates
Simvastatin plus gemfibrozil have an evidently high risk/benefit ratio because of clear pharmacological interactions, while, generally, the combination with gemfibrozil is associated with higher rates of DAEs compared to fenofibrate (ie, 15 vs 20.7/100,000 for rhabdomyolysis) as evaluated in a retrospective analysis.Citation90 Safety and efficacy about combination of bezafibrate with simvastatin, even if positive, are based only on two single experiences with poor sample sizes and brief follow-up.Citation91,Citation92
Comparison of fenofibrate with other statins
The addition of fenofibrate has been tested with other statins (fluvastatin, atorvastatin, pravastatin, and rosuvastatin) in comparison with monotherapy, with overall favorable results and comparable safety profile among different associations in regard of lipid levels.Citation93–Citation96 Rosuvastatin has alone been demonstrated to be noninferior to combination.Citation96 However, no double-blind, randomized, placebo-controlled, and multicentre clinical trial, as large as ACCORD and SAFARI studies, with hundreds of patients enrolled, has been done, and, thus, any head-to-head comparison is presently unreliable.
Special populations and conditions
DM and metabolic syndrome
DM patients represent the target population of the ACCORD Lipid trial; therefore, such results are the basis for treatment indications. Although not superior to placebo in reducing major CV events, the addition of fenofibrate to lipid-lowering therapy in DM2 patients has a series of healthy effects on endothelial function, inflammation, hemostasis, and glycemic control,Citation50,Citation52,Citation97 which could be the reason of the improvement of microangiopathy and diabetic nephropathy. In a small study, carried out by Vega et al, no impairment of glucose levels occurred, and the low and theoretic risk to develop DM2, mainly related to other preexisting conditions, should not refrain for initiating this vascular protective lipid-lowering therapy.Citation98 Nevertheless, combination therapy should neither reciprocally interfere with antidiabetic medications nor increase the risk of adverse effect (as myopathy risk in case of thiazolidinediones and fibrates).Citation99
Chronic kidney disease
Serum creatinine level ULN (>1.5 mg/dL) was an exclusion criteria in all great trials.Citation58,Citation64 However, mild-to-moderate renal insufficiency is more frequent in real practice; thus, precautionary laboratory and clinical monitoring should be performed in such patients. Fenofibrate alone is contraindicated in IV-V KDOQI stage and dose should be the lowest possible in case of creatinine clearance <50 mg/dL, according to the manufacturer.
Hypothyroidism
Hypothyroidism is associated with mixed dyslipidemia and abnormal CPK is correlated in >90% of cases; furthermore, low thyroid function decreases GFR and renal clearance.Citation100,Citation101 The primary treatment of secondary dyslipidemia is restoring hormones level, although, in case of preexisting or refractory dyslipidemia, the addition of lipid-lowering medications should be considered. Association therapy is not reported; nevertheless, simvastatin and fenofibrate alone have shown to be useful.Citation102,Citation103 Since the risk of muscular toxicity is increased and numerous isolated cases of rhabdomyolysis requiring hemodialysis have been reported,Citation104 great caution should be paid not only in case of known hypothyroidism but also in case of occult hypothyroidism.Citation102,Citation103 Therefore, a screening of thyroid function before initiating double therapy is recommended.
HIV
HIV infection is associated with atherogenic dyslipidemia:Citation105 endogenous IFN-α inhibits hepatic and endothelial lipase, thus increasing TG concentrations.Citation106 Moreover, CETP activity and HDL level are decreased.Citation107 HAART therapy also causes dyslipidemia stimulating lipogenesis.Citation108,Citation109 Double therapy is a reliable option for dyslipidemia: indeed, fenofibrate is very effective also in HIV patients;Citation110 however, simvastatin is contraindicated in case of protease inhibitors treatment, which could elevate simvastatin concentration by 10 times and increase the risk of overexposure via CYP3A4 inhibition.Citation111,Citation112 Therefore, other combinations should be preferred.
Childhood with CD
Acquired CD is a more prevalent form of dyslipidemia in childhood.Citation113 Diagnosis of familial combined hyperlipidemia (FH) requires the presence of increased Apo-B and sd-LDL particles in the patient and in at least two family members and one first-degree relative with the history of CHD. The family history is usually unknown and CHD could be silent, thus few cases of CD can be classified as purely genetic and familial.Citation113 Approximately 40% of obese adolescents have an atherogenic pattern typical of individuals with DM and metabolic syndrome. Intervention of lifestyle change is primary; however, if after 6 months lipid profile has not improved or baseline LDL and TG are severely high, medication should be considered, preferentially in children aged >10 years.Citation113 Low dose of simvastatin alone has demonstrated to improve vascular reactivity in children with FH and to be effective and safe in primary and secondary dyslipidemia.Citation114 Fenofibrate alone was shown to be effective and generally safe in a small randomized trial, but clinical efficacy on prevention of CVD is still unknown.Citation115 Similarly, no data about the use of drugs in combination are currently available.
Conclusion
Beside LDL reduction as a primary goal of lipid-lowering therapy, reduction of non-HDL cholesterol, decreasing TG and small dense LDL may be considered in primary and secondary prevention of CVD and may be pursued, if required, by implementing pharmacological therapy. In case of refractory CD, doubling statin dosage would not be convenient in terms of safety and efficacy; therefore, dual lipid-lowering therapy constitutes a viable solution. Combination therapy with simvastatin and fenofibrate, in various dosages, is an efficient and reliable mean of pharmacological prevention as large, multicenter, randomized trials reported. Moderate but significant clinical benefits are achievable in selected populations and, in absence of predisposing factors, toxicity is a marginal issue. However, cautions should be paid and patients should be clearly informed about risk–benefit ratio and possible adverse events. Moreover, fixed dose is equivalent to staggered dose and increases patient’s compliance.
Acknowledgments
We sincerely thank our trusted illustrator Raffaele Matteucci, professionally known as RaMat, for his precious graphic contribution in this and in other works (). The paper is not under consideration elsewhere. None of the paper’s contents have been previously published.
Disclosure
The authors report no conflicts of interest in this work.
References
- Global Burden of Disease Study 2013 CollaboratorsGlobal, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013Lancet201538674380026063472
- EzzatiMLopezADRodgersAVander HoornSMurrayCJSelected major risk factors and global and regional burden of disease. Comparative Risk Assessment Collaborating GroupLancet20023601347136012423980
- SharmaMGangulyNKPremature coronary artery disease in Indians and its associated risk factorsVasc Health Risk Manag2005121722517319107
- YusufSHawkenSOunpuuSEffect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case-control studyLancet200436493795215364185
- NelsonRHHyperlipidemia as a risk factor for cardiovascular diseasePrim Care20134019521123402469
- LacosteLLamJYHungJLetchacovskiGSolymossCBWatersDHyperlipidemia and coronary disease. Correction of the increased thrombogenic potential with cholesterol reductionCirculation199592317231777586300
- HossainPKawarBElNMObesity and diabetes in the developing world—a growing challengeN Engl J Med200735621321517229948
- MemberSBrugerMExperimental atherosclerosis; the effect of feeding olive oil on the absorption and deposition of cholesterolArch Pathol194540373375
- QiQLiangLDoriaAHuFBQiLGenetic predisposition to dyslipidemia and type 2 diabetes risk in two prospective cohortsDiabetes20126174575222315312
- VodnalaDRubenfireMBrookRDSecondary causes of dyslipidemiaAm J Cardiol201211082382522658245
- ShepherdJCobbeSMFordIPrevention of coronary heart disease with pravastatin in men with hypercholesterolemia. West of Scotland Coronary Prevention Study GroupN Engl J Med1995333130113077566020
- PedersenTRKjekshusJBergKRandomised trial of cholesterol lowering in 4444 patients with coronary heart disease: the Scandinavian Simvastatin Survival Study (4S)Lancet1994344138313897968073
- CatapanoALReinerZDe BackerGESC/EAS Guidelines for the management of dyslipidaemias: The Task Force for the management of dyslipidaemias of the European Society of Cardiology (ESC) and the European Atherosclerosis Society (EAS)Atherosclerosis201121734621882396
- StoneNJRobinsonJGLichtensteinAH2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice GuidelinesCirculation201412925 Suppl 2S1S4524222016
- CannonCPCombination therapy in mixed dyslipidemiaJ Intern Med200826335365
- LamarcheBLemieuxIDesprésJPThe small, dense LDL phenotype and the risk of coronary heart disease: epidemiology, patho-physiology and therapeutic aspectsDiabetes Metab19992519921110499189
- HalcoxJMisraAType 2 diabetes mellitus, metabolic syndrome, and mixed dyslipidemia: how similar, how different, and how to treat?Metab Syndr Relat Disord20151312125402738
- BrunzellJDIncreased ApoB in Small Dense LDL Particles Predicts Premature Coronary Artery DiseaseArterioscler Thromb Vasc Biol20052547447515731485
- ShimabukuroMHigaNMasuzakiHSataMUedaSImpact of individual metabolic risk components or its clustering on endothelial and smooth muscle cell function in menCardiovasc Diabetol2016157727188597
- KraussRMBurkeDJIdentification of multiple subclasses of plasma low density lipoproteins in normal humansJ Lipid Res198223971047057116
- LamarcheBTchernofACantinBDagenaisGRLupienPJDesprésJPSmall, dense low-density lipoprotein particles as a predictor of the risk of ischemic heart disease in men. Prospective results from the Quebec Cardiovascular StudyCirculation19979569758994419
- JacobsMJKleisliTPioJRMalikSL’ItalienGJChenRSWongNDPrevalence and control of dyslipidemia among persons with diabetes in the United StatesDiabetes Res Clin Pract20057026326915890427
- YounisNNSoranHPembertonPCharlton-MenysVElseweidyMMDurringtonPNSmall dense LDL is more susceptible to glycation than more buoyant LDL in Type 2 diabetesClin Sci201312434334922985435
- AgouridisAPRizosCVElisafMSFilippatosTDDoes combination therapy with statins and fibrates prevent cardiovascular disease in diabetic patients with atherogenic mixed dyslipidemia?Rev Diabet Stud20131017119024380091
- GittAKJungerCSmolkaWBestehornKPrevalence and overlap of different lipid abnormalities in statin-treated patients at high cardiovascular risk in clinical practice in GermanyClin Res Cardiol20109972373320521058
- MauroVFClinical pharmacokinetics and practical applications of simvastatinClin Pharmacokinet1993241952028343198
- MyersonMNgaiCJonesJHolleranSRamakrishnanRBerglundLGinsbergHNTreatment with high-dose simvastatin reduces secretion of apolipoprotein B-lipoproteins in patients with diabetic dyslipidemiaJ Lipid Res2005462735274416162940
- NawrockiJWWeissSRDavidsonMHReduction of LDL cholesterol by 25% to 60% in patients with primary hypercholesterolemia by atorvastatin, a new HMG-CoA reductase inhibitorArterioscler Thromb Vasc Biol19951556786827749881
- FarnierMPortalJJMaigretPEfficacy of atorvastatin compared with simvastatin in patients with hypercholesterolemiaJ Cardiovasc Pharmacol Ther200051273210687671
- KapurNKMusunuruKClinical efficacy and safety of statins in managing cardiovascular riskVasc Health Risk Manag20084234135318561510
- OseLDavidsonMHSteinEALipid-altering efficacy and safety of simvastatin 80 mg/day: long-term experience in a large group of patients with hypercholesterolemia. World Wide Expanded Dose Simvastatin Study GroupClin Cardiol2000231394610680028
- HunninghakeDBBallantyneCMMaccubbinDLShahAKGumbinerBMitchelYBComparative effect of simvastatin and atorvastatin on high-density lipoprotein cholesterol and apolipoprotein A1Clin Ther2003251670168612860491
- SerraNRosalesRMasanaLVallvéJCSimvastatin increases fibulin-2 expression in human coronary artery smooth muscle cells via rhoA/rho-kinase signaling pathway inhibitionPLoS One201510e013387526207907
- BellostaSViaDCanavesiMPfisterPFumagalliRPaolettiRBerniniFHMG-CoA reductase inhibitors reduce MMP-9 secretion by macrophagesArterioscler Thromb Vasc Biol199818167116789812903
- MeredithKGHorneBDPearsonRRMaycockCALappeDLAndersonJLMuhlesteinJBComparison of effects of high (80 mg) versus low (20 mg) dose of simvastatin on C-reactive protein and lipoproteins in patients with angiographic evidence of coronary arterial narrowingAm J Cardiol20079914915317223409
- ZouCQiHLiuZHHanLZhaoCYangXSimvastatin activates the PPARγ-dependent pathway to prevent left ventricular hypertrophy associated with inhibition of RhoA signalingTex Heart Inst J20134014014723678211
- AlmansobMAXuBZhouLSimvastatin reduces myocardial injury undergoing noncoronary artery cardiac surgery: a randomized controlled trialArterioscler Thromb Vasc Biol2012322304231322796581
- PedersenTRKjekshusJBergKRandomised trial of cholesterol lowering in 4444 patients with coronary heart disease: the Scandinavian Simvastatin Survival Study (4S)Lancet1994344138313897968073
- Heart Protection Study Collaborative GroupMRC/BHF Heart Protection Study of cholesterol lowering with simvastatin in 20,536 high-risk individuals: a randomised placebo-controlled trialLancet200236072212114036
- MAAS investigatorsEffect of simvastatin on coronary atheroma: the multicentre anti-atheroma study (MAAS)Lancet19943446336387864934
- SattarNPreissDMurrayHStatins and risk of incident diabetes: a collaborative meta-analysis of randomised statin trialsLancet201037573574220167359
- AbbasiSHMohammadinejadPShahmansouriNSimvastatin versus atorvastatin for improving mild to moderate depression in post-coronary artery bypass graft patients: a double-blind, placebo-controlled, randomized trialJ Affect Disord201518314915526005776
- KretzerIFMariaDAGuidoMCContenteTCMaranhãoRCSimvastatin increases the antineoplastic actions of paclitaxel carried in lipid nanoemulsions in melanoma-bearing miceInt J Nanomedicine20161188590427022257
- McKeageKKeatingGMFenofibrate: a review of its use in dyslipidaemiaDrugs2011711917194621942979
- SchoonjansKPeinado-OnsurbeJLefebvreAMPPAR alpha and PPAR gamma activators direct a distinct tissue-specific transcriptional response via PPRE in the lipoprotein lipase geneEMBO J199615533653488895578
- FarnierMUpdate on the clinical utility of fenofibrate in mixed dyslipidemias: mechanisms of action and rational prescribingVasc Health Risk Manag20084991100019183747
- LinzPELovatoLCByingtonRPParadoxical reduction in HDL-C with fenofibrate and thiazolidinedione therapy in type 2 diabetes: the ACCORD Lipid TrialDiabetes Care20143768669324296848
- MussoGCassaderMGambinoRCholesterol-lowering therapy for the treatment of nonalcoholic fatty liver disease: an updateCurr Opin Lipidol20112248949621986643
- KrysiakRStachura-KulachAOkopienBMetabolic and monocyte-suppressing actions of fenofibrate in patients with mixed dyslipidemia and early glucose metabolism disturbancesPharmacol Rep20106212013020360622
- PruskiMKrysiakROkopienBPleiotropic action of short-term metformin and fenofibrate treatment, combined with lifestyle intervention, in type 2 diabetic patients with mixed dyslipidemiaDiabetes Care2009321421142419435959
- Idzior-WalusBSieradzkiJRostworowskiWEffects of comicronised fenofibrate on lipid and insulin sensitivity in patients with polymetabolic syndrome XEur J Clin Invest20003087187811029601
- KrysiakRGdula-DymekAOkopienBThe effect of fenofibrate on lymphocyte release of proinflammatory cytokines and systemic inflammation in simvastatin-treated patients with atherosclerosis and early glucose metabolism disturbancesBasic Clin Pharmacol Toxicol201311219820222935083
- FilippatosTDElisafMSSafety considerations with fenofibrate/simvastatin combinationExpert Opin Drug Saf2015141481149326134595
- YeJKiageJNArnettDKBartolucciAAKabagambeEKShort-term effect of fenofibrate on C-reactive protein: a meta-analysis of randomized controlled trialsDiabetol Metab Syndr201132421939559
- KeechASimesRJBarterPEffects of long-term fenofibrate therapy on cardiovascular events in 9795 people with type 2 diabetes mellitus (the FIELD study): randomised controlled trialLancet20053661849186116310551
- ScottRO’BrienRFulcherGEffects of fenofibrate treatment on cardiovascular disease risk in 9,795 individuals with type 2 diabetes and various components of the metabolic syndrome: the Fenofibrate Intervention and Event Lowering in Diabetes (FIELD) studyDiabetes Care20093249349818984774
- SteinerGThe Diabetes Atherosclerosis Intervention Study (DAIS): a study conducted in cooperation with the World Health Organization. The DAIS Project GroupDiabetologia199639165516619081851
- GinsbergHNElamMBLovatoLCThe ACCORD Study GroupEffects of combination lipid therapy in type 2 diabetes mellitusN Engl J Med20103621563157420228404
- ElamMLovatoLCGinsbergHRole of fibrates in cardiovascular disease prevention, the ACCORD-Lipid perspectiveCurr Opin Lipidol201122556121102326
- The ACCORD Study Group and ACCORD Eye Study GroupEffects of medical therapies on retinopathy progression in type 2 diabetesN Engl J Med201036323324420587587
- Reyes-SofferGNgaiCILovatoLKarmallyWRamakrishnanRHolleranSGinsbergHNEffect of combination therapy with fenofibrate and simvastatin on postprandial lipemia in the ACCORD lipid trialDiabetes Care20133642242823033246
- BansalSBuringJERifaiNMoraSSacksFMRidkerPMFasting compared with nonfasting triglycerides and risk of cardiovascular events in womenJAMA200729830931617635891
- NordestgaardBGBennMSchnohrPTybjærg-HansenANonfasting triglycerides and risk of myocardial infarction, ischemic heart disease, and death in men and womenJAMA200729829930817635890
- GrundySMVegaGLYuanZBattistiWPBradyWEPalmisanoJEffectiveness and tolerability of simvastatin plus fenofibrate for combined hyperlipidemia (the SAFARI trial)Am J Cardiol20059546246815695129
- GrundySMVegaGLTomassiniJETershakovecAMCorrelation of non-high-density lipoprotein cholesterol and low-density lipoprotein cholesterol with apolipoprotein B during simvastatin + fenofibrate therapy in patients with combined hyperlipidemia (a subanalysis of SAFARI trial)Am J Cardiol200910454855319660610
- MohiuddinSMPepineCJKellyMTButtlerSMSetzeCMSleepDJStolzenbachJCEfficacy and safety of ABT-335 (fenofibric acid) in combination with simvastatin in patients with mixed dyslipidemia: a phase 3, randomized, controlled studyAm Heart J200915719520319081418
- MuhlesteinJBMayHTJensenJRThe reduction of inflammatory biomarkers by statin, fibrate, and combination therapy among diabetic patients with mixed dyslipidemia: the DIACOR (Diabetes and Combined Lipid Therapy Regimen) studyJ Am Coll Cardiol20064839640116843192
- MayHTAndersonJLPearsonRRComparison of effects of simvastatin alone versus fenofibrate alone versus simvastatin plus fenofibrate on lipoprotein subparticle profiles in diabetic patients with mixed dyslipidemia (from the Diabetes and Combined Lipid Therapy Regimen study)Am J Cardiol200810148648918312763
- StefanuttiCBucciADi GiacomoSEfficacy, safety and tolerability of combined low-dose simvastatin-fenofibrate treatment in primary mixed hyperlipidaemiaClin Drug Investig200424465477
- KayikçioğluMOzerkanFSoydanIEffectiveness and safety of alternate-day simvastatin and fenofibrate on mixed hyperlipidemiaAm J Cardiol19998311351137A910190536
- FoucherCAubonnetPReichertPNew fixed-dose combinations of fenofibrate/simvastatin therapy significantly improve the lipid profile of high-risk patients with mixed dyslipidemia versus monotherapiesCardiovasc Ther20153332933726227087
- ShahHDParikhKHChagMCBeneficial effects of the addition of fenofibrate to statin therapy in patients with acute coronary syndrome after percutaneous coronary interventionsExp Clin Cardiol200712919618650989
- SahebkarASerbanMCMikhailidisDPHead-to-head comparison of statins versus fibrates in reducing plasma fibrinogen concentrations: a systematic review and meta-analysisPharmacol Res201610323625226657419
- XuQYLiuYHZhangQMetabolomic analysis of simvastatin and fenofibrate intervention in high-lipid diet-induced hyperlipidemia ratsActa Pharmacol Sin2014351265127325220639
- KrysiakRGdula-DymekAOkopienBEffect of simvastatin and fenofibrate on cytokine release and systemic inflammation in type 2 diabetes mellitus with mixed dyslipidemiaAm J Cardiol20111071010101821276586
- BannwarthBDrug-induced myopathiesExpert Opin Drug Saf20021657012904161
- TomaszewskiMStępieńKMTomaszewskaJCzuczwarSJStatin-induced myopathiesPharmacol Rep20116385986622001973
- MammenALStatin-associated autoimmune myopathyN Engl J Med201637466466926886523
- CalderonRMCubedduLXGoldbergRBSchiffERStatins in the treatment of dyslipidemia in the presence of elevated liver aminotransferase levels: a therapeutic dilemmaMayo Clin Proc20108534935620360293
- PettersenJCPruimboom-BreesIFranconeOLAmacherDEBoldtSEKerlinRLBallingerWEThe PPARα agonists fenofibrate and CP-778875 cause increased β-oxidation, leading to oxidative injury in skeletal and cardiac muscle in the ratToxicol Pathol20124043544722301950
- BalfourJAMcTavishDHeelRCFenofibrate. A review of its pharmacodynamic and pharmacokinetic properties and therapeutic use in dyslipidaemiaDrugs1990402602902226216
- KobayashiASuzukiYKunoHSugaiSSakakibaraHShimoiKEffects of fenofibrate on plasma and hepatic transaminase activities and hepatic transaminase gene expression in ratsJ Toxicol Sci20093437738719652460
- PattersonADShahYMMatsubaraTKrauszKWGonzalezFJPeroxisome proliferator-activated receptor alpha induction of uncoupling protein 2 protects against acetaminophen-induced liver toxicityHepatology20125628129022318764
- ScottRO’BrienRFulcherGEffects of fenofibrate treatment on cardiovascular disease risk in 9,795 individuals with type 2 diabetes and various components of the metabolic syndrome: the Fenofibrate Intervention and Event Lowering in Diabetes (FIELD) studyDiabetes Care20093249349818984774
- NoéJPortmannRBrunMEFunkCSubstrate-dependent drug-drug interactions between gemfibrozil, fluvastatin and other organic anion-transporting peptide (OATP) substrates on OATP1B1, OATP2B1, and OATP1B3Drug Metab Dispos2007351308131417470528
- WinsemiusAAnsquerJCOlbrichMPharmacokinetic interaction between simvastatin and fenofibrate with staggered and simultaneous dosing: does it matter?J Clin Pharmacol2014541038104724691799
- CohenDEAnaniaFAChalasaniNAn assessment of statin safety by hepatologistsAm J Cardiol20069777C81C16377288
- GuoJMengFMaNMeta-analysis of safety of the coadministration of statin with fenofibrate in patients with combined hyper-lipidemiaAm J Cardiol20121101296130122840347
- Food and Drug AdministrationFDA drug safety communication: review update of Trilipix (fenofibric acid) and the ACCORD Lipid trial1192011 Available from: http://www.fda.gov/Drugs/DrugSafety/ucm278837.htmlAccessed June 22, 2016
- CurtinPOJonesWNTherapeutic rationale of combining therapy with gemfibrozil and simvastatinJ Am Pharm Assoc200747140146
- HorsmansYDesagerJPHarvengtCEffects of combined bezafibrate-simvastatin appraised in healthy subjectsJ Clin Pharmacol1992324224261587959
- KehelyAMacMahonMBarbirMWrayRHuntBJPrescottRJThompsonGRCombined bezafibrate and simvastatin treatment for mixed hyperlipidaemiaQJM199588749
- FarnierMDejagerSEffect of combined fluvastatin-fenofibrate therapy compared with fenofibrate monotherapy in severe primary hypercholesterolemia. French Fluvastatin Study GroupAm J Cardiol200085535711078237
- FarnierMSteinmetzARetterstølKCsászárAFixed-dose combination fenofibrate/pravastatin 160/40 mg versus simvastatin 20 mg monotherapy in adults with type 2 diabetes and mixed hyperlipidemia uncontrolled with simvastatin 20 mg: a double-blind, randomized comparative studyClin Ther20113311221397769
- AthyrosVGPapageorgiouAAAthyrouVVDemitriadisDSKontopoulosAGAtorvastatin and micronized fenofibrate alone and in combination in type 2 diabetes with combined hyperlipidemiaDiabetes Care200225119820212087019
- ChenYPChangKCTsengWKYinWHChenJWLeeYTWuCCIncreased rosuvastatin dose versus concomitant fenofibrate and rosuvastatin therapy to achieve lipid goal in patients with diabetes or atherosclerosis with metabolic syndromeZhonghua Minguo Xin Zang Xue Hui Za Zhi201329421428
- KeiALiberopoulosEElisafMEffect of hypolipidemic treatment on glycemic profile in patients with mixed dyslipidemiaWorld J Diabetes2013436537124379928
- VegaGLMaPTCaterNBFilipchukNMeguroSGarcia-GarciaABGrundySMEffects of adding fenofibrate (200 mg/day) to simvastatin (10 mg/day) in patients with combined hyperlipidemia and metabolic syndromeAm J Cardiol20039195696012686335
- LedlMHoheneckerJFrancesconiCRootsIBauerMFRodenMAcute myopathy in a type 2 diabetic patient on combination therapy with metformin, fenofibrate and rosiglitazoneDiabetologia2005481996199816132947
- ChertowBSMottoGSShahJHA biochemical profile of abnormalities in hypothyroidismAm J Clin Pathol1974617857884832117
- SindoniARodolicoCPappalardoMAPortaroSBenvengaSHypothyroid myopathy: a peculiar clinical presentation of thyroid failure. Review of the literatureRev Endocr Metab Disord Epub201657
- KiernanTJRochfordMMcDermottJHSimvastatin induced rhab-domyolysis and an important clinical link with hypothyroidismInt J Cardiol200711937437617098308
- QariFASevere rhabdomyolysis and acute renal failure secondary to the use of simvastatin in undiagnosed hypothyroidismIndian J Nephrol200818282920368919
- ClouâtreYLeblancMOuimetDPichetteVFenofibrate-induced rhabdomyolysis in two dialysis patients with hypothyroidismNephrol Dial Transplant1999141047104810328516
- FeeneyERMallonPWGHIV and HAART-associated dyslipidemiaOpen Cardiovasc Med J20115496321643501
- EhnholmCAhoKHuttunenJKKostiainenEMattilaKPakkarainenJCantellKEffect of interferon on plasma lipoproteins and on the activity of post heparin plasma lipasesArteriosclerosis1982268736174110
- VuCNRuiz-EspondaRYangEAltered relationship of plasma triglycerides to HDL cholesterol in patients with HIV/HAART-associated dyslipidemia: further evidence for a unique form of metabolic syndrome in HIV patientsMetabolism2013621014102023522788
- LumYDHeJGSlatterJGGene expression profiling of rat liver reveals a mechanistic basis for ritonavir-induced hyperlipidemiaGenomics20079046447317719200
- PenzakSRChuckSKManagement of protease inhibitor-associated hyperlipidemiaAm J Cardiovasc Drugs200229110614727985
- VisnegarwalaFMaldonadoMSajjaPLipid lowering effects of statins and fibrates in the management of HIV dyslipidemias associated with antiretroviral therapy in HIV clinical practiceJ Infect20044928329015474625
- HusainNEAhmedMHManaging dyslipidemia in HIV/AIDS patients: challenges and solutionsHIV AIDS20147110
- FeinsteinMJAchenbachCJStoneNJLloyd-JonesDMA systematic review of the usefulness of statin therapy in HIV-infected patientsAm J Cardiol20151151760176625907504
- KaveyRECombined dyslipidemia in childhoodJ Clin Lipidol201595 SupplS41S5626343211
- StefanuttiCLucaniGVivenzioADi GiacomoSDiet only and diet plus simvastatin in the treatment of heterozygous familial hypercholesterolemia in childhoodDrugs Exp Clin Res199925232810337501
- SteinmetzJMorinCPanekESiestGDrouinPBiological variations in hyperlipidemic children and adolescents treated with fenofibrateClin Chim Acta198111243536113065