Abstract
Rosacea is a common, chronic, skin condition characterized by recurrent episodes of facial flushing, transient or persistent erythema, papules, pustules, and telangiectasias, in a symmetrical facial distribution. The etiology of rosacea remains unknown and this condition represents a therapeutic challenge because of its chronic nature, progression, potential for disfigurement and psychological impact. Although there is no curative therapy for rosacea, the most widely used systemic agents are oral tetracycline derivatives, including tetracycline, doxycycline, and minocycline. This article reviews the available evidence for the use of doxycycline, a second-generation tetracycline, in the treatment or rosacea.
Keywords:
Rosacea is a common, chronic dermatologic condition, whose cause remains unknown. It has a higher prevalence in fair-skinned individuals and most commonly affects individuals between the ages of 30 and 50, women being more affected than men.Citation1,Citation2 The diagnosis of rosacea requires the presence of one or more of the following primary features concentrated on the central area of the face: flushing (transient erythema), nontransient erythema, papules and pustules, and telangiectasia.Citation3 Rosacea represents a therapeutic challenge because of its chronic nature, progression, potential for disfigurement, and psychological impact.
Tetracycline compounds were the first systemic drugs used in the treatment of rosacea, and have been the mainstay therapeutics for more than 40 years, although it has just recently been approved by the FDA for the treatment of this condition.Citation4,Citation5 Doxycycline, a second-generation tetracycline, exhibits superior pharmacokinetic properties and lesser toxicity than first-generation tetracyclines.Citation6 They also posses antiangiogenic and anti-inflammatory properties that make it a promising therapeutic option in the treatment of rosacea.Citation7 This paper reviews the safety and efficacy of doxycycline in the treatment of rosacea with emphasis on those clinical studies that support its use.
Pharmacology of doxycycline
Chemistry
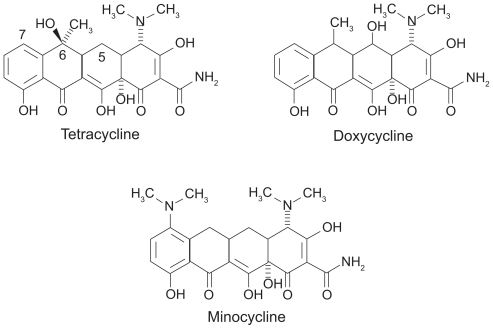
The basic chemical structure of tetracyclines consists of a tetracyclic naphtacene carboxamide ring system.Citation7 The structures of tetracycline, doxycycline, and minocycline are shown in . Doxycycline differs structurally from the tetracycline molecule in the modifications of substituent at positions 5 and 6 of the ring system, which make it more lipid soluble. Minocycline has a dimethylamino substituent at position 7.
Figure 1 Chemical structure of tetracyclines.
Absorption
Semi-synthetic second-generation tetracyclines, doxycycline and minocycline, are better absorbed after oral administration than first-generation counterparts due to their higher lipid solubility.Citation8–Citation11 Pooled data from studies show that mean absorption of oral doxycyline is close to 95%.Citation8,Citation9,Citation12,Citation13 After oral administration, the absorption of doxycycline is rapid, being detectable in blood in as little as 15 minutes.Citation12
Distribution, metabolism, and excretion
Doxycycline is widely distributed in tissues, including the skin, because of its high lipophilicity.Citation8–Citation12,Citation14,Citation15 No doxycycline metabolites have been found in blood, urine, or feces.Citation12 Doxycycline elimination occurs mainly through the gastrointestinal tract. Renal elimination accounts for 30% to 40% of the administered dose.Citation12 Doxycycline serum levels are minimally affected in patients with renal insufficiency and require no adjustments in dosage.Citation8–Citation9,Citation16
Mechanism of action
Bacteriostatic effects of tetracyclines are due to inhibition of protein synthesis, by binding to the 30S subunit on the bacterial ribosome, where they interfere with the binding of the aminoacyl tRNA to the acceptor site on the mRNA-ribosome complex.Citation14
Several studies have shown that tetracylines, including doxycycline, have immunomodulating properties.Citation7,Citation14,Citation17 These anti-inflammatory effects have been used to target several pathophysiological mechanisms in rosacea.
Tetracyclines have been shown to inhibit white cell movement during inflammation by interfering with calcium-dependent microtubular assembly and to inhibit lymphocytic proliferation by blockage of blast tranformation.Citation7,Citation17–Citation21 Tetracyclines have also been shown to inhibit arachidonic acid (AA) production from cell membrane components, in turn reducing the production of AA-derived proinflammatory mediators.Citation22
Tetracyclines can inhibit proteolysis mediated by matrix metalloproteinases (MMPs) which are secreted by activated neutrophils.Citation23,Citation24 Studies in vivo and in vitro have demonstrated inhibition of collagenase-3 (MMP-13), collagenase-2 (MMP-8), collagenase-1 (MMP-1), gelatinase A (MMP-2), gelatinase B (MMP-9), and macrophage metalloelastase (MMP-12).Citation25–Citation27 Inhibition of gelatinases A and B, which break down the basement membrane of the capillary vessels, promotes integrity of the capillary wall, reduces sensitivity to vasodilatory stimuli, prevents capillary leakage, improves the integrity of connective tissue, and downregulates cytokines (eg, TNF-α and IL-1β) that assist in erythema and inflammation associated with rosacea.Citation28,Citation29 Tetracyclines have also been shown to impair angiogenesis by the inhibition of MMPs, which may affect migration of endothelial cells during angiogenesis.Citation30
Tetracyclines may inhibit nitric oxide (NO) synthetase. This may prove beneficial in rosacea, as excess NO promotes vasodilation and inhibition of extracellular matrix synthesis.Citation31
Tetracyclines can affect molecular signaling pathways, such as the inhibition of calcium/calmodulin pathway and inhibition of protein kinase C activity. This results in decreased transcriptional activity for several MMPs, therefore reducing MMP-mediated extracellular matrix breakdown. Interference with this signaling also reduces vasodilation secondary to the decreased NO production.Citation32–Citation34
Several of these anti-inflammatory effects have been proven to occur with doxycycline ().
Table 1 Anti-inflammatory effects of doxycyclineCitation7
Doxycycline in rosacea
Subantimicrobial dose doxycycline
The use of doxycycline in rosacea has been proven in several clinical trials either alone or in combination with other therapies (). Before the introduction of 40 mg doxycycline monohydrate and its FDA approval in 2006 for the treatment of rosacea, there were several reports using subantimicrobial dose doxycycline hyclate 20 mg (SDD). Previous results of a study of doxycycline hyclate 20 mg twice daily for 6 months in the treatment of acne vulgaris had demonstrated a significant decrease in the clinical signs and symptoms without affecting the skin flora.Citation35
Table 2 Studies of doxycycline in rosacea
The first study that reported the efficacy of SDD in the treatment of rosacea was an open-label study that included 50 patients with all stages of rosacea.Citation24 Patients were treated with SDD 20 mg twice daily for 8 weeks. After an average of 4 weeks, patients experienced an 80% to 100% clearing in inflammatory lesions and a 50% reduction in erythema. At the end of treatment, there were no reports of gastrointestinal side effects, vaginitis, or photosensitivity.
A multicenter, randomized, double-blind, placebocontrolled, 16-week clinical trial evaluated the use of SDD twice daily versus placebo in 134 patients with moderate rosacea.Citation36 The assessment at week 16 relative to baseline showed a reduced lesion count (P = 0.009), decreased erythema score (P = 0.082), and global severity score (P = 0.034) in the study group compared with placebo. In the investigator’s global assessment scale (IGA), 13.1% of the study group patients achieved a score of 0 (clear) versus 1.5% of those with placebo (P = 0.014). Another single-center, randomized, double-blind, placebo-controlled trial evaluated the combined effect of SDD 20 mg and metronidazole 0.75% topical lotion in the treatment of moderate-to-severe rosacea.Citation37 Forty patients were randomized to receive SDD plus metronidaloze twice daily or placebo plus metronidazole twice daily for 12 weeks. SDD or placebo monotherapy continued for 4 weeks after metronidazole was discontinued. Results demonstrated a significant reduction from baseline in the total inflammatory lesion count at week 12 (P < 0.01) that was maintained at week 16, after 4 weeks of SDD as monotherapy (P < 0.01). Secondary endpoints of global severity and erythema were also reduced significantly by the combination treatment. There were no between-group differences observed in adverse events and there were no cases of photosensitivity or vaginitis reported.
Anti-inflammatory dose doxycycline
Anti-inflammatory dose doxycycline (Oracea®; Galderma) refers to a specific 40 mg capsule formulation of doxycycline monohydrate containing 30 mg immediate-release and 10 mg delayed-release beads administered once daily and that is devoid of antibiotic activity.Citation31 It was approved by the FDA in 2006 and is currently the only doxycyline formulation with FDA approval for the treatment of rosacea. Two phase 3, randomized, multicenter, double-blind, placebo-controlled, parallel-group monotherapy trials evaluated the use of once daily anti-inflammatory dose doxycycline (n = 269) or placebo (n = 268) for 16 weeks in the treatment of moderate to severe rosacea.Citation31 The mean changes from baseline in total inflammatory lesion count in the active treatment groups were −11.8 and −9.5 compared to −5.9 and −4.3 in the placebo arms (P < 0.001). This decrease in lesion count was seen as early as 3 weeks, and there was a progressive continued reduction throughout the entire study period. Also, a statistically significant greater reduction in mean total erythema from baseline was observed in the actively treated group compared with placebo-treated subjects in one pivotal study (P = 0.017). Anti-inflammatory dose doxycycline once daily was well tolerated. The percentage of patients discontinuing therapy because of adverse events was very low in both trials and was similar in both the active treatment and placebo group. Vaginal candidiasis and photosensitivity were not reported in the actively treated patients.
The efficacy of anti-inflammatory dose doxycycline in combination therapy for rosacea has also been reported. In a randomized, multicenter, double-blind, placebo-controlled, 16-week trial, the combined effect of anti-inflammatory dose doxycycline 40 mg and metronidazole gel 1% once daily (n = 36) was compared to placebo capsule and metronidazole gel 1% once daily (n = 36) in adults with mild to moderate rosacea.Citation38 After 12 weeks, metronidazole was discontinued allowing for comparison of anti-inflammatory dose doxycycline and placebo from week 12 to week 16. At both 4 weeks and 12 weeks assessments, the mean inflammatory lesion reduction from baseline was statistically significant in the anti-inflammatory dose doxycycline and metronidazole study arm (P = 0.008 week 4 and P = 0.002 week 12). From weeks 12 through 16, after discontinuation of metronidazole in both study arms, the improvement noted in the first 12 weeks receded in subjects who received only placebo compared with those subjects receiving only anti-inflammatory dose doxycycline. The results of this study indicate that concurrent use of anti-inflammatory dose doxycycline and metronidazole produces a greater magnitude of inflammatory lesion reduction than metronidazole alone.
Anti-inflammatory dose doxycycline compared with conventional dose doxycycline
When comparing anti-inflammatory dose doxycycline with anti-microbial dose doxycycline, a randomized, multi-center, double-blind, active-control, 16-week trial evaluated the efficacy of anti-inflammatory dose doxycycline (40 mg) and topical metronidazole gel 1% once daily (n = 44) versus conventional dose doxycycline (100 mg) and metronidazole gel 1% once daily (n = 47) in adults with moderate to severe rosacea.Citation39 The mean change from baseline to week 16 in inflammatory lesion count was similar in both study groups and at all study visits. The mean change in erythema score from baseline was slightly greater at all time points in the 40 mg group. This was statistically significant at week 12 (P < 0.04), but not at week 16. The most frequent adverse events included nausea, headache, influenza, nasopharyngitis, urticaria, diarrhea, esophageal pain, vomiting, abdominal pain, and upper abdominal pain in 32 patients. Of these, 26 subjects were in the 100 mg group and 6 subjects were in the 40 mg group. This study demonstrates that although both anti-inflammatory dose doxycycline (40 mg) and conventional dose doxycycline (100 mg) are effective once-daily treatments for moderate to severe rosacea, a higher incidence of adverse events is associated with the use of the 100 mg dose.
Doxycycline in ocular rosacea
Several nonplacebo-controlled studies have reported improvement in the signs and symptoms of ocular rosacea when treated with tetracycline or its derivatives. The largest restrospective study report described improvement in 98% of 113 patients given either tetracycline 250 mg 4 times daily or doxycycline 100 mg once daily.Citation40 Other prospective studies have demonstrated that between 87.5% and 100% of the patients have improvement of their symptoms of ocular rosacea after treatment with an initial dose of doxycycline 100 mg daily.Citation41–Citation43 Still, randomized, placebo-controlled studies evaluating the efficacy of doxycycline in ocular rosacea are lacking.
Doxycycline versus macrolides in the treatment of rosacea
The first randomized, open clinical trial evaluating the efficacy macrolides versus doxycycline in the treatment of rosacea was reported in 1997.Citation44 Patients were randomized to receive clarithromycin 250 mg twice daily for 4 weeks, then 250 mg once daily for four weeks (n = 23) or doxycycline 100 mg twice daily for 4 weeks, then 100 mg once daily for 4 weeks (n = 17). After 8 weeks of treatment, there were no significant differences observed in erythema, telangiectases, or in the number of lesions between the two groups. Still, a faster decrease in lesion count was observed in the clarithromycin group, showing a statistically significant (P <0.0005) difference in papules and pustules score between the two groups at weeks 4 and 6. The authors concluded that 6 weeks of clarithomycin treatment are as effective in the treatment of rosacea as 8 weeks of doxycycline treatment.
Another randomized, open clinical trial was performed to observe if azithromycin had an equivalent or superior effect to that produced by doxycycline in the treatment of adult patients with papulopustular rosacea.Citation45 Patients were randomized to receive azithromycin 500 mg 3 times weekly for 1 month, then 250 mg 3 times weekly for the second month, and 250 mg twice weekly for the third month in the first group (n = 37). The second group received doxycycline 100 mg once daily for 3 months (n = 30). In both treatment groups, the mean inflammatory lesion counts were significantly decreased at the third month (P < 0.001 in both groups), and at the second month post-treatment (P < 0.001 in both groups), when compared to baseline. When the efficacies of the two treatments were compared, there were no significant differences in the percentage of decrease in lesions (P = 0.771) or in the patients’ own assessment (P = 0.965). Adverse effects reported included diarrhea in four patients in the azithromycin group and epigastric burning in two patients in the doxycycline group. Only 2 patients discontinued the study because of adverse events, both of whom were in the azithromycin group. This study demonstrated that both treatments were equally effective in treating inflammatory rosacea and that intermittent azithromycin offers an alternative in the management of patients with rosacea.
Doxycycline versus minocycline
Minocycline is not approved by the FDA for the treatment of rosacea, but it is for the treatment of acne. There are currently no clinical trials that have evaluated the use of minocycline for the treatment of rosacea and due to the lack of clinical evidence comparisons of efficacy with doxycycline cannot be drawn. Minocycline has been used as a successful, long-term therapy for patients with acne vulgaris. Clinical trials of treatment of acne vulgaris with minocycline in doses of 100 mg daily have demonstrated a statistically significant decrease in lesion count when compared with placebo.Citation46 Still, no statistically significant differences have been demonstrated in clinical trials when comparing minocycline with doxycycline, and investigators have concluded that both are equally effective in the treatment of moderate to moderately severe acne vulgaris.Citation47–Citation49
An extended-release (ER) version of minocycline tablets at a dosage of 1 mg/kg/day (Solodyn®; Medicis Pharmaceutical Corporation) was approved in 2006 for the treatment of moderate-to-severe acne in patients older than 12.Citation50 Unlike the anti-inflammatory dose of doxycycline 40 mg for rosacea, the ER version of minocycline posses antibiotic activity.
Concerns about resistance
Conventional use of tetracycline agents in the treatment of rosacea includes doxycycline hyclate or monohydrate (100 to 200 mg daily), minocycline hydrochloride (100 to 200 mg daily), or tetracycline hydrochloride (500 to 1000 mg daily). These dosing regimens have proven both anti-inflammatory and antibiotic activity.Citation4 Still, concerns related to increased bacterial resistance have been raised in the last few years and several common pathogens encountered in dermatology have demonstrated bacterial resistance, including resistance to tetracyclines.Citation51
SDD 20 mg (Periostat®; CollaGenex Pharmaceuticals) is indicated for the treatment of adult periodontal disease, its mechanism having been attributed to its anticollagenase and antimatrix metalloproteinase properties.Citation52,Citation53 Studies have demonstrated that SDD administered twice daily for up to 18 months does not alter or promote antibiotic susceptibility patterns of normal flora or opportunistic periodontal pathogens.Citation53 Similarly, in acne patients treated over a 6-month period with SDD 20 mg twice daily there was no effect on Propionibacterium acnes or other cutaneous commensal bacteria.Citation35 Also, SDD did not alter microflora composition, and did not induce the emergence of organisms resistant to doxycycline, minocycline, tetracycline, erythromycin, clindamycin, or vancomycin.Citation35,Citation54 Analysis of the plasma concentrations of doxycycline demonstrated that administration of 20 mg twice daily produced maximal levels significantly lower than the minimum inhibitory concentration (MIC) required to produce an antimicrobial effect, while administration of doxycycline 50 mg once daily has been proven to produce plasma concentrations that exceed the MIC for 2 to 3 hours.Citation54
The lack of antibiotic resistance after treatment with anti-inflammatory dose doxycyline has also been previously demonstrated in the treatment of periodontitis.Citation55 In a subset of subjects (n = 34) treated for 9 months with anti-inflammatory dose doxycycline 40 mg once daily, microbiologic testing obtained from multiple subgingival sites demonstrated no evidence of antimicrobial selection pressure. Also, it did not alter the antibiotic susceptibility of subgingival flora and cross-resistance was not observed.
Adverse effects
The tetracycline antibiotic class has been used safely for long-term therapy in patients with rosacea and acne vulgaris. Within this antibiotic class, doxycycline is generally well tolerated. Minor side effects of tetracyclines are varied; serious side effects are rare.Citation56 ()
Table 3 Adverse events with doxycycline (100 to 200 mg daily)Table Footnotea
Serious drug reaction patterns to tetracycline antibiotics can be categorized as early or late. Early reactions include hypersensitivity syndrome reactions, serum-sickness-like reactions, and isolated single-organ dysfunction (involvement of one major organ: pancreatitis, hepatitis, cutaneous eruptions) which occur on average within 2 months of treatment.Citation57,Citation58 Late reactions include drug-induced lupus, which usually occurs an average of 2 years after initiation of treatment.Citation58 Drug-induced lupus has been reported in association with minocycline and not doxycycline use.
Second-generation tetracyclines (doxycycline hyclate, doxycycline monohydrate, minocycline) offer the patient the advantage of less frequent dosing and potentially fewer side effects.Citation8,Citation56 Based on the number of prescriptions dispensed from January 1, 1998 to August 31, 2003, Smith et alCitation59 estimated the overall incidence of adverse effects for doxycycline to be 13 per million in the United States (2.3 per million per year). A review of the literature (case reports and clinical trials) revealed that esophageal erosions and photosensitivity are the most commonly reported adverse effects of doxycycline.Citation59
Gastrointestinal adverse effects
The modifications in structure of the second-generation tetracyclines in comparison with the first-generation tetracyclines improve their gastrointestinal absorption. This increased absorption permits lower oral doses and reduces gastrointestinal side effects.Citation56
Doxycycline is the most common tetracycline associated with gastrointestinal upset.Citation56 The reported rates of gastrointestinal adverse events in clinical trials for the treatment of non-rosacea conditions have been found to range from 0.54% to 51.7% for doxycycline 100 to 200 mg daily.Citation59
Common gastrointestinal adverse effects include heartburn, nausea, vomiting, diarrhea, gastritis, and candidiasis.Citation56,Citation59,Citation60 Esophagitis and esophageal ulcerations are among the most severe gastrointestinal adverse events. They usually occur when the medication is taken before bedtime and with little or no water.Citation56,Citation60–Citation62 Tetracyclines, particularly doxycycline, are the drugs implicated in most of the reported drug-induced esophageal ulcerations (70%).Citation60
Doxycycline hyclate has been noted to be a common cause of drug-induced esophageal ulceration.Citation56,Citation57 The incidence of esophageal ulcers is greater for doxycycline hyclate capsules than with tablets. The capsule may stick to the mucosa of the esophagus if taken with little water. The ulceration results from the physical contact of the capsule with the epithelial lining of the esophagus. The identification of symptoms such as odynophagia, retrosternal pain and dysphagia can be useful in the diagnosis of a doxycycline-induced esophageal ulceration.Citation60,Citation63 The acidity of doxycycline hyclate (pH 2 to 3) contributes to its higher risk of esophageal ulceration when compared with doxycycline monohydrate (pH 5 to 6).Citation56,Citation57,Citation63 For doxycycline hyclate tablets, enteric coated delayed-release tablets (Doryx®; Warner Chilcott (US) Inc.) were found to be superior to the powder-containing tablets (Vibramycin®; Pfizer) when considering gastrointestinal side effects.Citation56,Citation64
Cutaneous adverse effects
The second most common reported adverse effect with doxycycline is skin reactions, which include photosensitivity, pruritus, and unspecified rashes.Citation56,Citation60,Citation62,Citation65 Photosensitivity and photo-onycholysis are reported in up to 7.5% of cases.Citation56,Citation57,Citation66 Doses of doxycycline less than 100 mg daily are a rare cause of photosensitivity.Citation56,Citation67 The relationship between the development of phototoxicity and doxycycline has been shown to be dose dependent occurring in 3% of the patients taking 100 mg daily, 20% of the patients at 150 mg daily and 42% at 200 mg daily.Citation67 Urticarial reactions may occur occasionally in doxycycline-treated patients.Citation57 The characteristic skin pigmentation that occurs during prolonged minocycline administration is not normally seen with doxycycline.Citation56
Other less common adverse effects
Rare side effects of doxycycline include hemolytic anemia, thrombocytopenia, eosinophilia, and neutropenia.Citation56,Citation57,Citation68 Tetracyclines have the potential to cause benign intracranial hypertension (headache, photophobia, diplopia, papilledema, and dizziness, nausea/vomiting), which usually resolve after the discontinuation of the drug.Citation56,Citation69 A yellow-gray-brown tooth discoloration may occur in children.Citation56,Citation60,Citation62 Recently a doxycycline-induced staining of teeth in an adult patient treated for acne was reported by Nelson et al.Citation70 Tetracyclines may temporally inhibit bone growth.Citation62 They are contraindicated in pregnancy (pregnancy category D), breast feeding women and in children younger than eight years.Citation62 Symptoms of dizziness, vertigo or lightheadedness are rarely seen with doxycycline.Citation56
Severe adverse effects associated with tetracyclines are rare events, nevertheless cases of doxycycline-induced Steven-Johnson syndrome and severe hypersensitivity reaction had been reported.Citation71–Citation74 Other uncommon reported doxycycline-induced skin eruptions include fixed drug eruption, acute generalized exanthematous pustular eruption, and Sweet’s syndrome.Citation75–Citation77
Safety of submicrobial dosage of doxycycline monohydrate for rosacea
No major safety concerns have been found for the SDD.Citation31,Citation56 The pooled data of reported adverse events include: nasopharyngitis, diarrhea, headache, upper respiratory infections, hypertension, sinusitis, AST elevation, abdominal pain, fungal infection, and influenza.Citation31,Citation56,Citation78 Gastrointestinal side effects were present but tolerable. Marked blood pressure elevation was reported but not thought to be related to the study drug.Citation31,Citation56 No cases of photosensitivity have been reported to date.Citation24,Citation31,Citation56 The SDD has shown a high safety profile.Citation24,Citation78
Safety of doxycycline in comparison with minocycline and tetracycline
Doxycycline and minocycline differ in their adverse event profile.Citation59 Considerably fewer adverse effects have been reported for doxycycline than for minocycline; the adverse effects for minocycline are 5 times more common than for doxycycline.Citation59
The case report data reviewed by Smith et alCitation59 revealed that the predominant adverse effect secondary to doxycycline use is esophageal erosions. For minocycline a predominance of hyperpigmentation, hypersensitivity, and autoimmune-related adverse effects was observed. Case reports do not necessarily represent the most common adverse events in the daily practice.
Based on the clinical trial data, Smith et alCitation59 found that doxycycline-treated patients most commonly present with gastrointestinal adverse effects (gastritis, bloating, and cramps), while for minocycline-treated patients the central nervous system (dizziness) and gastrointestinal adverse effects were the most common.
In the treatment of acne, gastrointestinal adverse effects have been the most commonly reported, occurring in up to 20% of the doxycyline-treated patients and 25% of minocycline-treated patients.Citation59 Harrison et alCitation79 noted that the tolerance for doxycycline (50 mg daily) was similar to minocycline (50 mg daily); an excellent tolerance was found in 53% and 37% of the patients, respectively.
In a review conducted by Shapiro et alCitation58 more reports of serious adverse events from minocycline use were observed in comparison with other tetracycline antibiotics. This may be related to the minocycline-derived reactive metabolites which are able to bind to tissue macromolecules causing direct cell damage. Minocycline metabolites may also act as haptens and may elicit immune responses such as druginduced lupus.Citation58 To date, there are no reports of tetracyclineor doxycycline-induced lupus. Single-organ dysfunction attributable to doxycycline presents most commonly as a cutaneous adverse reactions (70%), whereas single-organ dysfunction related to minocycline most commonly presents as pneumonitis (45%).Citation58
Group substitutions on the 4-ring structure of the tetracycline antibiotics account for the difference in their adverse events profile.Citation56,Citation58 Doxycycline has a hydroxyl side chain distinguishing it from tetracycline.Citation56,Citation58 Minocycline shares the basic 4-ring structure of the other tetracyclines but has a substitution of a dimethylamino group in the 7th positionCitation58,Citation80 (). Neither tetracycline nor doxycycline contains this amino acid side chain which has the potential to form an iminoquinone reactive metabolite.Citation58
Extrapolating from the literature on aromatic anticonvulsant hypersensitivity reactions, Shapiro et alCitation58 suggested avoiding all tetracyclines in those patients who experience a serious adverse effect while receiving doxycyxline, minocycline, or tetracycline until more information on potential crossreactivity is available.
Relevant drug interactions
Warfarin
The administration of tetracyclines to patients on chronic oral anticoagulation therapy may be associated with a marked enhancement in the anticoagulant effect.Citation56,Citation81 Citation84 An update of the clinicallysignificant drug interactions revealed doxycycline as a “red flag” drug. Doxycycline is one of the 16 red flag drugs that account for the 80% of the clinically significant drug interactions. The interaction of doxycyline with warfarin was classified as severe and well documented.Citation85
Penning-Van Beest et alCitation84 found doxycycline to be the main antibiotic drug (in addition to amoxicillin) in daily practice associated with a statistically significant increase in the risk of bleeding when used concomitantly with warfarin; the relative risk, adjusted for gender and age, was 3 to 5 for doxycycline. The proportion of major bleedings attributable to the interaction of warfarin with doxycycline was estimated to be 18%, gastrointestinal bleeding being the most frequent (79%).Citation84 The enhanced anticoagulation of warfarin by doxycycline administration requires a close monitoring of the patient’s anticoagulation parameters.Citation62
Pharmacodynamic as well as pharmacokinetic mechanisms are involved in the increased anticoagulant effect of warfarin when combined with doxycycline. Pharmacodynamic alteration may result from the elimination of the gut flora leading to a secondary vitamin K deficiency (main mechanism), or may result from the direct inhibition of the synthesis of the vitamin K-dependent coagulation factors.Citation84,Citation85 Pharmacokinetic interactions include the inhibition of the metabolism of warfarin, or the displacement of warfarin from plasma proteins.Citation84 Both doxycycline and warfarin are mostly protein bound, 80% to 90% and >97% respectively. Doxycycline probably displaces the albumin-bound warfarin with a subsequent increase in its fraction.Citation83 Interaction of doxycycline with the cytochrome P-450 system may also alter the enzyme activity, inhibiting the hepatic metabolism of warfarin and thereby leading to an elevated plasma level and an increased risk of bleeding.Citation83
Oral contraceptives
A possible association between the use of tetracyclines and failure of oral contraceptives (OCPs) had been suggested. Still, the true incidence of those failures is unknown.Citation86 In an analysis of unplanned pregnancies reported to the Committee on Safety of Medicines in women taking OCPs and concominant antibiotics, teracyclines, and penicillins were involved in 70% of the reports.Citation87 The largest numbers of apparent reported failures occur in women using low-dose monophasic oral contraceptives containing 30 μg of ethinyl estradiol.Citation78,Citation87
Most of the studies have not demonstrated any systematic interaction between antibiotics and OCPs. Evidence indicating that antibiotics alter blood concentrations of OCPs is lacking. Because the disposition of OCPs components is so variable among individuals, some women may be more susceptible to OCP failure.Citation86 Modern OCP preparations contain smaller amounts of estrogen and have fewer drug interactions, which may contribute to a decrease in their efficacy when combined with doxycycline.Citation86,Citation88
In a controlled clinical trial, Neely et alCitation89 evaluated the effects of doxycycline on OCPs hormone concentrations. No statistically significant differences in serum levels of ethinyl estradiol, norethindrone, or endogenous progesterone were seen between the control and treatment phases. However, a large inter-patient and intra-patient variability in ethinyl estradiol and norethindrone levels was observed. Neely et alCitation89 suggested that pregnancies attributed to failure of OCPs because of tetracycline use could represent a true interaction that only manifests itself in a small proportion of women at risk.
Murphy et alCitation90 found no significant decrease in the plasma ethinyl estradiol or norethindrone concentration in either short-term (24 hours) or long-term (5 to 10 days) ingestion of tetracycline (tetracycline 500 mg orally every 6 hours) in women ingesting oral contraceptives (ethinyl estradiol 35 μg and norethindrone 1 mg).
Archer et alCitation91 reviewed the pharmacokinetic and the clinical literature on the efficacy of oral contraceptives when used concomitantly with antibiotic therapy. Relevant clinical reports of contraceptive failure with antibiotic use were found to be retrospective, to have multiple potential biases, and were not supported by pharmacokinetic data. Archer et alCitation91 concluded that the available scientific and pharmacokinetic data do not support the hypothesis that antibiotics, with the exception of rifampin, lower the efficacy of oral contraceptives.
Other drug interactions
Concomitant use of tetracycline (primarily minocycline) and oral retinoids has been associated with benign intracranial hypertension.Citation78 It is a well-documented clinically significant drug interaction, where a synergistic effect of the medications increases the risk of pseudotumor cerebri.Citation85
Tetracyclines can interfere with methotrexate and other protein bound medications by displacing them from their binding sites.Citation56
Anticonvulsants (barbiturates, carbamazepine, and phenitoin) induce the hepatic microsomal metabolism of tetracyclines and consequently decrease tetracycline serum concentrations.Citation62 Cholesteramine and colestipol may bind tetracycline and reduce gastrointestinal absorption.Citation62
Dosing
Several oral formulations of doxycycline are currently approved by the FDA (), although only doxycycline 40 mg USP (Oracea®) is approved for the treatment of rosacea. Doses ranging between 40 mg to 100 mg daily from 8 to 16 weeks are most commonly used in the treatment of rosacea. They can be used safely in patients with renal failure.Citation9,Citation16
Table 4 Available formulations of doxycyclineCitation92
Milk, antiacids, iron supplements, and probably other substances with calcium, magnesium, aluminum, and iron have been shown to decrease tetracycline gastrointestinal absorption and should be ingested at least several hours before or after the administration of tetracyclines.Citation62 Although doxycycline absorption may be less affected by these divalent or trivalent cations, avoiding administration within 1 to 2 hours after ingestion of interfering food or medication is prudent.Citation62 Also, the risk of esophageal ulceration reported with the use of doxycycline can be minimized with adequate fluid intake and avoiding lying down after oral intake of the capsule or tablet.Citation63 For this reason, doxycycline is best administered in the morning with plenty of water. Doses of doxycycline <100 mg daily are seldom associated with photosensitivity and have not been reported to date with the use of SDD.Citation24,Citation56,Citation57 Still, patients should be warned about this potential side effect and advised to practice sun protection measures.
Conclusions
Available research and clinical experience have demonstrated that doxycycline safely improves the signs and symptoms of rosacea. Doxycycline exhibits antiangiogenic and anti-inflammatory properties that are effective in the treatment of rosacea and penetrates into normal and inflammatory tissues more readily than tetracycline. Also, it exhibits superior pharmacokinetic properties and lesser toxicity when compared with first-generation tetracyclines. Subantimicrobial dose doxycycline has not been associated with the development of antibiotic resistance. Anti-inflammatory dose doxycycline 40 mg is dosed once daily improving patient compliance without altering antibiotic susceptibility, and having lesser toxicity when compared to the standard 100 mg daily dose. In sum, a series of clinical studies have confirmed that doxycycline is safe and effective as a therapeutic option in rosacea.
Disclosures
The authors have no conflicts of interest to disclose.
References
- BergMLidenSAn epidemiological study of rosaceaActa Derm Venerol1989694194232572109
- PowellFCRosaceaN Engl J Med200535279380315728812
- WilkinJDahlMDetmarMStandard classification of rosacea: report of the National Rosacea Society Expert Committee on the Classification and Staging of RosaceaJ Am Acad Dermatol20024658458711907512
- PelleMTCrawfordGHJamesWDRosacea: II. TherapyJ Am Acad Dermatol20045149951215389184
- SneddonIBA clinical trial of tetracycline in rosaceaBr J Dermatol1966786496524224811
- SmilackJDThe tetracyclinesMayo Clin Proc19997472772910405705
- SapadinANFleischmajerRTetracyclines: Nonantibiotic properties and their clinical implicationsJ Am Acad Dermatol200654225826516443056
- MaibachHSecond-generation tetracyclines, a dermatologic overview: Clinical uses and pharmacologyCutis1991484114171764965
- CunhaBASibleyCMRistucciaAMReview doxycyclineTher Drug Monit198241151357048645
- JonasMCunhaBAReview minocyclineTher Drug Monit198241371457048646
- MacdonaldHKellyRGAllenESPharmacokinetic studies of minocycline in manClin Pharmacol Ther1973148524199710
- SaivinSHouinGClinical pharmacokinetics of doxycycline and minocyclineClinical Pharmacokinet198815355366
- FabreJMilekEKalfopoulosPThe kinetics of tetracyclines in man. Digestive absorption and serum concentrationsSchweiz Med Wochenschr19711015935984995974
- WeinbergJMThe anti-inflammatory effects of tetracyclinesCutis200575 Suppl 4S6S11
- CullenSCrounseRCutaneous pharmacology of the tetracyclinesJ Invest Dermatol1965452632684953785
- PallettAPSmythEGClinician’s guide to antibiotics. TetracyclineBr J Hosp Med1988403853903069173
- WebsterGDel RossoJQAntiinflammatory effects of TetracyclinesDermatology Clin200725133135
- EsterlyNBFureyNLFlannaganLEThe effect of antimicrobial agents on chemotaxisJ Invest Dermatol1978705155618981
- EsterlyNBKovanskyJSFureyNSNeutrophil chemotaxis in patients with acne receiving tetracyclinesArch Dermatol1984120130813136237616
- GablerWLCreamerHRSupression of human neutrophil functions by tetracyclineJ Periodontal Res19912652581847418
- ThongYHFerranteAInhibition of mitogen-induced human lymphocyte proliferative responses by tetracycline analogsClin Exp Immunol197935443446455782
- PruzanskiWGreenwaldRAStreetIPLaliberteFStefanskiEVadasPInhibition of enzymatic activity of phospholipase A2 by minocycline and doxycyclineBiochem Pharmacol1992P44116511701417938
- WiseRDSubmicrobial doxycycline and rosaceaComp Ther2007337881
- BikowskiJBSubantimicrobial dose doxycycline for acne and rosaceaSkinmed2003223424514673277
- GolubLMLeeHMRyanMEGiannobileWVPayneJSorsaTTetracyclines inhibit connective tissue breakdown by multiple non-antimicrobial mechanismsAdv Dent Res19981212269972117
- GolubLMLeeHMLehrerGMinocycline reduces gingival collagenolytic activity during diabetes: preliminary observations and a proposed new mechanism of actionJ Periodont Res1983185165266315909
- GolubLMRamamurthyNSMcNamaraTFGreenwaldRARifkinBRTetracyclines inhibit connective tissue breakdown: new therapeutic implications for an old family of drugsCrit Rev Oral Biol Med199122973211654139
- BermanBZellDSubantimicrobial dose doxycycline: a unique treatment for rosaceaCutis200575 Suppl 4S19S24
- BikowskiJNew approaches to rosacea therapySkin Aging200513 Suppl 2S13S15
- HanemaaijerRVisserHKoolwijkPInhibition of MMP synthesis by doxycycline and chemically modified tetracyclines (CMTs) in human endothelial cellsAdv Dent Res1998121141189972133
- Del RossoJQWebsterGFJacksonMTwo randomized phase III clinical trials evaluating anti-inflammatory dose doxycycline (40-mg doxycycline, USP capsules) administered once daily for treatment of rosaceaJ Am Acad Dermatol20075679180217367893
- WebsterGFTosoSMHegemannLInhibition of a model of in vitro granuloma formation by tetracyclines and ciprofloxacin. Involvement of protein kinase CArch Dermatol19941307487528002645
- AminARAtturMGThakkerGDA novel mechanism of action of tetracyclines: effects on nitric oxide synthasesProc Natl Acad of Sci U S A19969314014140198943052
- AminARPatelRNThakkerGDLowensteinCJAtturMGAbramsonSBPost-transcriptional regulation of inducible nitric oxide synthase mRNA in murine macrophages by doxycycline and chemically modified tetracyclinesFEBS Lett19974102592649237641
- SkidmoreRKovachRWalkerCEffects of subantimicrobial-dose doxycycline in the treatment of moderate acneArch Dermatol2003139 445946412707093
- ThiboutotDEfficacy and safety of subantmicrobial-dose doxycycline for the treatment of rosacea [poster]63rd Annual Meeting of the American Academy of DermatologyFebruary 18–22, 2005New Orleans, LAP128
- SanchezJSomolinosALAlmodovarPIWebsterGBradshawMPowalaCA randomized, double-blinded, placebo-controlled trial of the combined effect of doxycycline hyclate 20-mg tablets and metronidazole 0.75% topical lotion in the treatment of rosaceaJ Am Acad Dermatol20055379179716243127
- FowlerJFCombined effect of anti-inflammatory dose doxycycline (40-mg doxycycline, USP monohydrate controlled-release capsules) and metronidazole topical gel 1% in the treatment of rosaceaJ Drugs Dermatol2007664164517668530
- Del RossoJSchlessingerJWerschlerPComparison of anti-inflammatory dose doxycycline versus doxycycline 100 mg in the treatment of rosaceaJ Drugs Dermatol2008757357618561589
- AkpekEKMerchantAPinarVFosterCSOcular rosacea: Patient characteristics and follow-upOphthalmology1997104186318679373118
- Frucht-PeryJChayetASFelmanSTLinSBrownSIThe effect of doxycycline in ocular rosaceaAm J Ophthalmol19891074344352522739
- Frucht-PeryJSagiEHemoIEver-HadaniPEfficacy of doxycycline and tetracycline in ocular rosaceaAm J Ophthalmol199311688928328549
- QuatermanMJJohnsonDWAbeleDCLesherJLHullDSDavisLSOcular rosacea: Signs, symptoms, and tear studies before and after treatment with doxycyclineArch Dermatol199713349549006372
- TorresaniCPavesiAManaraGCClarithromycin versus doxycycline in the treatment of rosáceaInt J Dermatol1997369389469466205
- AkhyaniMEhsaniAHGhiasiMJafariAKComparison of efficacy of azithromycin vs. doxycycline in the treatment of rosacea: a randomized open clinical trialInt J Dermatol20084728428818289334
- HersleKGisslenHMinocycline in acne vulgaris: a double-blind studyCurr Ther Res197619339342131678
- HarrisonPVA comparison of doxycycline and minocycline in the treatment of acne vulgarisClin Exp Dermatol1988132422442977578
- LauxBTreatment of acne vulgaris. A comparison of doxycycline versus minocyclineDermatologist198940577581
- OlafssonJHGudgiersonJEggertsdottirGEKristjanssonFDoxycycline versus minocycline in the treatment of acne vulgaris: a doubleblind studyJ Dermatol Treat198911517
- Del RossoJQRecently approved systemic therapies for acne vulgaris and rosaceaCutis20078011312017944168
- EadyAHCoveJHLaytonAMIs antibiotic resitance in cutaneous propionibacteria clinically relevant? Implications of resistance for acne patients and prescribersAm J Clin Dermatol2003481383114640775
- ThomasJWalkerCBradshawMLong-term use of subantimicrobial dose doxycycline does not lead to changes in antimicrobial susceptibilityJ Perio20007114721483
- GolubLMSorsaTLeeHMDoxycycline inhibits neutrophil (PMN)-type matrix metalloproteinases in human adult periodontitis gingivaJ Clin Periodontol1995221001097775665
- Del RossoJQA status report on the use of subantimicrobial-dose doxycycline: A review of the biologic and antimicrobial effects of the tetracyclinesCutis20047411812215379364
- WalkerCWebsterGFDel RossoJQA muticenter, double-blind, randomized trial to evaluate the long-term anti-inflammatory doxycycline (40 mg) therapy: results of the lack of effect on bacterial flora [poster]Foundation for Reaserch and Education in Dermatology, Fall Clinical Dermatology ConferenceOctober 6–9, 2006Las Vegas, Nevada
- SloanBScheinfeldNThe use and safety of doxycycline hyclate and other second-generation tetracyclinesExpert Opin Drug Saf2008757157718759709
- Del RossoJQSystemic therapy for rosacea: focus on oral antibiotic therapy and safetyCutis20006671311455753
- ShapiroLEKnowlesSRShearNHComparative safety of tetracycline, minocycline, and doxycyclineArch Dermatol1997133122412309382560
- SmithKLeydenJJSafety of doxycycline and mnocycline: a systematic reviewClin Ther2005271329134216291409
- SegelnickSLWeinbergMARecognizing doxycycline-induced esophageal ulcers in dental practice: a case report and reviewJ Am Dent Assoc200813958158518451374
- BillerJAFloresABuieTMazorSKatzAJTetracycline-induced esophagitis in adolescent patientsJ Pediatr19921201441451731012
- SmilackJDThe tetracyclinesMayo Clin Proc19997472772910405705
- LanzaFLEsophageal ulceration produced by doxycycline Review of the literature and comparison of the injury from doxycycline hyclate and hydrochloride with that from doxycycline monohydrateCurr Ther Res Clin Exp198844475484
- BergerRSA double-blind, multiple-dose, placebo-controlled, cross-over study to compare the incidence of gastrointestinal complaints in healthy subjects given Doryx R and Vibramycin RJ Clin Pharmacol1988283673703392234
- SmithKLeydenJJSafety of doxycycline and minocycline: a systematic reviewClin Ther2005271329134216291409
- CarrollLALaumannAEDoxycycline-induced photo-onycholysisJ Drugs Dermatol2003266266314711147
- LaytonAMCunliffeWJPhototoxic eruptions due to doxycycline-a dose-related phenomenonClin Exp Dermatol1993184254278252763
- SimpsonMBPryzbylikJInnisBDenhamMAHemolytic anemia after tetracycline therapyN Engl J Med19853128408423974663
- PierogSHAl-SalihiFLCinottiDPseudotumor cerebri – a complication of tetracycline treatment of acneJ Adolesc Health Care198671391402937759
- NelsonRParkerSRDoxycycline-induced staining of adult teeth: the first reported caseArch Dermatol20061421081108216924074
- CacNNMessinghamMJSniezekPJWallingHWStevens-Johnson syndrome induced by doxycyclineCutis20077911912217388211
- CurleyRKVerbowJLStevens-Johnson syndrome due to tetracycline-a case report (doxycycline) and a review of the literatureClin Exp Dermatol1987121241253677470
- GallaisVRandrianjohannyARobineauMLarocheLStevens-Johnson syndrome caused by doxycyclinePresse Med1997268559207884
- RoblesDTLeonardJLComptonNSevere drug hypersensitivity reaction in a young woman treated with doxycyclineDermatology2008217232618332631
- GulUGonulMSoyluSKayaIDoxycycline-induced fixed drug eruptionJ Dermatolog Treat20081912612718484432
- TrüebRMBurgGAcute generalized exanthematous pustulosis due to doxycyclineDermatology199318675788435524
- Khan DuraniBJappeUDrug-induced Sweet’s syndrome in acne caused by different tetracyclines: case report and review of the literatureBr J Dermatol200214755856212207601
- BermanBPerezOAZellDUpdate on rosacea and anti-inflammatory-dose doxycyclineDrugs Today200743273417315050
- HarrisonPVA comparison of doxycycline and minocycline in the treatment of acne vulgarisClin Exp Dermatol1988132422442977578
- AllenJCMinocyclineAnn Intern Med197685482487788583
- BaciewiczAMBalBSBleeding associated with doxycycline and warfarin treatmentArch Intern Med2001161123111343446
- CaracoYRubinowAEnhanced anticoagulant effect of coumarin derivatives induced by doxycycline coadministrationAnn Pharmacother199226108410861421670
- HasanSAInteraction of doxycycline and warfarin: an enhanced anti-coagulant effectCornea20072674274317592328
- Penning-van BeestFJKoerselmanJHeringsRMRisk of major bleeding during concomitant use of antibiotic drugs and coumarin anticoagulantsJ Thromb Haemost2008628429018031295
- BarrancoVPUpdate on clinically significant drug interactions in dermatologyJ Am Acad Dermatol20065467668416546592
- DickinsonBDAltmanRDNielsenNHSterlingMLCouncil on Scientific Affairs, American Medical AssociationDrug interactions between oral contraceptives and antibioticsObstet Gynecol20019885386011704183
- BackDJGrimmerSFOrmeMLProudloveCMannRDBreckenridgeAMEvaluation of Committee on Safety of Medicines yellow card reports on oral contraceptive-drug interactions with anti-convulsants and antibioticsBr J Clin Pharmacol1988255275323408633
- SzokaPREdgrenRADrug interactions with oral contraceptives: compilation and analysis of an adverse experience report databaseFertil Steril19884931S38S3282933
- NeelyJLAbateMSwinkerMD’AngioRThe effect of doxycycline on serum levels of ethinyl estradiol, norethindrone, and endogenous progesteroneObstet Gynecol1991774164201992409
- MurphyAAZacurHACharachePBurkmanRTThe effect of tetracycline on levels of oral contraceptivesAm J Obstet Gynecol199116428331986620
- ArcherJSArcherDFOral contraceptive efficacy and antibiotic interaction: a myth debunkedJ Am Acad Dermatol20024691792312063491
- FDA.gov (homepage on the Internet)Approved Drug Products with Therapeutic Equivalence Evaluations (Orange Book) (updated 2009 Jan 23; cited 2009 Feb 26) Available from: http://www.fda.gov/cder/orange/default.htm