Abstract
After more than 40 years of clinical use, levodopa (LD) remains the gold standard of symptomatic efficacy in the drug treatment of Parkinson’s disease (PD). Compared with other available dopaminergic therapies, dopamine replacement with LD is associated with the greatest improvement in motor function. Long-term treatment with LD is, however, often complicated by the development of various types of motor response oscillations over the day, as well as drug-induced dyskinesias. Motor fluctuations can be improved by the addition of drugs such as entacapone or monoamine oxidase inhibitors, which extend the half-life of levodopa or dopamine, respectively. However, dyskinesia control still represents a major challenge. As a result, many neurologists have become cautious when prescribing therapy with LD. This review summarizes the available evidence regarding the use of LD to treat PD and will also address the issue of LD delivery as a critical factor for the drug’s propensity to induce motor complications.
Introduction
After more than 40 years of clinical use, levodopa (LD) remains the gold standard regarding symptomatic efficacy in the drug treatment of Parkinson’s disease (PD).Citation1 Compared with other available dopaminergic therapies, dopamine replacement with LD is associated with the greatest improvement in motor function, as assessed by reduced scores in the Unified Parkinson’s Disease Rating Scale [UPDRS]).Citation2–Citation5 In addition, responsiveness to LD (required to exceed 25%–30% reduction in the motor part of the UPDRS) is a diagnostic criterion for PD.Citation6 In clinical practice, LD slows the progression of disability as assessed by the Hoehn and Yahr staging system,Citation7 and is associated with a reduction in mortality.Citation8,Citation9 Importantly, LD is one of the best tolerated drugs to treat PD, particularly in the elderly population.Citation10
However, long-term treatment with LD is often complicated by the development of various types of motor response oscillations over the day as well as drug-induced dyskinesia, a complication characterized by erratic involuntary movements. Such treatment-related motor complications eventually develop in the majority of patients and are found in about one-third of patients after only two years of exposure.Citation11 Once established, motor complications are difficult to treat and can develop into a significant source of disability. In extreme cases, treatment-induced dyskinesias may completely annihilate the therapeutic benefit initially gained from the drug. Concerns about the potential induction of long-term motor complications have led many physicians to use LD in a restricted manner and reserve it as a second-line strategy. This approach has gained wide acceptance following clinical trials in early PD, showing significantly reduced risks of developing motor complications with dopamine agonists (DAs) as compared with LD monotherapy.Citation2–Citation5 While these trials have indeed established the potential of DAs to delay the onset of motor complications, they have also consistently demonstrated the superior symptomatic efficacy of LD, with a need for LD supplementation within the first 2–3 years in most patients started on a DA.Citation2
Despite such evidence from clinical trials of the need for LD supplementation to maintain symptomatic control in early PD, in general clinical practice, LD is often withheld beyond the time when symptomatic control with DAs has become insufficient.Citation12 This results, in part, from patient perceptions. Information gleaned from physicians or the media may alert patients to the risk of dyskinesia associated with LD. The alarming nature of dyskinesia can, in turn, lead to a phenomenon labeled “dopa-phobia”.Citation12 These concerns have even been extrapolated to using single doses of LD in challenge tests, in order to prime the striatum putatively for subsequent dyskinetic responses to dopaminergic therapies.Citation13
Increasing evidence now suggests that motor complications (particularly dyskinesia) associated with sustained LD therapy are a result of discontinuous and intermittent delivery of LD to the brain, resulting in nonphysiologic pulsatile stimulation of striatal dopamine receptors. Thus, the short half-life (90 minutes) of immediate-release LD formulations is thought to be the key factor in the pathogenesis of motor complications, rather than their induction being an intrinsic property of the LD molecule.Citation1 This review will summarize the available evidence regarding the use of LD to treat PD and will also address the issue of LD delivery as a critical factor for the drug’s propensity to induce motor complications.
Efficacy of levodopa in early Parkinson’s disease
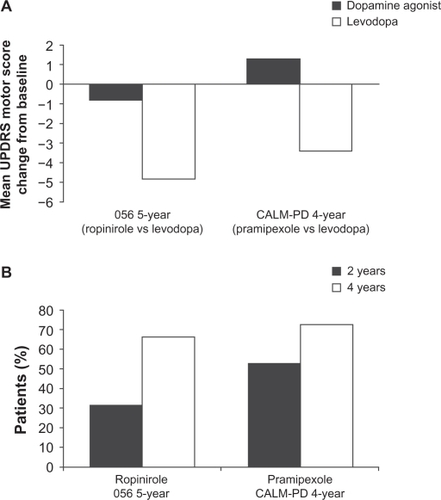
There have been a number of large-scale, long-term, LD-controlled monotherapy trials of DAs in early Parkinson’s disease on which strong conclusions about the relative effect size of LD compared with DAs can be based. The four-year randomized Comparison of the Agonist Pramipexole versus Levodopa on Motor Complications of Parkinson’s Disease (CALM-PD) trial, compared initial treatment with pramipexole (0.5 mg three times daily) versus LD-carbidopa (100/25 mg three times daily), followed by open-label LD supplementation as required.Citation2 The primary outcome measure was the time to first occurrence of dopaminergic complications, which included wearing-off (the re-emergence of PD symptoms due to the diminishing effect of LD), dyskinesias, “on–off ” fluctuations (unpredictable fluctuations varying between symptoms being well controlled [on] to uncontrolled [off]), and freezing. Secondary outcome measures were changes in UPDRS scores and quality of life. Although initial treatment with pramipexole resulted in lower incidences of dyskinesia and wearing-off compared with initial treatment with LD, symptom control, as assessed by the UPDRS, was superior in patients treated with LD. From baseline to month 48, there was a worsening from baseline of 1.3 ± 13.3 (mean ± standard deviation [SD]) points in UPDRS motor scores in the pramipexole group compared with an improvement of 3.4 ± 12.3 points in the LD group (treatment difference of 4.9 points, P = 0.001) as shown in .
Figure 1 Mean ± standard deviation change from baseline in A) Unified Parkinson’s Disease Rating Scale (UPDRS) motor scores during the course of the five-year 056 and four-year comparison of the CALM-PD (Comparison of Agonist Pramipexole versus Levodopa on Motor Complications of Parkinson’s Disease) trials by treatment assignment. B) Percentage of patients receiving monotherapy with dopamine agonists requiring levodopa supplementation after two and four years of treatment.Citation2
Interestingly, even though physicians in this trial had the option to use open-label LD supplementation to enhance symptomatic control, the group differences observed in the UPDRS motor and activities of daily living components between patients randomized to pramipexole or LD remained relatively uniform throughout the four years of the study. It is not definitely established why the UPDRS scores of the pramipexole group never caught up with the LD group, despite the option of open-label LD and other antiparkinsonian therapies, but it might be related to the lower dose of LD used in the supplemented pramipexole patients (434 ± 498 mg/day) compared with those on LD monotherapy (702 ± 461 mg/day). Indeed, the calculated LD equivalent dose used in the supplemented pramipexole patients falls in the range of 468–584 mg/day, which is notably less than the 702 ± 461 mg/day dose used in patients initiated on LD monotherapy. This indicates that combined treatment with a lower dose of LD and a DA is not equivalent to higher dose LD monotherapy in terms of symptomatic control, calling into question the concept of LD-equivalent doses of DAs.
In the five-year 056 study, which compared the safety and efficacy of ropinirole with that of LD, the primary efficacy measure was the occurrence of dyskinesia.Citation3 Ropinirole was initiated at 0.25 mg three times daily and increased weekly, as necessary, up to a maximum dose of 8 mg three times daily. Levodopa was initiated at a dose of 50 mg once daily and increased weekly, as necessary, to a maximum of 400 mg three times daily. As in the CALM-PD study, if symptoms were not adequately controlled by the assigned study medication, patients could receive supplementary LD, administered in an open-label fashion. In this study, 84% of all patients initiated on ropinirole monotherapy either required LD supplementation (427 ± 221 mg/day) or dropped out of the study. Although this study demonstrated a reduced incidence of dyskinesia for ropinirole versus LD (20% versus 45%, respectively), this benefit was once again found to be at the expense of symptomatic control. In those patients who completed the study, there was a minimal improvement from baseline of 0.8 ± 10.1 points in UPDRS motor scores in the ropinirole group, contrasting with an improvement of 4.8 ±8.3 points in the LD group (). Similar results confirming the superior efficacy of LD (in terms of UPDRS motor scores) were also observed in the two-year REAL-PET (ReQuip as Early Therapy versus L-dopa–Positron Emission Tomography) study of LD versus ropinirole monotherapy.Citation14
The clinical relevance of such differences in UPDRS scores has been debated, but is vividly illustrated by the increasing rates of supplementation with open-label LD over the course of these double-blind comparative trials. At four years’ follow-up in the CALM-PD trial, 72% of patients randomized to pramipexole monotherapy had required add-on LD to maintain symptomatic control, and this figure was 66% after five years in the 056 study with ropinirole ().Citation2–Citation5 The term “LD rescue”, commonly used in this context, aptly describes the role of LD as the most efficacious drug at hand to control motor symptoms when other drugs begin to fail.
The recently published PELMOPET (Pergolide versus L-dopa Monotherapy and Positron Emission Tomography) studyCitation5 employed a strict pergolide (0.75–5.0 mg/day) and LD (150–1200 mg/day) monotherapy design in which no rescue therapy was allowed. At one year, there was a relatively small difference in favor of LD in the mean change from baseline in UPDRS motor scores (−3.2 points in the pergolide treatment group compared with −5.2 points in the LD treatment group). However, after three years of monotherapy, patients receiving pergolide had deteriorated below baseline by 2.8 ± 9.8 points, whereas patients receiving LD were still improved by 2.8 ± 7.8 points.
Taken together, these LD-controlled trials of DA monotherapy in early PD clearly show the need for LD supplementation to maintain symptomatic control.
Delaying dyskinesias using initial monotherapy with dopamine agonists
Current recommendations to initiate dopaminergic therapy in early PD with a DA, or even a monoamine oxidase inhibitor, are chiefly based on concerns about the evolution of motor complications characteristic of sustained LD therapy, most notably drug-induced dyskinesias. While the monotherapy trials cited above have clearly established a reduced dyskinesia risk with DA monotherapy, they have also shown that this is exclusively due to the delay in starting patients on LD. Indeed, PD patients initiated on a DA in these trials eventually required supplemental LD in order to maintain symptomatic control, and developed dyskinesias at an identical rate (albeit with a delay) to those started on LD, leading to steady increases in dyskinesia rates from this point onwards.Citation15 Therefore, the question remains as to whether the initial benefit of reduced motor complication rates can be maintained in the longer term when virtually all patients will be on combined drug treatment with DAs, LD, and possibly other agents. While none of the aforementioned comparative trials has been designed to assess outcomes under double-blind conditions for longer than five years, longer term, open-label, follow-up data are available. The Parkinson Study Group recently reported on the six-year outcomes of patient groups initially randomized to receive monotherapy with pramipexole or LD in the CALM-PD trial. Results of this study showed a persistent, statistically significant difference in overall dyskinesia rates of about 37% in those randomized to initial LD compared with 20% in those initiated on pramipexole (P = 0.004).Citation16 Despite this, 90% of the population followed were on LD by six years.Citation16 Similarly, 10-year outcomes reported by Lees et alCitation17 comparing initial monotherapy with bromocriptine versus LD, along with Hauser et alCitation18 from the 056 ropinirole study, also demonstrated a reduced overall incidence of dyskinesias with DAs in the long term. After 10 years, 45% of patients who were initiated with bromocriptine had dyskinesias compared with 54% of those started on LD (corresponding to an incidence rate for first dyskinesia occurrence of 145.3 versus 105.9 per 1000 patient-years after starting treatment with LD or DA, respectively).Citation17 Similar figures were reported for the 10-year follow-up of patients of the 056 study of ropinirole versus LD (52.4% versus 77.8%, P = 0.0457).Citation19
While these results convincingly show long-term reductions in the incidence of dyskinesia with DAs compared with LD, rates of dyskinesia do not necessarily reflect differences in dyskinesia-related disability between treatments. Hauser et alCitation20 were the first to demonstrate differential functional significance of dyskinesias by asking patients to rate their involuntary movements as “troublesome” or “nontroublesome” in a modified “on/off ” diary. When patients were subsequently asked to rate their recorded “on” or “off ” times as functionally “good” or “bad” periods, 93.8% of “on” time with nontroublesome dyskinesia was considered functionally “good” time, whereas 84.9% of “off ” time and 89.9% of “on” time with troublesome dyskinesia was considered “bad” time.Citation20
In this respect, it is interesting to note that, at 10 and 14 years, respectively, neither the ropinirole nor bromocriptine studies found significant differences between treatment arms in the emergence of disabling dyskinesia.Citation15,Citation17,Citation21 This finding was also observed in the CALM-PD study at four years, where the rate of disabling dyskinesias was low in patients treated with either pramipexole or LD.Citation16 In addition, the recent STRIDE-PD (Stalevo Reduction In Dyskinesia Evaluation) trial comparing time to dyskinesia development in patients treated with either standard LD or a fixed combination of LD, carbidopa, and entacapone showed a less than 10% incidence of disabling dyskinesias in both groups.Citation22
Furthermore, patient surveys have also indicated that patients with dyskinesias are less concerned about their dyskinesias than those who have not yet experienced dyskinesias, and that more than 80% of these patients prefer having dyskinesia over their PD symptoms.Citation23 Since patients often tolerate mild dyskinesia well, the risk of dyskinesia should not cause physicians to delay LD initiation in patients whose PD symptoms cannot be sufficiently controlled with other treatments, regardless of patient age. Given these findings, the decision to initiate LD must be tailored to the patient’s needs and should include proper counseling about the impact of dyskinesia and current options to minimize their incidence, including cautious LD dosing, or to treat them once they are present.
Tolerability and safety issues
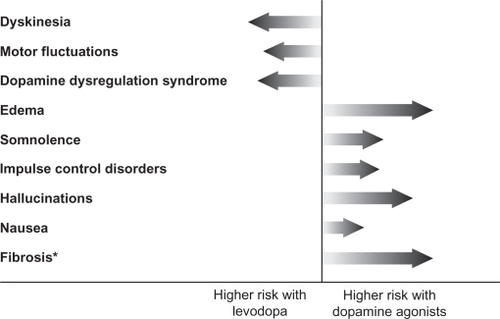
In routine clinical practice, the benefits and risks of any anti-PD therapy must be weighed before prescribing the medication. LD therapy is generally well tolerated, and acute side effects include nausea, vomiting, and hypotension.Citation24,Citation25 As such, LD is generally started at a low dose to minimize these risks. With chronic use, the most common complications include wearing-off and dyskinesia, which can be troublesome for the patient ().Citation26 However, while the use of DAs is not associated with motor complications, a different array of side effects, including hallucinations, somnolence, and edema, are observed more commonly with these anti-PD medications (). Dopamine agonists have also been linked to impulse-control disorders, such as pathologic gambling, hypersexuality, binge eating, or pathologic shopping, with about 13.7%–17.1% of patients on DA therapy showing signs of such disorders.Citation27–Citation29 While some of the adverse events associated with DA therapy are often perceived to be less bothersome for patients than LD-induced motor complications, others such as impulse-control disorders and sleep attacks, can have serious consequences for both the patient and their social relationships such that the advantages of delaying LD-associated risks by treatment with DAs may be negated. Therefore, the choice of therapy should be an individualized decision that takes into account the differential risk profiles of the various DA replacement strategies.
Figure 2 Comparison of the risk of motor complications and other adverse events associated with levodopa versus dopamine agonists. The length of the arrow reflects the extent of risk.
Levodopa and progression of Parkinson’s disease
Another perceived risk of LD that still causes concern among many neurologists is related to its effect on disease progression. In the early 1990s, a number of in vitro studies demonstrated that high doses of LD can be toxic to dopaminergic neurons in cell culture,Citation30–Citation32 causing some PD specialists to recommend withholding LD for as long as possible.Citation33 Since that time, data have accumulated showing that LD may also have protective effects for cultured dopamine neurons, depending on experimental conditions, such as presence or absence of gliaCitation34,Citation35 or ascorbic acid,Citation36,Citation37 as well as LD dose used.Citation38 In addition, many in vivo studies could not find evidence of LD-induced neurodegeneration in normal rodents,Citation39 primates,Citation40 and nonparkinsonian humans,Citation41 and some have even reported neuroprotective effects of LD on midbrain dopaminergic neurons.Citation42,Citation43 Of particular interest are pathology reports from patients with essential tremor or dopa-responsive dystonia who had been chronically exposed to large amounts of LD over many years. None of these patients have shown evidence of substantia nigra degeneration at autopsy.Citation8,Citation9,Citation44
After almost 40 years of established clinical use, the Parkinson Study Group recently conducted the first high-quality, randomized, placebo-controlled trial of LD to define better the effects of LD monotherapy on clinical progression in early PD.Citation45 The ELLDOPA (Earlier versus Later Levodopa) study included 361 patients with early PD who were randomized to receive LD–carbidopa at a daily dose of 150/37.5 mg, 300/75 mg, or 600/150 mg, respectively, or a matching placebo for a period of 40 weeks. The primary outcome was the difference in UPDRS scores between treatment groups at week 42 after withdrawal of treatment for two weeks. This endpoint was chosen to detect any potential underlying effect of active treatment on PD progression, with the assumption that a two-week washout period would remove all symptomatic LD effects, and any remaining differences in UPDRS scores between groups by this time would reflect treatment effects on disease progression. In addition, assessments of striatal dopamine transporter density using iodine-123-labeled 2-β-carboxymethoxy-3-β-(4-iodophenyl)tropane ([123I] β-CIT) single photon emission computed tomography were performed at baseline and at the end of study as a surrogate measure of progression of nigrostriatal terminal dysfunction. After a two-week washout period, the UPDRS motor scores in each group of LD-treated patients were still significantly improved compared with patients on placebo. This not only seems to exclude any evidence for negative effects of LD on the progression of PD but, on the contrary, suggests that treatment with LD results in a decline of UPDRS scores over time as compared with placebo. Nevertheless, there remains a possibility that a two-week washout could be insufficient for symptomatic effects of LD to wear off completely, thus precluding firm conclusions about the disease-modifying efficacy of LD from this study. Adding to this uncertainty, there was a significantly greater decline of striatal β-CIT binding in the high-dose arm of this trial compared with placebo in patients with abnormal scans at baseline. Interpretation of this finding is again confounded by the possibility of regulatory effects of LD on dopamine transporter binding or expression.
Integrating the currently available evidence from experimental studies and clinical trials, there is very little reason to assume that LD might hasten the clinical progression of PD, and withholding the drug because of such fears from patients in clinical need of optimized symptomatic control is not warranted. Accordingly, US and European PD practice guidelines consistently recommend early use of LD in patients requiring initiation of dopaminergic treatment when the perceived dyskinesia risk is low, as is the case in the elderly.Citation46
Challenge of optimizing levodopa delivery
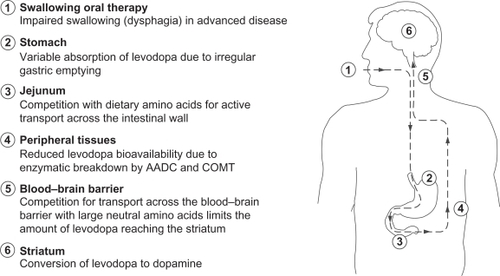
The mechanism of action of LD is related to its activity as a prodrug for central dopamine and involves a number of critical steps, including gastrointestinal absorption, passage across the blood–brain barrier, neuronal uptake, and conversion to dopamine via enzymatic action of aromatic amino acid decarboxylase (AADC) (), and eventually synaptic release of dopamine thus generated from exogenous LD. This sequence of events, needed for LD to exert its antiparkinsonian effect, is subject to a number of interfering processes, which can contribute to dose failures and long-term complications.Citation47 These include delayed gastric emptying and altered absorption of LD due to a competitive effect with ingested proteins at the level of amino acid transporters located in the gastrointestinal tract and the blood–brain barrier. Two major peripheral LD metabolic pathways, driven by the enzymes AADC and catechol-O-methyl transferase, significantly deplete the amount of LD reaching the brain. In addition, the short half-life (36–96 minutes) of LD is associated with fluctuating LD plasma levels, which eventually translate into fluctuating levels of synaptic dopamine derived from exogenous LD.Citation47 Consequently, for optimal benefit, LD has to be administered as multiple daily doses, but conventional three times daily regimens have not been found to be sufficient to establish constant plasma levels.Citation48
Figure 3 Oral levodopa therapy – hurdles on the route from the mouth to the brain. A number of factors impact on the progress of levodopa from the time of ingestion until it reaches the brain and is converted to dopamine.
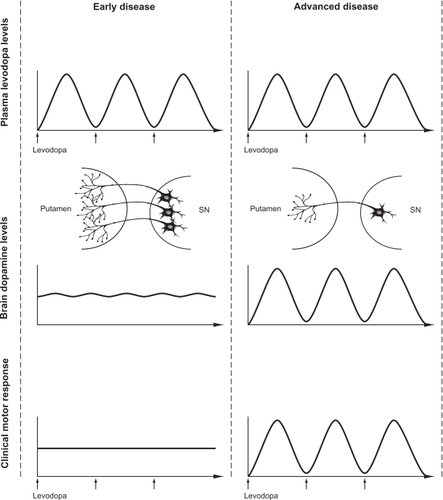
In the earlier stages of the disease, oscillations in plasma levels are not clearly associated with fluctuations in motor function, presumably due to central “buffering” via intraneuronal storage in surviving nigrostriatal terminals, providing continuous stimulation even in the context of discontinuous exogenous delivery (). However, with progressive loss of nigrostriatal terminals and accompanying changes in the central pharmacodynamics of LD, the clinical response to individual doses becomes progressively short-lived, resulting in wearing-off and “on-off ”-type motor fluctuations. These motor fluctuations can be completely abolished by continuous intravenous infusions of LD,Citation48 supporting the concept that providing a less pulsatile, more continuous, striatal dopamine receptor stimulation may be critical to restoring physiological motor processing in the striato-pallido-thalamo-cortical network in PD.Citation49–Citation53
Figure 4 The evolution of levodopa-associated motor fluctuations. A comparison of plasma levodopa levels, brain dopamine levels, and the resulting motor response in early and advanced stages of Parkinson’s disease is shown.
The issue of continuous drug delivery is also relevant to the current understanding of mechanisms underlying the development of LD-induced dyskinesia. In animal models of PD, administration of D1 or D2 agonists with short half-lives is associated with dyskinetic responses,Citation54–Citation57 while exposure to long-acting agonists does not induce dyskinesia.Citation58–Citation60 The same differences have also been observed in studies comparing pulsatile versus continuous delivery of the same dopaminergic agent.Citation61,Citation62 Such results are consistent with clinical studies of continuous infusions of DAs, such as apomorphineCitation63,Citation64 or lisuride,Citation65 which were found to downregulate pre-existing LD-induced dyskinesia. Indeed, when given as continuous intraduodenal infusions, marked reductions in dyskinesia have been reported for LD itselfCitation49,Citation53,Citation66,Citation67 and the gel preparation of LD (Duodopa®, Solvay Pharmaceuticals GmbH).Citation68,Citation69
Although pulsatile stimulation may not be sufficient to explain the mechanisms underlying the induction of dyskinesia completely, such observations highlight the need to optimize LD delivery in PD. The use of intravenous infusions is not feasible for chronic treatment, and intrajejunal infusion strategies are currently limited by high costs and the need for percutaneous gastrostomy. Other routes of LD delivery, eg, transdermal or transnasal, are currently under investigation but no nonenteral system has yet reached the market.Citation58–Citation60,Citation70,Citation71 Previous attempts to improve oral delivery have included the development of sustained-release preparations of LD, but unfortunately randomized controlled studies have failed to reveal any difference between such formulations and standard LD with respect to long-term dyskinesia risk.Citation72–Citation74 Sustained-release LD preparations exhibit erratic absorption patterns and unpredictable plasma levels,Citation67 resulting in dose failures as well as a delay in producing a clinical benefit.Citation75 As such, the unpredictable absorption of these agents may not abolish high peak and low trough LD plasma levels that are associated with the development of dyskinesia.
Likewise, controlled trials have not clearly established superiority of sustained-release LD in terms of control of motor fluctuations.Citation76 By contrast, prolonging the LD half-life via adjunctive treatment with a catechol-O-methyltransferase inhibitor, such as entacapone or tolcapone, has been found to be efficacious in reducing daily “off ” time in a number of well-performed, randomized, controlled trials in PD patients with wearing-off.Citation77–Citation80
The established efficacy of entacapone in PD patients with wearing-off has raised the possibility that it may also be effective in reducing the risk of dyskinesias. However, results of the recent STRIDE-PD trial demonstrated that, in patients with early PD who are not experiencing wearing-off, a four times daily dose of a LD formulation comprising LD, carbidopa, and entacapone is not superior to conventional LD in delaying dyskinesias.Citation22 The study investigators have proposed that entacapone may not have been administered frequently enough to achieve smooth levels of LD in the plasma.Citation22
As such, current research is focusing on the development of new LD formulations and delivery systems, such as novel controlled-release and transdermal preparations, which may improve delivery of LD in order to achieve smoother LD plasma levels. It remains to be seen whether these new LD formulations will prove effective in minimizing the risk of drug-induced motor complications.
Conclusions
Despite all recent advances in the medical management of PD, LD has remained the therapeutic gold standard in controlling the cardinal motor features of this illness. There is no evidence to support withholding LD for fear of hastening the progression of PD, although current three times daily regimens of standard oral LD carry a definite risk of inducing potentially disabling drug-induced involuntary movements. While dyskinetic responses are common with sustained LD therapy, the proportion of patients actually developing disabling and severe dyskinesia has been below 10% in a recent four-year randomized trialCitation2 and below 20% in a 10-year follow-up series.Citation17 This should be taken into account when the physician discusses the potential use of LD with the patient, particularly in patients who require enhanced symptomatic control despite optimized treatment with DAs. Moreover, when making individual decisions on how to initiate dopaminergic treatment, the weighing of relative risks and benefits of starting with a DA or LD should not only consider dyskinesia risks but also risks for other side effects, including daytime somnolence, impulse-control disorders and, in the case of ergot-derived DAs, cardiac valvulopathy and other forms of potentially life-threatening fibrosis.Citation27 In addition, individual needs for magnitude and speed of symptomatic improvement must be balanced against potential side effects. For over 40 years, LD has remained the cornerstone of PD therapy. Future endeavors will focus on optimizing delivery of LD in order to expand and improve the treatment options of PD.
Acknowledgements
The idea for the present review was originally discussed and formulated at a meeting of the Neuronet PD group, which was funded by an unrestricted educational grant from Novartis Pharma AG. We would like to thank Sevasti Bostantjopou-lou, Luc Defebvre, Bulent Elibol, Joaquim Ferreira, Spiros Konitstotis, Jaime Kulisevsky, Rosario Luquin, Johannes Van Hilten, and Marc Verin for their helpful comments. Editorial support for this manuscript was provided by Medicus International and funded by Novartis Pharma AG.
Disclosure
All authors are part of the Novartis-funded Neuronet PD group. WP has received consultancy and lecture fees from AstraZeneca, Teva, Novartis, GSK, Boehringer-Ingelheim, UCB, Orion Pharma and Merck Serono in relation to clinical drug development programs for PD. PRB has received a research grant from Novartis Pharma AG.
References
- OlanowCWAgidYMizunoYLevodopa in the treatment of Parkinson’s disease: Current controversiesMov Disord200419999715372588
- HollowayRGShoulsonIFahnSPramipexole vs levodopa as initial treatment for Parkinson disease: A 4-year randomized controlled trialArch Neurol20046171044105315262734
- RascolOBrooksDJKorczynADA five-year study of the incidence of dyskinesia in patients with early Parkinson’s disease who were treated with ropinirole or levodopa. 056 Study GroupN Engl J Med2000342201484149110816186
- RinneUKBraccoFChouzaCEarly treatment of Parkinson’s disease with cabergoline delays the onset of motor complications. Results of a double-blind levodopa controlled trial. The PKDS009 Study GroupDrugs199855Suppl 123309483167
- OertelWHWoltersESampaioCPergolide versus levodopa monotherapy in early Parkinson’s disease patients: The PELMOPET studyMov Disord200521334335316211594
- ClarkeCEDaviesPSystematic review of acute levodopa and apomorphine challenge tests in the diagnosis of idiopathic Parkinson’s diseaseJ Neurol Neurosurg Psychiatry200069559059411032609
- GoetzCGPoeweWRascolOMovement Disorder Society Task Force report on the Hoehn and Yahr staging scale: Status and recommendationsMov Disord20041991020102815372591
- RajputAHLevodopa prolongs life expectancy and is non-toxic to substantia nigraParkinsonism Relat Disord2001829510011489674
- HoehnMMThe natural history of Parkinson’s disease in the pre-levodopa and post-levodopa erasNeurol Clin19921023313391584177
- NuttJGWootenGFClinical practice. Diagnosis and initial management of Parkinson’s diseaseN Engl J Med2005353101021102716148287
- Parkinson Study GroupPramipexole vs levodopa as initial treatment for Parkinson disease: A randomised controlled trialJAMA2000284151931193811035889
- KurlanR“Levodopa phobia”: A new iatrogenic cause of disability in Parkinson diseaseNeurology200564592392415753443
- JennerPPathophysiology and biochemistry of dyskinesia: Clues for the development of non-dopaminergic treatmentsJ Neurol2000247Suppl 2II43II5010991665
- WhoneALWattsRLStoesslAJSlower progression of Parkinson’s disease with ropinirole versus levodopa: The REAL-PET studyAnn Neurol20035419310112838524
- RascolOBrooksDJKorczynADDevelopment of dyskinesias in a 5-year trial of ropinirole and L-dopaMov Disord200621111844185016958094
- Parkinson Study GroupLong-term effect of initiating pramipexole vs levodopa in early Parkinson diseaseArch Neurol200966556357019433655
- LeesAJKatzenschlagerRHeadJBen-ShlomoYTen-year follow-up of three different initial treatments in de-novo PD: A randomized trialNeurology20015791687169411706112
- HauserRARascolOKorczynADTen-year follow-up of Parkinson’s disease patients randomized to initial therapy with ropinirole or levodopaMov Disord200722162409241717894339
- RascolOKorczynADe DeynPPLangAIncidence of dyskinesias in a 10-year naturalistic follow-up of patients with early Parkinson’s disease (PD) initially receiving ropinirole compared with L-dopaMov Disord200520Suppl 10S63
- HauserRAFriedlanderJZesiewiczTAA home diary to assess functional status in patients with Parkinson’s disease with motor fluctuations and dyskinesiaClin Neuropharmacol2000232758110803796
- KatzenschlagerRHeadJSchragAFourteen-year final report of the randomized PDRG-UK trial comparing three initial treatments in PDNeurology200871747448018579806
- StocchiFRascolOKieburtzKInitiating levodopa/carbidopa therapy with and without entacapone in early Parkinson disease: the STRIDE-PD studyAnn Neurol2010681182720582993
- HungSAdeliGArenovichTFoxSLangAPatient perception of dyskinesias in Parkinson’s diseaseNeurology2007686A232
- LarsenJPWorm-PetersenJSidenAThe tolerability and efficacy of entacapone over 3 years in patients with Parkinson’s diseaseEur J Neurol200310213714612603288
- OlanowCWSternMBSethiKThe scientific and clinical basis for the treatment of Parkinson disease (2009)Neurology20097221 Suppl 4S1S13619470958
- ObesoJAOlanowCWNuttJGLevodopa motor complications in Parkinson’s diseaseTrends Neurosci200023Suppl 10S2S711052214
- AntoniniATolosaEMizunoYYamamotoMPoeweWHA reassessment of risks and benefits of dopamine agonists in Parkinson’s diseaseLancet Neurol200981092993719709931
- WeintraubDDopamine and impulse control disorders in Parkinson’s diseaseAnn Neurol200864Suppl 2S93S10019127573
- VoonVHassanKZurowskiMProspective prevalence of pathologic gambling and medication association in Parkinson diseaseNeurology200666111750175216769956
- MichelPPHeftiFToxicity of 6-hydroxydopamine and dopamine for dopaminergic neurons in cultureJ Neurosci Res19902644284351977925
- SpencerJPJennerAAruomaOIIntense oxidative DNA damage promoted by L-dopa and its metabolites. Implications for neurodegenerative diseaseFEBS Lett199435332462507957867
- MenaMAPardoBCasarejosMJFahnSGarcia de YebenesJNeurotoxicity of levodopa on catecholamine-rich neuronsMov Disord19927123311557063
- FahnSIs levodopa toxic?Neurology199647Suppl 3S184S1958959987
- MenaMACasarejosMJCarazoAPainoCLGarcia de YebenesJGlia conditioned medium protects fetal rat midbrain neurones in culture from L-DOPA toxicityNeuroreport1996724414458730801
- MenaMACasarejosMJCarazoAPainoCLGarcia de YebenesJGlia protect fetal midbrain dopamine neurons in culture from L-DOPA toxicity through multiple mechanismsJ Neural Transm19971044–53173289295168
- PardoBMenaMAFahnSGarcia de YebenesJAscorbic acid protects against levodopa-induced neurotoxicity on a catecholamine-rich human neuroblastoma cell lineMov Disord1993832782848341291
- MenaMAPardoBPainoCLDe YebenesJGLevodopa toxicity in foetal rat midbrain neurones in culture: Modulation by ascorbic acidNeuroreport1993444384408499605
- AgidYLevodopa: Is toxicity a myth?Neurology19985048588639566363
- PerryTLYongVWItoMNigrostriatal dopaminergic neurons remain undamaged in rats given high doses of L-DOPA and carbidopa chronicallyJ Neurochem19844349909936147392
- PearceRKHeikkilaMLindenIBJennerPL-dopa induces dyskinesia in normal monkeys: Behavioural and pharmacokinetic observationsPsychopharmacology (Berl)2001156440240911498717
- RajputAHFentonMBirdiSMacaulayRIs levodopa toxic to human substantia nigra?Mov Disord19971256346389380042
- MurerMGDziewczapolskiGMenalledLBChronic levodopa is not toxic for remaining dopamine neurons, but instead promotes their recovery, in rats with moderate nigrostriatal lesionsAnn Neurol19984355615759585350
- DatlaKPBluntSBDexterDTChronic L-DOPA administration is not toxic to the remaining dopaminergic nigrostriatal neurons, but instead may promote their functional recovery, in rats with partial 6-OHDA or FeCl(3) nigrostriatal lesionsMov Disord20011634243411391735
- HagenahJKleinCSiebererMViereggePExogenous levodopa is not toxic to elderly subjects with non-parkinsonian movement disorders: Further clinical evidenceJ Neural Transm19991063–430130710392538
- FahnSOakesDShoulsonILevodopa and the progression of Parkinson’s diseaseN Engl J Med2004351242498250815590952
- MiyasakiJMMartinWSuchowerskyOWeinerWJLangAEPractice parameter: Initiation of treatment for Parkinson’s disease: An evidence-based review: Report of the Quality Standards Subcommittee of the American Academy of NeurologyNeurology2002581111711781398
- PoeweWWenningGLevodopa in Parkinson’s disease: Mechanisms of action and pathophysiology of late failureJankovicJTolosaEParkinson’s Disease and Movement Disorders4th edPhiladelphia, PALippincott Williams and Wilkins2002
- StocchiFVaccaLRuggieriSOlanowCWIntermittent vs continuous levodopa administration in patients with advanced Parkinson disease: A clinical and pharmacokinetic studyArch Neurol200562690591015956161
- AntoniniAIsaiasIUCanesiMDuodenal levodopa infusion for advanced Parkinson’s disease: 12-month treatment outcomeMov Disord20072281145114917661426
- ObesoJARodriguez-OrozMCChanaPThe evolution and origin of motor complications in Parkinson’s diseaseNeurology20005511 Suppl 4S13S2011147505
- ObesoJARodriguez-OrozMMarinCThe origin of motor fluctuations in Parkinson’s disease: Importance of dopaminergic innervation and basal ganglia circuitsNeurology2004621 Suppl 1S17S3014718677
- OlanowWSchapiraAHRascolOContinuous dopamine-receptor stimulation in early Parkinson’s diseaseTrend Neurosci200023Suppl 10S117S12611052229
- StocchiFThe levodopa wearing-off phenomenon in Parkinson’s disease: Pharmacokinetic considerationsExpert Opin Pharmacother20067101399140716805724
- MaratosECJacksonMJPearceRKCannizzaroCJennerPBoth short- and long-acting D-1/D-2 dopamine agonists induce less dyskinesia than L-DOPA in the MPTP-lesioned common marmoset (Callithrix jacchus)Exp Neurol200317919010212504871
- GagnonCBedardPJDi PaoloTEffect of chronic treatment of MPTP monkeys with dopamine D-1 and/or D-2 receptor agonistsEur J Pharmacol199017811151201970537
- Gomez-MancillaBBedardPJEffect of chronic treatment with (+)-PHNO, a D2 agonist in MPTP-treated monkeysExp Neurol199211721851881354166
- LuquinMRLagunaJHerreroMTObesoJABehavioral tolerance to repeated apomorphine administration in parkinsonian monkeysJ Neurol Sci1993114140448094427
- BedardPJDi PaoloTFalardeauPBoucherRChronic treatment with L-DOPA, but not bromocriptine induces dyskinesia in MPTP-parkinsonian monkeys. Correlation with [3H]spiperone bindingBrain Res198637922942993488796
- MaratosECJacksonMJPearceRKJennerPAntiparkinsonian activity and dyskinesia risk of ropinirole and L-DOPA combination therapy in drug naive MPTP-lesioned common marmosets (Callithrix jacchus)Mov Disord200116463164111481686
- Hadj TaharAGregoireLBangassoroEBedardPJSustained cabergoline treatment reverses levodopa-induced dyskinesias in parkinsonian monkeysClin Neuropharmacol200023419520211020123
- BlanchetPJCalonFMartelJCContinuous administration decreases and pulsatile administration increases behavioral sensitivity to a novel dopamine D2 agonist (U-91356A) in MPTP-exposed monkeysJ Pharmacol Exp Ther199527228548597853204
- MorissetteMGouletMSoghomonianJJPreproenkephalin mRNA expression in the caudate-putamen of MPTP monkeys after chronic treatment with the D2 agonist U91356A in continuous or intermittent mode of administration: Comparison with L-DOPA therapyBrain Res Mol Brain Res1997491–255629387863
- KatzenschlagerRHughesAEvansAContinuous subcutaneous apomorphine therapy improves dyskinesias in Parkinson’s disease: A prospective study using single-dose challengesMov Disord200520215115715390035
- ColziATurnerKLeesAJContinuous subcutaneous waking day apomorphine in the long term treatment of levodopa induced interdose dyskinesias in Parkinson’s diseaseJ Neurol Neurosurg Psychiatry19986455735769598668
- StocchiFRuggieriSVaccaLOlanowCWProspective randomized trial of lisuride infusion versus oral levodopa in patients with Parkinson’s diseaseBrain2002125Pt 92058206612183351
- SyedNMurphyJZimmermanTJrMarkMHSageJITen years’ experience with enteral levodopa infusions for motor fluctuations in Parkinson’s diseaseMov Disord19981323363389539350
- NyholmDAskmarkHGomes-TrolinCOptimizing levodopa pharmacokinetics: Intestinal infusion versus oral sustained-release tabletsClin Neuropharmacol200326315616312782919
- DevosDPatient profile, indications, efficacy and safety of duodenal levodopa infusion in advanced Parkinson’s diseaseMov Disord2009247993100019253412
- AnnicADevosDSeguyD[Continuous dopaminergic stimulation by Duodopa in advanced Parkinson’s disease: Efficacy and safety]Rev Neurol (Paris)20091658–971827 French.19150100
- BrimeBBallesterosMPFrutosPPreparation and in vitro characterization of gelatin microspheres containing Levodopa for nasal administrationJ Microencapsul200017677778411063424
- BabitaKTiwaryAKTranscutaneous delivery of levodopa: Enhancement by fatty acid synthesis inhibitionMol Pharm200521576315804178
- DupontEAndersenABoasJSustained-release Madopar HBS compared with standard Madopar in the long-term treatment of de novo parkinsonian patientsActa Neurol Scand199693114208825266
- BlockGLissCReinesSIrrJNibbelinkDComparison of immediate-release and controlled release carbidopa/levodopa in Parkinson’s disease. A multicenter 5-year study. The CR First Study GroupEur Neurol199737123279018028
- KollerWCHuttonJTTolosaECapilldeoRImmediate-release and controlled-release carbidopa/levodopa in PD: A 5-year randomized multicenter study. Carbidopa/Levodopa Study GroupNeurology19995351012101910496260
- BrooksDJOptimizing levodopa therapy for Parkinson’s disease with levodopa/carbidopa/entacapone: Implications from a clinical and patient perspectiveNeuropsychiatr Dis Treat200841394718728816
- RascolOGoetzCKollerWPoeweWSampaioCTreatment interventions for Parkinson’s disease: An evidence based assessmentLancet200235993171589159812047983
- RinneUKLarsenJPSidenAWorm-PetersenJEntacapone enhances the response to levodopa in parkinsonian patients with motor fluctuations. NOMECOMT Study GroupNeurology1998515130913149818851
- BrooksDJSagarHEntacapone is beneficial in both fluctuating and non-fluctuating patients with Parkinson’s disease: A randomised, placebo controlled, double blind, six month studyJ Neurol Neurosurg Psychiatry20037481071107912876237
- PoeweWHDeuschlGGordinAKultalahtiERLeinonenMEfficacy and safety of entacapone in Parkinson’s disease patients with suboptimal levodopa response: A 6-month randomized placebo-controlled double-blind study in Germany and Austria (Celomen study)Acta Neurologica Scand20021054245255
- Parkinson Study GroupEntacapone improves motor fluctuations in levodopa-treated Parkinson’s disease patientsAnn Neurol19974257477559392574