Abstract
Changes in the lamina dura are associated with dental diseases around the root of the tooth and with systemic diseases; however, the lamina dura below the crown of horizontal, incompletely impacted third molars has not been studied. Using orthopantomography, we studied the age of subjects with and without the lamina dura in 419 subjects. The participants were between the ages of 21 and 89 years. Mean age in men with the lamina dura was 30.29 ± 9.92 and without the lamina dura was 47.64 ± 16.32 (P < 0.0001), and in women with a lamina dura it was 29.65 ± 8.19 and without a lamina dura 41.97 ± 11.07 (P < 0.0001). To study the effect of aging, the relationship between the lamina dura and dental status was assessed in subjects over the age of 31 years. Alveolar bone resorption in the canine and the first molar of the ipsilateral mandible in subjects without the lamina dura was not significantly higher than in those with the lamina dura. There were no significant differences in the number of teeth lost, except in men, the number of treated teeth and the number of decayed teeth differed between groups. Disruption of the lamina dura was related to age, but with no alveolar bone resorption in the mandible.
Introduction
The lamina dura surrounds the tooth during development with an egg-shell like effect.Citation1 After eruption, the lamina dura is observed as a thin radiopaque layer of dense bone around sound teeth in a normal dental arch, and is continuous with the shadow of the cortical bone at the alveolar crest.Citation1 The lamina dura is influenced by heavy occlusion,Citation1 dental diseases, and the presence of a radiographic crestal lamina dura is positively associated with clinical periodontal stability.Citation2 The lamina dura is affected not only by odontogenic infections but also systemic diseases such as hyperparathyroidism,Citation1,Citation3 renal osteodystrophy,Citation1,Citation4 hypophosphatasia,Citation1 and hypophosphatemia,Citation1 thus, the lamina dura could be valuable for diagnosis. Clinically, identification of a lamina dura is frequently difficult because small variations and disruptions in the continuity of the lamina dura may result from superimpositions of cancellous bone and small nutrient canals passing from the marrow spaces to the periodontal ligament.Citation1 Changes in the lamina dura from a normal to distorted status often can not be distinguished due to the subtle line, suggesting the necessity of other signs and symptoms for diagnosis. Previously, we have studied inflammation and radiolucency below the crown of horizontal incompletely impacted third molars.Citation5–Citation8 The radiolucency lamina dura below the crown, which is the shadow of cortical bone, was seen to be thick in the young, but not prevalent in the elderly. However, with regard to the relationship between the lamina dura and age few reports have been seen, except to give the prognosis for autotransplantation of maxillary canines, in which the frequency of the lamina dura was poor in patients aged over 20 years,Citation9 and alveolar bone loss with loss of lamina dura in the deciduous teeth.Citation10–Citation12 A description of the relationship between the presence of lamina dura in the permanent teeth and age has not yet been demonstrated.
However, the relationship between alveolar bone resorption and aging is seen in animals.Citation13–Citation16 In humans age-related alveolar bone loss has also been reported.Citation17–Citation23 The rate of bone loss increases between the ages of 33 and 57–68 yearsCitation17 and between 65 and 75 years,Citation20 in the incisors,Citation18 in subjects with chronic obstructive pulmonary disease,Citation21 and with systemic changes,Citation23 although age-related alterations in the periodontium may not inevitably be manifested with the loss of alveolar bone.Citation24
We hypothesized that such a decline of the lamina dura correlates with age after eruption through hard cortical bone covering the mandibular third molar. We therefore performed a cross-sectional study to show a relationship between loss of the lamina dura below the crown and age including marginal bone levels and the dental status using a panoramic radiograph in subjects with a mandibular horizontal incompletely impacted third molar, and report an unexpected disruption of the lamina dura with age.
Methods
Orthopantomographs were examined in 295 teeth from 251 men and 197 teeth from 168 women who had horizontal incompletely impacted third molars at the initial examination for diagnosis and treatment. These examinations took place between January 1984 and December 1995 at Matsumoto Dental University Hospital, Oral and Maxillofacial Surgery (). The mean age ± standard deviation (SD) of 251 men was 39.81 ± 14.46 (range, 21–89), and that of 168 women was 32.47 ± 10.93 (range, 21–75). Horizontal incompletely impacted third molars, in which the crown is partly at the level of the alveolar bone ridge, were monitored regarding the lamina dura below the crown of the tooth to the cementoenamel junction. The status of a horizontal incompletely impacted third molar was confirmed with orthopantomographs taken with a Panoramax Auto 20 mA, 80–84 kVp (Asahi, Kyoto, Japan) and the films were processed in an automatic developing machine (Konica SRX-501; Konica, Tokyo, Japan). Incompletely impacted third molars were horizontal to the second molar in angulation and were not fully covered with bone. Horizontal angulation was measured using horizontal lines drawn at various heights at the occlusal plane of the second molarCitation25 or the first molar when the second molar was lost, or the premolar when the second and first molars were lost. The inclination of the occlusal plane of the third molar was read from the line using a compass. Teeth with inclinations of 70° or greater were selected as horizontal angulation following Shiller guidelines.Citation25 Radiograms were measured twice by the same experienced oral surgeon. The second measurement was performed after a period of months without viewing the primary data. Teeth with an inclination of 69° or smaller on either measurement were excluded from the study. Teeth were classified into two groups based on the presence/absence of the lamina dura below the crown of the horizontal incompletely impacted third molar, and analyzed by comparing these groups. Lamina dura was assessed by visual observation at 2× magnification. The presence of the lamina dura below the crown was defined by a fully or partly uniform line as still present, even if the line was partly irregularly ruptured (). Absence of the lamina dura was defined as no detection of a white line below the crown ( and ). The degree of bone resorption at the mesial surface of the canine and the first molar was assessed for aging or periodontal disease. Exposure of the root surface of the teeth was measured from the cementoenamel junction to the alveolar crest at the mesial site of the teeth, and exposure of the root surface was calculated as a fraction of the root length as determined radiographically. The mean ± SD rate of bone resorption between the first and second measurements in the canine and first molar was calculated, and the mean ± SD in those teeth in relation to the ipsilateral third molar, and was grouped into two categories with or without the lamina dura below the crown of the third molar. Imperfect views of the root because of imbrication of individual roots due to curvature of the dental arch were excluded from the assessment. When the assessment of the presence or absence of a lamina dura was found to be different between the first and second measurements, these participants were also excluded from the study. Patients with an apical lesion at the root of the mandibular second or third molar, a radiographically true cyst or tumor in the mandible, diffuse radiolucency below the crown, a completely impacted third molar, vertical impaction, or distoangular impaction, and a restoration ending below the cementoenamel junction of the second molar were excluded from analysis.
Table 1 No. of teeth with and without lamina dura
Figure 1 Bilateral horizontal incompletely impacted third molars with lamina dura below the crown in a 36-year-old man.
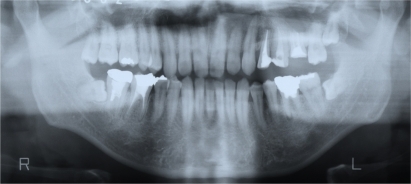
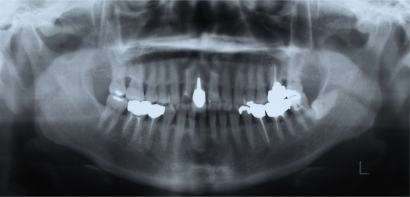
Figure 2 Right horizontal incompletely impacted third molar without lamina dura below the crown in a 39-year-old woman.

Figure 3 Left horizontal incompletely impacted third molar without lamina dura below the crown in a 53-year-old woman.
Statistical analysis
Rates of teeth with or without a lamina dura and the ages of patients were calculated and analyzed statistically using Fisher’s exact test or χ2 analysis, and Student’s t-test among these groups.
Results
Two hundred and thirty teeth in men and 168 teeth in women with a lamina dura and 65 teeth in men and 29 teeth in women without a lamina dura were seen in subjects with a mandibular horizontal incompletely impacted third molar (). Subjects with a lamina dura were significantly younger than those without (mean ± SD: 30.29 ± 9.92 vs 47.14 ± 16.32 in men, P < 0.0001, mean ± SD: 29.65 ± 8.19 vs 41.97 ± 11.07 in women, P < 0.0001). The participants were classified into four age groups, and we observed a significant prevalence in the younger age group (21 to 30 years) than in the older age groups of both men and women with a lamina dura, whereas subjects without a lamina dura increased with age. To study the effect of aging on the dental status, subjects over the age of 31 years were assessed and reviewed (). The number of teeth in men with a lamina dura was 72, and without a lamina dura was 55. The number of teeth in women with a lamina dura was 53 and without a lamina dura was 24. Men over the age of 31 years with a lamina dura were significantly younger than those without a lamina dura (mean ± SD: 42.03 ± 9.96 vs. 51.14 ± 14.35, P < 0.001). Women with a lamina dura were also significantly younger than those without a lamina dura (mean ± SD: 38.72 ± 7.85 vs 44.88 ± 9.83, P < 0.001). Alveolar bone resorption in the canine and first molar region could be assessed in 62 teeth with a lamina dura and 42 without a lamina dura in men, and 48 teeth with a lamina dura and 22 without a lamina dura in women. Alveolar bone resorption in the canine and first molar regions in subjects without a lamina dura was not significantly higher than in those with a lamina dura (0.07 ± 0.09 vs 0.09 ± 0.15, P = 0.60 in men, 0.02 ± 0.06 vs 0.05 ± 0.09, P = 0.13 in women). For other measures of tooth loss, the number of teeth treated with metal repair and the number of decayed teeth in the ipsilateral mandible, indicated no significant associations between subjects with and without a lamina dura below the crown except for the number of teeth lost in men (P < 0.05).
Table 2 Lamina dura and status of bone and teeth on ipsilateral side in subjects older than 31 years
Discussion
In this study, we found that disruption of the lamina dura below the crown of a mandibular horizontal incompletely impacted third molar is associated with age in both genders, but independently of the mean value of alveolar bone resorption in the canine and first molar region and other status of teeth in the ipsilateral mandible except for the number of teeth lost in men. Increased tooth loss in men may be related to variables of poor oral health, smoking or systemic risk factors; however the risk factors were difficult to determine in this study. It is necessary to consider the possible effect of aging. Demonstration of a lamina dura below the crown of the third molar before eruption affects age-related decline, although that was not in parallel with alveolar bone resorption in the canine and first molar regions, suggesting an effect of aging. However, a parallel relationship between them may be limited to a small group of the elderly since a few elderly people had severe alveolar bone resorption. Age-related alveolar bone loss is shown,Citation17–Citation23 but disruption of the lamina dura was independent of the alveolar bone resorption in the canine and first molar. Moreover, decline in the presence of a lamina dura may be caused by atrophy since the lamina dura seemed to be fully developed from the tooth bud to eruption, and disruption of the lamina dura began around 20 years of age. These stages could increase gradually with age, because erupted force could possibly decrease with the age of onset of complete formation of the root in the third molar, and incomplete impaction might be not affected by occlusal force, resulting in a direct reflection of accelerated decline of the lamina dura as a physical reaction. On the other hand, the lamina dura below the crown is likely to be indispensable for maintaining the cortical bone in the mandible to prevent stimuli from the outside and/or inside of the cortical bone. Disruption of the lamina dura could be influenced by pathogenic events, especially chronic and/or acute pericoronitis, which could increase with age, although disruption of the lamina dura may affect biological defense due to chronic inflammation. To study the risk factors affecting the lamina dura, circumstances such as alveolar bone resorption and oral hygiene were analyzed in subjects over the age of 31 years. However, with an exception for men, the number of treated teeth and the number of decayed teeth we found no correlation between disruption of the lamina dura and alveolar bone resorption in the canine and first molar regions, between disruption of the lamina dura and the number of teeth lost in our analysis. Thus, our findings show that age-related decline of the lamina dura is identified and is independent of alveolar bone resorption in both men and women. This might indicate that prediction of alveolar bone resorption is difficult to associate with disruption of the lamina dura because of slow alveolar bone loss progression, as noted by Hirschmann,Citation26 and various other factors.
The lamina dura below the crown of the mandibular horizontal incompletely impacted third molar does not contact with the cement but enamel at any degree. Therefore, the lamina dura below the crown could be independently controlled by the periodontium or cement, and could have common characteristics with the role of alveolar crestal cortical bone. GreensteinCitation27 noted that the crestal lamina dura on radiography does not appear to be related to the presence or absence of clinical inflammation, bleeding upon probing, periodontal pockets or loss of attachment. If the lamina dura below the crown is characteristically similar to that in the crestal cortical bone, disruption of the lamina dura below the crown could predict alveolar bone resorption, especially the early identification of bone loss, since both alterations may simply be related to aging. On the other hand, evaluation of the radiographic crestal lamina dura status appears valuable for assessing the risk of periodontitis disease activity at inter-proximal tooth sites;Citation2 however, it was impossible to demonstrate an evidence of chronic inflammation and presence of the lamina dura at the alveolar bone crest in this current study. Our study showed the frequency of the presence of the lamina dura because measuring the thickness of the lamina dura was almost impossible due to partial thinning or disruption, as noted by Cavalcanti.Citation28 This might show a limitation of panoramic radiography in dental diagnosis, and is the reason why a combination of panoramic and intraoral radiography is necessary, as noted by Molander.Citation29
The current study demonstrated that bone contacts the enamel without a lamina dura with aging. The lamina dura is wider and denser around the roots of teeth with heavy occlusion and thinner and less dense around teeth not subjected to occlusal functionCitation1 after formation of the lamina dura, which begins with the tooth germ. However, it is unclear whether the bone is hardened through reactions with the enamel in the young, and reduces sensitivity to the effect of enamel as environmental sensitivity. Recently, the coordination of bone resorption and bone formation with active TGF-β1 was shown.Citation30 New bone below the crown may be based on the perfect synchrony. We have previously observed a relationship between acute inflammation and radiolucency below the crown independently of the lamina dura;Citation5–Citation8 however, the present study focused only on the comparison between the presence or absence of the lamina dura, although radiolucency warrants caution in interpreting these results because of possible chronic inflammation. A relationship between radiolucency and the lamina dura in larger samples of subjects would be implicated in the pathogenesis of bone resorption.
Although changes of the lamina dura with aging have not been reported to date, we confirmed that disruption of the lamina dura increased with age associated independently with bone resorption in the canine and first molar, suggesting that the lamina dura below the crown could not be responsible for alveolar bone resorption of other teeth in the mandible. Elucidation of the lamina dura below the crown, which is not related with the status of cortical bone in other teeth, would not enable prediction of the prognosis of bone resorption with aging. Further study would be required for this analysis.
Disclosures
The authors report no conflicts of interest in this work.
References
- WhiteSCPharoahMJOral Radiology: Principles and interpretation6th edSt Louis, MOMosby Elsevier2009
- RamsTEListgartenMASlotsJUtility of radiographic crestal lamina dura for predicting periodontitis disease-activityJ Clin Periodontol19942195715767806671
- PadburyADJrTözümTFTabaMJrThe impact of primary hyperparathyroidism on the oral cavityJ Clin Endocrinol Metab20069193439344516822829
- MoriiHOkamotoTIbaKAge-related changes of renal osteodystrophyEndocrinol Jpn197926Suppl8184467353
- YamaokaMOnoYIshizukaMAcute inflammation at a mandibular solitary horizontal incompletely impacted molarInt J Gen Med200926772
- YamaokaMOnoYTakahashiMBone resorption in incompletely impacted mandibular third molars and acute pericoronitisClinical, Cosmetic and Investigational Dentistry20091712
- YamaokaMOnoYIshizukaMYasudaKUematsuTFurusawaKRadiolucency below the crown of mandibular horizontal incompletely impacted third molars and acute inflammation in men with diabetesClinical, Cosmetic and Investigational Dentistry200912734
- YamaokaMOnoYTakahashiMAcute inflammation in horizontal incompletely impacted third molar with radiolucency in the elderlyClin Interv Aging2009433734219696898
- AltonenMHaavikkoKMalmströmMEvaluation of autotransplantations of completely developed maxillary caninesInt J Oral Surg197875434441102598
- WolffAStarkHSarnatHBindermanIEisensteinBDrukkerAThe dental status of children with chronic renal failureInt J Pediatr Nephrol1985621271324030223
- BimsteinEGarcia-GodoyFThe significance of age, proximal caries, gingival inflammation, probing depths and the loss of lamina dura in the diagnosis of alveolar bone loss in the primary molarsASDC J Dent Child19946121251288046091
- DrummondBKBimsteinEPrevalence of marginal alveolar bone loss in children referred to treatment to the Paediatric Clinic at the School of Dentistry, University of OtagoN Z Dent J1995914061381408602288
- BarnettNARoweDJA comparison of alveolar bone in young and aged miceJ Periodontol19865774474523461153
- MorganJPMiyabayashiTAndersonJKlingeBPeriodontal bone loss in the aging beagle dog. A radiographic studyJ Clin Periodontol19901796306352250077
- KingGJLattaLRutenbergJOssiAKeelingSDAlveolar bone turnover in male rats: site-and age-specific changesAnat Rec199524233213287573979
- RivaldoEGPadlihaDPHugoFNAlveolar bone loss and aging: a model for the study in miceJ Periodontol200576111966197116274317
- AlbandarJMRiseJGjermoPJohansenJRRadiographic quantification of alveolar bone level changes. A 2-year longitudinal study in manJ Clin Periodontol19861331952003457808
- PapapanouPNWennströmJLGröndahlKPeriodontal status in relation to age and tooth type. A cross-sectional radiographic studyJ Clin Periodontol19881574694783263400
- JeffcoatMKChesnutCH3rdSystematic osteoporosis and oral bone loss: evidence shows increased risk factorsJ Am Dent Assoc19931241149568227773
- WheelerTTMcArthurWPMagnussonIModeling the relationship between clinical microbiologic, and immunologic parameters and alveolar bone levels in the elderly populationJ Periodontol199465168788133417
- HayesCSparrowDCohenMVokonasPSGarciaRIThe association between alveolar bone loss and pulmonary function: the VA Dental Longitudinal StudyAnn Periodontol1998312572619722709
- StreckfusCFParsellDEStrechfusJEPenningtonWJohnsonRBRelationship between oral alveolar bone loss and aging among African-American and Caucasian individualsGerontology19994521101149933734
- PilgramTKHildeboltCFYokoyama-CrothersNRelationships between longitudinal changes in radiographic alveolar bone height and probing depth measurements: data from postmenopausal womenJ Periodontol199970882983310476888
- PapapanouPNIndheJSterrettJDEnerothLConsiderations on the contribution of aging to loss of periodontal tissue supportJ Clin Periodontol19911886116151795058
- ShillerWRPosition changes in mesioangular impacted third molars during a yearJ Am Dent Assoc1979993460464288779
- HirschmannPNRadiographic interpretation of chronic periodontitisInt Dent J1987371393294597
- GreensteinGPoisonAIkerHMeltnerSAssociation between crestal lamina dura and periodontal statusJ Periodontol19815273623666942152
- CavalcantiMGRuprechtAJohnsonWTSouthardTEJakobsenJThe contribution of trabecular bone to the visibility of the lamina dura: and in vitro radiographic studyOral Surg Oral Med Oral Pathol Oral Radiol Endod200293111812211805787
- MolanderBPanoramic radiography in dental diagnosisSwed Dent J Suppl19961191268971997
- TangYWuXLeiWTGF-β1-induced migration of bone mesenchymal stem cells couples bone resorption with formationNat Med200915775776519584867