Abstract
Dietary supplements at high doses as part of medical therapy have been controversial, but the evidence suggests that they play a significant role in prevention and treatment of diseases as well as protection from accelerated aging that results from oxygen free-radical damage, inflammation, and glycation. This literature review examines several supplements that have documented roles in medical therapy, including vitamins C and E, coenzyme Q10, alpha-lipoic acid, chromium, L-carnitine, and quercetin. The evidence shows benefits in diabetes, cardiovascular disease, hypertension, congestive heart failure, age-related deterioration of brain function and vision, and immune function, as well as other age-related health problems.
Introduction
Dietary supplements, including vitamins, minerals, essential fatty acids, amino acids, flavonoids, herbs, and accessory food factors, are among the most valuable and safe substances for prevention and treatment of serious chronic and acute diseases associated with mortality, as well as everyday health problems that cause discomfort and disability. It is important to take adequate doses for their full benefits. Because they prevent deficiency diseases at low doses, they have acquired a reputation for being necessary only at these low levels. As a result, many physicians ignore the value of much higher doses that are useful for therapeutic purposes and protection from age-related degeneration.
Small amounts of essential nutrients treat deficiency diseases, but these conditions (scurvy, beri beri, pellagra, and rickets, for examples) are rarely seen in developed countries. Marginal nutrition associated with marginal health is much more likely to be the problem. For the most benefit from dietary supplements, it is important to ignore the RDA (recommended dietary allowances) levels that are found in food and most common dietary supplements and focus on the research that shows the benefits of appropriate doses, which are often much higher than the RDA.
Nutrients that are not essential but valuable as supplements include coenzyme Q10, alpha lipoic acid, GLA (gamma-linolenic acid), some non-essential amino acids, such as L-arginine, L-carnitine, and L-glutamine, and others. Additional valuable supplements, including flavonoids and other antioxidants, are found in foods but are not associated with specific deficiency diseases, although they provide specific health benefits in appropriate doses. People benefit from dietary supplements because of genetic physiological and biochemical variation, exposure to environmental contaminants, free radical damage from normal metabolism, exposure to ultraviolet light or ozone, and specific medical conditions. The process of aging leads to biochemical and physiological changes that can be slowed down and sometimes reversed through the appropriate use of dietary supplements.
Orthomolecular medicine
Orthomolecular medicine is the restoration and maintenance of health through the administration of adequate amounts of substances that are normally present in the body. Nobel Prize winner Linus Pauling, one of the leading molecular chemists of the century, established this definition of orthomolecular medicine in 1968. The aging process is typically accelerated as a result of free radical exposure, frequent or chronic inflammation, and toxic exposures (such as to heavy metals or industrial and agricultural hydrocarbons). Reversing this process or slowing it down is one goal of orthomolecular therapy, along with treatment of health problems.
An increasing number of scientific studies have been confirming the view that high doses of nutrients are therapeutic and preventive. Vitamins C and E, beta-carotene, B-complex vitamins, and coenzyme Q10 are among the many nutrients that have been shown to contribute positively to health and longevity at doses much higher than the RDA. While therapeutic levels for minerals, such as magnesium, zinc, and chromium, are much closer to the RDA, supplements beyond what is normally present in foods may still be essential for prevention and treatment of disease and slowing the aging process.
Supplements for anti-aging, prevention, and medical therapy
Vitamin C
Vitamin C has a wide range of metabolic functions. It offers protection from oxidative free-radical damage and it is essential for the production of collagen. Vitamin C reduces the wrinkling and sagging of the skin that occurs with aging. Vitamin C also helps maintain mucous membranes, adrenal hormone production, and immune function, including humoral immunity, and phagocytosis.
While the US RDA for vitamin C was recently raised (for men from 60 mg to its current 90 mg, and for women from 45 mg to 75 mg, and somewhat more for smokers), even higher doses have greater health benefits. For example, in a placebo controlled trial for six months, 40 men and women between 60 to 80 years old were administered 500 mg of vitamin C daily. This moderate dose of vitamin C modestly but significantly lowered blood pressure (CitationFotherby et al 2000). In another study of 514 people, plasma vitamin C levels were inversely related to blood pressure and pulse rate (CitationBates et al 1998). Elevated blood pressure is a risk factor for age-related atherosclerotic disease.
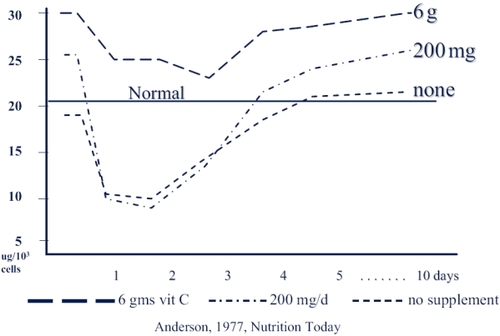
Early research showed a significant difference in leukocyte vitamin C during a viral infection depending on the level of supplementation (Figure ). At the start of an infection, vitamin C levels in leukocytes drops precipitously. With supplements of 200 mg, the initial level is higher, but it also drops quickly to about the same level as with no supplementation. With supplements of 6000 mg, the level starts much higher and stays above what is considered a normal baseline for the duration of the infection, and symptoms improve more quickly (CitationAnderson 1979).
Figure 1 Leukocyte vitamin C during infections. High dose vitamin C (6 g daily before and during infection) enhances leukocyte ascorbate levels at baseline and during infections. Low dose supplements (200 mg daily) have less pronounced effects.
A 1979 study showed immune system benefit from daily administration of 1g of vitamin C. Two children with autosomal recessive genetic chronic granulomatous disease were given this dose, prior to which they had recurrent infections, abnormal neutrophil function, and elevated serum IgE levels. They became free of recurrent infections and gained weight with this dose. Their neutrophil motility and phagocytosis improved while their serum immunoglobulin E (IgE) levels dropped (CitationAnderson and Dittrich 1979). Also in 1979, 10 patients with recurrent bacterial infections were noted to have abnormal neutrophil motility. Six of the patients were administered oral vitamin C (1 g daily for children and 3 g daily for adults). Testing at monthly intervals showed consistent improvement in neutrophil motility and clinical improvement in 5 of the 6 patients (CitationAnderson and Theron 1979).
Another study in 1980 evaluated the effect of vitamin C at 1 g, 2 g, and 3 g doses showed that neutrophil motility was enhanced with the higher doses, but not when the lower dose of 1 g was administered (CitationAnderson et al 1980). More recently, a Japanese study of vitamin C and upper respiratory infections showed that the frequency of colds could be reduced by a daily 500 mg supplement. In this research, 244 subjects completed a protocol in which they were assigned to a daily dose of either 50 mg or 500 mg of vitamin C. The frequency of colds was much less in the high-dose group. Those taking the 500 mg dose had a 66% lower relative risk of catching a common cold (CitationSasazuki et al 2006).
Age-related macular degeneration (AMD) is another disorder that is influenced by vitamin C and other nutrients. In the Age-Related Eye Disease Study (AREDS) subjects were administered a mixture of antioxidants and zinc, including 500 mg of vitamin C. In this multi-center trial, 3640 subjects at various stages of AMD were randomly assigned to the treatment group or placebo, and were followed for an average of 6.3 years. The supplements reduced the risk of developing advanced AMD by 28%, and the higher-risk subjects did even better (CitationAREDS 2001).
Overall, research suggests that vitamin C provides a wide variety of benefits in daily doses from 500 mg to 6000 mg, and higher doses may be of value in some conditions. Many of these benefits would be of particular value to the elderly, with compromised immunity, degenerative heart and brain disorders, as well as cancer and inflammatory processes. I typically recommend 3000 mg to 6000 mg daily for many patients.
Vitamin E
Vitamin E refers to a family of substances including alpha-, beta-, gamma-, and delta-tocopherols. The primary one in most research is alpha-tocopherol, but some research suggests that gamma-tocopherol is also very important. These are all antioxidants, and have many anti-aging effects. Vitamin E protects low density lipoprotein-cholesterol (LDL-C) from oxidation, and numerous epidemiological studies have suggested that higher vitamin E intake is associated with reduced heart disease and cardiac deaths (CitationKnekt et al 1994). Elderly people with higher vitamin E blood levels are less likely to have signs of vascular aging and have reduced levels of LDL oxidation (CitationCherubini et al 2001). More recent intervention studies have not shown the same benefits in patients who already have heart disease, possibly because many of the studies used only pure alpha-tocopherol, and most of them used synthetic vitamin E (dl-alpha-tocopherol), not the natural d-alpha-tocopherol, which is more active.
Vitamin E can also enhance immune function. Supplements of 200 IU to 800 IU are associated with reduced rates of infection in elderly subjects (CitationMeydani, Han, et al 2004). A study of 451 elderly subjects showed that 200 IU of vitamin E could reduce the incidence of viral upper respiratory infections, which are commonly associated with numerous complications in this age group (CitationMeydani, Leka, et al 2004).
Although some recent studies suggested that high doses of vitamin E might increase the risk of cardiovascular mortality, these studies were flawed in numerous ways, and their conclusions are unreliable. A subsequent review showed that both vitamin E and vitamin C are safe across a wide range of doses (at least up to 1600 IU for vitamin E, and 2000 mg for vitamin C). This review was authored by some of the most respected researchers in the field of vitamins and antioxidants (CitationHathcock et al 2005). They noted that a large number of people take a broad range of supplements well beyond the RDA, and that no consistent pattern of adverse effects has been seen at any dose for either vitamin. In addition, these supplements have important roles in antioxidant, free-radical protection, antiinflammatory effects, and other functions in maintaining homeostasis.
As noted above, vitamin E is one of the antioxidants that were studied in the AREDS research which showed benefits for AMD when administered in doses of 400 IU daily. The other nutrients in the AREDS research were zinc (80 mg), beta carotene (15 mg or 25 000 IU), and copper (2mg). Other antioxidants and carotenoids might also be useful for AMD, such as lutein (a carotenoid) and alpha-lipoic acid (a lipid and aqueous phase antioxidant).
Coenzyme Q10
Coenzyme Q10 (ubiquinone, or coQ10) is an antioxidant that is essential for mitochondrial energy production. It is manufactured in the body, but with aging the amounts are inadequate for optimum health. CoQ10 is essential for the heart muscle, and it helps lower blood pressure, improve congestive heart failure, and protect the brain in degenerative conditions such as Parkinson’s and Alzheimer’s diseases (CitationMorisco et al 1993). Statin drugs significantly lower the production of coQ10. Typical supplemental doses of coQ10 range from 100 mg daily for prevention against high blood pressure to 400 mg for heart disease patients (CitationMunkholm et al 1999). With severe congestive heart failure, higher doses may be beneficial. In neurologic disorders, research is now showing benefits from coQ10 in doses of 1200 mg or more (CitationSchults et al 2002).
Alpha lipoic acid
Alpha lipoic acid (ALA) is a sulfur-containing antioxidant that acts in both aqueous and lipid fractions of cells and tissues. It helps to detoxify heavy metals, such as mercury, and it helps protect neurologic tissues, and at high enough doses it can reverse early stages of diabetic peripheral neuropathy. Typical doses are from 100–200 mg for general prevention and up to 1000 mg for diabetics with neuropathy (CitationHahm et al 2004). At the higher doses it also helps to control blood sugar (CitationJacob et al 1999). Animal studies show that ALA protects the heart mitochondria against aging effects.
Chromium
Chromium is a trace mineral that helps to regulate blood sugar and lipid levels. Typical nutritional levels range from 50 mcg to 200 mcg in well nourished people. However, in diabetic patients, high doses of chromium, which are extremely safe, can significantly reduce blood sugar and enhance insulin sensitivity (CitationAnderson et al 1997). When 1000 mcg of chromium were administered to type II diabetics, 90% of them were able to eliminate the need for medication to control blood sugar levels (CitationAnderson 1997). Chromium supplements also lower total cholesterol and increase high density lipoprotein levels.
L-carnitine
L-carnitine is essential for the transport of free fatty acids across the mitochondrial membrane, where they are metabolized to create energy. Low L-carnitine levels reduce the functional capacity of the myocardium, leading to increases in angina and congestive heart failure. Supplements reduce angina and reduce mortality in patients with myocardial infarction. I typically recommend supplements of 1000 mg to 2000 mg of L-carnitine for prevention of heart disease for heart patients, and more in acute conditions.
Quercetin
Quercetin is a flavonoid that helps to control allergy symptoms of rhinitis and sinusitis. It stabilizes the membranes of mast cells, reducing the release of histamine. It is also helpful in lowering the risk of cataract by inhibiting glycoprotein formation in the lens (CitationCornish, et al 2002). Typical doses of quercetin are 800 mg to 1200 mg daily.
Conclusion
With basic knowledge of supplements, it is possible to avoid medications in the treatment and prevention of many health problems (Table and ). Numerous other supplements are valuable in appropriate doses, and they are part of a comprehensive health program, including diet, exercise, and stress management.
Table 1 Hypertension treatment program example
Table 2 Management of elevated lipid levels with supplements
Notes
This article was previously published in Anti-Aging Medicine, the official journal of the Japanese Academy of Anti-Aging Medicine (JAAM), an international affiliate of the Society for Applied Research in Aging (SARA).
References
- AndersonRDittrichOC1979Effects of ascorbate on leucocytes: Part IV. Increased neutrophil function and clinical improvement after oral ascorbate in 2 patients with chronic granulomatous diseaseS Afr Med J5647680550375
- AndersonROosthuizenRMaritzR1980The effects of increasing weekly doses of ascorbate on certain cellular and humoral immune functions in normal volunteersAm J Clin Nutr337167355784
- AndersonRTheronA1979Effects of ascorbate on leucocytes: Part III. In vitro and in vivo stimulation of abnormal neutrophil motility by ascorbateS Afr Med J5642933550365
- AndersonR1977Vitamin C and leukocyte ascorbateNutrition Today
- AndersonRAChengNBrydenNA1997Elevated intakes of supplemental chromium improve glucose and insulin variables in individuals with type 2 diabetesDiabetes461786919356027
- AndersonRA1997Nutritional factors influencing the glucose/insulin system: chromiumJ Am Coll Nutr16404109322187
- [AREDS] Age-Related Eye Disease Study Research Group2001A randomized, placebo-controlled, clinical trial of high-dose supplementation with vitamins C and E, beta carotene, and zinc for age-related macular degeneration and vision loss: AREDS report no. 8Arch Ophthalmol11914173611594942
- BatesCJWalmsleyCMPrenticeA1998Does vitamin C reduce blood pressure? Results of a large study of people aged 65 or olderJ Hypertens16925329794732
- CherubiniAZulianiGCostantiniF2001High vitamin E plasma levels and low low-density lipoprotein oxidation are associated with the absence of atherosclerosis in octogenariansJ Am Geriatr Soc49651411380761
- CornishKMWilliamsonGSandersonJ2002Quercetin metabolism in the lens: role in inhibition of hydrogen peroxide induced cataractFree Radic Biol Med33637012086683
- FotherbyMDWilliamsJCForsterLA2000Effect of vitamin C on ambulatory blood pressure and plasma lipids in older personsJ Hypertens184111510779091
- HahmJRKimBJKimKW2004Clinical experience with thioctacid (thioctic acid [lipoic acid]) in the treatment of distal symmetric polyneuropathy in Korean diabetic patientsJ Diabetes Complications18798515120701
- HathcockJNAzziABlumbergJ2005Vitamins E and C are safe across a broad range of intakesAm J Clin Nutr817364515817846
- JacobSRuusPHermannR1999Oral administration of RAC-alpha-lipoic acid modulates insulin sensitivity in patients with type-2 diabetes mellitus: a placebo-controlled pilot trialFree Radic Biol Med273091410468203
- KnektPReunanenAJarvinenR1994Antioxidant vitamin intake and coronary mortality in a longitudinal population studyAm J Epidemiol139118098209876
- MeydaniSNHanSNHamerDH2004Vitamin E and respiratory infection in the elderlyAnn N Y Acad Sci10312142215753147
- MeydaniSNLekaLSFineBC2004Vitamin E and respiratory tract infections in elderly nursing home residents: a randomized controlled trialJAMA2928283615315997
- MoriscoCTrimarcoBCondorelliM1993Effect of coenzyme Q10 therapy in patients with congestive heart failure: a long-term multicenter randomized studyClin Investig718 SupplS1346
- MunkholmHHansenHHRasmussenK1999Coenzyme Q10 treatment in serious heart failureBiofactors9285910416042
- SasazukiSSasakiSTsubonoY2006Effect of vitamin C on common cold: randomized controlled trialEur J Clin Nutr6091716118650
- ShultsCWOakesDKieburtzKParkinson Study Group2002Effects of coenzyme q10 in early Parkinson disease: evidence of slowing of the functional declineArch Neurol5915415012374491