Abstract
Objective
Fecal loading, cognitive impairment, loose stools, functional disability, comorbidity and anorectal incontinence are recognized as factors contributing to loss of fecal continence in older adults. The objective of this project was to assess the relative distribution of these factors in a variety of settings along with the outcome of usual management.
Methods
One hundred and twenty adults aged 65 years and over with fecal incontinence recruited by convenience sampling from four different settings were studied. They were either living at home or in a nursing home or receiving care on an acute or rehabilitation elderly care ward. A structured questionnaire was used to elicit which factors associated with fecal incontinence were present from subjects who had given written informed consent or for whom assent for inclusion in the study had been obtained.
Results
Fecal loading (Homes 6 [20%]; Acute care wards 17 [57%]; Rehabilitation wards 19 [63%]; Nursing homes 21 [70%]) and functional disability (Homes 5 [17%]; Acute care wards 25 [83%]; Rehabilitation wards 25 [83%]; Nursing homes 20 [67%]) were significantly more prevalent in the hospital and nursing home settings than in those living at home (P < 0.01). Loose stools were more prevalent in the hospital setting than in the other settings (Homes 11 [37%]; Acute care wards 20 [67%]; Rehabilitation wards 17 [57%]; Nursing homes 6 [20%]) (P < 0.01). Cognitive impairment was significantly more common in the nursing home than in the other settings (Nursing homes 26 [87%], Homes 5 [17%], Acute care wards 13 [43%], Rehabilitation wards 14 [47%]) (P < 0.01). Loose stools were the most prevalent factor present at baseline in 13 of the 19 (68%) subjects whose fecal incontinence had resolved at 3 months.
Conclusion
The distribution of the factors contributing to fecal incontinence in older people living at home differs from those cared for in nursing home and hospital wards settings. These differences need to be borne in mind when assessing people in different settings. Management appears to result in a cure for those who are not significantly disabled with loose stools as a cause for their fecal incontinence, but this would need to be confirmed by further research.
Introduction
Fecal incontinence (FI) is defined as the involuntary loss of liquid or solid stool that is a social or hygiene problem (CitationDepartment of Health 2002; CitationNorton et al 2002). Others exist (CitationKok et al 1992; CitationGroutz et al 1999; CitationCooper and Rose 2000), but they are not as robust. In addition this is the definition agreed by the International Continence Society which reflects a consensus amongst the experts in this field. There appear to be no gender differences in its prevalence in older adults (CitationO’Keefe et al 1995; CitationNakanishi et al 1997). The prevalence of FI ranges from 3% to 29% in the community (CitationThomas et al 1984; CitationCampbell et al 1985; CitationO’Keefe et al 1995; CitationPeet et al 1995; CitationNakanishi et al 1997; CitationProsser and Dobbs 1997; CitationEdwards et al 2001) with much higher figures in care homes (CitationBrocklehurst et al 1999; CitationChassagne et al 1999). The range is wide due to FI being defined differently in the various studies.
Several contributory factors are associated with FI in the older adult. These factors are fecal loading, loose stools, anorectal incontinence, comorbidity, impaired physical function, and impaired cognitive function (CitationBarrett 2002).
Having an idea of which contributory factors are more common in a particular setting will allow resources to be deployed in a way that is cost effective and also increase the likelihood of resolving the condition. It would also encourage further work as to why certain factors are more prevalent in a particular setting and following on that measures could be adopted to try and lessen the impact of the identified factors.
The objective of this study was to determine whether the distribution of the contributing factors to FI differed between elderly people in different care settings and to assess the usual outcome from management of the FI at three months post inclusion.
Methods
This cross sectional observational study was carried out on the Wirral Peninsula, Merseyside, UK between November 2002 and October 2003. Older adults aged 65 years and over with FI were recruited from the four settings used for this study: living at home (H); living in a nursing home (N); receiving care on acute (A) or rehabilitation (R) elderly care wards. All seven elderly care wards in the two local district general hospitals were involved. FI was defined as the involuntary or inappropriate passage of stool of whatever consistency on at least one occasion in the four weeks prior to giving consent.
The ethical approval granted by the local research ethics committee included the provision for obtaining assent for subjects who were unable to give consent themselves.
The questionnaire used for the study was modified after a pilot study to ensure reliability and validity.
The hospital or nursing home staff caring for the potential subjects in the participating hospital wards or nursing homes referred them to the study. These older adults with FI had the nature and purpose of the study explained to them and they were invited to participate. Subjects who gave both verbal and written informed consent were recruited. For those unable to give informed consent, relative assent was sought from their next of kin after the study was explained to them.
Potential subjects living in their own homes were identified through a database held by the continence specialist nurses. The continence specialist nurse wrote to these subjects explaining the nature and purpose of the study and inviting them to participate in it. Those who indicated their willingness to participate were then sent a patient information leaflet. After the principal investigator received a signed consent letter, a mutually convenient time was arranged for the interview. A letter was then sent to the general practitioner of each person recruited into the study informing them of their patient’s participation.
A recruitment target of 30 subjects in each group was set after a pilot study to allow comparisons to be made between the settings. The pilot study had indicated that recruitment would not be easy due to the sensitive nature of the topic being investigated. This also led to convenience sampling being utilized and therefore anyone who accepted an invitation to participate was recruited while those that did not were not asked why they declined. Also comparisons could not be made between those who accepted and declined as the principal investigator only had ethical approval to approach those who accepted to participate. The interventions in this study were the interviews and physical assessments.
Routine management here refers to whatever management strategies were utilized by the staff in the various settings to treat FI. This study did not look into this.
The study assessments were performed by Asangaedem Akpan (AA) and were based on a structured questionnaire to elicit which contributory factors for FI were present. The information collected also included: demographic information; previous medical and surgical history; Barthel Activities of Daily Living (ADL) score (CitationMahoney and Barthel 1965); Mini-Mental State Examination (MMSE) score (CitationFolstein et al 1975).
A physical examination limited to the abdomen and rectum was performed when specific consent was obtained.
The outcome of each subject’s FI was assessed three months after his or her first interview. Outcome here refers to whether the person was deceased or their FI had resolved or not if they were still alive.
Statistical analysis
The data was analysed using SPSS version 11 (SPSS Inc, Chicago, IL, USA). Descriptive statistics were used to summarize the results. The Chi-squared test was used to test categorical data for associations. If the overall Chi-squared test produced a significant result, paired comparisons were made by way of 2 × 2 tables with Yates correction. To allow for multiple comparisons, a Bonferroni correction was used (CitationTabachnick and Fidell 1996).
For continuous data with a normal distribution, a one-way analysis of variance (ANOVA) was utilized for comparing the various settings and in those with significant differences. Post-hoc multiple comparisons utilizing the Scheffe test was performed to determine where the differences existed. The Kruskal-Wallis test was utilized for continuous data that was not normally distributed (CitationPallant 2001).
The level of significance was a P value less than 0.05.
Results
Two hundred and thirty-nine older adults with FI were referred to the study. Recruitment was discontinued for each subgroup when the target sample size for that subgroup was reached. The participation rates (see ) were lowest in those living in their own homes (40%) and highest in those from the participating nursing homes (79%) though only three of the 52 nursing homes on the Wirral peninsula invited to participate in the study referred patients. The reasons why so many did not participate were not looked at, but this would have been an interesting area to explore in more detail.
Figure 1 Flow chart depicting the number of subjects with fecal incontinence referred to the study.
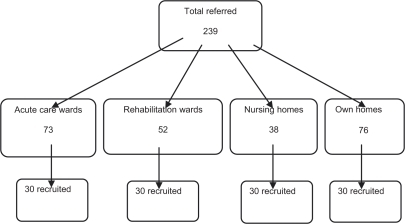
Thirty patients were assessed in each of the settings. The subjects who were living at home were significantly younger and less disabled than those in the other settings and were more likely to have had anorectal or urogenital surgery (see ).
Table 1 Baseline characteristics of the subjects in each setting. The childbirth data refers to the number of women who had one or more vaginal deliveries
Subjects in the nursing home setting had a significantly lower median MMSE score (N, 24) than in the other settings (H, 30; A, 27; R, 27) and were more likely to have cognitive impairment (N, 26 [87%]) identified as a factor contributing towards FI (see ). In the hospital settings just under half of those studied with FI had cognitive impairment (H, 5 [17%]; A, 13 [43%]; R, 14 [47%]).
Table 2 The prevalence of factors contributing to FI in the older adults studied in each of the settings
Functional disability was the main factor contributing to FI in the acute (25 [83%]) and rehabilitation ward settings (25 [83%]) and was common in the nursing home subjects (20 [67%]) but significantly less prevalent in the subjects living at home (5 [17%]). Although fecal loading was slightly less prevalent as a factor, the pattern was similar to that for functional disability (H, 6 [20%]; A, 17 [57%]; R, 19 [63%], N, 21 [70%]) ().
Loose stool was the most prevalent factor found to contribute to FI in subjects living at home (H, 11 [37%]), but it was found significantly more often in the acute and rehabilitation ward subjects (A, 20 [67%]; R, 17 [57%]), but was significantly less prevalent in the nursing home subjects (N, 6 [20%]) ().
There was considerable comorbidity in the study subjects, but this did not differ between the settings and was slightly more prevalent in the rehabilitation ward patients (H, 11 [37%]; A, 11 [37%]; R, 20 [67%]; N, 14 [47%]).
There was insufficient data collected on anorectal incontinence for reliable comment as the number of rectal examinations performed was low and many that were performed did not have sufficient detail recorded for evaluation. Of the 60 older adults seen in hospital for the study 21 (35%) had a rectal examination of which only 8 out of the 21 (38%) had sufficient details recorded regarding the examination (these were the ones performed by AA as part of the study). Thirty-nine out of the 60 (43%) hospital patients or their carer declined a rectal examination. Rectal examinations were not planned for those in nursing homes or living in their own homes. Their medical records were reviewed for any documented examination. Six (20%) of those living at home had documented evidence of a rectal examination being done while 4 (13%) of those in nursing homes had documented evidence of a rectal examination (). No patient had anorectal physiology tests.
Outcome at 3 months
At the three-month review FI was still an ongoing problem in 79 (66%) subjects included in the study (). It had resolved in 19 (16%) subjects who had a significantly higher median Barthel index at baseline (13 [interquartile range (IQR) 7–17]) than in the subjects in which the FI persisted (6 [IQR 2–12]) or had died (1 [IQR 0–5]).
Table 3 Comparison of the baseline characteristics of patients in relation to whether their FI had resolved or not when reviewed after 3 months
Fecal incontinence resolved with usual management from the regular care team within 3 months in 30% of the subjects living in their own homes, but not in any of the nursing home subjects. Loose stools were the most prevalent factor present at baseline in 13 of the 19 (68%) subjects whose problem resolved.
Mortality
Twenty-two of the 120 (18%) subjects in the study died before the 3 month review. All but 3 of these were in the hospital wards at the baseline assessment. Thirteen (43%) of the acute ward subjects with FI did not survive.
Discussion
This study has demonstrated that the relative distribution of the multiple contributory factors previously described for FI in older adults (CitationBarrett 2002) varies between the healthcare settings in which patients are seen.
The present study concentrated on the general health factors but it has underestimated the extent of the anorectal factors in FI in the four settings. Only a few had anorectal examinations as part of their routine medical care (which was not examined in this study) and assent or consent tended to be low for the physical examination for reasons given later in the discussion.
Previous anorectal physiology work has demonstrated abnormal anorectal physiology in a dependent group of older people with FI (CitationBarrett 1988), but that only accounted for 35% of the variance in a multiple regression analysis of the presence of FI and its frequency.
CitationSanford (1975) has previously demonstrated that the onset of FI is often the issue that leads to the discontinuation of home care and a move into an institution. The significant difference in age and Barthel ADL scores between the living at home and nursing home groups indicates that they are very different and this is reflected in the difference in the relative prevalence of the contributory factors in these two settings. More contributory factors were found in the nursing home subjects. Cognitive impairment was the most prevalent with a large element of fecal loading and functional disability which is consistent with previous studies (CitationJohanson et al 1997; CitationBrocklehurst et al 1999; CitationChassagne et al 1999). Loose stools were the most prevalent factor in the subjects living at home.
The relative prevalence of these factors should be borne in mind when clinically assessing patients in these settings as the relative importance of treatment approaches should reflect the difference in the contributory factors in various clinical settings.
Thirty percent of the living at home patients improved with routine medical care during the 3-month study period. These patients were on the register of the continence service and therefore included patients with long-term ongoing problems. The sample did not include new acute cases in whom a better result might have been anticipated though there is still a lack of reliable evidence to predict treatment success rates on general patients. CitationHarari and colleagues (2004) achieved an increase in bowel movements following a single intervention in community dwelling post stroke patients with constipation or FI, but no alteration in episodes of FI. The intervention was a one-off assessment by a nonspecialist nurse who had received some basic bowel management training. The patient and carer were given some education, provided with a booklet and the patient’s doctor was informed of the bowel condition and treatment.
In their landmark paper, CitationTobin and Brocklehurst (1986) demonstrated the potential for improvement in the care home sector using simple measures. These included daily enemas followed by lactulose and weekly enema for those with fecal loading and codeine phosphate daily with twice-weekly enemas for those with anorectal incontinence. The FI did not resolve in any of the nursing home subjects in the current study. This issue needs to be considered in future work as either the original study does not apply to the current nursing home population, or the findings are not being implemented, or both.
The subjects recruited from acute and rehabilitation elderly care wards were similar in many respects. Functional disability, fecal loading and loose stools were all contributory factors for FI in the majority of patients in these settings. This is similar to the only previous study when loose stools, increased severity of illness and older age were found to be the significant factors for FI on acute medical wards (CitationBliss et al 2000). Comorbidity was more common among the rehabilitation ward patients in the current study.
FI assessment
In routine clinical practice digital rectal examination is an essential component of the assessment of an older person with FI. Sadly these examinations were not performed in over 80% of the fecally incontinent patients in the rehabilitation wards studied even though continence has a major impact on discharge planning. The Royal College of Physicians national continence audit confirms that this lack of adequate assessment is widespread (CitationBBC 2005).
Only 13 (22%) of the 60 study subjects in the hospital setting had a digital rectal examination performed as part of their routine clinical assessment. Another 8 (13%) had one performed as part of this study. Some of the study subjects who did not have rectal examinations performed were too ill, but the majority had cognitive impairment and separate assent was not given for that part of the study. These findings are in contrast to a previous finding that most older adults with no cognitive impairment and that were not critically ill would give permission for a digital rectal examination to be performed on them (CitationMorgan et al 1998).
3-month mortality
The 3-month mortality rate was highest in the acute ward patients at 43%. It is increasingly recognized that fecal as well as urinary incontinence in early stroke patients is a poor prognostic factor for survival (CitationNakayama et al 1997). The mortality among the acute ward patients in this study data suggests that loss of continence in the setting of any acute illness may be a marker of terminal illness as suggested in previous studies in older adults living at home (CitationNakanishi et al 1999) or in a nursing home (CitationChassagne et al 1999).
There was an increased mortality associated with FI in frail older adults especially those in the hospital setting. This may be more related to the underlying illness than the incontinence itself.
Conclusions
The distribution of the factors contributing to FI in older people living at home differs from those cared for in nursing home and hospital wards settings. These differences need to be borne in mind when assessing people in different settings. Management appears to result in a cure for those who are not significantly disabled with loose stools as a cause for their FI.
Part of the reason why resolution of FI is poor may be related to inadequate assessments, especially rectal examinations. Further research would be useful in looking at treatment options and whether FI in the acute setting is a marker of terminal illness. It would be interesting to see if the distribution of the factors contributing to FI in older people in this study is similar outside the United Kingdom.
Acknowledgements
We wish to acknowledge the invaluable assistance to recruitment from Janice Evans, and Debbie Ollerhead from the Wirral Continence Service and the staff on the acute and Rehabilitation Elderly care wards in Wirral Hospital and the matrons of the participating nursing homes. We also wish to thank Professor Christine Norton and Dr Danielle Harari for commenting on the original protocol for the study. The Wirral NHS Trust Research award provided funding for this study. The Wirral Research Ethics Committee approved the study and approval letters can be provided on request.
References
- BarrettJA1988A study of the anorectal pathophysiology of geriatric patients with faecal incontinenceMD Thesis.LiverpoolUniversity of Liverpool
- BarrettJA2002Pathophysiology of constipation and faecal incontinence in older peoplePotterJNortonCCottendenABowel care in older peopleLondonRoyal College of Physicians522
- BBC news2005Incontinence care is ‘inadequate’ [online]. Accessed on 23 November 2005. URL: http://news.bbc.co.uk/1/hi/health/4459906.stm
- BlissDZJohnsonSSavikK2000Fecal incontinence in hospitalized patients who are acutely illNurs Res49101810768587
- BrocklehurstJDickinsonEWindsorJ1999Laxatives and faecal incontinence in long-term careNurs Stand1332610693509
- CampbellAJReinkenJMcCoshL1985Incontinence in the elderly: prevalence and prognosisAge Ageing1465704003185
- ChassagnePLandrinINeveuC1999Fecal incontinence in the institutionalized elderly: incidence, risk factors, and prognosisAm J Med10618519010230748
- CooperZRRoseS2000Fecal incontinence: a clinical approachMt Sinai J Med679610510747364
- Department of Health2002Good practice in continence servicesLondonDepartment of Health, PL/CMO/2000/2.2002.
- EdwardsNIJonesD2001The prevalence of faecal incontinence in older people living at homeAge Ageing30503711742780
- FolsteinMFolsteinSMcHughP1975Mini-mental state. A practical method for grading the cognitive state of patients for the clinicianJ Psychiatr Res12189981202204
- GroutzAFaitGLessingJB1999Incidence and obstetric risk factors of postpartum anal incontinenceScand J Gastroenterol343151810232879
- HarariDNortonCLockwoodL2004Treatment of constipation and fecal incontinence in stroke patients. Randomized controlled trialStroke3525495515486330
- JohansonJFIrizarryFDoughtyA1997Risk factors for fecal incontinence in a nursing home populationJ Clin Gastroenterol24156609179734
- KokALVoorhorstFJBurgerCW1992Urinary and faecal incontinence in community-residing elderly womenAge Ageing21211151615785
- MahoneyFBarthelD1965Functional evaluation: the Barthel indexMd State Med J1461514258950
- MorganRSpencerBKingD1998Rectal examinations in elderly subjects: attitudes of patients and doctorsAge Ageing273536
- NakanishiNTataraKNaramuraH1997Urinary and fecal incontinence in a community-residing older population in JapanJ Am Geriatr Soc45215199033523
- NakanishiNTataraKShinshoF1999Mortality in relation to urinary and faecal incontinence in elderly people living at homeAge Ageing28301610475868
- NakayamaHJorgensonHSPedersonPM1997Prevalence and risk factors of incontinence after strokeStroke2858628996489
- NortonCChristiansenJButlerU2002Anal incontinenceAbramsPCardozoLKhourySIncontinence: Second international consultation on incontinencePlymouthHealth Publications Ltd9871043
- O’KeefeEATalleyNJZinsmeisterAR1995Bowel disorders impair functional status and quality of life in the elderly: a population-based studyJ Gerontol A Biol Sci Med Sci50M18497614239
- PallantJ2001SPSS Survival Manual. A step by step guide to data analysis using SPSSBuckinghamOpen Univ Pr
- PeetSMCastledenCMMcGrotherCW1995Prevalence of urinary and faecal incontinence in hospitals and residential and nursing homes for older peopleBMJ311106347580664
- ProsserSDobbsF1997Case-finding incontinence in the over-75sBr J Gen Pract474985009302789
- SanfordJRA1975Tolerance of debility in elderly dependants by supporters at home: its significance for hospital practiceBr Med J347131156826
- TabachnickBGFidellLS1996Using multivariate statistics3rd editionNew YorkHarper Collins
- ThomasTMEganMWalgroveA1984The prevalence of faecal and double incontinenceCommunity Med6216206478780
- TobinGWBrocklehurstJC1986Faecal incontinence in residential homes for the elderly: prevalence, aetiology and managementAge Ageing154163953330