Abstract
Incidence rates of renal cell cancer, which accounts for 85% of kidney cancers, have been rising in the United States and in most European countries for several decades. Family history is associated with a two- to four-fold increase in risk, but the major forms of inherited predisposition together account for less than 4% of renal cell cancers. Cigarette smoking, obesity, and hypertension are the most consistently established risk factors. Analgesics have not been convincingly linked with renal cell cancer risk. A reduced risk of renal cell cancer among statin users has been hypothesized but has not been adequately studied. A possible protective effect of fruit and vegetable consumption is the only moderately consistently reported dietary finding, and, with the exception of a positive association with parity, evidence for a role of hormonal or reproductive factors in the etiology of renal cell cancer in humans is limited. A recent hypothesis that moderate levels of alcohol consumption may be protective for renal cell cancer is not strongly supported by epidemiologic results, which are inconsistent with respect to the categories of alcohol consumption and the amount of alcohol intake reportedly associated with decreased risk. For occupational factors, the weight of the evidence does not provide consistent support for the hypotheses that renal cell cancer may be caused by asbestos, gasoline, or trichloroethylene exposure. The established determinants of renal cell cancer, cigarette smoking, obesity, and hypertension, account for less than half of these cancers. Novel epidemiologic approaches, including evaluation of gene–environment interactions and epigenetic mechanisms of inherited and acquired increased risk, are needed to explain the increasing incidence of renal cell cancer.
Descriptive epidemiology
Kidney cancer is the ninth most common cancer in developed countries.Citation1 Approximately 85% of kidney cancers are renal parenchyma (renal cell) cancers, while the remainder for the most part are urothelial cancers of the renal pelvis.Citation2 Approximately 80% of renal cell cancers are clear cell adenocarcinomas, the remainder being papillary (∼15%), chromophobe (∼5%), and collecting duct carcinomas (<1%). Both renal cell and renal pelvis cancers are about twice as common among men as among women,Citation1–Citation3 with the mean age at diagnosis in the early 60s for renal cell cancer and in the late 60s for renal pelvis cancer. For renal pelvis cancer, there is a strong tendency to develop multiple transitional epithelial tumors, particularly in the urinary bladder and ureter.Citation4 For the most part, renal pelvis cancer parallels bladder cancer in epidemiologic characteristics and risk factors and has been addressed by the authors elsewhere.Citation4
Rates of renal cell cancer vary internationally as much as 10-fold (), suggesting a strong role for exogenous risk factors in addition to possible roles of geographic differences in genetic susceptibility and diagnostic variability. Incidence is generally highest in several Western and Eastern European countries, as well as in parts of Italy, in North America, and in Australia/New Zealand. The lowest rates are reported in Asia and Africa. How much of this difference is a function of completeness of reporting by country is not clear, but it probably plays a important role.
Table 1 International variation in age-adjusted incidence rates (per 100,000 person-years) for renal cell cancer in selected countries
Over the past several decades, incidence rates for renal cell cancer have been rising steadily each year in Europe and the United States,Citation5 although incidence rates appear to have recently stabilized or decreased in many European countries.Citation6 In the United States in 2008, 54,390 new cases and 13,010 deaths were expected from kidney cancer.Citation2 A recent report showed that, while the rate of new cancer diagnoses overall dropped 1.8% among men and 0.5% among women in the United States between 2001 and 2005, kidney cancer incidence rose 1.7% per year for males and 2.2% per year for females.Citation7 While there has been a decrease in the size of diagnosed renal cell tumors over time,Citation8,Citation9 as a result of rapidly improved imaging technology and earlier detection over the last 25 years, an increasing incidence of large and late-stage renal cell cancers has also been observed and accounts in part for the overall increase in incidence.Citation5,Citation9,Citation10 In the United States, increases in incidence have been more rapid among women than menCitation11 and, in particular, among blacks than whites,Citation10 leading to a substantial shift in excess from among whites to among blacks,Citation10 which is becoming pronounced over time (). Age-adjusted incidence rates of renal cell cancer among white men, white women, black men and black women in the United States during 2000–2005 were, respectively, 16.31, 8.03, 19.24, and 8.87 per 100,000 person-yearsCitation3 ().
Figure 1 Trends in age-adjusted (2000 United States standard) incidence of renal cell cancer by race and sex, 1973–2005 (Based on SEER data for nine geographic regions of the United States: Atlanta, Georgia; Connecticut; Detroit, Michigan; Hawaii; Iowa; New Mexico; San Francisco/Oakland, California; Seattle/Puget Sound, Washington; and Utah).Citation3
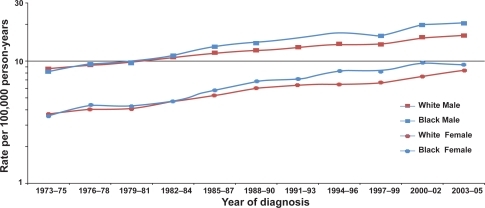
Table 2 Age-adjusted incidence ratesTable Footnote* for renal parenchyma cancer by racial/ethnic group and sex according to SEER program, 2000 through 2005
Five-year relative survival rates for renal cell cancer in the United States reached 65.1% among men and 66.8% among women by 2005,Citation3 compared with below 40% in the early 1960sCitation10 (). For localized renal cell cancer cases, the five-year relative survival rate is approximately 90%, regardless of race or gender.Citation3 In Europe, kidney cancer mortality peaked in the early 1990s at 4.8 per 100,000 in men and 2.1 per 100,000 in women, and then declined to 4.1 and 1.8 per 100,000, respectively, by 2004.Citation6 Despite increasing incidence rates, United States kidney cancer mortality rates, which are based on deaths from renal cell cancer as well as cancer of the renal pelvis, have been remarkably stable over the past 15 years, fluctuating between 4.1 and 4.3 per 100,000, suggesting a benefit of early detection and consequent surgical treatment.
Table 3 Five-year relative and cause-specific survival ratesTable Footnote* for renal parenchyma cancer by race and sex according to SEER program for cases diagnosed from 1990 through 2004
Risk factors for renal cell cancer
Epidemiologic studies for consideration in this review were identified through a MEDLINE® search of the literature. For the purposes of this review, all papers published through 2008 were identified by use of either the term “renal cancer” or the term “kidney cancer” together with the term “risk factor” or “epidemiology.” Moreover, all review papers addressing risk factors for kidney cancer in general or renal cell cancer in particular were identified, and references were examined to supplement, if necessary, papers recovered through the initial search. Findings of individual studies were evaluated, and a qualitative summary of the results is presented herein. In the interest of keeping the paper to a reasonable length, we have not attempted to cite every paper that we identified, but rather to emphasize those findings that reflect consistency in the literature.
Information on risk factors for renal cell cancer was established by a large number of case-control studies starting in the 1980s and supported more recently by cohort studies.Citation12–Citation71 The largest case-control study to date, based on 1,732 cases and 2,309 controls, was a multicenter collaborative investigation conducted in five countries using a common protocol, questionnaire, field procedures, and analytic techniques.Citation34,Citation72–Citation78 When citing results from this international collaborative investigation, only the combined multicenter results will be reported, not center-specific findings.
Genetic susceptibility
Renal cell cancer occurs in both sporadic and hereditary forms. Having a first degree relative with kidney cancer has been associated with a two- to four-fold increased risk in most studies.Citation79 Hereditary renal cell cancer tends to occur earlier in life than sporadic forms of the disease, and often involves bilateral, multifocal tumors.Citation80
Although only about 3%–4% of renal cell cancers are explained by inherited predisposition,Citation80,Citation81 it is surprising that no cancer has as many different types of genetic predisposition as renal cell cancer.Citation82 Among the rare high-penetrance genetic forms of renal cell cancer are von Hippel–Lindau (VHL) disease (predisposing to clear cell cancer), hereditary papillary carcinoma, hereditary leiomyomatosis and renal cell cancer (papillary), Birt–Hogg–Dubé syndrome (mainly chromophobe and oncocytoma), chromosome 3 translocation-associated (clear cell), tuberous sclerosis (clear cell), and a mutated succinate dehydrogenase (SDHB) gene.Citation80,Citation81 In contrast, the only hereditary syndrome with known predisposition to renal pelvis cancer is hereditary nonpolyposis colorectal cancer.Citation80 Genetics play a role in renal cell cancer beyond clearly inherited susceptibility, as it has been shown that the majority of noninherited clear cell carcinomas are associated with inactivation of the VHL gene through mutation or promoter hypermethylation.Citation80
Obesity
Renal cell carcinoma is consistently associated with obesity in virtually all epidemiologic studies, including recent large prospective studies in the Netherlands, Norway, and the United States.Citation59,Citation60,Citation62,Citation65,Citation70,Citation71,Citation78,Citation83–Citation85 Most studies have found an association with elevated body mass index (BMI) among both men and women, and abdominal obesity, as indicated by waist-to-hip ratio,Citation58,Citation65,Citation70,Citation71,Citation85 may play an important role in this association, particularly among women. A quantitative review of the published literature reported a summary relative risk for renal cell cancer of 1.07 per unit increase of BMI.Citation83 A more recent meta-analysis reported that associations with increased BMI were stronger in women than in men; summary risk ratios per 5 kg/m2 increase in BMI were 1.24 (95% confidence interval [CI] 1.15–1.34) among men and 1.34 (95% CI 1.25–1.43) among women.Citation86
Several plausible mechanisms have been suggested for the association between obesity and renal cell cancer, but the actual mechanism remains speculative. Obesity may promote changes in circulating levels of estrogen and other steroid hormones, or elevated levels of insulin-like growth factor-I (IGF-I), which could in turn contribute to the development of renal cell cancer.Citation87–Citation90 Lipid peroxidation, which is increased among obese subjects, has been hypothesized to be partly responsible for the association of obesity with renal cell cancer through the formation of DNA adducts.Citation91 Other conjectured mechanisms include elevated cholesterol level and down-regulation of low-density lipoprotein receptor, lower levels of vitamin D, and increases in adipose tissue-derived hormones and cytokines, such as leptin and adiponectin.Citation84,Citation92,Citation93
The increasing prevalence of obesity, rapidly becoming a worldwide epidemic,Citation93–Citation95 is likely to account in part for the rising incidence of renal cell cancer. Recent calculations suggest the proportion of renal cell cancer attributable to being overweight and obese could be as high as 40% in the United States and Canada and 30% in Europe.Citation83,Citation87,Citation93,Citation96,Citation97
Cigarette smoking
Cigarette smoking is a recognized though moderate cause of renal cell cancer.Citation98 A recent meta-analysisCitation99 of data from 19 case-control studies (8,032 cases and 13,800 controls) and five cohort studies (1,457,754 participants with 1,326 renal cell cancer cases) reports statistically significant relative risks of 1.5 and 1.2 for male and female smokers, respectively. There was a strong dose-dependent increase in risk, up to 2- and 1.6-fold among heavy (21 or more cigarettes per day) men and women smokers, respectively. There was a significant decline in risk in both sexes with years of cessation, with a 15% to 30% reduction in risk 10 to 15 years after quitting.Citation99 Approximately 20% to 30% of renal cell cancers among men and 10% to 20% among women are estimated to be attributable to cigarette smoking.Citation34,Citation100,Citation101
Hypertension and antihypertensive medications
The recent increases in renal cell cancer incidence may be associated, again in an unknown way, with the increasing prevalence of hypertension in the United States, particularly among blacks and among women.Citation101,Citation102 While it is difficult to separate the effects of hypertension or its treatment on renal cell cancer risk, as they are highly correlated variables, the collective epidemiologic evidence to date suggests that it is hypertension itself that is the determinant. Most studies have reported risks for renal cell cancer associated with either recorded blood pressure or reported hypertension ranging between 1.2 and 2 or greater,Citation48,Citation51,Citation54–Citation56,Citation62,Citation68,Citation69,Citation72,Citation103–Citation106 although not all of the studies were able to adjust for the effect of antihypertensive medications. Dose-response relations between measured blood pressure level and renal cell cancer risk have been reported,Citation54,Citation56,Citation106 although only one of these studies provided data on women and considered the effect of antihypertensive medication.Citation106 In that analysis of 254,935 men and women in the European Prospective Investigation into Cancer and Nutrition (EPIC), the relative risks for the highest versus the lowest category of systolic (≥160 vs <120 mmHg) and diastolic (≥100 vs <80 mmHg) blood pressure were 2.48 (95% CI 1.53–4.02) and 2.34 (95% CI 1.54–3.55), respectively, independent of use of antihypertensive medication. A case-control study reported that high systolic and diastolic blood pressures were independently associated with increased renal cell cancer risk in both sexes when analyses were restricted to those who never took antihypertensive medication.Citation103 SeveralCitation55–Citation57,Citation63,Citation106 cohort studies have demonstrated an increased risk even after exclusion of the early years of follow-up, when early stage, prediagnostic renal tumors may themselves lead to elevated blood pressure. Recent findings from the Netherlands cohort studyCitation105 suggest that the association with hypertension may be stronger among the small fraction of sporadic renal cell cancer patients with von Hippel–Lindau gene mutations, but this needs to be confirmed in future studies.
Most epidemiologic studies of antihypertensive drugs and renal cell cancer risk have found that diuretic use, a causal factor candidate in early studies, is not an independent risk factor, and adjustment for high blood pressure appears to eliminate any excess risk associated with diuretic use.Citation48,Citation62,Citation72,Citation103 In a study of the various classes of antihypertensive medications, no particular type or class of these medications was consistently associated with renal cell cancer risk.Citation107
The biologic mechanism for the association between high blood pressure and renal cell cancer risk is unknown. Among the candidate hypotheses regarding mechanism has been hypertension-induced renal injury and metabolic or functional changes within the renal tubule induced by hypertension increasing susceptibility to carcinogens. It has also been speculated that elevated levels of IGF-I or lipid peroxidation associated with hypertension, as well as up-regulation of hypoxia-inducible factors, could contribute to the development of renal cell cancer. Contrary to expectation, detection bias due to incidental diagnosis during work-ups for hypertension was not supported in a study which directly evaluated that hypothesis.Citation108
Analgesics
Historically, the causal connection of heavy use and abuse of phenacetin-containing analgesics and transitional cell cancers of the renal pelvis has long been recognized. Phenacetin’s effect on adenocarcinomas of the renal parenchyma, however, is inconclusive,Citation27,Citation28,Citation109 and it is now impossible to assess because phenacetin-containing analgesics have been off the market for up to 30 years in most countries and reliable recall of past intake is no longer achievable.
Among other analgesics, acetaminophen has received the most attention, since it is the major metabolite of phenacetin, although several studies have also examined the effect of aspirin use on renal cell cancer.Citation21,Citation73,Citation109–Citation113 Neither acetaminophen nor aspirin has been credibly associated with an increase in renal cell cancer risk.Citation73,Citation111
Statins
Statins are widely used drugs for the treatment of lipid disorders, particularly hypercholesterolemia. Despite reported antitumorigenic activity of statins, including their inhibition of proliferation and promotion of apoptosis, their potential effectiveness for the primary prevention of cancer remains to be reliably demonstrated. While some observational studies have reported inverse associations with cancer, neither the Cholesterol Treatment Trialists’ (CTT) CollaborationCitation114 nor two recent meta-analysesCitation115,Citation116 found evidence of an effect of statin therapy on cancer risk. A study based on Veteran Affair (VA) databases in the United States reported a 50% reduced risk of renal cell carcinoma among statin users compared with nonusers.Citation117 This finding may be influenced by selection bias, however, since the controls were drawn from frequent users of the VA system who might be more likely to be prescribed statins. Furthermore, the study did not address the influence of dose, duration, and type of statin in relation to renal cell cancer risk. There is some evidence that only lipophilic statins, such as simvastatin and lovastatin, possess antineoplastic effects, whereas hydrophilic statins, such as pravastatin, do not have chemopreventive potential.Citation118,Citation119 Other epidemiological studies reporting on the association of statin use and urologic cancers have yielded inconsistent results;Citation119–Citation125 however, only combined results for kidney and bladder cancer were presented in many of these studies. A follow-up study of 361,859 statin users, most of whom received lovastatin or simvastatin, found a non-significantly increased risk of kidney/renal pelvis cancer.Citation125 Two case-control studies reported no association between current or regular statin use and kidney cancer.Citation121,Citation123 Most published studies on statin use had relatively short follow-up and reported for the most part only on the most common cancer types. Further research is warranted to investigate the association between use of statins and any potential increase or decrease in risk of renal cell cancer, with particular focus on duration, intensity, and type and dose of statin used.
Dietary factors
Renal cell cancer has not been convincingly linked to any specific dietary factor, with the exception of a moderately consistent protective effect for overall fruit and vegetable consumption.Citation61,Citation126–Citation130 However, two recent large prospective studies, one based on 375,851 participants in the EPIC studyCitation131 and the other based on 120,852 men and women in the Netherlands Cohort Study on Diet and Cancer (NLCS),Citation132 reported no protective effect of vegetable and/or fruit consumption on renal cell cancer. Some epidemiologic studies suggest that elevated protein consumption may be a risk factor for renal cell cancer. There may be some biologic plausibility to a high protein diet affecting risk of renal cell cancer, because animal studies have shown protein intake can induce renal tubular hypertrophy, but the largest study to date to evaluate this association failed to provide clear support for this hypothesis,Citation78 as has a large, pooled analysis of 13 cohort studies.Citation133
Elevated risks have been reported for consumption of meat,Citation16,Citation24,Citation27,Citation28,Citation47,Citation128 milk,Citation21,Citation25 and margarine, oils and other fat types;Citation25,Citation47 however, most of these findings were not adjusted for confounding by energy intake. Sporadic inverse associations have been reported with respect to vitamin C,Citation47 Vitamin E,Citation78,Citation128 carotenoids,Citation127 and calcium,Citation128 but no particular micronutrient or vitamin has been consistently observed to decrease or increase the risk of renal cell cancer in case-control or cohort studies. Although originally thought almost 30 years ago to be a key area for renal cell cancer causation, dietary studies have not fulfilled their early promise.
Alcohol consumption
Early ecologic studies consistently suggested a positive correlation between kidney cancer and per capita consumption of alcohol.Citation134–Citation136 However, these ecologic findings were not confirmed by numerous analytic epidemiologic studies of renal cell cancer conducted during the ensuing two decades.Citation4,Citation66 After adjustment for the confounding effect of cigarette use, virtually all studies showed no association between alcohol consumption and renal cell cancer.Citation16–Citation20,Citation24,Citation25,Citation27,Citation28,Citation30,Citation78 Cohort studies of alcoholics and brewery workers have also reported no excess of mortality from kidney cancer.Citation137–Citation142
By contrast, a post hoc hypothesis has recently appeared in the literature that moderate levels of alcohol consumption may be protective for renal cell cancer. The findings of recent individual studies show considerable heterogeneity and inconsistency with respect to the categories of alcohol consumption, the amount of alcohol intake reportedly associated with decreased renal cell cancer risk, and differential observations between men and women. A pooled analysis of data from 12 prospective studies of renal cell cancer was recently published, based on results of five published studiesCitation58,Citation143–Citation145 as well as numerous others which had not previously published their data related to alcohol consumption.Citation146 The pooled analysis was based on 1430 incident cases of renal cell cancer (719 men and 711 women), and demonstrated an apparent inverse-response relation at levels of consumption equivalent to less than a drink per day, with no further protective effect at levels of intake above a drink a day. It is difficult to speculate what biologic mechanism could explain this type of dose-response pattern, unless of course one invokes a hormesis-like effect of low-dose alcohol on renal cancer risk while other organs seemingly do not enjoy this anticarcinogenic effect.
Finally, alcohol itself is a known human carcinogen and heavy alcohol drinking has been conclusively linked to increased risks of numerous types of cancer, including oral, pharyngeal, laryngeal, esophageal, liver and probably breast and colon and rectum.Citation147 A protective effect of alcohol consumption on renal cell cancer at very low levels of intake has little biologic plausibility or face validity. In addition to the extensive analytic epidemiologic evidence from the past 40 years, the descriptive patterns of renal cell carcinoma are not consistent with an inverse association with alcohol intake. In particular, the rate of renal cell carcinoma among men is twice that among women worldwide, whereas men tend to consume alcohol at substantially higher levels than women.
Hormonal and reproductive factors
Reductions in risk of renal cell cancer have been reported among users of oral contraceptives in some,Citation76,Citation148 but not all studies,Citation149,Citation150 and in the large international case-control study protection was restricted to nonsmokers.Citation76 Several studies have reported an almost two-fold increased risk among women with high parity compared with nulliparous women, after adjustment for obesity,Citation76,Citation148,Citation151 and an inverse association between age at first birth and risk of renal cell cancer has been reported in someCitation28,Citation39,Citation149,Citation151 but not all studies.Citation148,Citation150 Hormones have induced renal tumors in laboratory animals; however, with the exception of a positive association with parity, evidence for a role of hormonal or reproductive factors in the etiology of renal cell cancer in humans is limited and not entirely consistent to date.
Occupation
As compared with bladder cancer, renal cell cancer has not been convincingly linked to any occupational exposure.Citation4 However, because of the large number of epidemiologic studies, particularly case-control studies, that have been conducted over the last three decades, a number of sporadic associations have been reported between exposures or jobs/industries and renal cell cancer. Asbestos has been associated with elevated renal cancer mortality in two cohort studies, one of insulatorsCitation152 and one of asbestos products workers,Citation153 as has self-reported asbestos exposure in several case-control studies, including the large international study.Citation75 An extensive meta-analysis of occupational cohort studies of asbestos-exposed workers showed little relation to increased risk for renal cancer.Citation154
In the early 1980s, unleaded gasoline was suspected as a risk factor for renal cell cancer based on long-term rodent bioassays in which male rats developed renal tumors. Since then, a number of occupational cohort and nested case-control studies have examined the effect of gasoline exposure in numerous populations, and the collective evidence to date does not support a relation between gasoline and risk of renal cell cancer.Citation155–Citation165 Further, the mechanism by which male rats developed kidney cancer when exposed to unleaded gasoline vapors, via a unique protein molecule, alpha2 microglobulin, has no counterpart in humans.Citation156,Citation166
In recent years, considerable attention has focused on the solvent trichloroethylene (TCE), largely as a result of animal findings and of three epidemiologic studies conducted in one area of Germany, initiated in response to a cluster of renal cell cancer cases observed in a plant. All three of these studies reported strikingly elevated relative risks for renal cell cancer associated with TCE exposure.Citation167–Citation169 The findings contrast starkly with results from other investigations, and several serious methodological shortcomings of these studies have been noted,Citation170–Citation172 limiting any conclusion that can be drawn. To date, seven occupational cohort studies have evaluated the relationship between TCE exposure and specific types of cancer. The two largest employed sophisticated methods of exposure assessment and both internal and external comparisons.Citation173,Citation174 Neither of these studies reported a significantly increased risk of renal cell cancer among TCE-exposed workers. The most recent cohort study,Citation175 conducted in Denmark, evaluated cancer incidence among 40,049 workers with presumed TCE exposure and found a weak association with renal cell cancer among those thought to be heavily exposed to TCE. The weight of the evidence to date, however, does not provide consistent, credible support for the hypothesis that TCE is a cause of renal cell cancer in humans.Citation176 Whether TCE is a renal carcinogen in humans remains an open question, which will require more and better research.
A German study reported that VHL mutations were found in 33 of 44 RCC patients from North Rhine–Westphalia with TCE exposure.Citation177,Citation178 Of the 33 patients with VHL mutations, 14 had multiple VHL mutations and remarkably, 13 had the same C to T substitution in codon 81.Citation177 Two subsequent studies could not confirm either the tendency towards multiple VHL mutations or the VHL codon 81 mutation hot spot in TCE-exposed RCC patients from Germany and France.Citation179,Citation180 In view of the widespread use of TCE around the world, it is noteworthy that among approximately 600 VHL mutations reported in sporadic RCC patients from other published studies (predominately of western European patients), only one other C to T substitution in codon 81 has been reported.Citation181 This suggests that the VHL mutation hot spot in the German study resulted from either a unique TCE exposure situation in a restricted geographic area or some other environmental exposure prevalent in that geographic area. If the VHL codon 81 mutation hot spot is a marker for TCE-induced RCC, then the overall findings suggest that TCE is not a major contributor to the global RCC burden.
Kidney transplantation and dialysis
Acquired renal cystic disease of the native kidneys is believed to account for the substantially higher average annual incidence of renal cell carcinoma in dialysis patients, independent of patient age or underlying renal disease.Citation182,Citation183 Several recent studies of cancer risk subsequent to kidney transplantation have found a substantially increased risk of acquired renal cystic disease and renal cell cancer compared with the general population, presumed to be a result of immune-suppressing medications used in transplant patients.Citation184
Summary
To date, the causal determinants identified for renal cell cancer in epidemiologic studies, cigarette smoking, obesity, and hypertension, are at best moderate in their effect on risk and account for less than half of these cancers. Major, explanatory causes of renal cell cancer await novel epidemiologic approaches, including more sophisticated genetic studies. Because single-gene determinants of renal cell cancer have been thoroughly investigated for almost 30 years with at best very limited success, future investigations should examine more complex genetic associations, including gene-environment interactions and epigenetic mechanisms of inherited and acquired increased risk.
Acknowledgements
This paper is dedicated to the memory of Dr Edward Lipworth (1910–2009) a leading urologist in both South Africa and Israel whose lifelong passion for learning and helping mankind extended almost an entire century.
Disclosure
The authors report no conflicts of interest in this work.
References
- ParkinCMWhelanSLFerlayJTeppoLThomasDCancer Incidence in Five Continents, Volume VIII. IARC Scientific Publications No. 155. Lyon, FranceInternational Agency for Research on Cancer2002
- JemalASiegelRWardECancer statistics, 2008Ca Cancer J Clin200858719618287387
- National Cancer Institute DCCPS, Surveillance Research Program, Cancer Statistics Branch. SEER Program 17 Registries Public Use Tapes (1973–2005, varying), November 2007 Submission, Released April 2008.
- McLaughlinJKLipworthLTaroneREBlotWJRenal cancerSchottenfeldDFraumeniJFJrCancer Epidemiology and PreventionThird EditionNew York, NYOxford University Press200610871100
- MathewADevesaSSFraumeniJFJrChowWHGlobal increases in kidney cancer incidence, 1973–1992Eur J Cancer Prev20021117117811984136
- LeviFFerlayJGaleoneCThe changing pattern of kidney cancer incidence and mortality in EuropeBJU Int200810194995818241251
- JemalAThunMJRiesLAGAnnual report to the nation on the status of cancer, 1975–2005, featuring trends in lung cancer, tobacco use, and tobacco controlJ Natl Cancer Inst20081001672169419033571
- NguyenMMGillISEllisonLMThe evolving presentation of renal carcinoma in the United States: trends of the Surveillance, Epidemiology, and End Results ProgramJ Urol20061762397240017085111
- HollingsworthJMMillerDCDaignaultSHollenbeckBKRising incidence of small renal masses: a need to reassess treatment effectJ Natl Cancer Inst2006981331133416985252
- KosaryCLMcLaughlinJKKidney and renal pelvisMillerBARiesLAGHankeyBECancer Statistics Review: 1973–1990National Cancer Institute NIH Pub. No. 93–2789, 1993XlX22
- ChowWHDevesaSSWarrenJLThe rising incidence of renal cell cancer in the United StatesJAMA19992811628163110235157
- BenningtonJLLaubscherFAEpidemiologic studies of carcinoma of the kidney. I. Association of renal adenocarcinoma with smokingCancer196821106910715648044
- WynderELMabuchiKWhitemoreWFEpidemiology of adenocarcinoma of the kidneyJ Natl Cancer Inst197453161916344612162
- ArmstrongBGarrodADollRA retrospective study of renal cancer with special reference to coffee and animal protein consumptionBr J Cancer197633127136944046
- KolonelLNAssociation of cadmium with renal cancerCancer19763717821787769938
- McLaughlinJKMandelJSBlotWJSchumanLMMehlESFraumeniJFJrPopulation-based case-control study of renal cell carcinomaJ Natl Cancer Inst1984722752846582315
- YuMCMackTMHaneschRCicioniCHendersonBECigarette smoking, obesity, diuretic use, and coffee consumption as risk factors for renal cell carcinomaJ Natl Cancer Inst1986773513563461197
- GoodmanMTMorgensternHWynderELA case-control study of factors affecting the development of renal cell cancerAm J Epidemiol19861249269413776975
- BrownsonRCA case-control study of renal cell carcinoma in relation to occupation, smoking, and alcohol consumptionArch Environ Health1988432382413382249
- AsalNRRisserDRKadamaniSRisk factors in renal cell carcinoma. I. Methodology, demographics, tobacco, beverage use, and obesityCancer Detect Prev1988113593773390857
- McCredieMFordJMStewartJHRisk factors for cancer of the renal parenchymaInt J Cancer19884213163391702
- SharpeCRRochonJEAdamJMCase-control study of hydrocarbon exposures in patients with renal cell carcinomaCan Med Assoc J1989140130913182720514
- La VecchiaCNegriED’AvanzoBSmoking and renal cell carcinomaCancer Res199050523152332386932
- MaclureMWillettWA case-control study of diet and risk of renal adenocarcinomaEpidemiology199014304402090280
- TalaminiRBarónAEBarraSA case-control study of risk factors for renal cell cancer in northern ItalyCancer Causes Control199011251312102282
- PartanenTHeikkilaPHernbergSRenal cell cancer and occupational exposure to chemical agentsScand J Work Environ Health1991172312391925434
- McLaughlinJKGaoYTGaoRNRisk factors for renal cell cancer in Shanghai, ChinaInt J Cancer1992525625651399137
- KreigerNMarrettLDDoddsLRisk factors for renal cell carcinoma: results of a population-based case-control studyCancer Causes Control199341011108481488
- FinkleWDMcLaughlinJKRasgonSAIncreased risk of renal cell cancer among women using diuretics in the United StatesCancer Causes Control199345555588280833
- BenhamouSLenfantM-HOry-PaolettiCRisk factors for renal cell carcinoma in a French case-control studyInt J Cancer19935532368344750
- HiattRATolanKQuesenbergCPRenal cell carcinoma and thiazide use: a historical case-control studyCancer Causes Control199453193258080943
- WeinmannSGlassAGWeissNSUse of diuretics and other antihypertensive medications in relation to the risk of renal cell cancerAm J Epidemiol19941407928047977290
- MuscatJEHoffmnnDWynderELThe epidemiology of renal cell carcinoma: a second lookCancer199575255225577736400
- McLaughlinJKLindbladPMellemgaardAInternational renal-cell cancer study. I. Tobacco useInt J Cancer1995601941987829215
- McCredieMStewartJHRisk factors for kidney cancer in New South Wales: I. Cigarette smokingEur J Cancer199228A205020541419302
- McCredieMStewartJHRisk factors for kidney cancer in New South Wales. II. Urological disease, hypertension, obesity and hormonal factorsCancer Causes Control199233233311617119
- MellemgaardAEngholmGMcLaughlinJKRisk of renal cell carcinoma in Denmark. I. Role of socioeconomic status, tobacco use, beverages, and family historyCancer Causes Control199451051138167257
- MellemgaardANiwaSMehlESRisk factors for renal cell carcinoma in Denmark. II. Role of medication and medical historyInt J Epidemiol1994239239307860172
- MellemgaardAEngholmGMcLaughlinJKRisk of renal cell carcinoma in Denmark. III. Role of weight, physical activity, and reproductive factorsInt J Cancer19945666718262680
- MellemgaardAEngholmGMcLaughlinJKOccupational risk factors for renal cell carcinoma in DenmarkScand J Work Environ Health1994201601657973487
- ChowWHMcLaughlinJKLinetMSUse of analgesics and risk of renal cell cancerInt J Cancer1994594674707960214
- ChowWHGridleyGMcLaughlinJKProtein intake and risk of renal cell cancerJ Natl Cancer Inst199486113111398028035
- ChowWHMcLaughlinJKMandelJSObesity and risk of renal cell cancerCancer Epidemiol Biomarkers Prev1996517218770461
- SchlehoferBHeuerCBlettnerMOccupation, smoking and demographic factors, and renal cell carcinoma in GermanyInt J Epidemiol19952451577797356
- LindbladPWolkABergstromAThe role of obesity and weight fluctuations in the etiology of renal cell cancer: a population-based case-control studyCancer Epidemiol Biomarkers Prev199436316397881335
- LindbladPWolkABergstromRDiet and risk of renal cell cancer: a population-based case-control studyCancer Epidemiol Biomarkers Prev199762152239107425
- BoeingHSchlehoferBWahrendorfJDiet, obesity and risk for renal cell carcinoma: results from a case-control study in GermanyZ Ernahrungswiss1997363119095533
- YuanJMCastelaoJEGago-DominguezMHypertension, obesity and their medications in relation to renal cell carcinomaBr J Cancer199877150815139652770
- BianchiGDCerhanJRParkerASTea consumption and risk of bladder and kidney cancers in a population-based case-control studyAm J Epidemiol200015137738310695596
- PeschBHaertingJRanftUOccupational risk factors for renal cell carcinoma: agent-specific results from a case-control study in Germany. MURC Study Group. Multicenter urothelial and renal cancer studyInt J Epidemiol2000291014102411101542
- SemenzaJCZiogasALargentJGene-environment interactions in renal cell carcinomaAm J Epidemiol200115385185911323315
- HuJMaoYWhiteKOverweight and obesity in adults and risk of renal cell carcinoma in CanadaSoz Praventivmed20034817818512891869
- McLaughlinJKHrubecZHeinemanEFRenal cancer and cigarette smoking in a 26-year followup of US veteransPublic Health Rep19901055355372120735
- CoughlinSSNeatonJDRandallBPredictors of mortality from kidney cancer in 332,547 men screened for the Multiple Risk Factor Intervention TrialCancer199779217121779179064
- HeathCWJrLallyCACalleEEHypertension, diuretics, and antihypertensive medications as possible risk factors for renal cell cancerAm J Epidemiol19971456076139098177
- ChowWHGridleyGFraumeniJRJrObesity, hypertension, and the risk of kidney cancer in menN Engl J Med20003431305131111058675
- MahabirSLeitzmannMKPietinenPPhysical activity and renal cell cancer risk in a cohort of male smokersInt J Cancer200410860060514696127
- NicodemusKKSweeneyCFolsomAREvaluation of dietary, medical and lifestyle risk factors for incident kidney cancer in postmenopausal womenInt J Cancer200410811512114618625
- Van DijkBACSchoutenLJKiemeneyLALMRelation of height, body mass, energy intake, and physical activity to risk of renal cell carcinoma: results from the Netherlands Cohort StudyAm J Epidemiol20041601159116715583368
- BjorgeTTretliSEngelendARelation of height and body mass index to renal cell carcinoma in two million Norwegian men and womenAm J Epidemiol20041601168117615583369
- RashidkhaniBLindbladPWolkAFruits, vegetables and risk of renal cell carcinoma: a prospective study of Swedish womenInt J Cancer200511345145515455348
- FlahertyKTFuchsCSColditzGAA prospective study of body mass index, hypertension, and smoking and the risk of renal cell carcinoma (United States)Cancer Causes Control2005161099110616184476
- ChoiMYJeeSHSullJWThe effect of hypertension on the risk for kidney cancer in Korean menKidney Int20056764765215673312
- LindgrenAMNissinenAMTuomilehtoJOCancer pattern among hypertensive patients in North Karelia, FinlandJ Hum Hypertens20051937337915703772
- PischonTLahmannPHBoeingHBody size and risk of renal cell carcinoma in the European Prospective Investigation into Cancer and NutritionInt J Cancer200611872873816094628
- LipworthLTaroneREMcLaughlinJKThe epidemiology of renal cell carcinomaJ Urol20061762353235817085101
- McLaughlinJKLipworthLTaroneREEpidemiologic aspects of renal cell carcinomaSemin Oncol20063352753317045081
- ZucchettoADal MasoLTavaniAHistory of treated hypertension and diabetes mellitus and risk of renal cell cancerAnn Oncol20071859660017158772
- BrennanPvan der HelOMooreLETobacco smoking, body mass index, hypertension and kidney cancer risk in central and eastern EuropeBr J Cancer2008991912191519034282
- AdamsKFLeitzmannMFAlbanesDBody size and renal cell cancer incidence in a large US cohort studyAm J Epidemiol200816826827718544571
- LuoJMargolisKLAdamiHOLopezAMLessinLYeWBody size, weight cycling, and risk of renal cell carcinoma among postmenopausal women: the Women’s Health Initiative (United States)Am J Epidemiol200716675275917615089
- McLaughlinJKChowWHMandelJSInternational renal-cell cancer study. VIII. Role of diuretics, other anti-hypertensive medications and hypertensionInt J Cancer1995632162217591207
- McCredieMPommerWMcLaughlinJKInternational renal cell cancer study. II. AnalgesicsInt J Cancer1995603453497829242
- MellemgaardAOdakaNLindbladPInternational renal-cell cancer study. III. Role of weight, height, physical activity and use of amphetaminesInt J Cancer1995603503547829243
- MandelJSMcLaughlinJKSchlehoferBInternational renal-cell cancer study. IV. OccupationInt J Cancer1995616016057768630
- LindbladPChowWHChanJInternational renal-cell cancer study. V. Reproductive factors, gynecologic operations and exogenous hormonesInt J Cancer1995611921987705947
- SchlehoferBPommerWMellemgaardAInternational renal-cell cancer study. VI. The role of medical and family historyInt J Cancer1996667237268647639
- WolkAGridleyGNiwaSInternational renal-cell cancer study. VII. Role of dietInt J Cancer19966567738543399
- NoordzijMAMickischGHThe genetic make-up of renal cell tumorsUrol Res20043225125415497212
- ChoykePLGlennGMWaltherMMZbarBLinehanWMHereditary renal cancersRadiology2003226334612511666
- RickettsCWoodwardERKillickPGermline SDHB mutations and familial renal cell carcinomaJ Natl Cancer Inst20081001260126218728283
- CohenHTMcGovernFJRenal cell carcinomaN Eng J Med200535324772490
- BergstromAHsiehCCLindbladPObesity and renal cell cancer – a quantitative reviewBr J Cancer20018598499011592770
- PanSYDesMeulesMMorrisonHWenSWThe Canadian Cancer Registries Epidemiology GroupObesity, high energy intake, lack of physical activity and the risk of kidney cancerCancer Epidemiol Biomarkers Prev2006152453246017164370
- Dal MasoLZucchettoATavaniARenal cell cancer and body size at different ages: an Italian multicenter case-control studyAm J Epidemiol200716658259117591592
- RenehanAGTysonMEggerMHellerRFZwahlenMBody mass index and incidence of cancer: a systematic review and meta-analysis of prospective observational studiesLancet200837156957818280327
- CalleEEKaaksROverweight, obesity and cancer: epidemiological evidence and proposed mechanismsNature Rev Cancer2004457959115286738
- YuHRohanTRole of the insulin-like growth factor family in cancer development and progressionJ Natl Cancer Inst2000921472148910995803
- FrystykJVestboESkjaebaekCFree insulin-like growth factors in human obesityMetabolism19954437447476310
- KellererMvon EyeCHMuhlhoferAInsulin- and insulin-like growth-factor-I receptor tyrosine-kinase activities in human renal carcinomaInt J Cancer1995625015077665217
- Gago-DominguezMCastelaoJEYuanJMLipid peroxidation: a novel and unifying concept of the etiology of renal cell carcinoma (United States)Cancer Causes Control20021328729312020111
- MoyadMAObesity, interrelated mechanisms, and exposures and kidney cancerSemin Urol Oncol20011927027911769879
- PischonTNothlingsUBoeingHObesity and cancerProc Nutr Soc20086712814518412987
- FlegalKMCarrollMDOgdenCLJohnsonCLPrevalence trends in obesity among US adults, 1999–2000JAMA20022881723172712365955
- WHOObesity: preventing and managing the global epidemic. Report of a HO consultation on obesity WHO technical report series (no. 894). Geneva, SwitzerlandWorld Health Organization2000
- PanSYJohnsonKCUgnatAMAssociation of obesty and cancer risk in CanadaAm J Epidemiol200415925926814742286
- BergstromAPisaniPTenetVOverweight as an avoidable cause of cancer in EuropeInt J Cancer20019142143011169969
- VineisPAlavanjaMBufflerPTobacco and cancer: recent epidemiological evidenceJ Natl Cancer Inst2004969910614734699
- HuntJDvan der HelOLMcMillanGPRenal cell carcinoma in relation to cigarette smoking: meta-analysis of 24 studiesInt J Cancer200511410110815523697
- YuanJMCastelaoJEGago-DominguezMTobacco use in relation to renal cell carcinomaCancer Epidemiol Biomarkers Prev199854294339610793
- BenichouJChowWHMcLaughlinJKPopulation attributable risk of renal cell cancer in MinnesotaAm J Epidemiol19981484244309737554
- HajjarIKotchenTATrends in prevalence, awareness, treatment, and control of hypertension in the United States, 1988–2000JAMA200329019920612851274
- ShapiroJAWilliamsMAWeissNSHypertension, antihypertensive medication use, and risk of renal cell carcinomaAm J Epidemiol199914952153010084241
- GroveJSNomuraASeversonRKStemmermannGNThe association of blood pressure with cancer incidence in a prospective studyAm J Epidemiol19911349429471951291
- SchoutenLJvan DijkBAOosterwijkEHypertension, antihypertensives and mutations in the Von Hippel-Lindau gene in renal cell carcinoma: results from the Netherlands Cohort StudyJ Hypertens2005231997200416208141
- WeikertSBoeingHPischonTBlood pressure and risk of renal cell carcinoma in the European Prospective Investigation into Cancer and NutritionAm J Epidemiol200816743844618048375
- FryzekJPPoulsonAHJohnsenSPA cohort study of antihypertensive treatments and risk of renal cell cancerBr J Cancer2005921302130615812478
- RosenbergLStephensonWPRaoRSThe diagnosis of renal cell cancer in relation to hypertension (United States)Cancer Causes Control1998961161410189046
- McLaughlinJKBlotWJMehlESRelation of analgesic use to renal cancer: population-based findingsNCI Monogr198569213215
- DerbyLEJickHAcetaminophen and renal and bladder cancerEpidemiology199673583628793360
- RosenbergLRaoRSPalmerJRTransitional cell cancer of the urinary tract and renal cell cancer in relation to acetaminophen use (United States)Cancer Causes Control1998983889486467
- Gago-DominguezMYuanJMCastelaoJERegular use of analgesics is a risk factor for renal cell carcinomaBr J Cancer19998154254810507783
- KayeJAMyersMWJickHAcetaminophen and the risk of renal and bladder cancer in the general practice research databaseEpidemiology20011269069411679798
- BaigentCKeechAKearneyPMEfficacy and safety of cholesterol-lowering treatment: prospective meta-analysis of data from 90,056 participants in 14 randomized trials of statinsLancet20053661267127816214597
- DaleKMColemanCIHenyanNNKlugerJWhileCMStatins and cancer risk: a meta-analysisJAMA2006295748016391219
- BrowningDRLMartinRMStatins and cancer risk: a systematic review and metaanalysisInt J Cancer200612083384317131313
- KhuranaVCalditoGAnkemMStatins might reduce risk of renal cell carcinoma in humans: case-control study of 500,000 veteransUrology20087111812218242378
- DuncanREEl SohemyAArcherMCStatins and cancer developmentCancer Epidemiol Biomarkers Prev2005141897189816103434
- KarpIBehlouliHLeLorierJPiloteLStatins and cancer riskAm J Med200812130230918374689
- BlaisLDesgagneALeLorierJ3-Hydroxy-3-methylglutaryl coenzyme A reductase inhibitors and the risk of cancer: a nested case-control studyArch Intern Med20001602363236810927735
- KayeJAJickHStatin use and cancer risk in the General Practice Research DatabaseBr J Cancer20049063563714760377
- GraafMRBeiderbeckABEgbertsACRichelDJGuchelaarHJThe risk of cancer in users of statinsJ Clin Oncol2004222388239415197200
- CooganPFRosenbergLStromBLStatin use and the risk of 10 cancersEpidemiology20071821321917235211
- FarwellWRScrantonRELawlerEVThe association between statins and cancer incidence in a veterans populationJ Natl Cancer Inst200810013413918182618
- FriedmanGDFlickEDUdaltsovaNChanJQuesenberryCPHabelLAScreening statins for possible carcinogenic risk: up to 9 years of follow-up of 361,859 recipientsPharmacopidemiol Drug Safety2008172736
- WolkALindbladPAdamiHONutrition and renal cell cancerCancer Causes Control199675188850431
- YuanJMGago-DominguezMCastelaoJECruciferous vegetables in relation to renal cell carcinomaInt J Cancer1998772112169650554
- HuJMaoYWhiteKDiet and vitamin or mineral supplements and risk of renal cell carcinoma in CanadaCancer Causes Control20031470571414674734
- LeeJEGiovannucciESmith-WarnerSASpiegelmanDWillettWCCurhanGCIntakes of fruits, vegetables, vitamins A, C, and E, and carotenoids and risk of renal cell cancerCancer Epidemiol Biomarkers Prev2006152445245217164369
- BraviFBosettiCScottiLFood groups and renal cell carcinoma: a case-control study from ItalyInt J Cancer200612068168517058282
- WeikertSBoeingHPischonTFruits and vegetables and renal cell carcinoma: findings from the European Prospective Investigation into Cancer and Nutrition (EPIC)Int J Cancer20061183133313916425278
- van DijkBACSchoutenLJKiemeneyLALMGoldbohmAvan den BrandtPAVegetable and fruit consumption and risk of renal cell carcinoma: results form the Netherlands cohort studyInt J Cancer200511764865415929109
- LeeJESpiegelmanDHunterDJFat, protein, and meat consumption and renal cell cancer risk: a pooled analysis of 13 prospective studiesJ Natl Cancer Inst20081001695170619033572
- BreslowNEEnstromJEGeographic correlations between cancer mortality rates and alcohol-tobacco consumption in the United StatesJ Natl Cancer Inst1974536316394413571
- ArmstrongBDollREnvironmental factors and cancer incidence and mortality in different countries, with special reference to dietary practicesBr J Cancer197515617631
- HindsMWKolonelLMLeeJHirohataTAssociation between cancer incidence and alcohol/cigarette consumption among five ethnic groups in HawaiiBr J Cancer1980419299407426317
- SchmidtWDe LintCauses of death of alcoholicsQ J Stud Alcohol1972331711854551020
- PellSAlonzoCAA five-year mortality study of alcoholicsJ Occup Med1973151201214685423
- MonsonRRLyonJLProportional mortality among alcoholicsCancer197536107710791182660
- JensenOMCancer morbidity and causes of death among Danish brewery workersInt J Cancer197923454463437924
- AdamiHOMcLaughlinJKHsingAWAlcoholism and cancer risk: a population-based studyCancer Causes Control199234194251525322
- SchmidtWPophamREThe role of drinking and smoking in mortality from cancer and other causes in male alcoholicsCancer198147103110417226036
- LeeJEGiovannucciESmith-WarnerSASpiegelmanDWillettWCCurhanGCTotal fluid intake and use of individual beverages and risk of renal cell cancer in two large cohortsCancer Epidemiol Biomarkers Prev2006151204121116775182
- MahabirSLeitzmannMFVirtanenMJProspective study of alcohol drinking and renal cell cancer risk in a cohort of Finnish male smokersCancer Epidemiol Biomarkers Prev20051417017515668492
- RashidkhaniBAkessonALindbladPWolkAAlcohol consumption and risk of renal cell carcinoma: a prospective study of Swedish womenInt J Cancer200511784885315957170
- LeeJEHunterDJSpiegelmanDAlcohol intake and renal cell cancer in a pooled analysis of 12 prospective studiesJ Natl Cancer Inst20079980181017505075
- BagnardiVBlangiardoMLa VecchiaCCorraoGA meta-analysis of alcohol drinking and cancer riskBr J Cancer2001851700170511742491
- KabatGCNavarro SilveraSAMillerABRohanTEA cohort study of reproductive and hormonal factors and renal cell cancer risk in womenBr J Cancer20079684584917311018
- ZucchettoATalaminiRDal MasoLReproductive, menstrual, and other hormone-related factors and risk of renal cell cancerInt J Cancer20081232213221618711701
- SetiawanVWKolonelLNHendersonBEMenstrual and reproductive factors and risk of renal cell cancer in the multiethnic cohortCancer Epidemiol Biomarkers Prev20091833734019124517
- LambeMLindbladPWuuJPregnancy and risk of renal cell cancer: a population-based study in SwedenBr J Cancer2002861425142911986775
- SelikoffIJHammondECSeidmanHMortality experience of insulation workers in the United States and Canada, 1943–1976Ann NY Acad Sci197933091116294225
- EnterlinePEHartleyJHendersonVAsbestos and cancer: a cohort followed up to deathBr J Ind Med1987443964013606968
- SaliDBoffettaPKidney cancer and occupational exposure to asbestos: a meta-analysis of occupational cohort studiesCancer Causes Control200011374710680728
- McLaughlinJKRenal cell cancer and exposure to gasoline: a reviewEnviron Health Perspect Suppl1993101Suppl 6111114
- LyngeEAndersenANilssonRRisk of cancer and exposure to gasoline vaporsAm J Epidemiol19971454494589048519
- International Agency for Research on CancerOccupational exposures in petroleum refining; crude oil and major petroleum fuelsIARC Monogr Eval Carcinog Risks Hum19894539117
- WongOHarrisFSmithTJHealth effects of gasoline exposure. II. Mortality patterns among petroleum refinery workersEnviron Health Perspect1993101Suppl 663768020450
- WongOTrentLHarrisFNested case-control study of leukemia, multiple myeloma and kidney cancer in a cohort of petroleum workers exposed to gasolineOccup Environ Med19995621722110450237
- RushtonLThe UK oil refinery and distribution centre studies: a 39-year follow-upEnviron Health Perspect1993101Suppl 677848020451
- SchnatterARKatzAMNicolichMJA retrospective mortality study among Canadian petroleum marketing and distribution workersEnviron Health Perspect1993101Suppl 685998020452
- McCredieMStewartJHRisk factors for kidney cancer in New South Wales: IV. OccupationBr J Ind Med1993503493548494775
- GambleJFPearlmanEDNicolichMJA nested case-control study of kidney cancer among refinery/petrochemical workersEnviron Health Perspect19961046426508793353
- LohiJKyyronenPKauppinenTKujalaVPukkalaEOccupational exposure to solvents and gasoline and risk of cancers of the urinary tract among Finnish workersAm J Ind Med20085166867218561141
- LewisRJSchnatterARDrummondIMortality and cancer morbidity in a cohort of Canadian petroleum workersOccup Environ Med20036091892814634182
- SwenbergJALehman-McKeemanLDα2-Urinary globulin-associated nephropathy as a mechanism of renal tubule cell carcinogenesis in male ratsCapenCCDybingERiceJMSpecies differences in thyroid, kidney and urinary bladder carcinogenesis IARC Scientific Publication No. 147. Lyon, FranceInternational Agency for Research on Cancer199995117
- HenschlerDVamvakasSLammertMIncreased incidence of renal cell tumors in a cohort of cardboard workers exposed to trichloroethyleneArch Toxicol1995692912997654132
- VamvakasSBruningTThomassonBRenal cell cancer correlated with occupational exposure to trichloroetheneJ Cancer Res Clin Oncol19981243743829719500
- BruningTPeschBWiesenhutterBRenal cell cancer risk and occupational exposure to trichloroethylene: results of a consecutive case-control study in Arnsberg, GermanyAm J Ind Med20034327428512594774
- McLaughlinJKBlotWJA critical review of epidemiology studies of trichloroethylene and perchloroethylene and risk of renal cell cancerInt Arch Occup Environ Health1997702222319342621
- GreenLCLashTLRe: “Renal cell cancer correlated with occupational exposure to trichloroethylene.”J Cancer Res Clin Oncol199912543043210394965
- CherrieJWKromhoutHSempleSThe importance of reliable exposure estimates in deciding whether trichloroethylene can cause kidney cancerJ Cancer Res Clin Oncol200112740040411414201
- BlairAHartgePStewartPAMortality and cancer incidence of aircraft maintenance workers exposed to trichloroethylene and other organic solvents and chemicals: extended follow upOccup Environ Med1998551611719624267
- BoiceJDMaranoDEFryzekJPMortality among aircraft manufacturing workersOccup Environ Med19995658159710615290
- Raaschou-NielsenOHansenJMcLaughlinJKCancer risk among workers at Danish companies using Trichloroethylene: a cohort studyAm J Epidemiol20031581182119214652303
- WongOCarcinogenicity of trichloroethylene: an epidemiologic assessmentClin Occup Environ Med2004455758915325321
- BrauchHWeirichGHornauerMAStörkelSWöhlTBrüningTTrichloroethylene exposure and specific somatic mutations in patients with renal cell carcinomaJ Natl Cancer Inst19999185486110340905
- BrauchHWeirichGKleinBRabsteinSBoltHBrüningTVHL mutations in renal cell cancer: does occupational exposure to trichloroethylene make a difference?Toxicol Lett200415130131015177666
- CharbotelBGadSCaïolaDTrichloroethylene exposure and somatic mutations of the VHL gene in patients with renal cell carcinomaJ Occup Med Toxicol200721317997830
- SchramlPZhaouMRichterJAnalysis of renal tumors in trichloroethylene-exposed workers by comparative genomic hybridization and DNA sequencing analysesVerh Dtsch Ges Path19998321822410714214
- van HouweligenKPvan DijkBACHulsbergen-van de KaaCAPrevalence of von Hippel-Lindau gene mutations in sporadic renal cell carcinoma: results of the Netherlands cohort studyBMC Cancer200555715932632
- StewartJHBucciantiGAgodoaLCancers of the kidney and urinary tract in patients on dialysis for end-stage renal disease: analysis of data from the United States, Europe, and Australia and New ZealandJ Am Soc Nephrol20031419720712506152
- SatohSTsuchiyaNHabuchiTRenal cell and transitional cell carcinoma in a Japanese population undergoing maintenance dialysisJ Urol20051741749175316217276
- NeuzilletYLayFLuccioniADe novo renal cell carcinoma of native kidney in renal transplant recipientsCancer200510325125715593084