Abstract
Purpose
This study tested the logistical feasibility of obtaining data on social support systems from cancer patients enrolled on clinical trials and compared the social support of older adults (age ≥65) and younger adults (<50 years of age) with cancer.
Methods
Patients had to be eligible for a phase II or phase III oncology clinical trial and enter the study prior to treatment. Patients filled out the Lubben Social Network Scale (LSNS) at baseline. The Symptom Distress Scale (SDS) and single-item overall quality of life (QOL) Uniscale were assessed at baseline and weekly for 4 weeks.
Results
There was no significant difference in overall mean Lubben social support levels by age. Older patients had more relatives they felt close to (85% versus 53% with 5 or more relatives, P = 0.02), heard from more friends monthly (84% versus 53% with 3 or more friends, P = 0.02), less overall symptom distress (P = 0.03), less insomnia (P = 0.003), better concentration (P = 0.005), better outlook (P = 0.01), and less depression (P = 0.005) than younger patients.
Conclusions
Younger subjects reported worse symptoms, a smaller social support network, and fewer close friends and relatives than older subjects. Having someone to discuss decisions and seeing friends or relatives often was associated with longer survival.
Keywords:
Approximately 10.1 million individuals in this country have a history of cancer and 1,372,910 new individuals were diagnosed in the year 2006. The prevalence of cancer is about 13% in patients 18–49 and about 60% in ages 65 or over.Citation1 Receiving a cancer diagnosis affects individuals in a multitude of ways. It is critical for cancer patients to have support, especially in light of the fear and social ‘stigma’ of cancer.Citation2 The availability of support may decrease as a result of these issues and social networks of older people tend to be smaller than those of younger individuals.Citation3,Citation4 In previous studies in noncancer cohorts, better social support has been linked to longer survival times,Citation5,Citation6 lower hospitalization rates,Citation7 better adjustment after diagnosis of disease,Citation8 and better retention of cognitive function.Citation9 More research is needed on the impact of social networks among cancer patients.
Studies have reported the positive effects of social support at the time of diagnosis and during adaptation to the disease.Citation10–Citation16 Conversely, cancer patients with diminished emotional support report more symptoms and lower QOL.Citation14,Citation17 Cancer patients have unique social support issues. For them, support from a spouse, immediate family, and peers are critical.Citation15,Citation18 The fear associated with cancer diagnosis and treatment increase the need for support,Citation14,Citation19 while at the same time the social stigma of having cancer can decrease the availability of support when it is most needed.Citation14,Citation20,Citation21 Social support models must be tailored to fit the specific needs of the individual because social support needs vary by treatment and stage of disease.Citation11,Citation14,Citation16,Citation22
The primary goal of this pilot study was to gain experience with assessing social support in cancer patients. This experience will lead to further studies of social networks in this cohort. The research hypotheses for this study were that the level of social support diminishes with age and has an impact on secondary goals. These secondary goals included symptoms captured by the SDS, mortality, and overall QOL.
Methods
Study design
The present study was a prospective, non-randomized cohort design. The accrual goal was 30 patients in each group. This sample size would provide 80% power to detect a difference of 0.7 of a standard deviation between the two groups. This effect size is considered a moderate to large effect size.Citation23 Completion rates were calculated, with 80% completeness as a criterion for acceptability for further study.
Patients
This study was approved by the Mayo Foundation Institutional Review Board and participants provided informed consent. Patients had to be eligible for a Mayo phase II or III oncology clinical trial and had to be enrolled on this study prior to starting treatment for their primary malignant disease. Two groups of patients were entered on this study. Patients at least 18 years old and less than 50 years old were entered into a group considered young cancer patients, and patients at least 65 years old were entered into a group considered older adults. These two age groupings were selected to maximize the potential to demonstrate the effects of age on social support. Patients were enrolled between 7/16/1999 and 01/11/2002. Accruing younger patients proved more difficult than expected, given the lower incidence rate of cancer in younger adults. Nationally, only about 13% of cancer patients are under the age of 50.24 At our institution, about twice as many patients age 65 or older go on phase II or III studies compared to patients less than age 50. Accrual for this younger cohort was stopped at 20 because of the slow accrual rate.
Measures
Lubben social network scale
The Lubben Social Network Scale (LSNS) is a validated self-reported 10 item scale measuring embedded support, perceived support, and the reciprocation of support.Citation25–Citation28 All 10 items are highly intercorrelated (Cronbach’s alpha = 0.70).Citation29,Citation30 Each question was scored on a zero to five scale with high scores indicating more social support. The overall LSNS social support score was calculated for each patient by summing the 10 questions. The LSNS was assessed at baseline before the patient started their cancer treatment. Our group recently used this same scale in a retrospective analysis of two lung cancer clinical trials to successfully demonstrate a lack of gender effect in social support among elderly patients.Citation31 Differences in the individual LSNS questions were also analyzed.
The uniscale overall quality of life scale
The UniscaleCitation32 tool used in this study was a single item visual analogue. Patients mark an ‘X’ along a bar to indicate their overall QOL. The bar ranges from ‘LOWEST QUALITY’ on the left side of the bar to ‘HIGHEST QUALITY’ on the right side of the bar. The patient’s score is the measured distance from the left of the bar to the ‘X’ divided by the total length of the bar times 100. Scores then range from 0 to 100 with 100 being the best possible score. The UNISCALE has been validated in cancer clinical trials.Citation33 The Uniscale was assessed at baseline (before the start of treatment) and weekly for the remaining four weeks of the study.
The symptom distress scale
The Symptom Distress Scale (SDS)Citation34 is a reliable and validated, self-reported 13-item questionnaire designed to identify physical and psychosocial symptoms of concern to patients and the degree of distress associated with each symptom. The scale has demonstrated convergent validity with the MOS-SF36 and discriminant validity has been established.Citation35 The SDS was assessed at baseline (before the start of treatment) and weekly for the remaining four weeks of the study. For this and for all other patient-reported outcomes we translate scores onto a 0–100 point scale, where appropriate, so that higher scores always mean a positive indication for the patient (less pain or symptom distress, better quality of life).
Analysis plan
This prospective study compared social support, symptoms and QOL between the cohort of younger patients and the cohort of older patients. Secondary analyses included testing for gender differences. Fisher’s exact tests were used to test for differences in discrete variables between groups. Kruskal-Wallis tests were used to test differences in continuous variables between the two age groups, Kaplan-Meier curves and log-rank tests were used to compare survival between the groups, and Spearman correlations were used to determine associations between social support and symptoms. Changes in symptoms and QOL over time were tested by applying t-tests to the differences between baseline and week 4 values.
Results
Demographics
shows baseline demographics between the older and younger cohort. The baseline demographics were similar between the two groups. Almost all (93%) of the patients had late stage cancer.
Table 1 Baseline characteristics by age group
LSNS form completion
During this 3-year period, 52 patients were enrolled in this study. Two patients did not provide any baseline information. Out of the 50 patients with baseline information, 41 (82%) filled out the LSNS. This completion percentage was sufficient to recommend the use of the LSNS in future studies of this patient population.
Age differences in social support networks
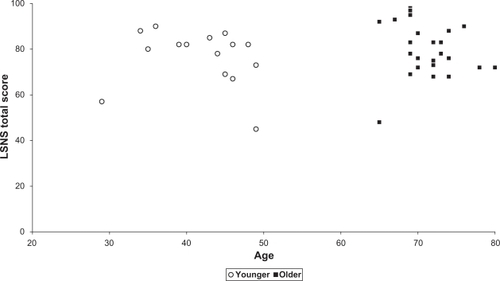
and show LSNS by age group. There was no significant difference in overall mean LSNS by age (76.4 for younger patients, 80 for older patients, P = 0.49). However, contrary to the pre-study hypothesis, younger patients had lower levels of social support than older patients on individual Lubben questions. Patients in the younger group were more likely relied on by others on a daily basis (69% vs 35%, P = 0.04). Despite having advanced cancer, the younger patients had the added stress of being responsible for others. Patients ≥65 years of age had more relatives they felt close to (85% vs 54% with >4 relatives, P = 0.017) and more friends they heard from monthly (85% vs 54% with >2 friends, P = 0.016).
Table 2 Lubben Social Network Scale levels by age group
Figure 1 Age by total Lubben Social Network Scale (LSNS) score. Spearman correlation = −0.05 (P = 0.78).
Age differences in symptoms
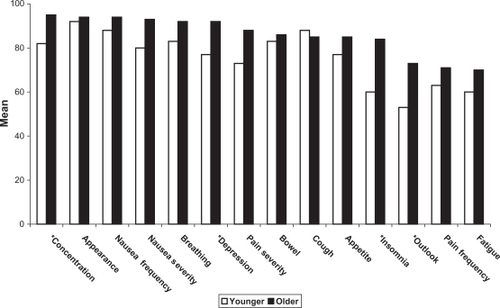
shows that older patients reported fewer symptoms than the younger patients. Older patients reported less overall symptom distress (mean of 86 vs 77, P = 0.03), less insomnia (11% vs 47% with frequent trouble sleeping, P = 0.003), better concentration (81% vs 40% with their normal ability to concentrate, P = 0.005), better outlook (86% vs 40% with little or no worries, P = 0.01), and less depression (74% vs 27% seldom feel depressed, P = 0.005).
Figure 2 Mean baseline symptoms by age group.
*Indicates significant differences at P <0.05.
Social support levels and symptoms by gender
There were no significant differences in overall social support levels by gender (mean overall LSNS scores of 81 for females vs 77 males, P = 0.40). However, females were more likely to see close relatives daily (70% vs 19%, P = 0.0027) and were more likely to have other people discuss their problems with them (60% of women reported “very often” or “always” compared to only 25% of men, P = 0.02). Women reported more overall symptom distress at baseline (mean overall SDS score of 78 vs 86 for men, P = 0.02) and a higher frequency of SDS pain (10% of women almost never had pain vs 59% of men, P = 0.005).
Age dfferences in QOL
There were no statistically significant differences in baseline quality of life or changes in quality of life by age group or gender.
Age differences in survival
There were no statistically significant differences in survival times by age group (log-rank P = 0.98). There was no a survival difference even after adjusting for stage of disease and gender (Cox model P = 0.60).
Social support and survival
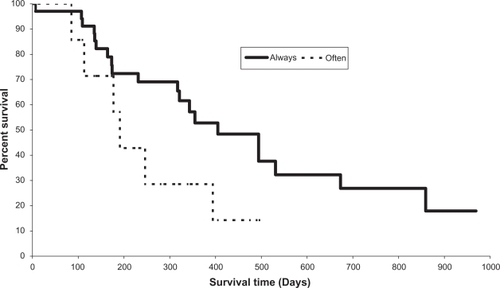
Due to the small sample size and the lack of a survival difference, the two age cohorts were combined to explore the relationship between social support and survival. Some levels of the LSNS questions were also combined because of the sparse responses in some levels. As shown in , always having someone to talk to about decisions was a significant predictor for survival even after adjusting for age and gender (Cox proportional hazard P = 0.01, hazard ratio = 0.31, 95% confidence interval for the odds ratio of 0.002 to 0.492). For this analysis, patients with responses of ‘often’ and ‘very often’ were combined and compared to patients responding with ‘always’.
Figure 3 Overall survival by having someone to discuss issues.
Correlations between social support and symptoms
There was a modest correlation between symptoms and how often they saw their closest friend (−0.50 correlation with overall SDS, and 0.51 correlation with fatigue).
Changes in symptoms and QOL over time
There were no significant differences in the changes in symptoms or QOL over time by age group. The combined cohort of patients in both age groups showed a significant decrease in QOL over time (mean decrease of 7.9, P = 0.02), a decrease in pain frequency (mean improvement of 0.4, P = 0.02), and a decrease in SDS outlook (mean decrease −0.3, P = 0.04).
Discussion
Social support networks are important factors in the health of the elderly.Citation36,Citation37 Better social support networks have been linked with patient survival, overall health, their ability to carry out routine daily tasks, and their ability to cope with major life events and disease.Citation5,Citation38–Citation40 Patients can become very isolated after a cancer diagnosis due to the social stigma associated with cancer, but this is the time these patients need the most support, and their level of support is associated with outcome. Recent evidence has emerged that both supports the importance of social networks on healthCitation41,Citation42 and challenges the notion that older adults are more isolated.Citation43
This study suggests there may be a generational gap in the level of social support experienced by cancer patients. In this study, younger patients tended to have smaller support networks and fewer close friends. Younger patients also reported higher levels of symptoms. These results were in perfect opposition to our research hypothesis. The reasons for these results should be explored further. It is possible that the younger patients do not have a spouse or partner to lean on or their parents or other family members around for support. Their friends are younger and may be busy with their own careers and families. The rapid growth of internet social networks may also have resulted in an increase in the size of social networks, but a decrease in face-to-face social skills and therefore less direct social networking among younger adults. The effects of internet networking on cancer patients, requires further investigation. It is also possible that older patients had developed social networks as they aged in response to previous illness and disability and that these established social networks were maintained. Younger patients would be less likely to have developed and maintained similar social networks. The younger patients also were more likely to be relied on by others on a daily basis. This likely meant the patients had the added burden of dealing with how their cancer will affect their young children or a spouse.
Age group and gender were not significant factors for survival in this study. These results are not terribly surprising in that the impact of age groupCitation44,Citation45 and genderCitation46,Citation47 on survival is variable across patient populations and clinical studies. However, there was some evidence that having someone to discuss decisions with and being able to see friends and relatives often was linked to longer survival. This is an intriguing result that requires further investigation.
This study suggests that cancer patients may benefit from a system that fosters positive, supportive social networks. Social networking with close trusted friends and relatives should be encouraged, as these interactions promote improved quality of life and longer survival. Cancer health providers should be aware of the potential for social isolation and its effects on cancer patients.Citation48 Future interventions could include screening for insufficient social networks, enhancing and encouraging existing social networks, and connecting isolated patients to potential social links. The quality of these social networks also needs to be considered. Social supports need to be positive, supportive and tailored to the individual.
A methodological note from this study indicates that the LSNS was easy for participants to complete and provided reasonably detailed data on the relative well-being of patient social networks. In particular, the use of individual item analysis provided supplementary insights that could not be garnered from the total score. This is a phenomenon that has been seen in other studies and is a particular focus of the research program of the senior author.Citation49,Citation50 These findings have supported the examination of results for individual items within a summated score since changes in individual items may be lost among the summated scores of multi-item assessments.
A limitation of this study is that the patients were all from cancer clinical trials. Patients going on clinical trials are only a small fraction of all cancer patients and they may have higher levels of support than other patients. Higher levels of support are likely needed for patients on clinical trials to support the extra trips and expenses. The findings may be magnified in patients not able to participate in a clinical trial.
Future research
The data suggest that social networks can be successfully evaluated in cancer patients. More definitive studies are needed into the differences in social support networks between age groups, the impact of social networks on patient outcomes, and the impact of identifying and alleviating social isolation. Future plans include testing an intervention targeted at improving social networks in patients identified as having low social support. A “menu” of support services will be assembled by the investigators and provided to patients to see if patients that receive structured, active encouragement and information from an enhanced social network will report higher QOL, fewer symptoms, and improved toxicity profiles. Future studies will also include patients in the middle age group (50 to 64).
Acknowledgment of financial support
This study was conducted as a collaborative trial of the Mayo Clinic and was supported in part by Public Health Service grants CA-25224, CA-37404, CA-63848, CA-63849, and CA-35195. The authors report no conflicts of interest in this work.
Disclosures
The authors report no conflicts of interest in this work.
References
- Surveillance, Epidemiology, and End Results (SEER) Program (www.seer.cancer.gov). Prevalence database: “US Estimated 29-Year L-D Prevalence Counts on 1/1/2004 by Duration”. National Cancer Institute, DCCPS, Surveillance Research Program, Statistical Research and Applications Branch, released 2007, based on the 2006 SEER data submission.
- ChappleAZieblandSMcPhersonAStigma, shame, and blame experienced by patients with lung cancer: qualitative studyBMJ2004 J3287454147015194599
- NorbeckJSSocial Support: A model for clinical research and applicationAdv Nurs Sci1981344359
- RyanLSPsychosocial issues and lung cancer: A behavioral approachSemin Oncol Nurs19961243183238936648
- CeriaCDMasakiKHRodriguezBLChenRYanoKCurbDThe relationship of psychosocial factors to total mortality among older Japanese-American men: The Honolulu Heart ProgramJ Am Geriatr Soc200149672573111454110
- RutledgeTMatthewsKLuiLYStoneKLCauleyJASocial networks and marital status predict mortality in older women: prospective evidence from the Study of Osteoporotic Fractures (SOF)Psychosom Med200365468869412883123
- MistryRRosanskyJMcGuireJMcDermottCJarvikLUPBEAT Collaborative Group. Social isolation predicts re-hospitalization in a group of older American veterans enrolled in the UPBEAT Program. Unified Psychogeriatric Biopsychosocial Evaluation and TreatmentInt J Geriatr Psychiatry2001161095095911607938
- NosartiCRobertsJVCrayfordTMcKenzieKDavidASEarly psychological adjustment in breast cancer patients: a prospective studyJ Psychosom Res20025361123113012479995
- CrooksVCLubbenJPetittiDBLittleDChiuVSocial network, cognitive function, and dementia incidence among elderly womenAm J Public Health20089871221122718511731
- BakerACThe spouse’s positive effect on the stroke patient’s recoveryRehabil Nurs199318130338430261
- CarlssonJHamrinEPsychological and psychosocial aspects of breast cancer treatment. A literature reviewCancer Nurs19941754184287954390
- DowKHA review of late effects of cancer in womenSemin Oncol Nurs19951121281367604191
- SuominenTLeino-KilpiHLaippalaPWho provides support and how? Breast cancer patients and nurses evaluate patient supportCancer Nurs19951842782857664255
- AkechiTOkamuraHYamawakiSPredictors of patients’ mental adjustment to cancer: patient characteristics and social supportBr J Cancer19987712238123859649163
- GuidryJJAdayLAZhangDThe role of informal and formal social support networks for patients with cancerCancer Pract1997542412469250081
- HelgesonVSCohenSSocial support and adjustment to cancer: reconciling descriptive, correlational, and interventional researchHealth Psychol19961521351488681922
- CourtensAMStevensFCCrebolderHFLongitudinal study on quality of life and social support in cancer patientsCancer Nurs19961931621698674024
- KaplanKMWeinbergGBSmallABreast cancer screening among relatives of women with breast cancerAm J Public Health1991819117411791951830
- LugtonJThe nature of social support as experienced by women treated for breast cancerJ Adv Nurs1997256118411919181415
- Dunkel-SchetterCWortmanCThe interpersonal dynamics of cancer: Problems in social relationships and their impact on the patientsFriedmanHSDiMatteoMRInterpersonal Issues in Health CareNew YorkAcademic Press198269100
- KrishnasamyMSocial support and the patient with cancer: a consideration of the literatureJ Adv Nurs19962347577628675894
- BottomleyAJonesLSocial support and the cancer patient-A need for clarityEur J Cancer Care1997617277
- CohenJStatistical Power Analysis for the Behavioral Sciences2nd EditionLawrence Erlbaum Associates, IncHillsdale, New Jersey1988
- National Cancer Institute http:/seer.cancer.gov/faststats.
- LubbenJEFamily and Community Health19881134252
- LubbenJGirondaMMeasuring social networks and assessing their benefitsSocial Networks and Social Exclusion: Sociological and Policy PerspectivesPhillipsonAllanMorganAshgate2004
- LubbenJEAssessing social networks among elderly populationsJournal of Family and Community Health1988114252
- LubbenJEWeilerPGChiIHealth practices of the elderly poorAm J Public Health19897967317342658629
- NahmEResnickBGainesJTesting the reliability and validity of computer-mediated social support measures among older adults: A pilot studyComput Inform Nurs200422421121915494651
- YuDSFLeeDTFWooJPsychometric testing of the Chinese version of the Medical Outcomes Study Social Support Survey (MOS-SSS-C)Res Nurs Health200427213514315042639
- JatoiAHillmanSLAllen ZieglerKLStellaPJSooriGSRowlandKMJrIs social support associated with improved clinical outcomes in geriatric lung cancer patients? Observations from North Central Cancer Treatment Group Studies N9921 and N0222Cancer Manag Res200916168
- SpitzerWODobsonAJChestermanEMeasuring the quality of life of cancer patients: a concise QL-index for use by physiciansJ Chronic Dis198134125855977309824
- SloanJALoprinziCLKurossSARandomized comparison of four tools measuring overall quality of life in patients with advanced cancerJ Clin Oncol19981611366236739817289
- McCorkleRYoungKDevelopment of a symptom distress scaleCancer Nurs197815373378250445
- MoinpourCMFeiglPMetchBQuality of life end points in cancer clinical trials: review and recommendationsJ Natl Cancer Inst19898174854952646455
- LubbenJGirondaMCentrality of social ties to the health and well-being of older adultsBerkmanBHarootyanLSocial Work and Health Care in an Aging SocietySpringer Publishing Company2003
- TremethickMJThriving, not just surviving. The importance of social support among the elderlyJ Psychosoc Nurs Ment Health Serv199735927319298462
- RubinsteinRLLubbenJEMintzerJESocial isolation and social support: And applied perspectiveJ Appl Gerontol19941315872
- HouseJSWork, Stress, and Social SupportAddision Wesley, ReadingMassachusetts1981
- Mor-BarakMEMillerLSA longitudinal study of the causal relationship between social networks and health of the poor frail elderlyJ Appl Gerontol199110329331010113726
- CacioppoJTHawkleyLCSocial isolation and health, with an emphasis on underlying mechanismsPerspect Biol Med2003463 SupplS39S5214563073
- CacioppoJTHughesMEWaiteLJHawkleyLCThistedRALoneliness as a specific risk factor for depressive symptoms: crosssectional and longitudinal analysesPsychol Aging200621114015116594799
- CornwellEYWaiteLJMeasuring social isolation among older adults using multiple indicators from the NSHAP studyJ Gerontol Social Sciences200964BS1i38i46
- DomingoESurinachJMMurilloJPrognostic factors in the diagnostic work-up of cancer patients in an internal medicine department: does age matter?Int J Clin Pract200862111723172919143858
- LeviFRandimbisonLVecchiaCLBreast Cancer Survival in Relation to Sex and AgeOncology19924964134171465277
- International Early Lung Cancer Action Program InvestigatorsHenschkeCIYipRMiettinenOSWomen’s susceptibility to tobacco carcinogens and survival after diagnosis of lung cancerJAMA2006296218018416835423
- HendifarAYangDLenzFGender Disparities in Metastatic Colorectal Cancer SurvivalClin Cancer Res200915206391639719789331
- TremethickMJAlone in a crowd: A study of social networks in home health and assisted livingJ Gerontol Nurs2001275424711915274
- SloanJAAaronsonNCappelleriJCAssessing the clinical significance of single items relative to summated scoresMayo Clin Proc200277547948712004998
- SloanJABerkLRoscoeJNational Cancer Institute. Integrating patient-reported outcomes into cancer symptom management clinical trials supported by the National Cancer Institute-sponsored clinical trials networksJ Clin Oncol200725325070507717991923