Abstract
Acute exacerbations of COPD can complicate the course of the disease in patients with severe airway obstruction. Reduction of exacerbations is an important clinical outcome in evaluating new therapies in COPD. Combination therapies with long-acting β-agonists and inhaled corticosteroids have now been approved for use. Three 1-year randomized clinical trials, which studied the effect of combining a long-acting β2-agonist with an inhaled corticosteroid in COPD, documented that exacerbation frequency was lower with therapy than placebo. Combination therapy had a similar effect to its monocomponents in the trial evaluating salmeterol/fluticasone combination. However, when patients with more severe COPD were studied using a combination of budesonide and formoterol, a clear improvement was seen in the overall exacerbation rates compared with the use of a long-acting β2-agonist alone.
Introduction
Acute exacerbations of COPD are characterized by a change in cough, sputum production, and respiratory symptoms from baseline that cause the patient to seek medical attention and involve increasing the dose and/or frequency of existing bronchodilator therapy. Systemic corticosteroids are also recommended in patients with more advanced COPD that may require hospitalization. Exacerbations may be mild, necessitating only outpatient therapy such as antibiotics and/or systemic steroids but often may be severe enough to require hospitalization and admission to the intensive care unit. Therefore, prevention of exacerbations is one of the most important goals of chronic obstructive pulmonary disease (COPD) management (CitationGlobal Initiative for Chronic Obstructive Lung Disease 2005) because of the impact on patients’ daily activities and health-related quality of life (HRQoL), with these effects lasting for several weeks or months (CitationHaughney and Gruffydd-Jones 2004). Frequent exacerbations also lead to a poorer recovery in terms of improvement in health status (CitationHaughney and Gruffydd-Jones 2004). Furthermore, the frequency of acute exacerbation has a significant impact on the accelerated decline of lung function (CitationDonaldson et al 2002) and also on healthcare costs (CitationHaughney and Gruffydd-Jones 2004). Consequently, strategies for preventing COPD exacerbations may have an important effect on the natural course, cost of management, and mortality in COPD (CitationMartinez and Anzueto 2005).
In recent years, several large-scale clinical trials in COPD have analyzed the exacerbation-preventing aspects of different treatments (Niewoehner 2004; CitationSolèr 2005). These include inhaled bronchodilators, inhaled corticosteroids (ICSs), and a limited number of antimicrobial strategies. However, most antimicrobial strategies have been used therapeutically in the form of antibiotic treatment during an established exacerbation, apart from vaccinations against influenza and pneumococci, which can protect from these infections which are particularly dangerous for COPD patients (CitationCazzola et al 2005).
Effect of long-acting β2-agonists and inhaled corticosteroid in preventing COPD exacerbations
Long-acting β2-agonists (LABAs) have both bronchodilator and non-bronchodilator properties, whereas ICSs are potent anti-inflammatory agents (CitationCazzola and Dahl 2004). It is, therefore, obvious that LABAs and ICSs treat different aspects of COPD (CitationCazzola and Dahl 2004). LABAs are central in the symptomatic control of COPD (CitationAmerican Thoracic Society/European Respiratory Society 2005), whereas conflicting results have been reported with ICSs (CitationBarnes 2000; CitationCalverley 2000). This may reflect the fact that the inflammation in COPD is poorly suppressed by corticosteroids, with small reduction in inflammatory cells, cytokines, or proteases in induced sputum even with oral corticosteroids (CitationBarnes 2004), although there are some subgroups of patients (eg, those with eosinophilia) who respond very well (CitationChanez et al 1997).
Nonetheless, findings from several clinical studies have shown that treatment with ICSs improve expiratory airflow and reduce symptoms and the rate of exacerbations associated with COPD (CitationAlsaeedi et al 2002), and, moreover, reduce all-cause mortality in COPD (CitationSin et al 2005). ICSs in relatively high doses (eg, budesonide 800 μg/day or fluticasone propionate 1 mg/day) reduce exacerbations by 20%–30% and improve the health status of COPD patients by a similar amount compared with placebo (CitationMan and Sin 2005). In particular, a meta-analysis of six trials, which evaluated the long-term effects (≥ 6 months) of ICSs in stable COPD and provided information about total exacerbations, demonstrated that ICSs reduce exacerbation rates in COPD by nearly one third relative to placebo (relative risk [RR], 0.70; 95% CI, 0.58–0.84) (CitationAlsaeedi et al 2002). In the ISOLDE (Inhaled Steroid in Obstructive Lung Disease in Europe) study, the major benefit of therapy was seen in those whose lung function was less than 50% of predicted; however, the number of patients having at least one exacerbation per year was reduced with ICSs irrespective of baseline lung function (CitationJones et al 2003). A convincing demonstration of the effectiveness of these agents in COPD patients has come from the COPE study (an investigation of COPD in the Department of Pulmonology, Enschede, the Netherlands) (Citationvan der Valk et al 2002). This study showed that the discontinuation of therapy with ICSs was associated with a more rapid onset and a higher risk of recurrence of exacerbations, and with a significant deterioration in aspects of HRQoL, in the majority of patients. However, 40% of subjects in the COPE study experienced no untoward effect from the withdrawal of ICSs. This finding indicates that there is an urgent need to identify which subgroups of COPD patients respond well to prolonged ICSs therapy. In any case, a recent article that has reviewed the diverse approaches to data analysis used in the randomized trials of ICSs in the treatment of COPD and their meta-analysis, has concluded that the reports that ICSs reduce COPD exacerbation rates are the result of improper statistical analysis techniques (CitationSuissa 2006). The only two studies that used the correct statistical approach found insignificant effects with these drugs. It is not a surprise, therefore, that the evaluation of a cohort of newly treated COPD patients formed from the Administrative Databases of Saskatchewan Health documented that ICSs do not seem to be beneficial in preventing the risk of a first exacerbation of COPD (Citationde Melo et al 2004). Interestingly, a recent paper has documented that immortal time bias cannot account for the risk reduction associated with ICSs exposure in observational studies (CitationKiri et al 2005). This finding is strengthened by the observed relationship between increased regularity of ICSs prescriptions and reductions in event rates.
Although LABAs have been shown to reduce exacerbation rates of COPD, the magnitude of the effect appears modest at best. Published trials reveal that salmeterol is the only LABA with a significant effect on the rate of exacerbations. In a 1-year study comparing salmeterol with placebo, salmeterol significantly reduced the mean number of exacerbations per patient by 20% and the mean number of exacerbations requiring oral corticosteroids per patient by 29% (CitationCalverley et al 2003a). Recently, it has been documented that the addition of salmeterol to existing treatment in patients with a history of COPD exacerbations and poor reversibility of airflow obstruction reduces exacerbations in patients who comply with treatment (CitationStockley et al 2006). On the contrary, formoterol, in twice daily doses, failed to show such an effect in two other trials (CitationCalverley et al 2003b; CitationSzafranski et al 2003), although a subsequent study has documented that it can influence exacerbation surrogates, for example “bad days” (CitationDahl et al 2002). Salmeterol has been shown in several model systems to reduce inflammatory cell activation, to reduce formation of edema and to enhance edema clearance, and to mitigate epithelial damage induced by bacteria (CitationRennard 2004). Whether these effects have any clinical importance remains to be determined, but they may account for its ability to reduce frequency of exacerbations of COPD. Formoterol may have similar non-bronchodilator effects; however, studies are needed to document these effects.
Pharmacological rationale for combining long-acting β2-agonists and inhaled corticosteroid in COPD
Interaction at the molecular level between ICSs and LABAs
Combining two therapies that possess different modes of action could be expected to have a greater benefit in the management of COPD. There is an exciting possibility that the potential benefit in combining ICSs and LABAs might be due to a synergistic interaction. However, the basic molecular mechanism of such an interaction has still to be fully identified. Recent in vitro and in vivo evidence suggest a mechanistic interaction at the molecular level between ICSs and LABAs. Corticosteroids have been shown to up-regulate the β2-adrenoceptor in the human airways, which in turn may provide more receptors for β2-agonists to activate (CitationMak et al 1995; CitationBaraniuk et al 1997). At the same time, LABAs may potentiate the molecular mechanism of corticosteroid actions by increasing the nuclear translocation of glucocorticoid receptors (GRs) and thus causing an additive or sometimes synergistic suppression of inflammatory mediator release (CitationEickelberg et al 1999; CitationKorn et al 2001; CitationPang and Knox 2000, Citation2001). Similar interactions between ICSs and LABAs in vivo are a likely explanation for the effects seen in the study of CitationBarnes and coworkers (2006) documenting that the combination of inhaled salmeterol and fluticasone propionate significantly reduced the absolute numbers of biopsy (CD45+) leukocytes, CD8+ cells, and CD4+ cells together with decreases in cells expressing genes for the proinflammatory mediators IFN-γ and TNF-α. In the complementary airway compartment sampled by induced sputum, combination treatment significantly reduced sputum differential neutrophils and total eosinophils. Furthermore, in vitro studies suggest that the addition of a LABA to an ICS may counter some of the potential negative effects of the corticosteroid (CitationTse et al 2003) or alternatively, some of those elicited by LABA (CitationSeeto et al 2003).
Increasing compliance
In addition to the complementary interaction of LABAs and ICSs at the molecular level, the delivery of these medications together in a single device may also help simplify treatment regimens and improve patient adherence (CitationCazzola and Dahl 2004). It is widely recognized that adherence to treatment of chronic obstructive airways diseases declines as the regime becomes more complicated, either by increasing the number of medications and/or the number of daily doses (CitationCoutts et al 1992; CitationChapman et al 2000). As a result, improved compliance would be expected to occur through the use of a single combination inhaler simply because of the reduction in the number of medications and actuations required with such a regime. In particular, it would be expected that the use of combination therapy should improve compliance with ICS therapy as its use is linked with LABA therapy, which patients are more likely to take because of the greater symptomatic benefit.
Enhanced respiratory cytoprotection against viral and bacterial infection
Because of the above effects, it is not unexpected that long-term use of ICSs with LABAs may be associated with a reduction in COPD exacerbations (CitationCazzola and Dahl 2004). However, the capacity of both ICSs and LABAs to reduce the total number of bacteria adhering to the respiratory mucosa in a concentration-dependent manner without altering the bacterial tropism for mucosa, and to preserve ciliated cells, is important in this context (CitationDowling et al 1999). ICSs and LABAs, when administered together at low concentrations, exhibited a synergistic effect with respect to the preservation of ciliated cells, showing a trend toward reduced damage and a significant preservation of the number of ciliated cells compared with either agent alone at the same concentrations. This result may have clinical significance as it is thought that ciliated cells are the most sensitive to damage by bacterial infection (CitationTsang et al 1994). It is well-known that airway colonization and chronic infection contribute to progressive pulmonary damage in COPD patients via the action of proinflammatory substances in what is known as the “vicious circle theory” (CitationWilson 1991). Recently, the synergistic effects of salmeterol and fluticasone in human rhinovirus-induced proinflammatory cytokine production have also been documented (CitationEdwards et al 2006). Rhinoviruses are implicated in many acute exacerbations of COPD, perhaps by inducing proinflammatory cytokines (CitationSeemungal et al 2001).
Effect of combination therapy in preventing COPD exacerbations
The efficacy of combination therapy with ICSs and LABAs delivered via a single inhaler to COPD patients has repeatedly been documented (). In particular, the impact on acute exacerbations of long-term treatments with combined therapy is shown in and , and . It is very important to also mention that the definition of exacerbation and the patient population enrolled in these studies are not uniform (), and these facts have to be taken in consideration when analyzing their results.
Table 1 Long-term effect of combination therapy in COPD
Table 2 Absolute and relative risk reductions for exacerbations of COPD requiring medical intervention with number needed to treat in three randomized and double-blind multinational trials
Table 3 Definitions of COPD exacerbation used in combination therapy studies
Figure 1 Total severe exacerbation rate.
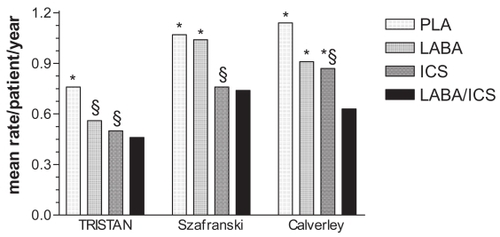
Notes: PLA, placebo; LABA, salmeterol 50 μg bid or formoterol 12 μg bid; ICS, fluticasone propionate 500 μg bid or budesonide 400 μg bid; LABA/ICS, salmeterol 50 μg/fluticasone 500 μg bid or formoterol 12 μg/budesonide 400 μg bid. * difference between combination treatment and single compound treatment and/or PLA statistically significant (p<0.05); § difference between single compound treatment and PLA statistically significant (p<0.05). Data from CitationCalverley et al 2003a (TRISTAN); CitationCalverley et al 2003b; CitationSzafranski et al 2003.
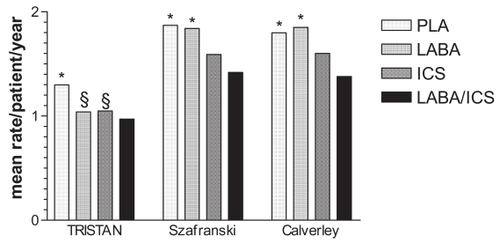
Figure 2 Rate of exacerbations requiring oral corticosteroids.
In a multicenter, randomized, placebo-controlled study, CitationHanania et al (2003) compared the efficacy and safety of fluticasone propionate (250 μg) and salmeterol (50 μg), when administered twice daily together in a single device for 6 months, with that of placebo and the individual agents alone in patients with COPD. This study was unable to observe significant differences among treatment groups in the number of exacerbations or the time to first exacerbation. However, this study was of short duration and was designed and powered to evaluate the treatment effect on FEV1, which was the primary measure of efficacy, rather than to evaluate the rates of exacerbations.
In a study with a similar design but evaluating the higher dose formulation of this combination therapy, fluticasone propionate (500 μg) with salmeterol (50 μg) twice daily given for 6 months (CitationMahler et al 2002), there were no statistically significant differences between treatment groups in time to exacerbation. This study also demonstrated no difference in the number of participants who exacerbated once (placebo: 8.8%; salmeterol: 5.6%; fluticasone: 10.1%; fluticase/salmeterol combination [FSC]: 8.5%), but no p values were presented. Also this study was of short duration and was designed and powered to evaluate the treatment effect on FEV1, which was the primary measure of efficacy, rather than to evaluate the rates of exacerbations.
The TRISTAN study (CitationCalverley et al 2003a), a randomized controlled trial over 1 year of combination treatment with salmeterol (50 μg) and fluticasone (500 μg) administered together in a single device twice daily versus each of the components alone and versus placebo, enrolled patients with a baseline FEV1 before bronchodilation that was 25%–70% of that predicted. In this study, the rate of exacerbations requiring medical intervention, defined as a worsening of COPD symptoms that required treatment with antibiotics or oral corticosteroids, or both, fell by 25% in the combination group and by 20% and 19% in the salmeterol and fluticasone groups, respectively, compared with placebo. In particular, there was a significant difference in the mean exacerbation rate per participant per year in favor of the combination therapy when compared with placebo (FSC: 0.97 vs placebo: 1.30, p<0.0001), but, interestingly, differences among the three active treatment arms were small and not statistically significant. The treatment effect was more pronounced in patients with severe disease (ie, a baseline FEV1 <50% of predicted), who showed a 30% reduction with combination therapy compared with placebo, compared with a 10% reduction in patients who had a baseline FEV1 greater than 50% of predicted. However, this beneficial effect was also seen for exacerbations treated with oral corticosteroids, which have conventionally been thought to be more severe episodes. The combination therapy was associated with an approximate 39% reduction in the number of this type of exacerbations compared with placebo (0.46 vs 0.76 exacerbations per year, p<0.0001) but, again, the differences between FSC and salmeterol or fluticasone were not significant. It is worth mentioning that the TRISTAN was longer, but still based on FEV1. Hence, the ability to observe exacerbation differences may have been helped by study duration.
In a study using a design similar to that of the TRISTAN study but including patients with an FEV1 below 50% predicted, CitationSzafranski et al (2003) compared the effects of two inhalations twice daily of either budesonide/formoterol combination (BFC) 160/4.5 μg (delivered dose) in a single inhaler, budesonide 200 μg (metered dose), formoterol 4.5 μg, or placebo for 12 months. Data from this study demonstrate a significant reduction in the number of severe exacerbations by 24% in the BFC group vs placebo, 23% vs formoterol, and 11% vs budesonide. This reflects a mean reduction in the mean annual exacerbation rates of 0.42 (95% CI 0.14–0.70), 1.84–1.42 exacerbations per year when combination therapy was used. Compared with placebo, both BFC and budesonide significantly reduced the number of oral steroid courses used in association with exacerbations (31% and 29%, respectively, compared with 3% for formoterol vs placebo). In addition, BFC significantly reduced the number of oral steroid courses compared with formoterol (−28%). Mild exacerbations were also significantly reduced on BFC when compared with placebo (−62%) and budesonide (−35%), but not with formoterol (−15%).
In another study investigating BFC, CitationCalverley et al (2003b) studied patients who initially received formoterol alone (9 μg delivered dose twice daily) and a short course of oral prednisolone (30 mg once daily) for 2 weeks before randomization. The patients were subsequently randomized to twice daily inhaled BFC 320/9 μg (delivered dose), budesonide 400 μg (metered dose), formoterol 9 μg, or placebo for 12 months, BFC prolonged time to first exacerbation requiring medical intervention, defined as a need for antibiotics and/or oral corticosteroids and/or hospitalization due to respiratory symptoms, compared with all other treatments. Hazard rate analysis showed that the risk of having an exacerbation while being treated with BFC was reduced by 22.7%, 29.5%, and 28.5% vs budesonide, formoterol, and placebo, respectively. The exacerbation rate with BFC was reduced compared with placebo (23.6%) and formoterol (25.5%) but not with budesonide alone (13.6%). Neither budesonide nor formoterol affected either measure of exacerbation compared with placebo. Furthermore, BFC prolonged the time to first course of oral corticosteroids after randomization; risk reductions were 32.7% and 33.8% vs budesonide and formoterol, respectively, and 42.3% vs placebo. BFC also reduced the rate of oral corticosteroid courses by 28.2%, 30.5%, and 44.7% vs budesonide, formoterol, and placebo, respectively; budesonide alone reduced the number of oral corticosteroid courses compared with placebo but formoterol did not.
Considerations on the role of the combination therapy in preventing COPD exacerbations
Data of three large studies (CitationCalverley et al 2003a, Citation2003b; CitationSzafranski et al 2003) that have examined the effects of a combination of LABA and ICS on the risk of developing exacerbation in COPD have shown that the patients receiving combination therapy were less likely to report an exacerbation than those receiving the LABA alone. Nevertheless, a recent Cochrane review (CitationNannini et al 2004) concluded that there were conflicting results when the different combination therapies were compared with the single components alone. In particular, the results of the studies showed that BFC and FSC were effective and reduced the frequency of exacerbations compared with dummy medication to a level of three quarters of the previous rates, with one exacerbation prevented every 2–4 years in the participants in the clinical trials. When the combination treatment was compared with one of the component drugs given as single treatments, BFC was better than its component LABA at preventing the frequency of exacerbations, but FSC did not show a significant advantage over LABA. Recently, two different reviews (CitationHalpin 2005; CitationCazzola 2006), which have evaluated the applicability and clinical relevance of number needed to treat (NNT) analysis for determining the effectiveness of combination therapies against COPD exacerbations, have calculated that for every 100 patients treated with BFC for 1 year, between 42 and 47 exacerbations requiring medical intervention would be prevented vs LABA therapy alone, whereas for every 100 patients treated with FSC for 1 year, only 7 exacerbations would be prevented vs LABA alone (). It should be noted, however, that the NNT value relating to FSC should be interpreted with caution as there was no significant difference between FSC and salmeterol alone (p=0.345 for treatment ratios for combination vs salmeterol therapy). This means that the hypothetical 95% CI would include infinity and that an NNT of infinity should be more appropriately applied to the difference between the two treatments, which indicates no true net clinical benefit of FSC over salmeterol alone.
In any case, in a recent study investigating the effect withdrawal of fluticasone from patients with severe COPD (FEV1 <50% predicted) using FSC (COSMIC study) for 3 months, CitationWouters et al (2005) demonstrated an acute and sustained decrease in FEV1, increase in symptoms, and an increase in mild exacerbations in patients treated with salmeterol alone compared with those who continued treatment with FSC over the one year of the study. These results emphasize the key role of ICSs in managing COPD.
The conflicting findings between the results of the different studies may be accounted for by dissimilar study designs. In particular, definitions of exacerbation that have been used in the examined studies have been rather different (). For example, in Mahler’s study (CitationMahler et al 2002), exacerbation was defined by treatment (mild = increased use of salbutamol; moderate = use of either oral antibiotics and/or corticosteroids; severe = hospitalization). In the Szafranski’s study (CitationSzafranski et al 2003), the definition of mild exacerbation was a day with ≥ 4 inhalations of reliever medication above the mean run-in use, whereas that of severe exacerbation was a requirement for oral steroids and/or antibiotics and/or hospitalization due to respiratory symptoms. In the TRISTAN study (CitationCalverley et al 2003a), exacerbations were defined a priori as a worsening of COPD symptoms that required treatment with antibiotics or oral corticosteroids, or both. Episodes that required corticosteroid treatment or hospital admission were noted separately. CitationPauwels et al (2004) correctly highlighted that considerable heterogeneity in the aetiology and manifestation of COPD exacerbations makes identification and quantification of defining symptoms extremely difficult. However, with the emergence of a number of drugs designed or developed specifically to treat COPD and associated exacerbations, the absence of a uniform definition is a significant issue. In fact, the choice of definition can significantly affect study outcomes, with varying criteria likely to result in different levels of demonstrated treatment success. Furthermore, emerging data confirm that exacerbation is a term not easily understood by patients, who prefer to use simpler words such as “crisis” (CitationHaughney and Gruffydd-Jones 2004).
It is also interesting to stress that there was some difference in the patient populations enrolled in the studies described above. Patients enrolled in the TRISTAN study (CitationCalverley et al 2003a) had to have suffered from at least one episode of acute COPD symptom exacerbation per year in the previous 3 years, and at least one exacerbation in the year immediately before trial entry that required treatment with oral corticosteroids, antibiotics, or both. In the Szafranski study (CitationSzafranski et al 2003), patients had to have suffered from at least one severe (use of oral corticosteroids and/or antibiotics and/or hospitalization due to respiratory symptoms) COPD exacerbation within 2±12 months before the first clinic visit. Moreover, the mean pre-trial FEV1 was 45% predicted in the TRISTAN study (CitationCalverley et al 2003a) and 36% predicted in the Szafranski’s study (CitationSzafranski et al 2003). Moreover, the mean total exacerbation rate per patient per year under placebo was 1.30 in the TRISTAN study (CitationCalverley et al 2003a) and 1.9 in the Szafranski study (CitationSzafranski et al 2003). This differences indicate that the Szafranski’s study (CitationSzafranski et al 2003) probably enrolled patients with more severe disease or, at least, with a higher possibility of suffering from acute exacerbation. In fact, also in the Calverley study (CitationCalverley et al 2003b), the mean pre-trial FEV1 was 36% predicted and the mean total exacerbation rate per patient per year under placebo was 1.80. As correctly highlighted by CitationCalverley et al (2003b), the more severe disease in the patients enrolled in BFC studies is the likely explanation of the greater number of episodes that they observed compared with other studies, a difference that increased the power of the study to detect an effect of treatment. It is also important to highlight that the authors of the three studies did not report the number of exacerbations in the year before the enrolment in the studies. This is a real lack of information because, as recently documented by CitationDonaldson et al (2003), annual exacerbation frequency remains constant over time.
As CitationRabe (2003) stated in his editorial comment on the Calverley paper (CitationCalverley et al 2003b), the data of the combination therapy trials in COPD seem to indicate that patients experiencing more severe exacerbations benefit the most from combination therapy, whereas, if the definition of a (mild) exacerbation for clinical trials also includes aggravation of symptoms, such as in the paper by CitationSzafranski et al (2003), the relative effect of a long-acting bronchodilator might be more pronounced. This clearly highlights the importance of definitions of exacerbations for clinical trials and calls for studies comparing the effect of maximal bronchodilation with, for example, the combination of LABAs with long-acting anticholinergics (LAMAs) in COPD with mild and severe exacerbations as an outcome. In effect, some studies are documenting the clinical value of combining a LABA with a LAMA in COPD (CitationCazzola et al 2004; Citationvan Noord et al 2005, Citation2006), although the information of the impact of such a type of combination on exacerbations is still lacking.
Borrowing Jones’ opinion (CitationJones 2004), we believe that there are a number of possible mechanisms to account for the apparent additive effect of inhaled combination therapy with ICSs and LABAs in preventing exacerbations and to explain the discrepancies observed between the studies. It is likely that: (1) the individual drugs were not at the top of their dose–response curve for this outcome; (2) they have different, and additive, mechanisms of action, which can also be linked to the specific compound; or (3) the different agents were preventing different types of exacerbation. CitationJones (2004) has highlighted that an operational definition based upon a worsening of symptoms and the treatment required (moderate exacerbations are those that can be treated with oral corticosteroids and/or antibiotics, severe exacerbations are those requiring hospital admission) does not identify the type of exacerbation. This emphasizes again the importance for the need of a uniform definition of COPD exacerbation for clinical trials in order to reach more solid conclusions.
Whatever the case may be, it must be emphasized that a treatment regimen with administration of an ICS and LABA in a single inhaler prolongs the time to a first COPD exacerbation, compared with treatment with the single components in patients with an FEV1 <50% predicted (CitationCalverley et al 2003b). Intriguingly, this finding has been observed with BFC (CitationCalverley et al 2003b), but not with FSC (CitationCalverley et al 2003a). The prolonged time to first exacerbation may delay the deterioration of the disease and help maintain health status and patient well-being. It is an important outcome because it indicates that following aggressive treatment of an acute exacerbation with an oral corticosteroid, therapy with an ICS/LABA combination may better control the disease than treatment with bronchodilator alone. In particular, as highlighted by CitationCalverley (2004), combining treatments is certainly something to be considered in patients who have reported exacerbations on a regular basis but have not yet received ICS or LABA therapy in combination, although there are concerns about the increased risk of side-effects and cost of using LABA/ICS therapy in COPD.
Disclosures
Dr Cazzola has received financial support for research and attending meetings and fees for speaking and consulting from Abbott, Altana, AstraZeneca, Boerhinger Ingelheim, Chiesi Farmaceutici, GSK, Meda, Menarini Farmaceutici, Novartis, Pfizer, and Valeas. Dr Hanania has received research grant support from GSK, Boerhinger Ingelheim, AstraZeneca, Dey, Sepracor, and Altana and has served on the advisory board for GSK and Dey. No funding source had any role in the preparation of this paper.
References
- AlsaeediASinDDMcAlisterFA2002The effects of inhaled corticosteroids in chronic obstructive pulmonary disease: a systematic review of randomized placebo-controlled trialsAm J Med113596512106623
- American Thoracic Society/European Respiratory Society2005Standards for the diagnosis and management of patients with COPDAccessed 22 January 2006 URL: http://www.thoracic.org
- BaraniukJNAliMBrodyD1997Glucocorticosteroids induce β2-adrenergic receptor function in human nasal mucosaAm J Respir Crit Care Med155704109032216
- BarnesPJ2000Inhaled corticosteroids are not beneficial in chronic obstructive pulmonary diseaseAm J Respir Crit Care Med161342410673166
- BarnesPJ2004Corticosteroid resistance in airway diseaseProc Am Thorac Soc1264816113444
- BarnesNCQiuYSPavordID2006Antiinflammatory effects of salmeterol/fluticasone propionate in chronic obstructive lung diseaseAm J Respir Crit Care Med1737364316424444
- CalverleyPM2000Inhaled corticosteroids are beneficial in chronic obstructive pulmonary diseaseAm J Respir Crit Care Med161341210673165
- CalverleyPM2004Reducing the frequency and severity of exacerbations of chronic obstructive pulmonary diseaseProc Am Thorac Soc1121416113424
- CalverleyPMBoonsawatWCsekeZ2003bMaintenance therapy with budesonide and formoterol in chronic obstructive pulmonary diseaseEur Respir J22912914680078
- CalverleyPPauwelsRVestboJ2003aTRial of Inhaled STeroids ANd long-acting β2 agonists study group. Combined salmeterol and fluticasone in the treatment of chronic obstructive pulmonary disease: a randomised controlled trialLancet3614495612583942
- CazzolaM2006Application of number needed to treat (NNT) as a measure of treatment effect in respiratory medicineTreat Respir Med5798416512688
- CazzolaMDahlR2004Inhaled combination therapy with long acting β2-agonists and corticosteroids in stable COPDChest1262203715249466
- CazzolaMDi MarcoFSantusP2004The pharmacodynamic effects of single inhaled doses of formoterol, tiotropium and their combination in patients with COPDPulm Pharmacol Ther1735914643169
- CazzolaMSalzilloADe GiglioC2005Treatment of acute exacerbation of severe-to-very severe COPD with azithromycin in patients vaccinated against Streptococcus pneumoniaeRespir Med99663915878482
- ChanezPVignolaAMO’ShaugnessyT1997Corticosteroid reversibility in COPD is related to features of asthmaAm J Respir Crit Care Med1551529349154853
- ChapmanKRWalkerLCluleyS2000Improving patient compliance with asthma therapyRespir Med942910714473
- CouttsJAPGibsonNAPatonJY1992Measuring compliance with inhaled medication in asthmaArch Dis Child6733231575560
- DahlRGreefhorstLANowakD2002Inhaled formoterol dry powder versus ipratropium bromide in chronic obstructive pulmonary diseaseAm J Respir Crit Care Med1647788411549532
- de MeloMNErnstPSuissaS2004Inhaled corticosteroids and the risk of a first exacerbation in COPD patientsEur Respir J23692715176681
- DonaldsonGCSeemungalTABhowmikA2002Relationship between exacerbation frequency and lung function decline in chronic obstructive pulmonary diseaseThorax578475212324669
- DonaldsonGCSeemungalTAPatelIS2003Longitudinal changes in the nature, severity and frequency of COPD exacerbationsEur Respir J22931614680081
- DowlingRBJohnsonMColePJ1999Effect of fluticasone propionate and salmeterol on Pseudomonas aeruginosa infection of the respiratory mucosa in vitroEur Respir J14363910515415
- EdwardsMRJohnsonMJohnstonSL2006Combination therapy: synergistic suppression of virus induced chemokines in airway epithelial cellsAm J Respir Cell Mol Biol119 [Epub ahead of print]
- EickelbergORothMLorxR1999Ligand-independent activation of the glucocorticoid receptor by β2-adrenergic receptor agonists in primary human lung fibroblasts and vascular smooth muscle cellsJ Biol Chem2741005109873044
- Global Initiative for Chronic Obstructive Lung Disease2005Global Strategy for the Diagnosis Management and Prevention of Chronic Obstructive Pulmonary Disease NHBLI/WHO Workshop ReportAccessed 22 January 2006 URL: http://www.goldcopd.com
- HalpinDM2005Evaluating the effectiveness of combination therapy to prevent COPD exacerbations: the value of NNT analysisInt J Clin Pract5911879416178987
- HananiaNADarkenPHorstmanD2003The efficacy and safety of fluticasone propionate (250 μg)/salmeterol (50 μg) combined in the Diskus inhaler for the treatment of COPDChest1248344312970006
- HaughneyJGruffydd-JonesK2004Patient-centred outcomes in primary care management of COPD - what do recent clinical trial data tell us?Primary Care Resp J1318597
- JonesPW2004Clinical effects of inhaled corticosteroids in chronic obstructive pulmonary diseaseProc Am Thorac Soc11677016113430
- JonesPWWillitsLRBurgePS2003Disease severity and the effect of fluticasone propionate on chronic obstructive pulmonary disease exacerbationsEur Respir J21687312570111
- KiriVAPrideNBSorianoJB2005Inhaled corticosteroids in chronic obstructive pulmonary disease: results from two observational designs free of immortal time biasAm J Respir Crit Care Med172460415901610
- KornSHJerreABrattsandR2001Effects of formoterol and budesonide on GM-CSF and IL-8 secretion by triggered human bronchial epithelial cellsEur Respir J171070711491146
- MahlerDAWirePHorstmanD2002Effectiveness of fluticasone propionate and salmeterol combination delivered via the Diskus device in the treatment of chronic obstructive pulmonary diseaseAm J Respir Crit Care Med16610849112379552
- MakJCNishikawaMShirasakiH1995Protective effects of a glucocorticoid on downregulation of pulmonary β2-adrenergic receptors in vivoJ Clin Invest96991067615841
- ManSFSinDD2005Inhaled corticosteroids in chronic obstructive pulmonary disease: is there a clinical benefit?Drugs655799115748094
- MartinezFJAnzuetoA2005Appropriate outpatient treatment of acute bacterial exacerbations of chronic bronchitisAm J Med118Suppl 7AS3944
- NanniniLCatesCJLassersonTJ2004Combined corticosteroid and long-acting β-agonist in one inhaler for chronic obstructive pulmonary diseaseCochrane Database Syst Rev3CD00379415266502
- Niewoehn2004Interventions to prevent chronic obstructive pulmonary disease exacerbationsAm J Med117Suppl 12AS418
- PangLKnoxAJ2000Synergistic inhibition by β2-agonists and corticosteroids on tumor necrosis factor-α-induced interleukin-8 release from cultured human airway smooth-muscle cellsAm J Respir Cell Mol Biol23798510873156
- PangLKnoxAJ2001Regulation of TNF-β-induced eotaxin release from cultured human airway smooth muscle cells by β2-agonists and corticosteroidsFASEB J15261911149914
- PauwelsRCalverleyPBuistAS2004COPD exacerbations: the importance of a standard definitionRespir Med989910714971871
- RabeK2003Combination therapy for chronic obstructive pulmonary disease: one size fits all?Eur Respir J22874514680071
- RennardSI2004Treatment of stable chronic obstructive pulmonary diseaseLancet36479180215337408
- SeemungalTHarper-OwenRBhowmikA2001Respiratory viruses, symptoms, and inflammatory markers in acute exacerbations and stable chronic obstructive pulmonary diseaseAm J Respir Crit Care Med16416182311719299
- SeetoLJBurgessJKJohnsonPR2003Effect of fluticasone and salmeterol on human alveolar macrophage cytokine production in patients with chronic obstructive pulmonary disease (COPD) [abstract]Am J Respir Crit Care Med167A318
- SinDDWuLAndersonJAAnthonisenNR2005Inhaled corticosteroids and mortality in chronic obstructive pulmonary diseaseThorax60992716227327
- SolèrM2005Modulation of airway inflammation to prevent exacerbations of COPDEur Respir Rev147882
- StockleyRAChopraNRiceL2006Addition of salmeterol to existing treatment in patients with COPD: a 12 month studyThorax61122816443706
- SuissaS2006Statistical treatment of exacerbations in therapeutic trials of chronic obstructive pulmonary diseaseAm J Respir Crit Care Med173842616439716
- SzafranskiWCukierARamirezA2003Efficacy and safety of budesonide/formoterol in the management of chronic obstructive pulmonary diseaseEur Respir J21748112570112
- TsangKWRutmanATanakaE1994Interaction of Pseudomonas aeruginosa with human respiratory mucosa in vitroEur Respir J71746537828679
- TseRMarroquinBADorscheidDR2003β-adrenergic agonists inhibit corticosteroid-induced apoptosis of airway epithelial cellsAm J Physiol Lung Cell Mol Physiol285L39340412730077
- van der ValkPMonninkhofEvan der PalenJ2002Effect of discontinuation of inhaled corticosteroids in patients with chronic obstructive pulmonary disease: the COPE studyAm J Respir Crit Care Med16613586312406823
- van NoordJAAumannJLJanssensE2005Comparison of tiotropium once daily, formoterol twice daily and both combined once daily in patients with COPDEur Respir J262142216055868
- van NoordJAAumannJLJanssensE2006Effects of tiotropium with and without formoterol on airflow obstruction and resting hyper-inflation in patients with COPDChest1295091716537846
- WilsonR1991Infections of the airwaysCurr Opin Infect Dis416677
- WoutersEFMPostmaDSFokkenstB2005Withdrawal of fluticasone propionate from combined salmeterol/fluticasone treatment in patients with COPD causes an immediate and sustained disease deterioration: a randomised controlled trialThorax60480715923248