Abstract
We studied 21 COPD patients in stable clinical conditions to evaluate whether changes in lung function induced by cumulative doses of salbutamol alter diffusing capacity for carbon monoxide (DLCO), and whether this relates to the extent of emphysema as assessed by high resolution computed tomography (HRCT) quantitative analysis. Spirometry and DLCO were measured before and after cumulative doses of inhaled salbutamol (from 200 μg to 1000 μg). Salbutamol caused significant increments of forced vital capacity (FVC), forced expiratory volume in one second (FEV1), and flows at 30% of control FVC taken from both partial and maximal forced expiratory maneuvers. Functional residual capacity and residual volume were reduced, while total lung capacity did not change significantly. DLCO increased progressively with the incremental doses of salbutamol, but this became significant only at the highest dose (1000 μg) and was independent of the extent of emphysema, as assessed by radiological parameters. No significant changes were observed in CO transfer factor (DLCO/VA) and alveolar volume (VA). The results suggest that changes in lung function induced by cumulative doses of inhaled salbutamol are associated with a slight but significant increase in DLCO irrespective of the presence and extent of emphysema.
Introduction
In chronic obstructive pulmonary disease (COPD) carbon monoxide uptake in the lung (DLCO) is determined to assess the associated presence of emphysema (CitationPauwels et al 2001). Reduction of the parameter is deemed to be due to functional and/or anatomical reductions of the alveolar and capillary surfaces available for gas exchange (CitationKrogh 1915; CitationCadigan et al 1961; CitationRose et al 1979). For bronchodilator therapy may improve lung volume recruitment as a result of a decrease in RV in both chronic obstructive bronchitis and emphysema (CitationCerveri et al 2000), and thus increase the amount of gas inhaled with a single inspiration, it would be reasonable to expect an increase in DLCO in COPD after bronchodilatation. However, the few studies conducted in this regard gave contrasting results. Two studies demonstrated that at least for diagnostic purposes, the test may be safely performed either before or after dilator agonists (CitationJones et al 1961; CitationChinn et al 1988), whereas a study showed a significant increase in DLCO with inhaled terbutaline 1.5 mg (CitationÅkesson et al 2000). Part of these discrepancies could be explained by the different degree of bronchodilatation achieved with different pharmacological agents and/or the variable association of emphysema with chronic obstructive bronchitis in COPD, both possibly affecting the DLCO measurement as a result of different lung volume and pulmonary vascular bed recruitment.
Gaining information on the effects of the bronchodilator agents on the test is clinically relevant as DLCO is a functional marker of the progression of a disease treated with different therapeutic protocols and doses of beta-2 agonists. Indeed, the variable course of the disease and/or the chronic effects of bronchodilator therapy may lead to recruitment of alveolar volume within lung regions previously served by closed or near-closed airways and/or improvement of blood perfusion across the lung over time, thus potentially affecting the DLCO and its interpretation.
On this ground, we wondered whether DLCO varies with the degree of pharmacologically-induced bronchodilatation and/or extent of emphysema in COPD.
To test this hypothesis, we studied lung function and diffusing capacity before and after cumulative doses of inhaled salbutamol. The study was conducted in a group of 21 COPD patients well characterized for degree of emphysema, as assessed by radiological criteria.
Methods
Patients
Eighteen male and tree female patients affected by COPD, as defined by the international guidelines (CitationPauwels et al 2001) participated in the study (). Six of them were current smokers and fifteen former smokers, with an average smoking history of 51.6 ± 18.8 pack-years. Airflow obstruction ranged from moderately severe to very severe. All patients were required to abstain from short-acting bronchodilators for at least 12 h prior to each study session, to be in stable clinical conditions, and not to have suffered from respiratory exacerbation in the previous four weeks. The Ethics Committee approved the experimental protocol, and a written informed consent was obtained prior to the study from each subject.
Table 1 Main anthropometric, functional, and imaging data
Study design
The patients attended the laboratory in the morning of two separate days. On the first day, absolute lung volumes, DLCO, and partial (PEFV) and maximal (MEFV) flow-volume curves were measured at baseline (Step 1). The same measurements were repeated in the same order 15 min after each of the following sequential doses of salbutamol given through a spacer by metered dose inhaler: 200 μg (Step 2), 400 μg (Step 3), and 400μg (Step 4). The doses were chosen to cover at least part of the broad range of bronchodilator responses reported in COPD (CitationAnthonisen et al 1986; CitationCalverley et al 2003). On the second day, a high resolution computed tomography (HRCT) of the lung was obtained.
Lung function measurements
Inspired and expired volumes were obtained by numerical integration of mouth flow measured by a mass flow sensor (Sensor Medics, Yorba Linda, CA). After at least 8 regular tidal breaths, the patients were asked to expire forcefully from about 60% of vital capacity (VC) to residual volume (RV) (PEFV maneuver), to rapidly inspire to total lung capacity (TLC), and forcefully expire to RV (MEFV maneuver) without breath hold. The latter allowed the forced expiratory volume in one second (FEV1) and forced vital capacity (FVC) to be computed. At least three technically acceptable curves were recorded. Flows at 30% of control FVC were taken on MEFV (Vmax30) and PEFV (Vpart30) curves.
Lung volumes were measured with the patients sitting in a body plethysmograph (Jaeger Masterlab, Jaeger, Würzburg, Germany) and panting against a closed shutter at a frequency slightly <1 Hz, cheeks supported by hands. TLC was obtained as the sum of thoracic gas volume (TGV) and the linked inspiratory capacity. Functional residual capacity (FRC) was obtained from TGV corrected for any difference between the volume at which the shutter was closed and the average end-expiratory volume of the four preceding regular tidal breaths. RV was the difference between TLC and VC. Predicted values for spirometry and lung volume are from Quanjer and colleagues (1979).
DLCO was measured according to the American Thoracic Society (ATS) recommendations (CitationCrapo et al 1995) with a Baires System (Biomedin, Padua, Italy), using a gas mixture of 0.3% CO, 10% helium, and balance air. Breath holding time was measured by the method of Jones-Meade (CitationJones and Meade 1961). At each step of the study, two measurements of DLCO were made at a 4-min interval and were accepted if their inspired volumes were within 0.2 L between each other and 10% of the VC measured by spirometry. Adjustment for carboxyhemoglobin (HbCO) to account for the effect of increasing CO concentrations, and adjustment for Hb concentrations with repeated DLCO measurements were done according to the ATS statement (CitationATS 1987) in 10 patients who had their arterial blood drawn at the four steps of the study. In the other 11 patients, DLCO was corrected for the average slope of the linear regression analysis of DLCO adjusted versus nonadjusted for HbCO in the 10 patients. Reference values for DLCO are from CitationCotes (1979).
Imaging
Lung HRCT was performed with a third-generation, continuous-rotation-computerized tomograph with single scan acquisition (Somaton Plus, Siemens, Erlangen, Germany). Technical parameters were the following: 1mm collimation, 137 kVp, 195 mAs, and <1s scanning time. The lungs were scanned from the apex through the base at 1cm intervals and reconstructed with a lung algorithm.
All scan images were processed off-line using a semiautomated image-processing program, which extracts boundaries of the lungs, calculates lung cross sectional areas and histograms of attenuation values (CT numbers) of individual highlighted sections, and summarizes data to obtain the frequency distribution of attenuation values for both lungs. From the frequency distribution of CT numbers, mean CT number in Hounsfield units (HU) were derived. Percent of the whole lung area with attenuation values lower than −950 HU (RA950) was taken as an index of extent of emphysema (CitationGevenois et al 1995, Citation1996).
Statistical analysis
Data are expressed as mean ± standard deviation. Relationships between variables were tested by linear regression analysis. Analysis of variance (ANOVA) for repeated measures was used to compare the effects of increasing doses of salbutamol at the different steps. When F values were significant, Tukey’s post hoc test was used for multiple comparisons. P < 0.05 was considered statistically significant.
Results
The severity of airway obstruction, based on spirometric data, ranged from moderate to very severe (). Emphysema was variably present, as suggested by the wide ranges of RA950, lung hyperinflation and DLCO ().
Seventeen patients completed the four steps of study, and four asked to interrupt the test at step 3 after a cumulative dose of 600 μg. Increasing the dose of salbutamol caused a progressive and significant increase in Vmax30, V part30, FEV1, and FVC, and a decrease in FRC and RV, consistent with effective bronchodilatation and decrease in lung hyperinflation (). Average DLCO progressively increased with bronchodilatation, but this became significant only with the highest dose of salbutamol (p < 0.05) (). In contrast, no significant changes occurred in VA and DLCO/VA ().
Table 2 Main respiratory functional parameters at baseline and after additional doses of salbutamol
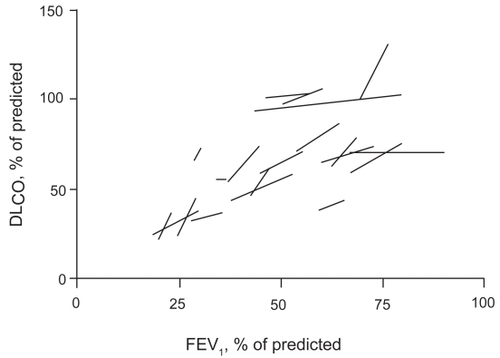
The slopes of linear regression analysis of DLCO plotted against FEV1, VC, and FRC at the four steps in individual patients were significantly different from 0 ( and ), thus suggesting that DLCO tended to increase with bronchodilatation and volume recruitment. In contrast, only the slope of the linear regression of DLCO/VA versus FEV1attained statistical significance ().
Table 3 Average linear regression slopes of DLCO, and DLCO/VA versus key variables with inhalation of increasing doses of salbutamol.
Figure 1 Linear regression lines of DLCO versus FEV1 with incremental doses of salbutamol in individual patients. Values are expressed as % of predicted.
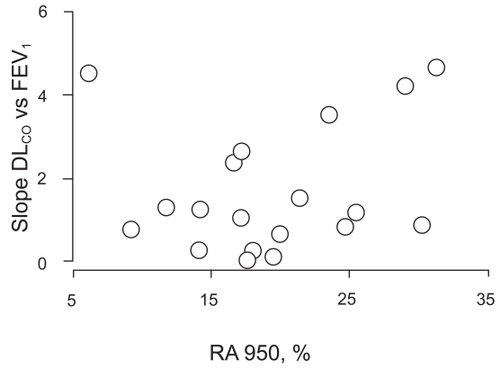
Neither of these slopes correlated with the extent of emphysema as assessed by HRCT scan, thus suggesting that DLCO increased with bronchodilatation irrespective of the extent of emphysema, as assessed with imaging techniques ().
Figure 2 Relationships between linear regression slopes of DLCO versus FEV1 with increasing doses of salbutamol and extent of emphysema, as assessed by HRCT scan quantitative analysis (RA950).
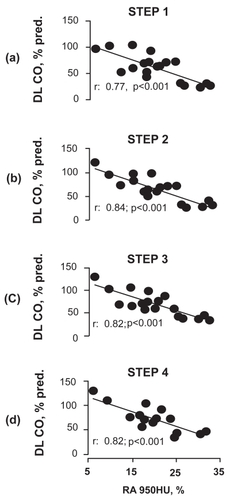
DLCO % pred correlated with the extent of emphysema at all 4 steps of the study ().
Figure 3 Relationships between DLCO as % of predicted and extent of emphysema, as assessed by HRCT scan quantitative analysis (RA950), at the four steps of the study.
Discussion
The major findings of the present study on COPD patients are that DLCO progressively increased with cumulative doses of inhaled salbutamol to become significant at doses higher than those commonly used for clinical treatments. In addition, this occurred independently of the presence and extent of emphysema, as assessed by radiological parameters. VA tended to increase, so that DLCO/VA remained unchanged.
Theory predicts that VA, permeability characteristics of the alveolar-to-capillary barrier, and ability of hemoglobin to combine with CO are the main determinants of DLCO (CitationKrogh 1915; CitationCadigan et al 1961; CitationChinn et al 1988). Therefore, any intervention resulting in recruitment of lung volume would be expected to increase DLCO. Unexpectedly however, the substantial increase in slow VC observed with salbutamol in our COPD patients was not associated with a significant increase in DLCO. The increment in VC was due to a decrease in RV and not to an increase in TLC, which suggests opening of airways previously closed. Had the lack of increase in DLCO mostly manifested in patients with low lung elastic recoil as in emphysema despite the decrease in RV, this would have been presumably the result of opening of airways subtending enlarged emphysematous units with disrupted vascular component unable to subtract CO from the alveoli. The absence of any relationship between changes in DLCO and DLCO/VA after salbutamol and HRCT data suggests, therefore, additional and/or alternative mechanisms. Among them is the possibility that VA was already fully recruited at maximal inflation even before inhaling the bronchodilator. Under these conditions, the effects of the medication on bronchial tone were negligible to recruit new VA useful for gas exchange. Alternatively, alveolar recruitment with salbutamol in COPD occurred in the airways subtending alveolar units with hypoxic vasoconstriction. As documented in many animal species including humans, a decrease in O2 tension in the alveolar compartment would cause a local increase in pulmonary vascular resistance, as a result of narrowing of pre-capillary arteries by mechanisms involving K+ and Ca++ channels (CitationPost et al 1992) and enhanced by local acidosis (CitationEnson et al 1964). With bronchodilatation and ensuing alveolar recruitment, hypoxic vasoconstriction might have disappeared and DLCO increased, unless vascular reopening lagged behind alveolar reopening.
An additional cause for an increased DLCO with high doses of salbutamol might have been the increase in cardiac output and the resulting distension of the pulmonary bed. Though we do not bring direct evidence for this, the increase in heart rate reported in healthy volunteers after doses of salbutamol similar to ours (CitationBremner et al 1993) would suggest that the cardiovascular side-effects of high doses of β2 agonists might be indeed capable of increasing cardiac output, thus possibly contributing to increase DLCO. Yet, it remains to demonstrate that these doses of salbutamol can really do that.
Previous studies have documented that imposing an inspiratory resistance in healthy subjects is associated with an increase in DLCO, as a result of an increase in pleural pressure and ensuing amount of blood shifted from the abdomen to the chest wall and lungs (CitationCotes et al 1960; CitationSmith et al 1969). By converse, a decreased inspiratory resistance would be expected to lower DLCO. Whether the bronchodilatation observed in the present study might have affected DLCO is a matter of speculation, though it could have also contributed to blunt the expected increase in DLCO.
The fact that DLCO increased with progressive reduction in bronchial tone may have some clinical relevance. For instance, in clinical trials using this parameter as a functional outcome for follow-up or evaluation of the effects of new, nonbronchodilator treatments in emphysema, any significant change of DLCO should be taken with cautiousness before concluding that this reflects a clear disease modification. In contrast, the maintenance of the correlation between DLCO as % pred and extent of emphysema () at all 4 steps would apparently suggest that the effect of bronchial tone on DLCO is insignificant with respect to the diagnosis of the disease.
In conclusion, the present study documents that improved lung function induced with cumulative doses of inhaled salbutamol is associated with a slight but significant increase in DLCO irrespective of the presence and extent of emphysema. These findings implicate that changes in DLCO over time, as observed in clinical or therapeutic trials, may be at least in part affected by changes in airway caliber.
References
- [ATS] American Thoracic Society1987Single breath carbon monoxide diffusing capacity (transfer factor). Recommendations for a standard technique. Statement of the American Thoracic SocietyAm Rev Respir Dis13612993073674590
- ÅkessonUDahlströmJ-AWollmerP2000Changes in transfer factor of the lung in response to bronchodilatationClin Physiol20141810651787
- AnthonisenNRWrightEC1986Bronchodilator response in chronic obstructive pulmonary diseaseAm Rev Respir Dis133814193706890
- BremnerPWoodmanKBurgessC1993A comparison of the cardiovascular effects of formoterol, salbutamol and fenoterolEur Respir J6204108095240
- CadiganJBMarksAEllicottMF1961An analysis of factor affecting the measurement of pulmonary diffusing capacity by the single breath methodJ Clin Invest40149551413689722
- CalverleyPMABurgePSSpencerSthe Isolde Study Investigators2003Bronchodilator reversibility testing in chronic obstructive pulmonary diseaseThorax586596412885978
- CerveriIPellegrinoRDoreR2000Mechanisms for isolated volume response to a broncho-dilator in patients with COPDJ Appl Physiol8819899510846010
- ChinnDJAskewJRowleyL1988Measurement technique influences the response of transfer factor (TLCO) to salbutamol in patients with airflow limitationEur Respir J115213366232
- CotesJESnidalDPShepardRH1960Effect of negative intra-alveolar pressure on pulmonary diffusing capacityJ Appl Physiol15372613812266
- CotesJE1979Lung function: assessment and application in medicineOxford4th edBlackwell Scientific Publication
- CrapoROHankinsonJLIrvinC1995Single-breath carbon monoxide diffusing capacity (Transfer factor). Recommendations for a standard technique - 1995 UpdateAm J Respir Crit Care Med1522185988520796
- EnsonYGiuntiniCLewisML1964The influence of hydrogen ion concentration and hypoxemia on the pulmonary circulationJ Clin Invest4311466214171792
- GevenoisPADe MaertelaerVDeVuystP1995Comparison of computed density and macroscopic morphometry in pulmonary emphysemaAm J Respir Crit Care Med15265377633722
- GevenoisPADeVuystPDe MaertelaerV1996Comparison of computed density and macroscopic morphometry in pulmonary emphysemaAm J Respir Crit Care Med154187928680679
- JonesRSMeadeF1961A theoretical and experimental analysis of anomalies in the estimation of pulmonary diffusing capacity by single breath methodQ J Exp Physiol4613143
- KroghM1915The diffusion of gases through the lungs of manJ Physiol London4927130016993296
- PauwelsRABuistSCalverleyPMA2001Global Strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. NHLBI/WHO Global initiative for chronic obstructive lung disease (GOLD)Am J Respir Crit Care Med16312567611316667
- PostJMHumeJRArcherSL1992Direct role for the potassium channel inhibition in hypoxic pulmonary vasoconstrictionAm J Physiol262C882901566816
- QuanjerPhHTammelingGJCotesJE1993Standardized lung function testingEur Respir J65408381090
- RoseGLCassidySSJohnsonRLJr1979Diffusing capacity at different lung volumes during breath holding and rebreathingJ Appl Physiol47327468670
- SmithTCRankinJ1969Pulmonary diffusing capacity and the capillary bed during Valsalva and Müller maneuversJ Appl Physiol27826334901006